
Factors Associated with Esthetic Outcomes of Flapless Immediate Placed and Loaded Implants in the Maxillary Incisor Region—Three-Year Results of a Prospective Case Series
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Procedure
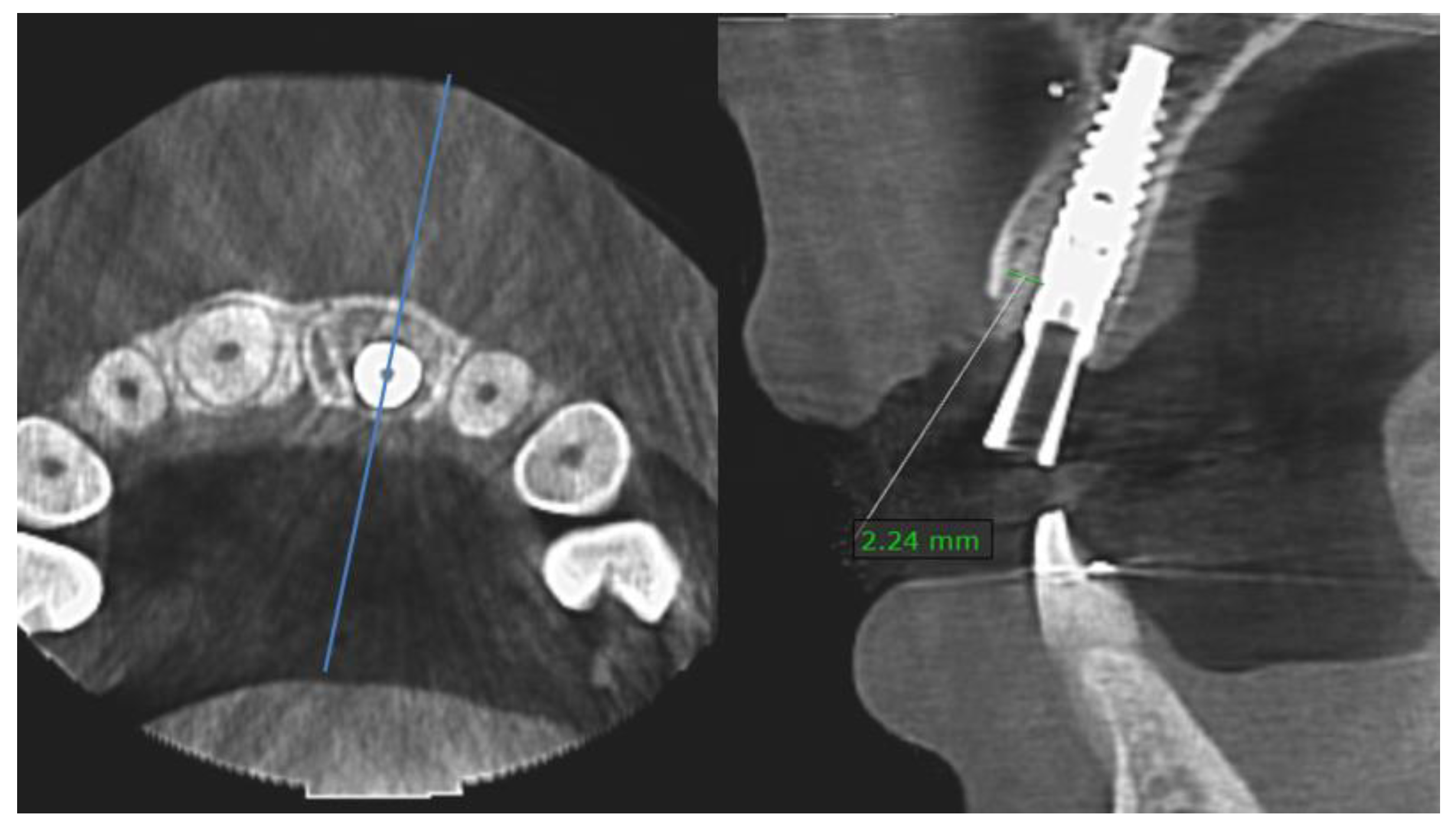
2.2. Clinical and Radiological Measurements
2.3. Esthetic Measurements
2.4. Patient Satisfaction
2.5. Statistical Analysis
3. Results
3.1. Implant Survival and Complications
3.2. General Periodontal Health
3.3. Buccal Bone Defects
3.4. Bone Gap Measurements
3.5. Patient Satisfaction
3.6. Soft-Tissue Esthetic Outcome
3.7. Tooth-Related Esthetic Outcome
3.8. Classification of Esthetic Outcomes
3.9. Multilevel Regression Analysis (MRA)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hämmerle, C.H.F.; Araújo, M.G.; Simion, M.; On Behalf of the Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin. Oral Implant. Res. 2012, 23 (Suppl. S5), 80–82. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Beagle, J.; Jensen, S.S.; Chiapasco, M.; Darby, I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int. J. Oral Maxillofac. Implant. 2009, 24, 272–278. [Google Scholar]
- Cosyn, J.; Hooghe, N.; De Bruyn, H. A systematic review on the frequence of advanced recession following single immediate implant treatment. J. Clin. Periodontol. 2012, 39, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh-Ba, G.; Pjetursson, B.E.; Sanz, M.; Cecchinato, D.; Ferrus, J.; Lindhe, J.; Lang, N.P. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin. Oral Implant. Res. 2010, 21, 37–42. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontol. 2000 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extraction alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Shahim, K.; Reyes, M.; Katsaros, C.; Buser, D. Ridge Alterations Post-Extraction in the Esthetic Zone: A 3D Analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef] [Green Version]
- Grunder, U.; Gracis, S.; Capelli, M. Influence of the 3-D bone-to-implant relationship on esthetics. Int. J. Periodontics Restor. Dent. 2005, 25, 113–119. [Google Scholar] [PubMed]
- Qahash, M.; Susin, C.; Polimeni, G.; Hall, J.; Wikesjö, U.M.E. Bone healing dynamics at buccal peri-implant sites. Clin. Oral Implant. Res. 2008, 19, 166–172. [Google Scholar] [CrossRef]
- Tomasi, C.; Sanz, M.; Cecchinato, D.; Pjetursson, B.; Ferrus, J.; Lang, N.P.; Lindhe, J. Bone dimensional variations at implants placed in fresh extraction sockets: A multilevel multivariate analysis. Clin. Oral Implant. Res. 2010, 21, 30–36. [Google Scholar] [CrossRef]
- Caneva, M.; Salata, L.A.; de Souza, S.S.; Baffone, G.; Lang, N.P.; Botticelli, D. Influence of implant positioning in extraction sockets on osseointegration: Histomorphometric analyses in dogs. Clin. Oral Implant. Res. 2010, 21, 43–49. [Google Scholar] [CrossRef]
