
Evaluation of the Prevalence of Refractive Defects and Ocular Function in a Group of 1518 Children Aged 8 Years in Northwestern Poland—A Retrospective Study

Abstract
:1. Introduction
2. Definitions
3. Materials and Methods
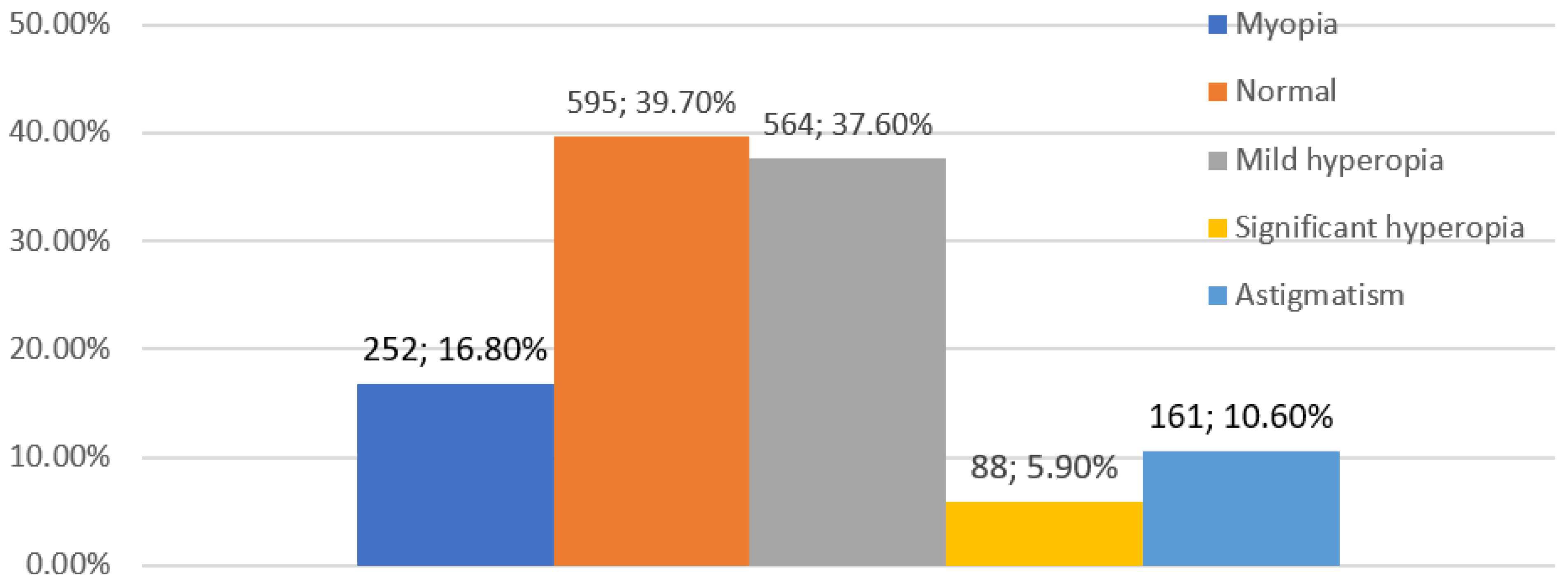
4. Results
5. Discussion

{kind=link}
{kind=link}
{kind=link}
| Author | Country and Year | Age Range in Years | Average Age | Size of Study Population | Cycloplegia | Refractive Error and Its Prevalence in Population |
|---|---|---|---|---|---|---|
| Popović-Beganović [53] | Bosnia and Herzegovina 2017 | 7–16 | 997 | YES | Myopia 20.4% Hyperopia 3.3% Astigmatism 18.1% | |
| Harrington SC [54] | Ireland 2016–2018 | Two groups 6–7 12–13 | 1626 | YES | Age group 6–7 years Myopia 3.3% Hyperopia 25% Astigmatism 19.2% Age group 12–13 years Myopia 19.9% Hyperopia 8.9% Astigmatism 15.9% | |
| O’DomoghueL [55] | Northern Ireland 2006–2008 | Two groups 6–7 12–13 | 392 (age group 6–7 years) 661 (age group 12–13 years) | YES | Age group 6–7 years Myopia 2.8% Hyperopia 26% Age group 12–13 years Myopia 17.7% Hyperopia 14.7% | |
| Falkenberg [38] | Norway 2003–2013 | 7–15 | 1126 | NO | Emmetropia 32% Hyperopia 51% Myopia 17% | |
| Szaflik et al. [29] | Poland 2002–2003 | 6–16 | 10 | 10,021 | YES | Emmetropia 33.77% Hyperopia 19.91% Myopia 16.94% Astigmatism 5.57% Complex vision errors 24.05% |
| Villarreal MG [56] | Sweden 2000 | 12–13 | 1045 | YES | Myopia 39% Hyperopia 8.4% Astigmatism 5.2% |
| Author | Country and Year | Age Range in Years | Average Age | Size of Study Population | Cycloplegia | Refractive Error and Its Prevalence in Population |
|---|---|---|---|---|---|---|
| Morgan [30] | Nepal, India, Chile, South Africa 2005 | 5–15 | 38,811 | YES | Myopia < 20% Emmetropia 20–47.2% Hyperopia 15–73% | |
| RobaeiD [57] | Australia 2003–2004 | 5.5–8.4 | 6.7 | 1740 | YES | Myopia 1.6% Hyperopia 13.2% Astigmatism 7.6% Normovision 80% |
| Ojaimi [58] | Australia 2005 | 6–7 | 1724 | YES | Emmetropia 7.57% Hyperopia 91% Myopia 1.43% | |
| Lira [59] | Brazil 2012 | 6–17 | 778 | YES | Emmetropia 15.9% Hyperopia 74.6% Myopia 9.6% | |
| MaulE [2] | Chile 2000 | 5–15 | 6998 | YES | Myopia 7.3% Hyperopia 19.3% Astigmatism 27% | |
| Li H, Li S, Liu L [60] | China 2014 | 12.9–17.6 | 14.7 | 1839 | YES | Hyperopia 7.5% Myopia 82.7% Emmetropia 9.8% |
| Ma Y [61] | China 2016 | 3–10 | 8398 | YES | Hyperopia 17.8% Myopia 20.1% | |
