
Targeting of Periprosthetic Muscles for the Ultrasonographic Screening of Hip Abnormalities in Hip Resurfacing Arthroplasty Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
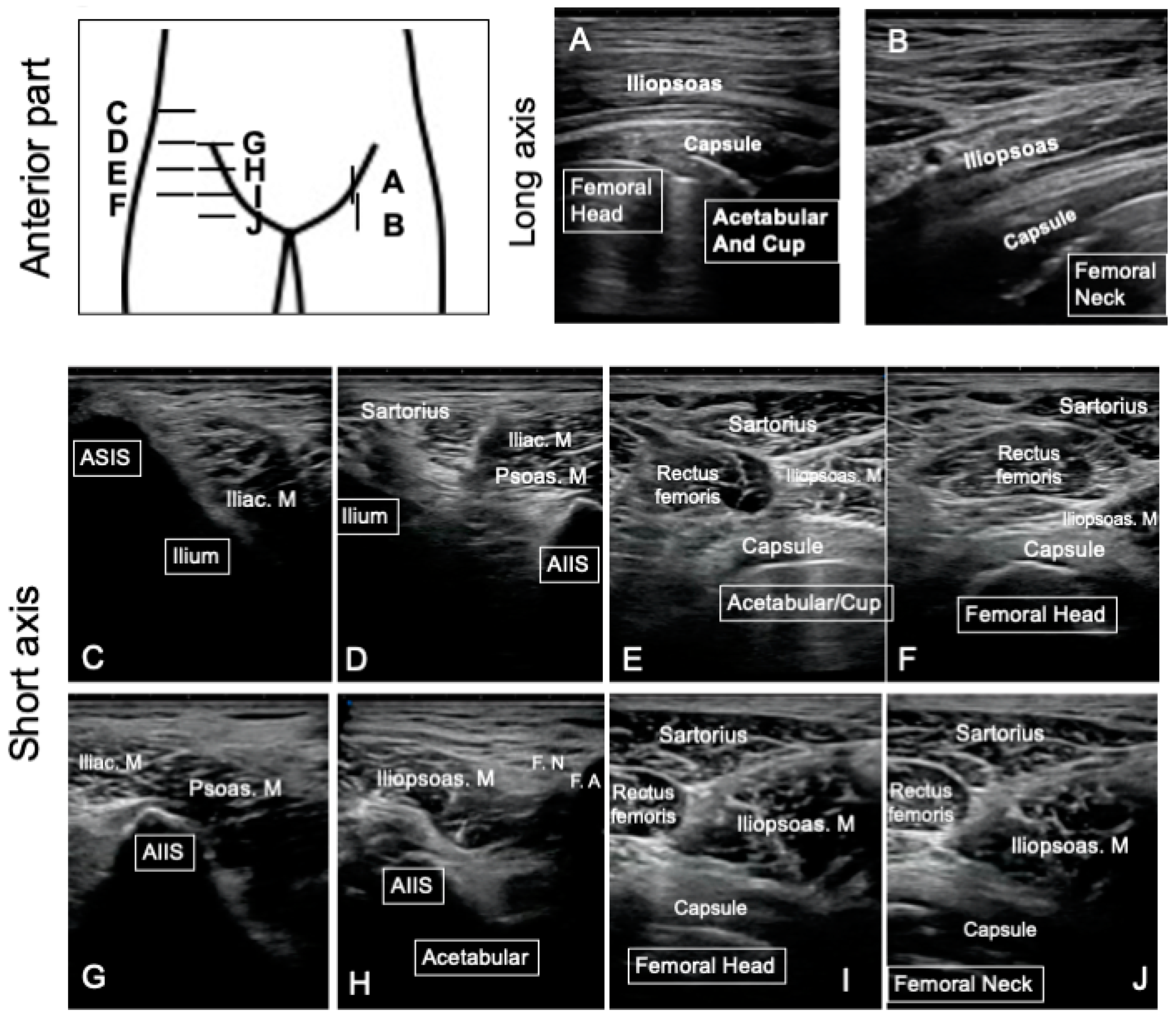
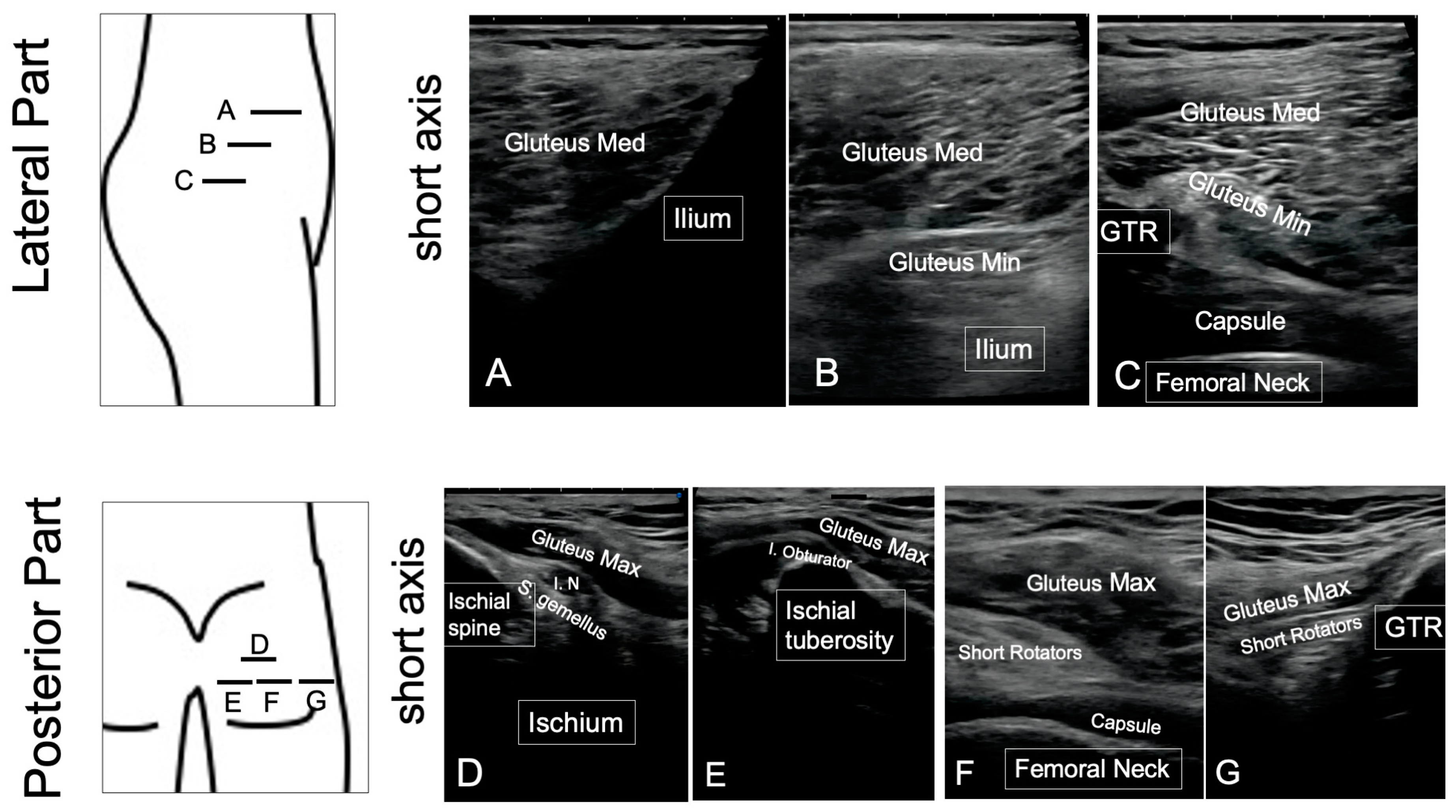
2.2. Ultrasonography
2.3. MRI
2.4. Clinical Outcome
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Henderson, R.A.; Lachiewicz, P.F. Groin pain after replacement of the hip: Aetiology, evaluation and treatment. J. Bone Jt. Surg. Br. 2012, 94, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issa, K.; Palich, A.; Tatevossian, T.; Kapadia, B.H.; Naziri, Q.; Mont, M.A. The outcomes of hip resurfacing compared to standard primary total hip arthroplasty in Men. BMC Musculoskelet. Disord. 2013, 14, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, Y.-M.; Glyn-Jones, S.; Simpson, D.J.; Kamali, A.; McLardy-Smith, P.; Gill, H.S.; Murray, D.W. Analysis of wear of retrieved metal-on-metal hip resurfacing implants revised due to pseudotumours. J. Bone Jt. Surg. 2010, 92, 356–361. [Google Scholar] [CrossRef]
- Achten, J.; Parsons, N.R.; Edlin, R.P.; Griffin, D.R.; Costa, M.L. A randomised controlled trial of total hip arthroplasty versus resurfacing arthroplasty in the treatment of young patients with arthritis of the hip joint. BMC Musculoskelet. Disord. 2010, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Matharu, G.S.; Pandit, H.G.; Murray, D.W.; Judge, A. Adverse reactions to metal debris occur with all types of hip replacement not just metal-on-metal hips: A retrospective observational study of 3340 revisions for adverse reactions to metal debris from the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. BMC Musculoskelet. Disord. 2016, 17, 495. [Google Scholar]
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Nishii, T.; Sakai, T.; Takao, M.; Yoshikawa, H.; Sugano, N. Is ultrasound screening reliable for adverse local tissue reaction after hip arthroplasty? J. Arthroplast. 2014, 29, 2239–2244. [Google Scholar] [CrossRef]
