
Effects of Uni- vs. Bilateral Upper Limb Robot-Assisted Rehabilitation on Motor Function, Activities of Daily Living, and Electromyography in Hemiplegic Stroke: A Single-Blinded Three-Arm Randomized Controlled Trial
 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Setting, Recruitment, and Consent
2.3. Participants
2.4. Interventions
2.4.1. Unilateral
2.4.2. Bilateral
2.4.3. Conventional
2.5. Outcomes
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Randomization
2.7. Blinding
2.8. Sample Size Calculation
2.9. Statistical Analysis
3. Results
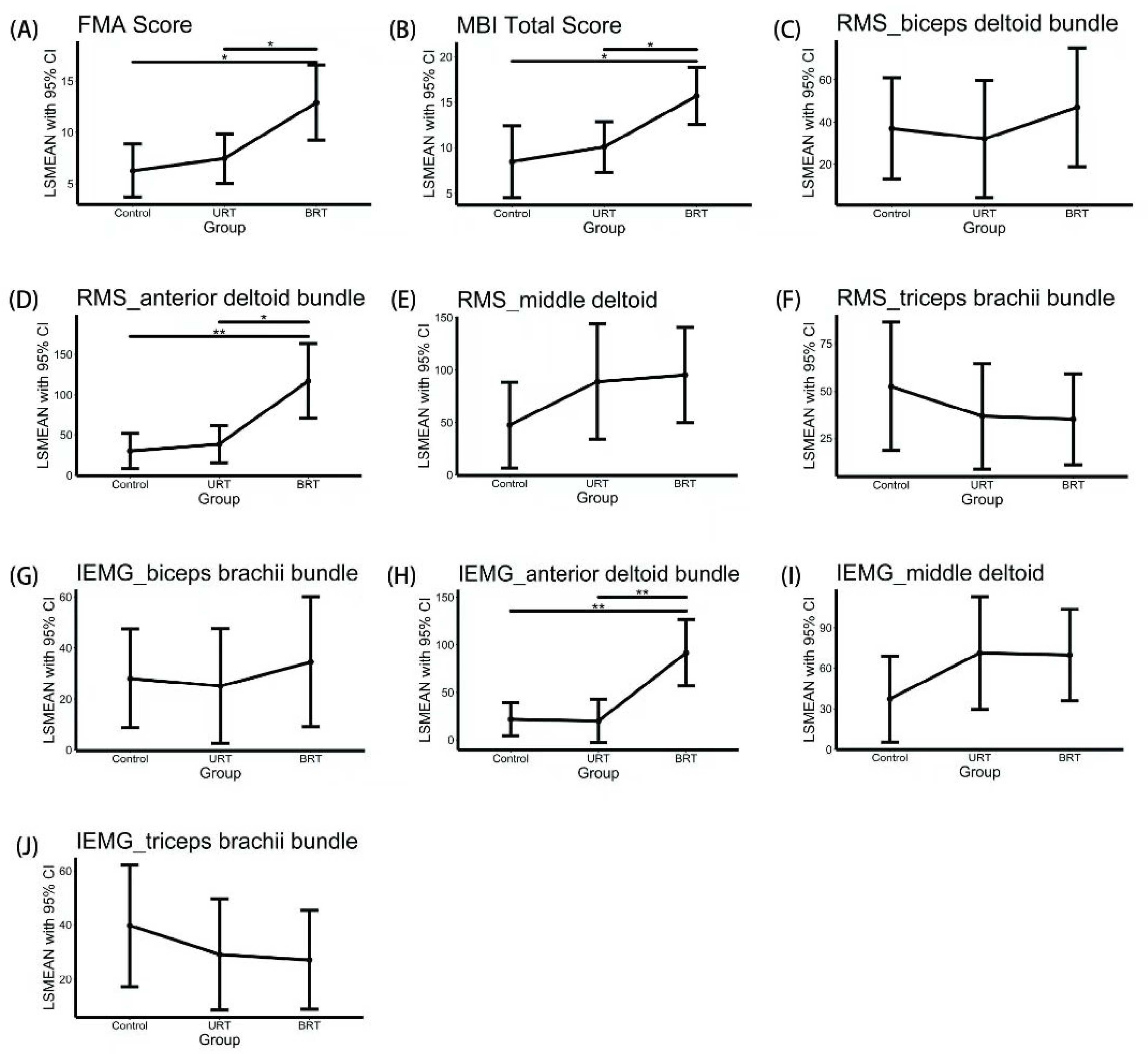
3.1. Primary Outcome Measure
3.2. Secondary Outcome Measures
3.3. Sensitivity Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saini, V.; Guada, L.; Yavagal, D.R. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology 2021, 97, S6–S16. [Google Scholar] [CrossRef]
- Rodgers, H.; Bosomworth, H.; Krebs, H.I.; van Wijck, F.; Howel, D.; Wilson, N.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Robot assisted training for the upper limb after stroke (RATULS): A multicentre randomised controlled trial. Lancet 2019, 394, 51–62. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Mekbib, D.B.; Zhao, Z.; Wang, J.; Xu, B.; Zhang, L.; Cheng, R.; Fang, S.; Shao, Y.; Yang, W.; Han, J.; et al. Proactive Motor Functional Recovery Following Immersive Virtual Reality–Based Limb Mirroring Therapy in Patients with Subacute Stroke. Neurotherapeutics 2020, 17, 1919–1930. [Google Scholar] [CrossRef] [PubMed]
- Dehem, S.; Gilliaux, M.; Stoquart, G.; Detrembleur, C.; Jacquemin, G.; Palumbo, S.; Frederick, A.; Lejeune, T. Effectiveness of upper-limb robotic-assisted therapy in the early rehabilitation phase after stroke: A single-blind, randomised, controlled trial. Ann. Phys. Rehabil. Med. 2019, 62, 313–320. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Sinigaglia, C. The mirror mechanism: A basic principle of brain function. Nat. Rev. Neurosci. 2016, 17, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Veerbeek, J.M.; Van Wegen, E.E.H.; Wolf, S.L. Constraint-induced movement therapy after stroke. Lancet Neurol. 2015, 14, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, D.; Sirtori, V.; Castellini, G.; Moja, L.; Gatti, R. Constraint-induced movement therapy for upper extremities in people with stroke. Cochrane Database Syst. Rev. 2015, 2015, CD004433. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Okita, Y.; Kubo, H.; Hachisuka, K.; Domen, K. Impact of the robotic-assistance level on upper extremity function in stroke patients receiving adjunct robotic rehabilitation: Sub-analysis of a randomized clinical trial. J. Neuroeng. Rehabil. 2022, 19, 1–10. [Google Scholar] [CrossRef]
