

Decreased Interoceptive Awareness as a Risk Factor for Moderate to Severe Pain in Japanese Full-Time Workers: A Longitudinal Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Methods
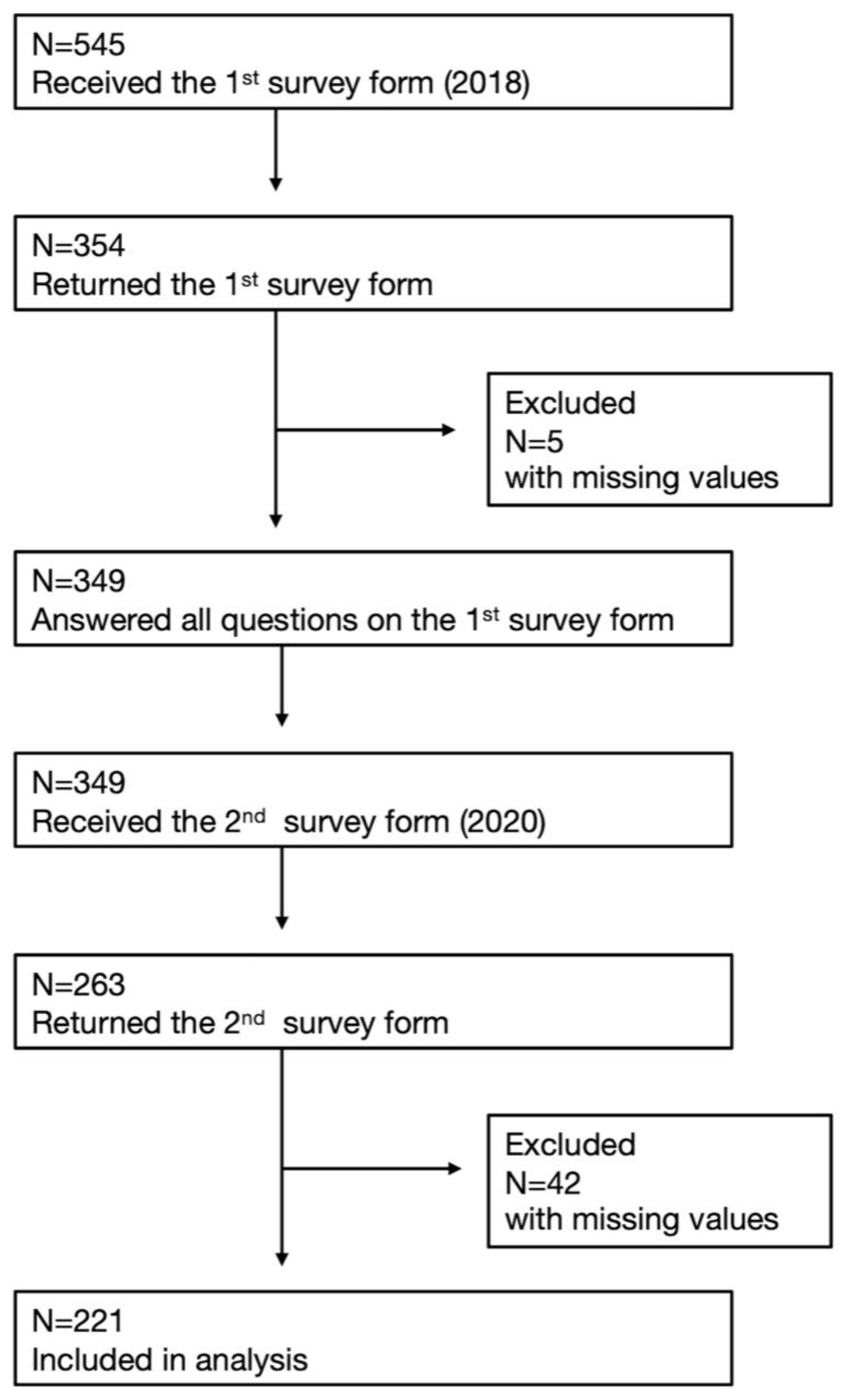
2.1. Participants
2.2. Measurements
2.2.1. Pain Intensity
2.2.2. Interoceptive Awareness
2.2.3. Psychological Distress
2.2.4. Fear of Movement
2.2.5. Work Stress
2.2.6. Home Stress
2.2.7. Demographic and Lifestyle Related Measures
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Association of Emotional Stability and the Onset of Pain
4.2. Prevention of Pain Chronicity
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministry of Health Labor and Welfare. Summary Report of Comprehensive Survey of Living Conditions 2019. Available online: https://www.mhlw.go.jp/english/database/db-hss/cslc-report2019.html (accessed on 19 November 2022).