- Kwon, Y.M.; Dimitriou, D.; Liow, M.H.; Tsai, T.Y.; Li, G. Is Ultrasound As Useful As Metal Artifact Reduction Sequence Magnetic Resonance Imaging in Longitudinal Surveillance of Metal-on-Metal Hip Arthroplasty Patients? J. Arthroplast. 2016, 31, 1821–1827. [Google Scholar] [CrossRef]
- Robinson, D.J.; Lee, S.; Marks, P.; Schneider, M.E. Ultrasound Screening for Adverse Local Tissue Reaction after Hip Arthroplasty. Ultrasound Med. Biol. 2017, 43, 1549–1556. [Google Scholar] [CrossRef]
- Ghirardelli, S.; Touloupakis, G.; Antonini, G.; Violante, B.; Fidanza, A.; Indelli, P.F. Debridement, antibiotic, pearls, irrigation and retention of the implant and other local strategies on hip periprosthetic joint infections. Minerva Orthop. 2022, 73, 409–415. [Google Scholar] [CrossRef]
- Parisi, T.J.; Konopka, J.F.; Bedair, H.S. What is the Long-term Economic Societal Effect of Periprosthetic Infections After THA? A Markov Analysis. Clin. Orthop. Relat. Res. 2017, 475, 1891–1900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, A.V., Jr.; Barrack, R.L.; Berend, K.R.; Cuckler, J.M.; Jacobs, J.J.; Mont, M.A.; Schmalzried, T.P. The Hip Society: Algorithmic approach to diagnosis and management of metal-on-metal arthroplasty. J. Bone Jt. Surg. Br. 2012, 94, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Hauptfleisch, J.; Pandit, H.; Grammatopoulos, G.; Gill, H.S.; Murray, D.W.; Ostlere, S. A MRI classification of periprosthetic soft tissue masses (pseudotumours) associated with metal-on-metal resurfacing hip arthroplasty. Skeletal Radiol. 2012, 41, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Yanny, S.; Cahir, J.G.; Barker, T.; Wimhurst, J.; Nolan, J.F.; Goodwin, R.W.; Marshall, T.; Toms, A.P. MRI of aseptic lymphocytic vasculitis-associated lesions in metal-on-metal hip replacements. AJR Am. J. Roentgenol. 2012, 198, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Hayter, C.L.; Koff, M.F.; Potter, H.G. Magnetic resonance imaging of the postoperative hip. J. Magn. Reson. Imaging 2012, 35, 1013–1025. [Google Scholar] [CrossRef]