- Budhota, A.; Chua, K.S.G.; Hussain, A.; Kager, S.; Cherpin, A.; Contu, S.; Vishwanath, D.; Kuah, C.W.K.; Ng, C.Y.; Yam, L.H.L.; et al. Robotic Assisted Upper Limb Training Post Stroke: A Randomized Control Trial Using Combinatory Approach To-ward Reducing Workforce Demands. Front. Neurol. 2021, 12, 622014. [Google Scholar] [CrossRef] [PubMed]
- Kiper, P.; Szczudlik, A.; Agostini, M.; Opara, J.; Nowobilski, R.; Ventura, L.; Tonin, P.; Turolla, A. Virtual Reality for Upper Limb Rehabilitation in Subacute and Chronic Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 834–842.e4. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Imura, T.; Suzukawa, T.; Fukuyama, H.; Ishii, T.; Taki, S.; Imada, N.; Shibukawa, M.; Inagawa, T.; Araki, H.; et al. Combination of Exoskeletal Upper Limb Robot and Occupational Therapy Improve Activities of Daily Living Function in Acute Stroke Patients. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2019, 28, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, T.; Takahashi, K.; Amano, S.; Gosho, M.; Sakai, M.; Hashimoto, K.; Hachisuka, K.; Uchiyama, Y.; Domen, K. Robot-Assisted Training as Self-Training for Upper-Limb Hemiplegia in Chronic Stroke: A Randomized Controlled Trial. Stroke 2022, 53, 2182–2191. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Werner, C.; Pohl, M.; Rueckriem, S.; Mehrholz, J.; Lingnau, M.L. Computerized arm training improves the motor control of the severely affected arm after stroke: A single-blinded randomized trial in two centers. Stroke 2005, 36, 1960–1966. [Google Scholar] [CrossRef]
- Liao, W.W.; Wu, C.Y.; Hsieh, Y.W.; Lin, K.C.; Chang, W.Y. Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic stroke: A randomized controlled trial. Clin. Rehabil. 2012, 26, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-W.; Wu, C.-Y.; Wang, W.-E.; Lin, K.-C.; Chang, K.-C.; Chen, C.-C.; Liu, C.-T. Bilateral robotic priming before task-oriented approach in subacute stroke rehabilitation: A pilot randomized controlled trial. Clin. Rehabil. 2016, 31, 225–233. [Google Scholar] [CrossRef]
- Hung, C.-S.; Hsieh, Y.-W.; Wu, C.-Y.; Chen, Y.-J.; Lin, K.-C.; Chen, C.-L.; Yao, K.G.; Liu, C.-T.; Horng, Y.-S. Hybrid Rehabilitation Therapies on Upper-Limb Function and Goal Attainment in Chronic Stroke. OTJR Occup. Particip. Health 2019, 39, 116–123. [Google Scholar] [CrossRef]
- Hung, C.-S.; Lin, K.-C.; Chang, W.-Y.; Huang, W.-C.; Chang, Y.-J.; Chen, C.-L.; Yao, K.G.; Lee, Y.-Y. Unilateral vs Bilateral Hybrid Approaches for Upper Limb Rehabilitation in Chronic Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 2225–2232. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Yang, C.L.; Chen, M.D.; Lin, K.C.; Wu, L.L. Unilateral versus bilateral robot-assisted reha-bilitation on arm-trunk control and functions post stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2013, 10, 35. [Google Scholar] [CrossRef]