| DandonaR [62] | India 2002 | <15 | 11 786 | YES | Hyperopia 62.62% Myopia 3.19% | |
| GursoyH [63] | Iran 2011 | 7–8 | 709 | YES | Myopia 22.6% Hyperopia 10.6% Astigmatism 11.0% | |
| HashemiH [64] | Iran 2013 | 7 | 4072 | YES | Myopia 3.04% Hyperopia 6.20% Astigmatism 17.43% | |
| Yingyong [65] | Thailand 2008–2009 | 6–12 | 1100 | YES | Myopia 11.1% Hyperopia 1.4% Astigmatism 0.3% | |
| CacaI [66] | Turkey | 6–14 | 10.56 ± 3.59 | 21.062 | YES | Myopia 3.2% Hyperopia 5.9% Astigmatism 14.3% |
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maul, E.; Barroso, S.; Munoz, S.R.; Sperduto, R.D.; Ellwein, L.B. Refractive error study in children: Results from La Florida, Chile. Am. J. Ophthalmol. 2000, 129, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Pan, X.; Sui, R.; Munoz, S.R.; Sperduto, R.D.; Ellwein, L.B. Refractive error study in children: Results from Shunyi District, China. Am. J. Ophthalmol. 2000, 129, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Harvey, E.M.; Dobson, V.; Miller, J.M. Prevalence of High Astigmatism, Eyeglass Wear, and Poor Visual Acuity among Native American Grade School Children. Optom Vis. Sci. 2006, 83, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmetz, J.D.; Bourne, R.R.A.; Briant, P.S.; Flaxman, S.R.; Taylor, H.R.B.; Jonas, J.B. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health. 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Borsting, E.; Rouse, M.W. Detecting learning-related visual problems in the primary care setting. J. Am. Optom. Assoc. 1994, 65, 642–650. [Google Scholar]
- Rose, K.; Younan, C.; Morgan, I.; Mitchell, P. Prevalence of undetected ocular conditions in a pilot sample of school children. Clin. Exp. Ophthalmol. 2003, 31, 237–240. [Google Scholar] [CrossRef]
- Hopkins, S.; Narayanasamy, S.; Vincent, S.J.; Sampson, G.P.; Wood, J.M. Do reduced visual acuity and refractive error affect classroom performance? Clin. Exp. Optom. 2020, 103, 278–289. [Google Scholar] [CrossRef]
- Tongue, A.C. Refractive Errors in Children. Pediatr. Clin. N. Am. 1987, 34, 1425–1437. [Google Scholar] [CrossRef]
