
Effect of Functional Electrical Stimulation in Convalescent Stroke Patients: A Multicenter, Randomized Controlled Trial
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
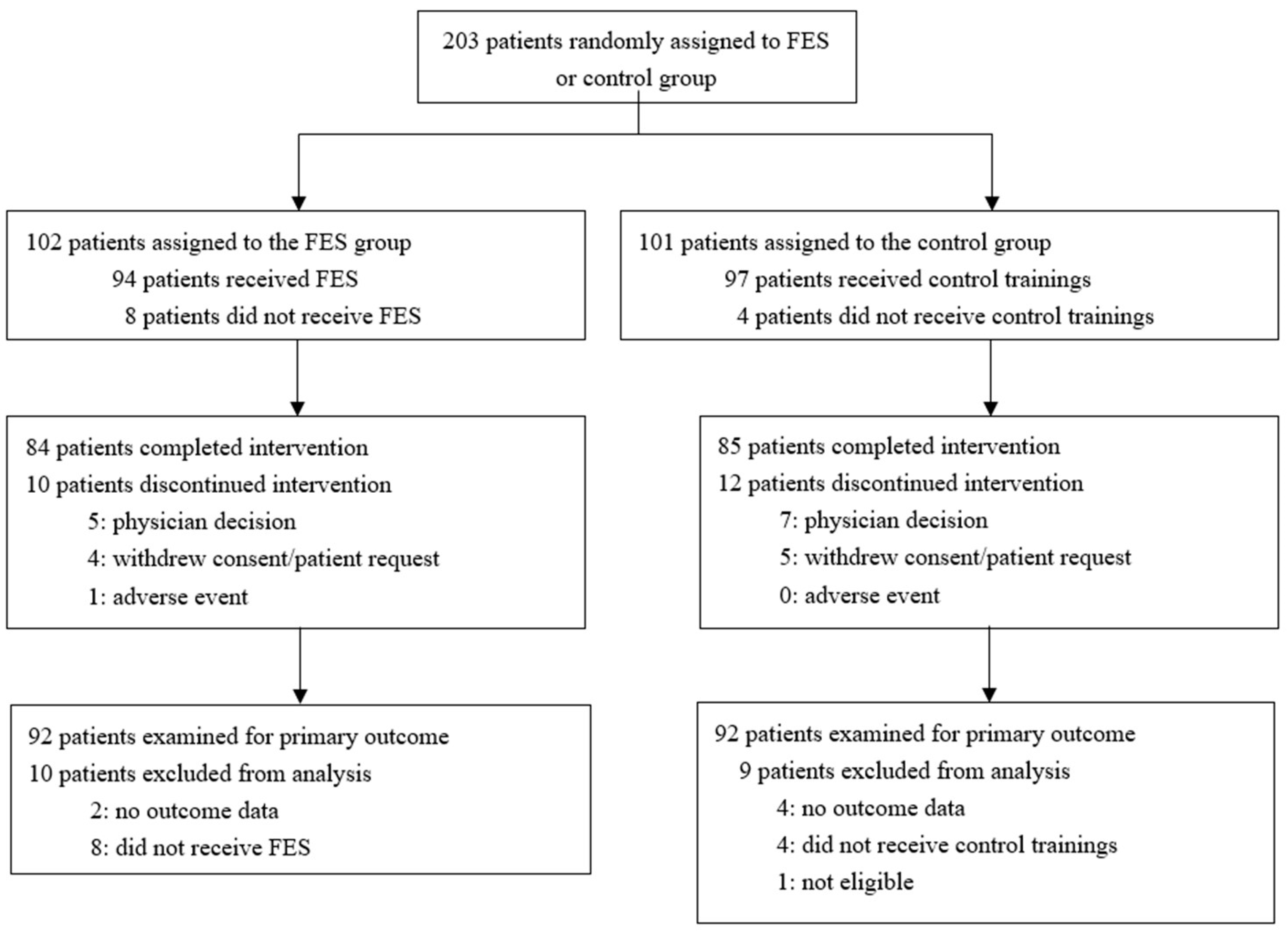
2.3. Randomization and Masking
2.4. Procedures
2.4.1. FES Group
2.4.2. Control Group
2.5. Outcomes
2.6. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| FES (n = 92) | ||||
|---|---|---|---|---|
| Baseline | Follow-Up | Change | ||
| 6-MWT distance, m | 193.07 (108.05) | 257.08 (110.47) | 64.01 (61.99) | |
| 10 m walk test speed, m/s | 0.58 (0.27) | 0.78 (0.29) | 0.20 (0.15) | |
| Timed up and go test, s | At comfortable speed | 25.78 (18.92) | 18.18 (9.58) | −7.61 (16.8) |
| At maximum speed | 21.71 (18.12) | 15.35 (8.12) | −6.37 (16.23) | |
| Gait disturbance at 10 m walk test | At stance phase | 6.27 (11.31) | 11.83 (11.1) | 5.56 (5.99) |
| At swing phase | 4.67 (9.24) | 9.08 (8.91) | 4.41 (4.69) | |
| At all phases | 10.94 (20.48) | 20.91 (19.96) | 9.97 (10.51) | |
Appendix B
- The RALLY trial investigators and committees
- Principal Investigator:
- Shuji Matsumoto, Center of Medical Education, Faculty of Health Sciences, Ryotokuji University, Japan.
- Vice Principal Investigator:
- Megumi Shimodozono, Department of Rehabilitation and Physical Medicine, Graduate School of Medical and Dental Sciences, Kagoshima University, Japan.
- Ryuji Miyata, Department of Rehabilitation and Physical Medicine, Graduate School of Medical and Dental Sciences, Kagoshima University, Japan.
- Data And Safety Monitoring Committee.
- Toyoko Asami, Department of Rehabilitation Medicine, Saga University Hospital, Japan.