- Nouredanesh, M.; Frazer, M.; Tung, J.; Jeon, S.; Arami, A. Effect of Visual Information on Dominant and Non-dominant Hands During Bimanual Drawing with a Robotic Platform. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 1221–1226. [Google Scholar] [CrossRef]
- Nudo, R.J. Recovery after brain injury: Mechanisms and principles. Front. Hum. Neurosci. 2013, 7, 887. [Google Scholar] [CrossRef]
- Liu, L.; Chen, W.; Zhou, H.; Duan, W.; Li, S.; Huo, X.; Xu, W.; Huang, L.A.; Zheng, H.; Liu, J.; et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: Executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc. Neurol. 2020, 5, 159–176. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Smith, M.B. Interrater Reliability of a Modified Ashworth Scale of Muscle Spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Ohura, T.; Hase, K.; Nakajima, Y.; Nakayama, T. Validity and reliability of a performance evaluation tool based on the modified Barthel Index for stroke patients. BMC Med Res. Methodol. 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Merletti, R.; Hermens, H. Introduction to the special issue on the SENIAM European Concerted Action. J. Electromyogr. Kinesiol. 2000, 10, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.G.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.W.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef] [PubMed]
- Arya, K.N.; Verma, R.; Garg, R.K. Estimating the minimal clinically important difference of an upper ex-tremity recovery measure in subacute stroke patients. Top Stroke Rehabil. 2011, 18, 599–610. [Google Scholar] [CrossRef]
- Ma, D.; Li, X.; Xu, Q.; Yang, F.; Feng, Y.; Wang, W.; Huang, J.-J.; Pei, Y.-C.; Pan, Y. Robot-Assisted Bimanual Training Improves Hand Function in Patients with Subacute Stroke: A Randomized Controlled Pilot Study. Front. Neurol. 2022, 13, 884261. [Google Scholar] [CrossRef]
- Coffman, C.J.; Edelman, D.; Woolson, R.F. To condition or not condition? Analysing ‘change’ in longitudinal randomised controlled trials. BMJ Open 2016, 6, e013096. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Yang, L. Comparison of Several Filling Methods and Their Application in Longitudinal Data Missing. Master’s Thesis, Shanxi Medical University, Taiyuan, China, 2014. [Google Scholar]