- Matsumura, H.; Hirai, H. Prevalence of Myopia and Refractive Changes in Students from 3 to 17 Years of Age. Surv. Ophthalmol. 1999, 44, S109–S115. [Google Scholar] [CrossRef]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K. IMI–Defin. Cl. Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Opthalmol. Vis. Sci. 2019, 60, M20. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.; Dahlmann-Noor, A. Myopia and its progression in children in London, UK: A retrospective evaluation. J. Optom. 2020, 13, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P. Global Prevalence of Myopia and High. Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, A.K.; Ahluwalia, B.K.; Rajan, C. Status of cyclopentolate as a cycloplegic in children: A comparison with atropine and homatropine. Acta Ophthalmol. 2009, 66, 721–724. [Google Scholar] [CrossRef]
- Mutti, D.O.; Zadnik, K.; Egashira, S.; Kish, L.; Twelker, J.D.; Adams, A.J. The effect of cycloplegia on measurement of the ocular components. Investig. Ophthalmol. Vis. Sci. 1994, 35, 515–527. [Google Scholar]
- Khalid, K.; Padda, J.; Pokhriyal, S.; Hitawala, G.; Khan, M.S.; Upadhyay, P. Pseudomyopia and Its Association with Anxiety. Cureus [Internet]. 2021. Available online: https://www.cureus.com/articles/68472-pseudomyopia-and-its-association-with-anxiety (accessed on 1 January 2020).
- Duke-Elder, S. The Practice of Refraction, 8th ed.; Churchill: London, UK, 1969; p. 329 s. [Google Scholar]
- Diniz, D.; Irochima, F.; Schor, P. Ophthalmology W: Optics of the Human Eye; 2000; pp. 26–37. [Google Scholar]
- Giordano, L.; Friedman, D.S.; Repka, M.X.; Katz, J.; Ibironke, J.; Hawes, P. Prevalence of Refractive Error among Preschool Children in an Urban Population: The Baltimore Pediatric Eye Disease Study. Ophthalmology 2009, 116, 739–746.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, B.L.; Roch-Levecq, A.C.; Klonoff-Cohen, H.S.; Brown, S.I. Refractive Errors in Low-Income Preschoolers. Ophthalmic Epidemiol. 2007, 14, 223–229. [Google Scholar] [CrossRef]
- Atkinson, J.; Braddick, O.; Nardini, M.; Anker, S. Infant Hyperopia: Detection, Distribution, Changes and Correlates—Outcomes From the Cambridge Infant Screening Programs. Optomtry Vis. Sci. 2007, 84, 84–96. [Google Scholar] [CrossRef] [Green Version]
- Chau, F.Y.; Wallace, D.; Vajaranant, T.; Herndon, L.; Lee, P.; Challa, P. Osteogenesis Imperfecta and the Eye. In W: Osteogenesis Imperfecta [Internet]; Elsevier: Amsterdam, The Netherlands, 2014; pp. 289–303. Available online: https://linkinghub.elsevier.com/retrieve/pii/B9780123971654000319 (accessed on 1 January 2020).