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Rayner, L.; Hotopf, M.; Petkova, H.; Matcham, F.; Simpson, A.; McCracken, L.M. Depression in patients with chronic pain attending a specialised pain treatment centre: Prevalence and impact on health care costs. Pain 2016, 157, 1472–1479. [Google Scholar] [CrossRef]
- Rogers, A.H.; Farris, S.G. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur. J. Pain 2022, 26, 1611–1635. [Google Scholar] [CrossRef]
- Phillips, C.J. The Cost and Burden of Chronic Pain. Rev. Pain 2009, 3, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Kobayashi, F.; Nishihara, M.; Arai, Y.C.; Ikemoto, T.; Kawai, T.; Inoue, M.; Hasegawa, T.; Ushida, T. Chronic Pain in the Japanese Community--Prevalence, Characteristics and Impact on Quality of Life. PLoS ONE 2015, 10, e0129262. [Google Scholar] [CrossRef]
- Tanaka, C.; Wakaizumi, K.; Takaoka, S.; Matsudaira, K.; Mimura, M.; Fujisawa, D.; Kosugi, S. A Cross-Sectional Study of the Impact of Pain Severity on Absenteeism and Presenteeism Among Japanese Full-Time Workers. Pain Ther. 2022, 11, 1179–1193. [Google Scholar] [CrossRef]
- Stevans, J.M.; Delitto, A.; Khoja, S.S.; Patterson, C.G.; Smith, C.N.; Schneider, M.J.; Freburger, J.K.; Greco, C.M.; Freel, J.A.; Sowa, G.A.; et al. Risk Factors Associated with Transition from Acute to Chronic Low Back Pain in US Patients Seeking Primary Care. JAMA Netw. Open 2021, 4, e2037371. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Meints, S.M.; Edwards, R.R. Evaluating psychosocial contributions to chronic pain outcomes. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 87, 168–182. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef]
- Fischer, J.M.; Kandil, F.I.; Kessler, C.S.; Nayeri, L.; Zager, L.S.; Rocabado Hennhöfer, T.; Steckhan, N.; Koppold-Liebscher, D.A.; Bringmann, H.C.; Schäfer, T.; et al. Stress Reduction by Yoga versus Mindfulness Training in Adults Suffering from Distress: A Three-Armed Randomized Controlled Trial including Qualitative Interviews (RELAX Study). J. Clin. Med. 2022, 11, 5680. [Google Scholar] [CrossRef]
- Mehling, W.E.; Daubenmier, J.; Price, C.J.; Acree, M.; Bartmess, E.; Stewart, A.L. Self-reported interoceptive awareness in primary care patients with past or current low back pain. J. Pain Res. 2013, 6, 403–418. [Google Scholar] [CrossRef]
- Turk, D.C.; Dworkin, R.H.; Allen, R.R.; Bellamy, N.; Brandenburg, N.; Carr, D.B.; Cleeland, C.; Dionne, R.; Farrar, J.T.; Galer, B.S.; et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003, 106, 337–345. [Google Scholar] [CrossRef]
- Shoji, M.; Mehling, W.E.; Hautzinger, M.; Herbert, B.M. Investigating multidimensional interoceptive awareness in a Japanese population: Validation of the Japanese MAIA-J. Front. Psychol. 2018, 9, 1855. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Kikuchi, N.; Matsudaira, K.; Sawada, T.; Oka, H. Psychometric properties of the Japanese version of the Tampa Scale for Kinesiophobia (TSK-J) in patients with whiplash neck injury pain and/or low back pain. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2015, 20, 985–992. [Google Scholar] [CrossRef]