- Wu, C.-Y.; Yang, C.-L.; Chuang, L.-L.; Lin, K.-C.; Chen, H.-C.; Chen, M.-D.; Huang, W.-C. Effect of Therapist-Based Versus Robot-Assisted Bilateral Arm Training on Motor Control, Functional Performance, and Quality of Life After Chronic Stroke: A Clinical Trial. Phys. Ther. 2012, 92, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-W.; Liing, R.-J.; Lin, K.-C.; Wu, C.-Y.; Liou, T.-H.; Lin, J.-C.; Hung, J.-W. Sequencing bilateral robot-assisted arm therapy and constraint-induced therapy improves reach to press and trunk kinematics in patients with stroke. J. Neuroeng. Rehabil. 2016, 13, 1–9. [Google Scholar] [CrossRef]
- Hsu, H.; Chiu, H.; Kuan, T.; Tsai, C.; Su, F.; Kuo, L. Robotic-assisted therapy with bilateral practice improves task and motor performance in the upper extremities of chronic stroke patients: A randomised controlled trial. Aust. Occup. Ther. J. 2019, 66, 637–647. [Google Scholar] [CrossRef]
- Yang, C.-L.; Lin, K.-C.; Chen, H.-C.; Wu, C.-Y.; Chen, C.-L. Pilot Comparative Study of Unilateral and Bilateral Robot-Assisted Training on Upper-Extremity Performance in Patients with Stroke. Am. J. Occup. Ther. 2012, 66, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.-T.; Lin, K.-C.; Liu, H.-L.; Wu, C.-Y.; Wai, Y.-Y.; Lee, T.-H. Neural correlates of motor recovery after robot-assisted stroke rehabilitation: A case series study. Neurocase 2016, 22, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; Van Wegen EE, H.; Meskers CG, M.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke: A Systematic Review and Meta-analysis. Neurorehabilit. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef]
- Jia, J. Exploration on neurobiological mechanisms of the central–peripheral–central closed-loop rehabilitation. Front. Cell. Neurosci. 2022, 16, 982881. [Google Scholar] [CrossRef]
- Zhu, G.; Zhang, X.; Tang, X.; Chen, X.; Gao, X. Examining and monitoring paretic muscle changes during stroke rehabilitation using surface electromyography: A pilot study. Math. Biosci. Eng. 2019, 17, 216–234. [Google Scholar] [CrossRef] [PubMed]
- Murase, N.; Duque, J.; Mazzocchio, R.; Cohen, L.G. Influence of interhemispheric interactions on motor function in chronic stroke. Ann. Neurol. 2004, 55, 400–409. [Google Scholar] [CrossRef]
- Bakker, C.; Massa, M.; Daffertshofer, A.; Pasman, J.; van Kuijk, A.; Kwakkel, G.; Stegeman, D. The addition of the MEP amplitude of finger extension muscles to clinical predictors of hand function after stroke: A prospective cohort study. Restor. Neurol. Neurosci. 2019, 37, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Fujiki, M.; Matsushita, W.; Kawasaki, Y.; Fudaba, H. Monophasic-Quadripulse Theta Burst Magnetic Stimulation for Motor Palsy Functional Evaluation After Intracerebral Hemorrhage. Front. Integr. Neurosci. 2022, 16, 827518. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.J.; Gallina, A.; Neva, J.L.; Ivanova, T.D.; Snow, N.J.; Ledwell, N.M.; Xiao, Z.G.; Menon, C.; Boyd, L.A.; Garland, S.J. Effect of repetitive transcranial magnetic stimulation combined with robot-assisted training on wrist muscle activation post-stroke. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2019, 130, 1271–1279. [Google Scholar] [CrossRef]
- Simkins, M.; Kim, H.; Abrams, G.; Byl, N.; Rosen, J. Robotic unilateral and bilateral upper-limb movement training for stroke survivors afflicted by chronic hemiparesis. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–6. [Google Scholar] [CrossRef]
- Ranzani, R.; Lambercy, O.; Metzger, J.-C.; Califfi, A.; Regazzi, S.; Dinacci, D.; Petrillo, C.; Rossi, P.; Conti, F.M.; Gassert, R. Neurocognitive robot-assisted rehabilitation of hand function: A randomized control trial on motor recovery in subacute stroke. J. Neuroeng. Rehabil. 2020, 17, 115. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Schlaug, G. Resting State Interhemispheric Motor Connectivity and White Matter Integrity Correlate with Motor Impairment in Chronic Stroke. Front. Neurol. 2013, 4, 178. [Google Scholar] [CrossRef] [PubMed]
- Stefano, M.; Patrizia, P.; Mario, A.; Ferlini, G.; Rizzello, R.; Rosati, G. Robotic upper limb rehabilitation after acute stroke by NeReBot: Evaluation of treatment costs. BioMed Res. Int. 2014, 2014, 265634. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Total, N = 70 | Control, N = 23 | URT, N = 23 | BRT, N = 24 | p Value * |
|---|---|---|---|---|---|
| Sex, N (%) | 1 | ||||
| Male | 61 (87.1%) | 20 (87%) | 20(87%) | 21 (87.5%) | |
| Female | 9 (12.9%) | 3 (13%) | 3 (13%) | 3 (12.5%) | |
| Age, Mean (SD) | 58.2(9.1) | 58.9(10.3) | 56.7 (8.9) | 59.0 (8.3) | 0.6 |
| Stroke type, N (%) | 0.9 | ||||
| Ischemic | 56 (80%) | 18(78.3%) | 19 (82.6%) | 19 (79.2%) | |
| Hemorrhage | 14 (20%) | 5 (21.7%) | 4 (17.4%) | 5(20.8%) | |
| Stroke side, N (%) | 0.8 | ||||
| left | 40 (57.1%) | 12 (52.2%) | 14 (60.9%) | 14 (58.3%) | |
| right | 30 (42.9%) | 11 (47.8%) | 9(39.1%) | 10 (41.7%) | |
| Stroke weeks, Mean (SD) | 5.1 (4.5) | 5.0 (3.6) | 4.7(4.3) | 5.5(5.5) | 0.8 |
| Measurements | Baseline | Post Intervention | Between-Group Comparison | Treatment Effect | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD */ N (%) § | Mean ± SD */N (%) § | Adjusted Mean †/OR ‡ | 95% CI | F Value (df) | p Value | Adjusted Mean with 95% CI | |
| Primary Outcome | |||||||
| FMA–UE | |||||||
| Control | 18.57 ± 11.47 | 24.83 ± 15.10 | 24.79 | 22.23–27.35 | 4.328 (66) | 0.017 | 6.26 (3.70–8.82) |
| URT | 17.91 ± 11.56 | 25.30 ± 13.99 | 25.97 | 23.57–28.36 | 7.44 (5.04–9.83) | ||