- Shih, Y.F.; Ho, T.C.; Chen, M.S.; Lin, L.L.K.; Wang, P.C.; Hou, P.K. Experimental myopia in chickens induced by corneal astigmatism. Acta Ophthalmol. 2009, 72, 597–601. [Google Scholar] [CrossRef]
- Alward, W.L.; Bender, T.R.; Demske, J.A.; Hall, D.B. High prevalence of myopia among young adult Yupik Eskimos. Can. J. Ophthalmol. 1985, 20, 241–245. [Google Scholar]
- Gwiazda, J.; Grice, K.; Held, R.; McLellan, J.; Thorn, F. Astigmatism and the development of myopia in children. Vis. Res. 2000, 40, 1019–1026. [Google Scholar] [CrossRef] [Green Version]
- Lansche, R.K. Asthenopia Caused by “Against-The-Rule” Astigmatism. Headache J. Head Face Pain 1966, 6, 147–151. [Google Scholar] [CrossRef]
- Dobson, V.; Harvey, E.M.; Clifford-Donaldson, C.E.; Green, T.K.; Miller, J.M. Amblyopia in Astigmatic Infants and Toddlers. Optom. Vis. Sci. 2010, 87, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazdani, N.; Sadeghi, R.; Momeni-Moghaddam, H.; Zarifmahmoudi, L.; Ehsaei, A. Comparison of cyclopentolate versus tropicamide cycloplegia: A systematic review and meta-analysis. J. Optom. 2018, 11, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Iribarren, R.; Fotouhi, A.; Grzybowski, A. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 2015, 93, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Szaflik, J.; Prost, M.; Zaleska-Zmijewska, A.; Hapunik, A.; Wójcik, A. The analysis of refractive error in children adolescents from 6-15 years of age based on 1000 examinations in two major Polish regions. Klin Ocz. 2004, 106 (Suppl. S3), 471–473. [Google Scholar]
- Morgan, I.G.; Rose, K.A.; Ellwein, L.B.; The Refractive Error Study in Children Survey Group. Is emmetropia the natural endpoint for human refractive development? An analysis of population-based data from the refractive error study in children (RESC). Acta Ophthalmol. 2010, 88, 877–884. [Google Scholar] [CrossRef]
- Hu, Y.; Zhao, F.; Ding, X.; Zhang, S.; Li, Z.; Guo, Y. Rates of Myopia Development in Young Chinese Schoolchildren during the Outbreak of COVID-19. JAMA Ophthalmol. 2021, 139, 1115. [Google Scholar] [CrossRef]
- Yolton, D.P.; Kandel, J.S.; Yolton, R.L. Diagnostic pharmaceutical agents: Side effects encountered in a study of 15,000 applications. J. Am. Optom. Assoc. 1980, 51, 113–118. [Google Scholar]
- Kempen, J.H.; Mitchell, P.; Lee, K.E.; Tielsch, J.M.; Broman, A.T.; Taylor, H.R.; Ikram, M.K.; Congdon, N.G.; O’Colmain, B.J.; Eye Diseases Prevalence Research Group. The Prevalence of Refractive Errors among Adults in the United States, Western Europe, and Australia. Arch. Ophthalmol. 2004, 122, 495. [Google Scholar]
- Mayer, D.L.; Hansen, R.M.; Moore, B.D.; Kim, S.; Fulton, A.B. Cycloplegic Refractions in Healthy Children Aged 1 through 48 Months. Arch. Ophthalmol. 2001, 119, 1625. [Google Scholar] [CrossRef]
- Mutti, D.O.; Mitchell, G.L.; Jones, L.A.; Friedman, N.E.; Frane, S.L.; Lin, W.K. Axial Growth and Changes in Lenticular and Corneal Power during Emmetropization in Infants. Investig. Opthalmol. Vis. Sci. 2005, 46, 3074. [Google Scholar] [CrossRef] [Green Version]
- Ostadimoghaddam, H.; Fotouhi, A.; Hashemi, H.; Yekta, A.; Heravian, J.; Rezvan, F. Prevalence of the refractive errors by age and gender: The Mashhad eye study of Iran: Refractive errors in Mashhad, Iran. Clin. Exp. Ophthalmol. 2011, 39, 743–751. [Google Scholar] [CrossRef]
- Lin, L.L.K.; Shih, Y.F.; Hsiao, C.K.; Chen, C.J. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann. Acad. Med. Singap. 2004, 33, 27–33. [Google Scholar] [PubMed]
- Falkenberg, H.K.; Langaas, T.; Svarverud, E. Vision status of children aged 7–15 years referred from school vision screening in Norway during 2003–2013: A retrospective study. BMC Ophthalmol. 2019, 19, 180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fotedar, R.; Rochtchina, E.; Morgan, I.; Wang, J.J.; Mitchell, P.; Rose, K.A. Necessity of Cycloplegia for Assessing Refractive Error in 12-Year-Old Children: A Population-Based Study. Am. J. Ophthalmol. 2007, 144, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Jones, R. Physiological Pseudomyopia. Optom. Vis. Sci. 1990, 67, 610–616. [Google Scholar] [CrossRef]