- Cho, Y.-B.; Moon, S.-J.; Chung, C.-H.; Kim, H.-J. Resorption of labial bone in maxillary anterior implant. J. Adv. Prosthodont. 2011, 3, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Zuiderveld, E.G.; den Hartog, L.; Vissink, A.; Raghoebar, G.M.; Meijer, H.J.A. Significance of bucco-palatal implant position, biotype, platform switching, and pre-implant bone augmentation on the level of the mid-buccal mucosa. Int. J. Prosthodont. 2014, 27, 477–479. [Google Scholar] [CrossRef] [Green Version]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]
- Belser, U.C.; Grutter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef]
- Buser, D.; Wittneben, J.; Bornstein, M.M.; Grütter, L.; Chappuis, V.; Belser, U.C. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. J. Periodontol. 2011, 82, 342–349. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Kuchler, U.; Bornstein, M.M.; Wittneben, J.G.; Buser, R.; Cavusoglu, Y.; Belser, U.C. Long-term stability of early implant placement with contour augmentation. J. Dent. Res. 2013, 92, 176S–182S. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Bornstein, M.M.; Wittneben, J.-G.; Frei, M.; Belser, U.C. Long term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: A prospective, cross-sectional study in 41 patients with a 5- to 9- year follow up. J. Periodontol. 2013, 84, 1517–1527. [Google Scholar] [CrossRef]
- Meijndert, C.M.; Raghoebar, G.M.; Santing, H.J.; Vissink, A.; Meijer, H.J.A. Performance of bone-level implants with conical connections in the anterior maxilla: A 5-year prospective cohort study. Clin. Oral Implant. Res. 2020, 31, 173–180. [Google Scholar] [CrossRef]
- Mangano, F.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piatelli, A. Single tooth morse taper connection implants placed into fresh extraction sockets of the anterior maxilla: An esthetic evaluation. Clin. Oral Implant. Res. 2012, 23, 1302–1307. [Google Scholar] [CrossRef]
- Furze, D.; Byrne, A.; Donos, N.; Mardas, N. Clinical and esthetic outcomes of single tooth implants in the anterior maxilla. Quintessence Int. 2012, 43, 127–134. [Google Scholar] [PubMed]
- Van Nimwegen, W.G.; Goené, R.J.; van Daelen, A.C.L.; Stellingsma, K.; Raghoebar, G.M.; Meijer, H.J.A. Immediate implant placement and provisionalisation in the aesthetic zone. J. Oral Rehabil. 2016, 43, 745–752. [Google Scholar] [CrossRef]
- Slagter, K.W.; Raghoebar, G.M.; Hentenaar, D.F.M.; Vissink, A.; Meijer, H.J.A. Immediate placement of single implants with or without immediate provisionalization in the maxillary aesthetic region: A 5-year comparative study. J. Clin. Periodontol. 2021, 48, 272–283. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Cortellini, P.; Graziani, F.; Cairo, F.; Lang, N.P.; Abundo, R.; Conforti, G.P.; Marquardt, S.; Rasperini, G.; Silvestri, M.; et al. Immediate versus delayed implant placement after anterior single tooth extraction: The timing randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Cosyn, J.; Eghbali, A.; De Bruyn, H.; Collys, K.; Cleymaet, R.; De Rouck, T. Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J. Clin. Periodontol. 2011, 38, 746–753. [Google Scholar] [CrossRef]