| BRT | 19.08 ± 9.17 | 32.00 ± 11.44 | 31.40 | 27.74–35.07 | 12.88 (9.21–16.54) | ||
| Secondary Outcome | |||||||
| MBI Total Score | |||||||
| Control | 54.74 ± 13.44 | 63.13 ± 16.31 | 62.75 | 59.42–66.09 | 5.266 (66) | 0.008 | 8.48 (4.56–12.41) |
| URT | 53.52 ± 12.82 | 63.74 ± 11.54 | 64.34 | 61.01–67.68 | 10.07 (7.31–12.84) | ||
| BRT | 54.54 ± 11.67 | 70.17 ± 10.27 | 69.95 | 66.69–73.21 | 15.68 (12.55–18.80) | ||
| RMS_biceps brachii bundle | |||||||
| Control | 120.76 ± 81.50 | 157.86 ± 110.82 | 162.55 | 138.60–186.50 | 0.283 (64) | 0.755 | 36.99 (13.04–60.94) |
| URT | 128.30 ± 96.44 | 160.25 ± 95.57 | 157.57 | 129.82–185.33 | 32.01 (4.26–59.77) | ||
| BRT | 127.76 ± 76.76 | 174.72 ± 104.55 | 172.57 | 144.35–200.79 | 47.01 (18.79–75.23) | ||
| RMS_anterior deltoid bundle | |||||||
| Control | 148.47 ± 119.00 | 177.61 ± 131.79 | 170.77 | 148.97–192.58 | 5.664 (64) | 0.006 | 30.05 (8.25–51.86) |
| URT | 139.19 ± 114.10 | 177.70 ± 115.11 | 179.05 | 156.03–202.07 | 38.33 (15.31–61.35) | ||
| BRT | 134.63 ± 75.72 | 252.41 ± 116.69 | 257.79 | 211.45–304.12 | 117.07 (70.73–163.40) | ||
| RMS_middle deltoid | |||||||
| Control | 159.09 ± 103.13 | 206.04 ± 156.59 | 202.11 | 156.84–247.38 | 1.317 (64) | 0.275 | 47.42 (6.37–88.47) |
| URT | 134.80 ± 108.52 | 225.89 ± 163.69 | 243.63 | 196.02–291.25 | 88.94 (33.81–144.07) | ||
| BRT | 167.88 ± 113.33 | 261.69 ± 112.02 | 249.92 | 205.50–294.35 | 95.23 (49.71- 140.75) | ||
| RMS_triceps brachii bundle | |||||||
| Control | 73.40 ± 54.73 | 126.23 ± 100.02 | 135.55 | 107.21–163.88 | 0.458 (64) | 0.635 | 52.42 (18.58–86.26) |
| URT | 77.41 ± 63.15 | 114.25 ± 90.48 | 119.72 | 90.13–149.30 | 36.59 (8.74–64.45) | ||
| BRT | 97.44 ± 89.06 | 131.85 ± 95.84 | 118.14 | 90.29–146.00 | 35.02 (10.98–59.06) | ||
| iEMG_biceps brachii bundle | |||||||
| Control | 93.87 ± 64.75 | 122.05 ± 87.77 | 125.06 | 105.61–144.51 | 0.148 (64) | 0.863 | 28.13 (8.68–47.58) |
| URT | 100.15 ± 74.21 | 125.24 ± 74.96 | 122.08 | 99.50–144.67 | 25.15 (2.57–47.73) | ||
| BRT | 97.06 ± 61.55 | 131.62 ± 90.08 | 131.49 | 105.96–157.02 | 34.56 (9.02–60.09) | ||
| iEMG_anterior deltoid bundle | |||||||
| Control | 118.28 ± 95.42 | 138.37 ± 101.79 | 132.09 | 114.51–149.68 | 6.812 (64) | 0.002 | 21.69 (4.10–39.27) |
| URT | 109.22 ± 90.30 | 129.43 ± 67.98 | 130.38 | 107.50–153.26 | 19.97 (−2.91–42.86) | ||
| BRT | 103.90 ± 56.95 | 196.83 ± 96.77 | 202.01 | 167.09–236.94 | 91.61 (56.68–126.53) | ||
| iEMG_middle deltoid | |||||||
| Control | 127.10 ± 88.57 | 161.80 ± 125.66 | 157.49 | 117.63–197.35 | 1.865 (64) | 0.163 | 36.79 (−2.98–76.56) |
| URT | 102.84 ± 78.95 | 156.02 ± 80.47 | 168.03 | 126.07–210.00 | 47.34 (22.54–72.13) | ||