- Matsudaira, K.; Inuzuka, K.; Kikuchi, N.; Sakae, C.; Arisaka, M.; Isomura, T.; Miller, R.P. Development of a Japanese Version of the Tampa Scale for Kinesiophobia (TSK-J): Translation and Linguistic Validation. Seikei Geka (Orthop. Surg.) 2013, 48, 13–19. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef]
- Furda, J. Werk, Persoon en Welzijn: Een Toets van het JD-C Model [Work, Personality, and Well-Being: A Test of the JD-C Model]. Ph.D. Thesis, Utrecht University, Utrecht, The Netherlands, 1995. [Google Scholar]
- van Veldhoven, M.; Broersen, S. Measurement quality and validity of the “need for recovery scale”. Occup. Environ. Med. 2003, 60 (Suppl. 1), i3–i9. [Google Scholar] [CrossRef] [PubMed]
- Shimomitsu, T. The final development of the Brief Job Stress Questionnaire mainly used for assessment of the individuals. In Ministry of Labour Sponsored Grant for the Prevention of Work-Related Illness: The 1999 Report; Tokyo Medical University: Tokyo, Japan, 2000; pp. 126–164. [Google Scholar]
- Peeters, M.C.W.; Montgomery, A.; Schaufeli, W. Balancing Work and Home: How Job and Home Demands Are Related to Burnout. Int. J. Stress Manag. 2005, 12, 43. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Hülsebusch, J.; Hasenbring, M.I.; Rusu, A.C. Understanding Pain and Depression in Back Pain: The Role of Catastrophizing, Help-/Hopelessness, and Thought Suppression as Potential Mediators. Int. J. Behav. Med. 2016, 23, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Petrini, L.; Arendt-Nielsen, L. Understanding Pain Catastrophizing: Putting Pieces Together. Front. Psychol 2020, 11, 603420. [Google Scholar] [CrossRef]
- Shires, A.; Sharpe, L.; Davies, J.N.; Newton-John, T.R.O. The efficacy of mindfulness-based interventions in acute pain: A systematic review and meta-analysis. Pain 2020, 161, 1698–1707. [Google Scholar] [CrossRef]
- Veehof, M.M.; Oskam, M.-J.; Schreurs, K.M.G.; Bohlmeijer, E.T. Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain 2011, 152, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Worthen, M.; Cash, E. Stress Management. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513300/ (accessed on 19 November 2022).
- Goilean, C.; Gracia, F.J.; Tomás, I. Clarifying the relationship between trait mindfulness and objective performance. Curr. Psychol. 2021. [Google Scholar] [CrossRef]
- McCracken, L.M.; Gauntlett-Gilbert, J.; Vowles, K.E. The role of mindfulness in a contextual cognitive-behavioral analysis of chronic pain-related suffering and disability. Pain 2007, 131, 63–69. [Google Scholar] [CrossRef]
- Kosugi, T.; Ninomiya, A.; Nagaoka, M.; Hashimoto, Z.; Sawada, K.; Park, S.; Fujisawa, D.; Mimura, M.; Sado, M. Effectiveness of Mindfulness-Based Cognitive Therapy for Improving Subjective and Eudaimonic Well-Being in Healthy Individuals: A Randomized Controlled Trial. Front. Psychol. 2021, 12, 700916. [Google Scholar] [CrossRef]
- Jinich-Diamant, A.; Garland, E.; Baumgartner, J.; Gonzalez, N.; Riegner, G.; Birenbaum, J.; Case, L.; Zeidan, F. Neurophysiological Mechanisms Supporting Mindfulness Meditation-Based Pain Relief: An Updated Review. Curr. Pain Headache Rep. 2020, 24, 56. [Google Scholar] [CrossRef]
- Marchand, W.R. Neural mechanisms of mindfulness and meditation: Evidence from neuroimaging studies. World J. Radiol. 2014, 6, 471. [Google Scholar] [CrossRef]