- Matharu, G.S.; Janardhan, S.; Brash, L.; Pynsent, P.B.; Dunlop, D.J.; James, S.L. The utility of repeat ultrasound imaging in the follow-up of metal-on-metal hip arthroplasty patients. Ann. R. Coll. Surg. Engl. 2016, 98, 143–149. [Google Scholar] [CrossRef]
- Willert, H.G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Koster, G.; Lohmann, C.H. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J. Bone Jt. Surg. Am. 2005, 87, 28–36. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; International Consensus Group on Periprosthetic Joint Infection. Definition of periprosthetic joint infection. J. Arthroplast. 2014, 29, 1331. [Google Scholar] [CrossRef] [Green Version]
- Campbell, P.; Beaule, P.E.; Ebramzadeh, E.; Le Duff, M.J.; De Smet, K.; Lu, Z.; Amstutz, H.C. The John Charnley Award: A study of implant failure in metal-on-metal surface arthroplasties. Clin. Orthop. Relat. Res. 2006, 453, 35–46. [Google Scholar] [CrossRef]
- Pandit, H.; Glyn-Jones, S.; McLardy-Smith, P.; Gundle, R.; Whitwell, D.; Gibbons, C.L.; Ostlere, S.; Athanasou, N.; Gill, H.S.; Murray, D.W. Pseudotumours associated with metal-on-metal hip resurfacings. J. Bone Jt. Surg. Br. 2008, 90, 847–851. [Google Scholar] [CrossRef] [Green Version]
- Nawabi, D.H.; Gold, S.; Lyman, S.; Fields, K.; Padgett, D.E.; Potter, H.G. MRI predicts ALVAL and tissue damage in metal-on-metal hip arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 471–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabi, D.; Levine, B.; Paprosky, W.; Della Valle, C.; Sporer, S.; Klein, G.; Levine, H.; Hartzband, M. Metal-on-metal total hip arthroplasty: Causes and high incidence of early failure. Orthopedics 2012, 35, e1009–e1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, Y.M.; Ostlere, S.J.; McLardy-Smith, P.; Athanasou, N.A.; Gill, H.S.; Murray, D.W. "Asymptomatic" pseudotumors after metal-on-metal hip resurfacing arthroplasty: Prevalence and metal ion study. J. Arthroplast. 