| BRT | 130.19 ± 89.27 | 214.99 ± 118.95 | 208.60 | 169.53–247.67 | 87.90 (40.29–135.52) | ||
| iEMG_triceps brachii bundle | |||||||
| Control | 52.24 ± 40.46 | 93.25 ± 76.31 | 97.71 | 70.05–125.37 | 0.104 (64) | 0.901 | 38.06 (6.65–69.48) |
| URT | 53.45 ± 44.97 | 85.87 ± 67.30 | 89.60 | 60.70–118.51 | 29.96 (3.72–56.19) | ||
| BRT | 72.17 ± 64.3 | 97.79 ± 73.30 | 90.25 | 62.98–117.52 | 30.60 (7.39–53.82) | ||
| MEP (response) | |||||||
| Control | 8 (34.8%) | 11 (47.8.0%) | Reference | ||||
| URT | 7 (30.4%) | 11 (47.8.0%) | 1.82 | 0.29–15.25 | 0.54 | ||
| BRT | 6 (25.0%) | 15 (62.5%) | 5 | 0.93–39.81 | 0.08 | ||
| Measurement | ITT Based Primary Analysis (NControl = 24, NURT = 23, NBRT = 24) | PP Based Analysis * (NControl = 23, NURT = 20, NBRT = 24) | ITT, MI with Chained Equations § (NControl = 24, NURT = 23, NBRT = 24) | |||
|---|---|---|---|---|---|---|
| Estimates of Treatment Effects (95%CI)/OR (95%CI) | p Value | Estimates of Treatment Effects (95%CI)/OR (95%CI) | p Value | Estimates of Treatment Effects (95%CI)/OR (95%CI) | p Value | |
| Primary Outcome | ||||||
| FMA–UE | ||||||
| Control | 6.26 (3.70–8.82) | 0.017 | 6.53 (3.89–9.17) | 0.022 | - | - |
| URT | 7.44 (5.04–9.83) | 7.38 (4.68–10.09) | - | |||
| BRT | 12.88 (9.21–16.54) | 12.90 (9.25–16.56) | - | |||
| Secondary Outcomes | ||||||
| MBI | ||||||
| Control | 8.48 (4.56–12.41) | 0.008 | 8.97 (4.93–13.01) | 0.014 | - | - |
| URT | 10.07 (7.31–12.84) | 10.07 (7.01–13.12) | - | |||
| BRT | 15.68 (12.55–18.80) | 15.68 (12.56–18.79) | - | |||
| RMS_biceps brachii bundle | ||||||
| Control | 36.99 (13.04–60.94) | 0.755 | 40.12 (16.34–63.91) | 0.824 | 36.96 (12.96–60.96) | 0.491 |
| URT | 32.01 (4.26–59.77) | 34.01 (4.97–63.04) | 29.60 (4.08–55.13) | |||
| BRT | 47.01 (18.79–75.23) | 47.00 (18.75–75.26) | 47.01 (18.80–75.22) | |||
| RMS_anterior deltoid bundle | ||||||
| Control | 30.05 (8.25–51.86) | 0.006 | 30.69 (7.92–53.46) | 0.006 | 30.15 (8.36–51.94) | 0.001 |
| URT | 38.33 (15.31–61.35) | 39.60 (15.62–63.58) | 41.53 (20.10–62.97) | |||
| BRT | 117.07 (70.73–163.40) | 116.66 (70.45–162.87) | 117.14 (70.82–163.45) | |||
| RMS_middle deltoid | ||||||
| Control | 47.42 (6.37–88.47) | 0.275 | 50.24 (7.76–92.72) | 0.358 | 47.61 (6.68–88.55) | 0.205 |
| URT | 88.94 (33.81–144.07) | 86.04 (28.50–143.58) | 90.55 (39.38–141.71) | |||
| BRT | 95.23 (49.71–140.75) | 95.04 (49.58–140.50) | 95.44 (49.99–140.90) | |||
| RMS_triceps brachii bundle | ||||||
| Control | 52.42 (18.58–86.26) | 0.635 | 54.89 (20.00–89.77) | 0.505 | 52.31 (18.44–86.19) | 0.493 |
| URT | 36.59 (8.74–64.45) | 33.00 (4.71–61.29) | 35.31 (10.14–60.48) | |||