- Akihiko Oowatashi, School of Health Sciences, Faculty of Medicine, Kagoshima University, Japan.
- Saburo Omine, Faculty of Rehabilitation, Kyusyu Nutrition Welfare University.
- Blinded Independent Central Review Board (Fugl–Meyer assessment, gait evaluation):
- Rina Ijichi, Department of Rehabilitation, Kirishima Sugiyasu Hospital, Japan.
- Tetsuya Onoda, Department of Rehabilitation, Kirishima Medical Center, Japan.
- Trial Statistician:
- Masanori Taketsuna, Translational Research Center for Medical Innovation, Japan.
- Study sites and trial investigators:
- Jun Ohkawara, Department of Rehabilitation, Ohkawara Neurosurgical Hospital.
- Takashi Shigematsu, Shintaro Iio, Tetsuya Suzuki, Department of Rehabilitation, Hamamatsu City Rehabilitation Hospital.
- Akira Satone, Keisuke Ono, Senshuu Abe, Eri Tanita, Department of Rehabilitation, Tokachi Rehabilitation Center.
- Hidenobu Okuma, Hironori Fujisaki, Department of Rehabilitation, Kumamoto Takumadai Rehabilitation Hospital.
- Makiko Seto, Junya Sasahara, Hiroyuki Yamamoto, Department of Rehabilitation, Nagasaki Kita Hospital.
- Shigeatsu Natsume, Masamori Fujiwara, Department of Rehabilitation, Eishokai Medical Corporation, Yoshida Hospital Cerebrovascular Research Institute.
- Norihito Kimura, Department of Rehabilitation, Caress Sapporo Tokeidai Memorial Hospital.
- Hirokazu Kawano, Department of Rehabilitation, Junwakai Memorial Hospital.
- Osamu Kira, Yousuke Miyanaga, Department of Rehabilitation Therapy, Junwakai Memorial Hospital.
- Kenji Matsumoto, Makiko Hayakawa, Department of Rehabilitation, Kansai Rehabilitation Hospital.
- Yuji Hashimoto, Department of Rehabilitation, Sapporo Shiroishi Memorial Hospital.