- Williams, O.A. Base in Prisms and Pseudo Myopia. Clin. Exp. Optom. 1956, 39, 260. [Google Scholar] [CrossRef]
- Rutstein, R.P.; Marsh-Tootle, W. Acquired Unilateral Visual Loss Attributed to an Accommodative Spasm. Optom Vis. Sci. 2001, 78, 492–495. [Google Scholar] [CrossRef]
- Stenson, S.M.; Raskind, R.H. Pseudomyopia: Etiology, Mechanisms and Therapy. J. Pediatr. Ophthalmol. Strabismus 1970, 7, 110–115. [Google Scholar] [CrossRef]
- Walker, J.P.S. Myopia And Pseudo-Myopia. Br. J. Ophthalmol. 1946, 30, 735–742. [Google Scholar] [CrossRef] [Green Version]
- Sankaridurg, P.; He, X.; Naduvilath, T.; Lv, M.; Ho, A.; Smith, E. Comparison of noncycloplegic and cycloplegic autorefraction in categorizing refractive error data in children. Acta Ophthalmol. 2017, 95, e633–e640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E. Low-Concentration Atropine for Myopia Progression (LAMP) Study. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Walline, J.J.; Walker, M.K.; Mutti, D.O.; Jones-Jordan, L.A.; Sinnott, L.T.; Giannoni, A.G. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020, 324, 571. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Cheung, S.W.; Shah, N.; Dakin, S.C.; Anderson, R.S. Retardation of Myopia in Orthokeratology (ROMIO) Study: A 2-Year Randomized Clinical Trial. Investig. Opthalmol. Vis. Sci. 2012, 53, 7077. [Google Scholar] [CrossRef] [PubMed]
- Fan, D.S.P.; Lam, D.S.C.; Lam, R.F.; Lau, J.T.F.; Chong, K.S.; Cheung, E.Y.Y. Prevalence, Incidence, and Progression of Myopia of School Children in Hong Kong. Investig. Opthalmol. Vis. Sci. 2004, 45, 1071. [Google Scholar] [CrossRef] [Green Version]
- Horwood, J.; Waylen, A.; Herrick, D.; Williams, C.; Wolke, D. Common Visual Defects and Peer Victimization in Children. Investig. Opthalmol. Vis. Sci. 2005, 46, 1177. [Google Scholar] [CrossRef]
- Dias, L.; Hyman, L.; Manny, R.E.; Fern, K. Evaluating the Self-esteem of Myopic Children over a Three-Year Period: The COMET Experience. Optom. Vis. Sci. 2005, 82, 338–347. [Google Scholar] [CrossRef]
- Terry, R.L.; Stockton, L.A. Eyeglasses and Children’s Schemata. J. Soc. Psychol. 1993, 133, 425–438. [Google Scholar] [CrossRef]
- Popović-Beganović, A.; Zvorničanin, J.; Vrbljanac, V.; Zvorničanin, E. The Prevalence of Refractive Errors and Visual Impairment among School Children in Brčko District, Bosnia and Herzegovina. Semin Ophthalmol. 2018, 33, 858–868. [Google Scholar] [CrossRef]
- Harrington, S.C.; Stack, J.; Saunders, K.; O’Dwyer, V. Refractive error and visual impairment in Ireland schoolchildren. Br. J. Ophthalmol. 2019, 103, 1112–1118. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, L.; McClelland, J.F.; Logan, N.S.; Rudnicka, A.R.; Owen, C.G.; Saunders, K.J. Refractive error and visual impairment in school children in Northern Ireland. Br. J. Ophthalmol. 2010, 94, 1155–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villarreal, M.G.; Ohlsson, J.; Abrahamsson, M.; Sjöström, A.; Sjöstrand, J. Myopisation: The refractive tendency in teenagers. Prevalence of myopia among young teenagers in Sweden. Acta Ophthalmol. Scand. 2000, 78, 177–181. [Google Scholar] [PubMed]
- Robaei, D.; Rose, K.; Kifley, A.; Mitchell, P. Patterns of spectacle use in young Australian school children: Findings from a population-based study. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2005, 9, 579–583. [Google Scholar] [CrossRef]
- Ojaimi, E.; Rose, K.A.; Smith, W.; Morgan, I.G.; Martin, F.J.; Mitchell, P. Methods for a Population-Based Study of Myopia and Other Eye Conditions in School Children: The Sydney Myopia Study. Ophthalmic Epidemiol. 2005, 12, 59–69. [Google Scholar] [CrossRef]