- Quentin, C.; Bagheri, R.; Ugbolue, U.C.; Coudeyre, E.; Pélissier, C.; Descatha, A.; Menini, T.; Bouillon-Minois, J.B.; Dutheil, F. Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8430. [Google Scholar] [CrossRef]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; van Tulder, M.W. Exercise therapy for chronic low back pain. Cochrane Database Syst. Rev. 2021, 9, Cd009790. [Google Scholar] [CrossRef]
- Steiger, F.; Wirth, B.; de Bruin, E.D.; Mannion, A.F. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur. Spine J. 2012, 21, 575–598. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Frey-Law, L.; Hoeger Bement, M. Exercise-induced pain and analgesia? Underlying mechanisms and clinical translation. Pain 2018, 159 (Suppl. 1), S91–S97. [Google Scholar] [CrossRef]
- Shinohara, Y.; Wakaizumi, K.; Ishikawa, A.; Ito, M.; Hoshino, R.; Tanaka, C.; Takaoka, S.; Kawakami, M.; Tsuji, O.; Fujisawa, D.; et al. Improvement in Disability Mediates the Effect of Self-Efficacy on Pain Relief in Chronic Low Back Pain Patients with Exercise Therapy. Pain Res. Manag. 2022, 2022, 4203138. [Google Scholar] [CrossRef] [PubMed]
- Kernan, T.; Rainville, J. Observed outcomes associated with a quota-based exercise approach on measures of kinesiophobia in patients with chronic low back pain. J. Orthop. Sport. Phys. Ther. 2007, 37, 679–687. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pain Intensity in 2020 | Slight or No Pain | Moderate to Severe Pain | t or Z | p | |||
|---|---|---|---|---|---|---|---|
| N | 107 | 114 | |||||
| Age (years), mean (SEM) | 40.87 | (1.07) | 41.8 | (1.03) | 0.64 | 0.521 | |
| Male, n (%) | 95 | (88.79) | 90 | (78.95) | 3.99 | 0.046 | * |
| BMI (kg/m2), mean (SEM) | 23.12 | (0.31) | 23.1 | (0.30) | 0.00 | 0.999 | |
| Low education, n (%) | 28 | (26.17) | 27 | (23.68) | 2.34 | 0.673 | |
| Short sleep (< 6 h/day), n (%) | 73 | (68.22) | 78 | (68.42) | 0.00 | 0.975 | |
| Work stress, mean (SEM) | 30.59 | (0.82) | 32.3 | (0.79) | 1.53 | 0.128 | |
| Home stress, mean (SEM) | 22.54 | (0.46) | 23.2 | (0.45) | 1.06 | 0.292 | |
| TSK, mean (SEM) | 22.92 | (0.46) | 23.3 | (0.45) | 0.57 | 0.572 | |
| Psychological distress (K6 ≥ 13), n (%) | 11 | (10.28) | 11 | (9.65) | 0.03 | 0.876 | |
| MAIA, mean (SEM) | |||||||
| Not distracting | 3.25 | (0.12) | 2.8 | (0.12) | −2.90 | 0.004 | ** |
| Not worrying | 3.00 | (0.09) | 2.7 | (0.09) | −2.05 | 0.042 | * |
| Attention regulation | 2.99 | (0.09) | 2.8 | (0.09) | −1.14 | 0.255 | |
| Self-regulation | 2.92 | (0.10) | 2.8 | (0.09) | −1.14 | 0.254 | |
| Trusting | 2.92 | (0.10) | 2.8 | (0.10) | −1.12 | 0.265 | |
| No exercise habit, n (%) | 28 | (26.17) | 43 | (32.13) | 3.40 | 0.065 | |
| Odds Ratio | 95% CI (LL, UL) | p | ||
|---|---|---|---|---|
| Age | 1.028 | (0.999, 1.057) | 0.053 | |
| Male | 0.368 | (0.154, 0.881) | 0.025 | * |
| Work stress | 1.025 | (0.988, 1.064) | 0.190 | |
| Home stress | 0.992 | (0.933, 1.055) | 0.804 | |
| TSK | 0.984 | (0.923, 1.049) | 0.620 | |
| Psychological distress | 0.453 | (0.163, 1.256) | 0.128 | |
| Emotional stability | 0.640 | (0.463, 0.887) | 0.006 | ** |
| Self-control | 0.853 | (0.612, 1.188) | 0.345 | |