2011, 26, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Goderecci, R.; Fidanza, A.; Necozione, S.; Francione, V.; Indelli, P.F.; Calvisi, V. Ultrasound-based decision making following metal-on-metal hip arthroplasty. J. Clin. Orthop. Trauma 2020, 11, 79–84. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Hips (Patients): 45 (40) | Mean | Range | |
|---|---|---|---|
| Age at surgery (years old) | 50 | 34–64 | |
| Gender (hips) | Female: 35, Male 10 | ||
| Harris Hip Score (Points) | Pre-operative | Mean: 55 (pain: 20) | 33–80 (10–30) |
| Postoperative (at 1 year) | 98 (pain: 43) | 80–100 (30–44) | |
| Follow-up period (years) | 8.6 | 4.1–10.7 | |
| Complications during follow-up (Hips) | Adverse reaction metal debris: 2 Periprosthetic joint infection: 2 Greater trochanteric bursitis: 4 Iliopsoas impingement: 1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choe, H.; Kobayashi, N.; Abe, K.; Hieda, Y.; Ike, H.; Kumagai, K.; Miyatake, K.; Fujisawa, T.; Inaba, Y. Targeting of Periprosthetic Muscles for the Ultrasonographic Screening of Hip Abnormalities in Hip Resurfacing Arthroplasty Patients. J. Clin. Med. 2023, 12, 2871. https://doi.org/10.3390/jcm12082871
Choe H, Kobayashi N, Abe K, Hieda Y, Ike H, Kumagai K, Miyatake K, Fujisawa T, Inaba Y. Targeting of Periprosthetic Muscles for the Ultrasonographic Screening of Hip Abnormalities in Hip Resurfacing Arthroplasty Patients. Journal of Clinical Medicine. 2023; 12(8):2871. https://doi.org/10.3390/jcm12082871
Chicago/Turabian StyleChoe, Hyonmin, Naomi Kobayashi, Koki Abe, Yuta Hieda, Hiroyuki Ike, Ken Kumagai, Kazuma Miyatake, Takahiro Fujisawa, and Yutaka Inaba. 2023. "Targeting of Periprosthetic Muscles for the Ultrasonographic Screening of Hip Abnormalities in Hip Resurfacing Arthroplasty Patients" Journal of Clinical Medicine 12, no. 8: 2871. https://doi.org/10.3390/jcm12082871