| BRT | 35.02 (10.98–59.06) | 34.91 (10.83–58.99) | 34.94 (10.91–58.97) | |||
| iEMG_biceps brachii bundle | ||||||
| Control | 28.13 (8.68–47.58) | 0.863 | 30.54 (11.15–49.92) | 0.915 | 28.10 (8.60–47.61) | 0.545 |
| URT | 25.15 (2.57–47.73) | 26.99 (3.39–50.60) | 23.51 (2.83–44.20) | |||
| BRT | 34.56 (9.02–60.09) | 34.56 (8.99–60.12) | 34.55 (9.03–60.07) | |||
| iEMG_anterior deltoid bundle | ||||||
| Control | 21.69 (4.10–39.27) | 0.002 | 22.31 (3.92–40.70) | 0.003 | 21.15 (4.07–38.23) | 0.000 |
| URT | 19.97 (−2.91–42.86) | 20.43 (−3.35–44.21) | 23.43 (1.23–45.63) | |||
| BRT | 91.61 (56.68–126.53) | 91.07 (56.10–126.03) | 91.58 (56.69–126.48) | |||
| iEMG_middle deltoid | ||||||
| Control | 36.79 (−2.98–76.56) | 0.163 | 39.40 (6.43–72.36) | 0.398 | 37.10 (5.37–68.84) | 0.306 |
| URT | 47.34 (22.54–72.13) | 68.77 (25.29–112.25) | 73.46 (35.29–111.63) | |||
| BRT | 87.90 (40.29–135.52) | 69.60 (35.64–103.56) | 69.65 (35.61–103.69) | |||
| iEMG_triceps brachii bundle | ||||||
| Control | 38.06 (6.65–69.48) | 0.901 | 41.60 (18.52–64.69) | 0.499 | 39.62 (17.32–61.92) | 0.636 |
| URT | 29.96 (3.72–56.19) | 26.16 (5.56–46.76) | 28.90 (9.89–47.92) | |||
| BRT | 30.60 (7.39–53.82) | 27.13 (8.79–45.46) | 27.00 (8.83–45.17) | |||
| MEP (response) | ||||||
| Control | Reference | Reference | Reference | |||
| URT | 0.29–15.25 | 0.54 | 1.10 (0.17–7.20) | 0.9 | 1.82 (0.36–10.62) | 0.48 |
| BRT | 0.93–39.81 | 0.08 | 3.67 (0.81–20.50) | 0.1 | 4.00 (0.90–22.21) | 0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, R.; Qiao, X.; Tang, C.; Zhou, T.; Chen, W.; Song, R.; Jiang, Y.; Reinhardt, J.D.; Wang, H. Effects of Uni- vs. Bilateral Upper Limb Robot-Assisted Rehabilitation on Motor Function, Activities of Daily Living, and Electromyography in Hemiplegic Stroke: A Single-Blinded Three-Arm Randomized Controlled Trial. J. Clin. Med. 2023, 12, 2950. https://doi.org/10.3390/jcm12082950
Yuan R, Qiao X, Tang C, Zhou T, Chen W, Song R, Jiang Y, Reinhardt JD, Wang H. Effects of Uni- vs. Bilateral Upper Limb Robot-Assisted Rehabilitation on Motor Function, Activities of Daily Living, and Electromyography in Hemiplegic Stroke: A Single-Blinded Three-Arm Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(8):2950. https://doi.org/10.3390/jcm12082950
Chicago/Turabian StyleYuan, Runping, Xu Qiao, Congzhi Tang, Ting Zhou, Wenli Chen, Ruyan Song, Yong Jiang, Jan D. Reinhardt, and Hongxing Wang. 2023. "Effects of Uni- vs. Bilateral Upper Limb Robot-Assisted Rehabilitation on Motor Function, Activities of Daily Living, and Electromyography in Hemiplegic Stroke: A Single-Blinded Three-Arm Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 8: 2950. https://doi.org/10.3390/jcm12082950