| No exercise habit | 1.719 | (0.924, 3.198) | 0.087 |
| Slight or No Pain in 2018 (N = 111) | Moderate to Severe Pain in 2018 (N = 110) | |||||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI (LL, UL) | p | Odds Ratio | 95% CI (LL, UL) | p | |||
| Age | 1.052 | (1.003, 1.102) | 0.030 | * | 1.016 | (0.974, 1.059) | 0.467 | |
| Male | 0.346 | (0.066, 1.809) | 0.209 | 0.441 | (0.129, 1.511) | 0.193 | ||
| Work stress | 1.033 | (0.980, 1.088) | 0.229 | 1.039 | (0.973, 1.109) | 0.242 | ||
| Home stress | 0.917 | (0.829, 1.015) | 0.094 | 1.035 | (0.944, 1.135) | 0.464 | ||
| TSK | 0.917 | (0.820, 1.025) | 0.123 | 0.966 | (0.879, 1.062) | 0.475 | ||
| Psychological distress | 0.449 | (0.108, 1.858) | 0.269 | 0.657 | (0.098, 4.410) | 0.665 | ||
| Emotional stability | 0.406 | (0.236, 0.699) | 0.001 | *** | 1.046 | (0.606, 1.803) | 0.872 | |
| Self-control | 0.790 | (0.473, 1.319) | 0.365 | 1.094 | (0.633, 1.891) | 0.747 | ||
| No exercise habit | 0.974 | (0.359, 2.643) | 0.959 | 3.956 | (1.391, 11.255) | 0.010 | ** | |
| 2018 | 2020 | No Exercise Habit | Time | No Exerice Habit × Time | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (SEM) | Mean | (SEM) | F | p | F | p | F | p | ||||
| TSK | 23.99 | (0.48) | 22.85 | (0.58) | 7.715 | 0.007 | ** | 4.737 | 0.032 | * | 5.131 | 0.026 | * |
| Work stress | 31.89 | (0.80) | 31.12 | (0.82) | 0.199 | 0.656 | 0.138 | 0.711 | 0.220 | 0.640 | |||
| Home stress | 23.35 | (0.49) | 23.80 | (0.47) | 0.030 | 0.863 | 0.549 | 0.460 | 0.001 | 0.980 | |||
| MAIA | |||||||||||||
| Attention regulation | 2.88 | (0.09) | 2.89 | (0.10) | 0.015 | 0.904 | 0.076 | 0.784 | 0.038 | 0.846 | |||
| Self-regulation | 2.81 | (0.09) | 2.82 | (0.10) | 3.735 | 0.056 | 0.025 | 0.876 | 0.014 | 0.906 | |||
| Trusting | 2.75 | (0.10) | 2.77 | (0.10) | 4.303 | 0.041 | * | 0.233 | 0.630 | 0.155 | 0.694 | ||
| Not distracting | 2.84 | (0.11) | 2.98 | (0.12) | 0.850 | 0.359 | 0.160 | 0.690 | 1.688 | 0.197 | |||
| Not worrying | 2.78 | (0.09) | 2.68 | (0.09) | 0.751 | 0.388 | 0.277 | 0.600 | 0.278 | 0.599 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takaoka, S.; Wakaizumi, K.; Tanaka, C.; Tanaka, S.; Kawate, M.; Hoshino, R.; Matsudaira, K.; Fujisawa, D.; Morisaki, H.; Kosugi, S. Decreased Interoceptive Awareness as a Risk Factor for Moderate to Severe Pain in Japanese Full-Time Workers: A Longitudinal Cohort Study. J. Clin. Med. 2023, 12, 2896. https://doi.org/10.3390/jcm12082896
Takaoka S, Wakaizumi K, Tanaka C, Tanaka S, Kawate M, Hoshino R, Matsudaira K, Fujisawa D, Morisaki H, Kosugi S. Decreased Interoceptive Awareness as a Risk Factor for Moderate to Severe Pain in Japanese Full-Time Workers: A Longitudinal Cohort Study. Journal of Clinical Medicine. 2023; 12(8):2896. https://doi.org/10.3390/jcm12082896
Chicago/Turabian StyleTakaoka, Saki, Kenta Wakaizumi, Chisato Tanaka, Shintaro Tanaka, Morihiko Kawate, Reiko Hoshino, Ko Matsudaira, Daisuke Fujisawa, Hiroshi Morisaki, and Shizuko Kosugi. 2023. "Decreased Interoceptive Awareness as a Risk Factor for Moderate to Severe Pain in Japanese Full-Time Workers: A Longitudinal Cohort Study" Journal of Clinical Medicine 12, no. 8: 2896. https://doi.org/10.3390/jcm12082896