- Yasuhide Kido, Osamu Yamazaki, Yuuichi Suzuki, Department of Rehabilitation, Matsuyama Rehabilitation Hospital.
- Megumi Shimodozono, Rintaro Ohama, Ryuji Miyata, Department of Rehabilitation and Physical Medicine, Graduate School of Medical and Dental Sciences, Kagoshima University.
- Tomohiro Uema, Department of Rehabilitation, Kagoshima University Hospital.
- Makoto Ide, Koichiro Tobinaga, Tsutomu Asou, Shun Kumamoto, Department of Rehabilitation, St Mary’s Healthcare Center.
- Keizo Shigenobu, Yumeko Amano, Department of Rehabilitation, Kohshinkai Ogura Hospital.
- Toshihiro Nakamura, Kota Homan, Department of Rehabilitation, Acras Central Hospital.
- Yuki Onishi, Atsushi Manji, Kazuki Ogashira, Department of Rehabilitation, Saitama Misato General Rehabilitation Hospital.
- Tojiro Yanagi, Tetuya Noda, Horoki Fukuda, Department of Rehabilitation, Yame Rehabili Hospital.
- Katsuhiro Harada, Yuki Nakama, Keisuke Shibuya, Department of Rehabilitation, Fujimoto Kamimachi Hospital.
- Kanjiro Suzuki, Nobuaki Oshikawa, Tatsuya Yamashita, Department of Rehabilitation, Nichinan Municipal Chubu Hospital.
- You Ikegami, Kouhei Totiki, Department of Rehabilitation, Yohkoh Rehabilitation Hospital.
- Taisuke Arai, Kenji Ogushi, Shinya Nakagawa, Department of Rehabilitation, Shin Yachiyo Hospital.
- Rintaro Ohama, Yuji Sakashita, Kazutoshi Tomioka, Sota Araki, Department of Rehabilitation, Tarumizu Municipal Medical Center, Tarumizu Central Hospital.
- Yuko Takiyoshi, Hirohisa Oyadomari, Wakako Omine, Sayoko Hirayama, Department of Rehabilitation, Nambu Tokushukai Hospital.
- Shoichi Tanaka, Keisuke Sato, Takafumi Miyagi, Department of Rehabilitation, Chuzan Hospital.
- Masahiko Toshima, Kazuhiro Yanai, Naoki Shoji, Yuto Yamamoto. Department of Rehabilitation, Hokusei Memorial Hospital. Makoto Kawasaki, Sakurajyuji Hospital.
- Satoru Matayoshi, Department of Rehabilitation, Okinawa Rehabilitation Center Hospital.
- Keisuke Horinouchi, Department of Rehabilitation, Kajikionsen Hospital.
- Yuichi Komaba, Daiki Ooshima, Department of Rehabilitation, Hakujikai Memorial Hospital.
- Taro Ogawa, Department of Rehabilitation, Sapporo Keijinkai Rehabilitation Hospital.
- Jun Takeshita, Department of Rehabilitation, IMS Itabashi Rehabilitation Hospital.
- Data Center:
- Translational Research Center for Medical Innovation.
- Satoshi Nakagawa, Project Manager.
- Kuniko Hosokawa, Data Manager.
- Yoko Nakagawa, Statistical Programmer.