- Lira, R.P.C.; Arieta, C.E.L.; Passos, T.H.M.; Maziero, D.; Astur, G.L.; do Espírito Santo, Í.F. Distribution of Ocular Component Measures and Refraction in Brazilian School Children. Ophthalmic Epidemiol. 2017, 24, 29–35. [Google Scholar] [CrossRef]
- Li, H.; Li, S.; Liu, L.; Li, S.; Kang, M.; Ji, Y.; Meng, H.; Zhang, F.; Zhan, S.; Wang, N. Distribution of refraction and ocular biometric parameters in a population of junior middle school children in Anyang of Henan province. Zhonghua Yi Xue Za Zhi 2014, 94, 1284–1288. [Google Scholar] [PubMed]
- Ma, Y.; Qu, X.; Zhu, X.; Xu, X.; Zhu, J.; Sankaridurg, P.; Lin, S.; Lu, L.; Zhao, R.; Wang, L.; et al. Age-Specific Prevalence of Visual Impairment and Refractive Error in Children Aged 3–10 Years in Shanghai, China. Investig. Opthalmol. Vis. Sci. 2016, 57, 6188. [Google Scholar] [CrossRef] [Green Version]
- Dandona, R.; Dandona, L.; Srinivas, M.; Giridhar, P.; McCarty, C.A.; Rao, G.N. Population-based assessment of refractive error in India: The Andhra Pradesh eye disease study: Refractive error in India. Clin. Exp. Ophthalmol. 2002, 30, 84–93. [Google Scholar] [CrossRef]
- Gursoy, H.; Basmak, H.; Yaz, Y.; Colak, E. Vision Screening in Children Entering School: Eskisehir, Turkey. Ophthalmic Epidemiol. 2013, 20, 232–238. [Google Scholar] [CrossRef]
- Hashemi, H.; Yekta, A.; Jafarzadehpur, E.; Ostadimoghaddam, H.; Etemad, K.; Asharlous, A. High Prevalence of Refractive Errors in 7 Year Old Children in Iran. Iran. J. Public Health 2016, 45, 194–202. [Google Scholar]
- Yingyong, P. Refractive errors survey in primary school children (6–12 year old) in 2 provinces: Bangkok and Nakhonpathom (one year result). J. Med. Assoc. Thail 2010, 93, 1205–1210. [Google Scholar]
- Caca, I.; Cingu, A.K.; Sahin, A.; Ari, S.; Dursun, M.E.; Dag, U.; Balsak, S.; Alakus, F.; Yavuz, A.; Palanci, Y. Amblyopia and Refractive Errors among School-Aged Children with Low Socioeconomic Status in Southeastern Turkey. J. Pediatr. Ophthalmol. Strabismus 2013, 50, 37–43. [Google Scholar] [CrossRef] [Green Version]



| Refraction Parameter | Spherical Equivalent Criteria (D) |
|---|---|
| Emmetropia | −0.5 to ≤+0.5 |
| Pre-myopia | −0.50–+0.75 |
| Myopia | ≤−0.50 |
| Low myopia | −0.50–6 |
| High myopia | ≤−6 |
| Refractive myopia | a myopic refractive state that can be attributed to changes in the structure or location of the image-forming structures of the eye; that is, the cornea and/or lens |
| Axial myopia | a myopic refractive state that can be attributed to excessive axial elongation |
| Secondary Myopia | a myopic refractive state for which a single, specific cause (drug, corneal disease or systemic clinical syndrome) can be identified that is not a recognized population risk factor for the development of myopia |
| Pseudomyopia | instrument myopia, night myopia or accommodative spasm |
| Mild hyperopia | ≥+0.50–≤+2.0 |
| Significant hyperopia | ≥+2.00 |
| Anisometropia | ≥1.00 (difference between eyes) |
| Astigmatism | ≤−0.75 (cylinder) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monika, M.; Durajczyk, M. Evaluation of the Prevalence of Refractive Defects and Ocular Function in a Group of 1518 Children Aged 8 Years in Northwestern Poland—A Retrospective Study. J. Clin. Med. 2023, 12, 2880. https://doi.org/10.3390/jcm12082880
Monika M, Durajczyk M. Evaluation of the Prevalence of Refractive Defects and Ocular Function in a Group of 1518 Children Aged 8 Years in Northwestern Poland—A Retrospective Study. Journal of Clinical Medicine. 2023; 12(8):2880. https://doi.org/10.3390/jcm12082880
Chicago/Turabian StyleMonika, Modrzejewska, and Magdalena Durajczyk. 2023. "Evaluation of the Prevalence of Refractive Defects and Ocular Function in a Group of 1518 Children Aged 8 Years in Northwestern Poland—A Retrospective Study" Journal of Clinical Medicine 12, no. 8: 2880. https://doi.org/10.3390/jcm12082880