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and Regional Burden of Stroke During 1990–2010: Findings From the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Da Cunha, M.J.; Rech, K.D.; Salazar, A.P.; Pagnussat, A.S. Functional electrical stimulation of the peroneal nerve improves post-stroke gait speed when combined with physiotherapy. A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2021, 64, 101388. [Google Scholar] [CrossRef] [PubMed]
- Prenton, S.; Hollands, K.L.; Kenney, P.J.L. Functional electrical stimulation versus ankle foot orthoses for foot-drop: A meta-analysis of orthotic effects. J. Rehabil. Med. 2016, 48, 646–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohata, K.; Yasui, T.; Tsuboyama, T.; Ichihashi, N. Effects of an Ankle-Foot Orthosis with Oil Damper on Muscle Activity in Adults After Stroke. Gait. Posture 2011, 33, 102–107. [Google Scholar] [CrossRef]
- Shahabi, S.; Shabaninejad, H.; Kamali, M.; Jalali, M.; Ahmadi Teymourlouy, A. The Effects of Ankle-Foot Orthoses on Walking Speed in Patients with Stroke: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin. Rehabil. 2020, 34, 145–159. [Google Scholar] [CrossRef]
- Gil-Castillo, J.; Alnajjar, F.; Koutsou, A.; Torricelli, D.; Moreno, J.C. Advances in Neuroprosthetic Management of Foot Drop: A Review. J. Neuroeng. Rehabil. 2020, 17, 46. [Google Scholar] [CrossRef] [PubMed]
- Kluding, P.M.; Dunning, K.; O’Dell, M.W.; Wu, S.S.; Ginosian, J.; Feld, J.; McBride, K. Foot Drop Stimulation Versus Ankle Foot Orthosis After Stroke: 30-Week Outcomes. Stroke 2013, 44, 1660–1669. [Google Scholar] [CrossRef] [Green Version]
- Everaert, D.G.; Stein, R.B.; Abrams, G.M.; Dromerick, A.W.; Francisco, G.E.; Hafner, B.J.; Huskey, T.N.; Munin, M.C.; Nolan, K.J.; Kufta, C.V. Effect of a Foot-Drop Stimulator and Ankle-Foot Orthosis on Walking Performance After Stroke: A Multicenter Randomized Controlled Trial. Neurorehabil. Neural Repair. 2013, 27, 579–591. [Google Scholar] [CrossRef]
- Sheffler, L.R.; Taylor, P.N.; Gunzler, D.D.; Buurke, J.H.; IJzerman, M.J.; Chae, J. Randomized Controlled Trial of Surface Peroneal Nerve Stimulation for Motor Relearning in Lower Limb Hemiparesis. Arch. Phys. Med. Rehabil. 2013, 94, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bethoux, F.; Rogers, H.L.; Nolan, K.J.; Abrams, G.M.; Annaswamy, T.M.; Brandstater, M.; Browne, B.; Burnfield, J.M.; Feng, W.; Freed, M.J.; et al. The Effects of Peroneal Nerve Functional Electrical Stimulation Versus Ankle-Foot Orthosis in Patients with Chronic Stroke: A Randomized Controlled Trial. Neurorehabil. Neural Repair 2014, 28, 688–697. [Google Scholar] [CrossRef]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of New Policies for Inpatient Rehabilitation Coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef]
- Reed, S.D.; Blough, D.K.; Meyer, K.; Jarvik, J.G. Inpatient Costs, Length of Stay, and Mortality for Cerebrovascular Events in Community Hospitals. Neurology 2001, 57, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Gillum, R.F.; Kwagyan, J.; Obisesan, T.O. Ethnic and Geographic Variation in Stroke Mortality Trends. Stroke 2011, 42, 3294–3296. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Shimodozono, M.; Noma, T. Rationale and Design of the theRapeutic Effects of Peroneal Nerve functionAl Electrical stimuLation for Lower Extremity in Patients with Convalescent Poststroke Hemiplegia (RALLY) Study: Study Protocol for a Randomised Controlled Study. BMJ Open 2019, 9, e026214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical Gait Assessment in the Neurologically Impaired: Reliability and Meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef]
- Solway, S.; Brooks, D.; Lacasse, Y.; Thomas, S. A Qualitative Systematic Overview of the Measurement Properties of Functional Walk Tests Used in the Cardiorespiratory Domain. Chest 2001, 119, 256–270. [Google Scholar] [CrossRef]
- Wade, D.T.; Wood, V.A.; Heller, A.; Maggs, J.; Langton Hewer, R. Walking after Stroke. Measurement and Recovery Over the First 3 Months. Scand. J. Rehabil. Med. 1987, 19, 25–30. [Google Scholar]
- Street, T.; Taylor, P.; Swain, I. Effectiveness of Functional Electrical Stimulation on Walking Speed, Functional Walking Category, and Clinically Meaningful Changes for People with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2015, 96, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing Walking Speed in Clinical Research: A Systematic Review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef]
- Stein, R.B.; Everaert, D.G.; Thompson, A.K.; Chong, S.L.; Whittaker, M.; Robertson, J.; Kuether, G. Long-Term Therapeutic and Orthotic Effects of a Foot Drop Stimulator on Walking Performance in Progressive and Nonprogressive Neurological Disorders. Neurorehabil. Neural Repair 2010, 24, 152–167. [Google Scholar] [CrossRef]
- Salisbury, L.; Shiels, J.; Todd, I.; Dennis, M. A Feasibility Study to Investigate the Clinical Application of Functional Electrical Stimulation (FES), for Dropped Foot, During the Sub-acute Phase of Stroke-A Randomized Controlled Trial. Physiother. Theory Pract. 2013, 29, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Sheffler, L.R.; Taylor, P.N.; Bailey, S.N.; Gunzler, D.D.; Buurke, J.H.; IJzerman, M.J.; Chae, J. Surface Peroneal Nerve Stimulation in Lower Limb Hemiparesis: Effect on Quantitative Gait Parameters. Am. J. Phys. Med. Rehabil. 2015, 94, 341–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesci, N.; Ozdemir, F.; Kabayel, D.D.; Tokuc, B. The Effects of Neuromuscular Electrical Stimulation on Clinical Improvement in Hemiplegic Lower Extremity Rehabilitation in Chronic Stroke: A Single-Blind, Randomised, Controlled Trial. Disabil. Rehabil. 2009, 31, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.A.; Burridge, J.; Strike, P.; Taylor, P. A Randomised Controlled Trial of Integrated Electrical Stimulation and Physiotherapy to Improve Mobility for People Less Than 6 Months Post Stroke. Disabil. Rehabil. Assist. Technol. 2015, 10, 468–474. [Google Scholar] [CrossRef]
- Bethoux, F.; Rogers, H.L.; Nolan, K.J.; Abrams, G.M.; Annaswamy, T.; Brandstater, M.; Browne, B.; Burnfield, J.M.; Feng, W.; Freed, M.J.; et al. Long-Term Follow-Up to a Randomized Controlled Trial Comparing Peroneal Nerve Functional Electrical Stimulation to an Ankle Foot Orthosis for Patients with Chronic Stroke. Neurorehabil. Neural Repair 2015, 29, 911–922. [Google Scholar] [CrossRef]
- Bosch, P.R.; Harris, J.E.; Wing, K.; American Congress of Rehabilitation Medicine (ACRM) Stroke Movement Interventions Subcommittee. Review of Therapeutic Electrical Stimulation for Dorsiflexion Assist and Orthotic Substitution from the American Congress of Rehabilitation Medicine Stroke Movement Interventions Subcommittee. Arch. Phys. Med. Rehabil. 2014, 95, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [Green Version]
- Dean, J.C.; Kautz, S.A. Foot placement control and gait instability among people with stroke. J. Rehabil. Res. Dev. 2015, 52, 577–590. [Google Scholar] [CrossRef]
- Hachisuka, K.; Ochi, M.; Kikuchi, T.; Saeki, S. Clinical effectiveness of peroneal nerve functional electrical stimulation in chronic stroke patients with hemiplegia (PLEASURE): A multicentre, prospective, randomised controlled trial. Clin Rehabil. 2021, 35, 367–377. [Google Scholar] [CrossRef]

| FES (n = 92) | Control (n = 92) | ||
|---|---|---|---|
| Age, years | 63.5 (10.5) | 64.3 (11.8) | |
| Sex (male) | 70 (76) | 68 (74) | |
| Body weight, kg | 62.6 (10.9) | 61.4 (12.0) | |
| Time since stroke onset, days | 59.5 (32.6) | 63.7 (30.4) | |
| Cause of hemiplegia | Cerebral hemorrhage | 42 (46) | 40 (43) |
| Cerebral infarction | 50 (54) | 52 (57) | |
| FAC category | 3 | 49 (53) | 52 (57) |
| 4 | 43 (47) | 40 (43) | |
| MAS score of plantar flexor muscles, knee extended | 0 | 10 (11) | 14 (15) |
| 1 | 28 (30) | 27 (29) | |
| 1+ | 32 (35) | 31 (34) | |
| 2 | 17 (18) | 18 (20) | |
| 3 | 5 (5) | 1 (1) | |
| 4 | 0 (0) | 0 (0) | |
| MAS score of plantar flexor muscles, knee flexed | 0 | 21 (23) | 21 (23) |
| 1 | 34 (37) | 34 (37) | |
| 1+ | 24 (26) | 25 (27) | |
| 2 | 11 (12) | 10 (11) | |
| 3 | 2 (2) | 1 (1) | |
| 4 | 0 (0) | 0 (0) | |
| Dorsiflexion range of motion | Active | 5.5 (5.5) | 7.6 (7.6) |
| Passive, knee extended | 7.0 (6.1) | 6.0 (7.6) | |
| Passive, knee flexed | 13.6 (6.6) | 14.7 (7.5) |
| FES (n = 92) | Control (n = 92) | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Change | Baseline | Follow-Up | Change | p-Value | ||
| 6-MWT (barefoot) distance, m | 164.21 (105.99) | 232.57 (122.88) | 68.37 (62.42) | 153.87 (113.96) | 211.37 (126.89) | 57.50 (68.17) | 0.26 | |
| 6-MWT (with AFO) distance, m | 179.46 (92.66) | 238.24 (97.87) | 58.78 (55.66) | 178.61 (109.96) | 245.00 (123.76) | 66.40 (55.25) | 0.39 | |
| 10-m walk test (barefoot) speed, m/s | 0.55 (0.29) | 0.76 (0.31) | 0.21 (0.18) | 0.51 (0.3) | 0.68 (0.37) | 0.17 (0.17) | 0.16 | |
| 10-m walk test (with AFO) speed, m/s | 0.54 (0.25) | 0.71 (0.28) | 0.17 (0.16) | 0.55 (0.28) | 0.71 (0.33) | 0.16 (0.14) | 0.86 | |
| Lower extremity FMA score | 25.65 (4.87) | 27.31 (4.33) | 1.66 (2.49) | 25.16 (5.14) | 26.43 (5.29) | 1.28 (2.9) | 0.34 | |
| MAS score of plantar flexor muscles | Knee extended | 1.36 (0.69) | 1.21 (0.68) | −0.15 (0.67) | 1.24 (0.66) | 1.06 (0.67) | −0.18 (0.61) | 0.76 |
| Knee flexed | 1.06 (0.71) | 1.07 (0.72) | 0.01 (0.68) | 1.04 (0.68) | 0.90 (0.65) | −0.14 (0.65) | 0.15 | |
| Dorsiflexion range of motion | Active | 5.46 (5.57) | 8.54 (6.54) | 3.08 (4.21) | 7.73 (7.6) | 8.33 (8.7) | 0.61 (4.25) | 0.001 |
| Passive, knee flexed | 13.62 (6.59) | 14.66 (6.37) | 1.03 (5.51) | 14.72 (7.48) | 15.06 (7.74) | 0.34 (5.58) | 0.41 | |
| Timed up and go test (barefoot), s | At comfortable speed | 28.52 (15.88) | 19.18 (10.09) | −9.34 (10.23) | 31.29 (18.84) | 22.84 (16.66) | −8.45 (10.71) | 0.58 |
| At maximum speed | 23.32 (13.07) | 16.30 (9.82) | −7.03 (8.61) | 27.02 (17.83) | 18.99 (13.66) | −8.03 (10.24) | 0.49 | |
| Timed up and go test (with AFO), s | At comfortable speed | 27.81 (16.77) | 20.12 (11.69) | −7.68 (12.45) | 29.68 (19.66) | 21.48 (15.65) | −8.20 (10.8) | 0.78 |
| At maximum speed | 23.32 (13.07) | 16.30 (9.82) | −7.03 (8.61) | 27.02 (17.83) | 18.99 (13.66) | −8.03 (10.24) | 0.49 | |
| Stroke Impact Scale | Mobility | 53.49 (21.26) | 76.17 (17.61) | 22.69 (21.61) | 52.17 (21.11) | 71.71 (23.03) | 19.54 (21.52) | 0.33 |
| Total score | 54.32 (12.17) | 64.50 (13.84) | 10.18 (11.92) | 54.15 (13.32) | 62.92 (14.3) | 8.77 (10.9) | 0.41 | |
| Patient-reported | Burden in raising the foot during barefoot walking | 40.76 (22.23) | 59.42 (20.57) | 18.66 (23.44) | 37.35 (23.73) | 51.45 (22.76) | 14.10 (24.32) | 0.20 |
| Spasticity while walking bare-footed | 50.53 (28.79) | 67.58 (26.64) | 17.05 (33.84) | 57.49 (32.74) | 60.08 (28.12) | 2.59 (33.37) | 0.005 | |
| Stability in bare-footed walking | 41.85 (24.93) | 64.25 (23.22) | 22.41 (22.69) | 40.19 (25.36) | 54.55 (26.79) | 14.35 (24.91) | 0.02 | |
| Gait disturbance evaluated by the care providers (barefoot) | At stance phase | 3.15 (12.54) | 9.38 (12.34) | 6.23 (6.96) | 1.99 (11.85) | 6.05 (12.97) | 4.06 (6.32) | 0.04 |
| At swing phase | 2.42 (10.23) | 7.12 (10.26) | 4.70 (5.45) | 1.77 (9.79) | 4.68 (10.53) | 2.90 (4.71) | 0.02 | |
| At all phases | 5.57 (22.69) | 16.50 (22.52) | 10.93 (12.17) | 3.76 (21.55) | 10.73 (23.44) | 6.96 (10.79) | 0.03 | |
| Gait disturbance (AFO) | At stance phase | 2.76 (9.49) | 8.28 (10.13) | 5.53 (5.71) | 2.79 (10.23) | 6.87 (10.98) | 4.08 (6.62) | 0.15 |
| At swing phase | 1.81 (7.99) | 6.26 (8.26) | 4.45 (4.38) | 1.90 (8.48) | 5.19 (9.02) | 3.29 (5.09) | 0.13 | |
| At all phases | 4.57 (17.37) | 14.54 (18.31) | 9.97 (9.81) | 4.69 (18.63) | 12.06 (19.94) | 7.37 (11.53) | 0.13 | |
| FES (n = 94) | Control (n = 96) | p-Value | |
|---|---|---|---|
| Any adverse event | 7 (7) | 2 (2) | 0.10 |
| Adverse events related to treatment | 0 | 0 | - |
| Any serious adverse event | 1 (1) | 0 | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, S.; Shimodozono, M.; Noma, T.; Miyara, K.; Onoda, T.; Ijichi, R.; Shigematsu, T.; Satone, A.; Okuma, H.; Seto, M.; et al. Effect of Functional Electrical Stimulation in Convalescent Stroke Patients: A Multicenter, Randomized Controlled Trial. J. Clin. Med. 2023, 12, 2638. https://doi.org/10.3390/jcm12072638
Matsumoto S, Shimodozono M, Noma T, Miyara K, Onoda T, Ijichi R, Shigematsu T, Satone A, Okuma H, Seto M, et al. Effect of Functional Electrical Stimulation in Convalescent Stroke Patients: A Multicenter, Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(7):2638. https://doi.org/10.3390/jcm12072638
Chicago/Turabian StyleMatsumoto, Shuji, Megumi Shimodozono, Tomokazu Noma, Kodai Miyara, Tetsuya Onoda, Rina Ijichi, Takashi Shigematsu, Akira Satone, Hidenobu Okuma, Makiko Seto, and et al. 2023. "Effect of Functional Electrical Stimulation in Convalescent Stroke Patients: A Multicenter, Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 7: 2638. https://doi.org/10.3390/jcm12072638