- Noelken, R.; Kunkel, M.; Wagner, W. Immediate implant placement and provisionalization after long-axis root fracture and complete loss of the facial bony lamella. Int. J. Periodontics Restor. Dent. 2011, 31, 175–183. [Google Scholar] [PubMed]
- Noelken, R.; Neffe, B.A.; Kunkel, M.; Wagner, W. Maintenance of marginal bone support and soft tissue esthetics at immediately provisionalized OsseoSpeed implants placed into extraction sites: 2-year results. Clin. Oral Implant. Res. 2014, 25, 214–220. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; de Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef]
- Felice, P.; Pistilli, R.; Barausse, C.; Trullenque-Eriksson, A.; Esposito, M. Immediate Non-Occlusal Loading of Immediate Post-Extractive Versus Delayed Placement of Single Implants in Preserved Sockets of the Anterior Maxilla: 1-year Post-Loading Outcome of a Randomised Controlled Trial. Eur. J. Oral Implantol. 2015, 8, 361–372. [Google Scholar] [PubMed]
- Noelken, R.; Oberhansl, F.; Kunkel, M.; Wagner, W. Immediately provisionalized OsseoSpeed™ Profile implants inserted into extraction sockets: 3-year results. Clin. Oral Implant. Res. 2016, 27, 744–749. [Google Scholar] [CrossRef]
- Groenendijk, E.; Staas, T.A.; Graauwmans, F.E.J.; Bronkhorst, E.; Verhamme, L.; Maal, T.; Meijer, G.J. Immediate Implant Placement: The Fate of the Buccal Crest. A retrospective Cone Beam Computed Tomography Study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1600–1606. [Google Scholar] [CrossRef]
- Noelken, R.; Moergel, M.; Kunkel, M.; Wagner, W. Immediate and flapless implant insertion and provisionalization using autogenous bone grafts in the esthetic zone: 5-year results. Clin. Oral Implant. Res. 2018, 29, 320–327. [Google Scholar] [CrossRef]
- Noelken, R.; Moergel, M.; Pausch, T.; Kunkel, M.; Wagner, W. Clinical and esthetic outcome with immediate insertion and provisionalization with or without connective tissue grafting in presence of mucogingival recessions: A retrospective analysis with follow-up between 1 and 8 years. Clin. Implant. Dent. Relat. Res. 2018, 20, 285–293. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Immediate and early implant placement in single tooth gaps in the anterior maxilla: A prospective study on ridge dimensional, clinical, and aesthetic changes. Clin. Oral Implant. Res. 2018, 29, 1143–1154. [Google Scholar] [CrossRef]
- Groenendijk, E.; Staas, T.A.; Bronkhorst, E.; Raghoebar, G.M.; Meijer, G.J. Immediate Implant Placement and Provisionalization: Aesthetic Outcome 1 year after Implant Placement. A Prospective Clinical Multicenter Study. Clin. Implant. Dent. Relat. Res. 2020, 1, 193–200. [Google Scholar] [CrossRef]
- Seyssens, L.; Eghbali, A.; Cosyn, J. A 10-year prospective study on single immediate implants. J. Clin. Periodontol. 2020, 47, 1248–1258. [Google Scholar] [CrossRef]
- Pohl, V.; Fürhauser, L.; Haas, R.; Pohl, S. Gingival recession behavior with immediate implant placement in the anterior maxilla with buccal dehiscence without additional augmentation—A pilot study. Clin. Oral Investig. 2020, 24, 1455–1464. [Google Scholar] [CrossRef] [Green Version]
- Groenendijk, E.; Meijer, G.J. Flapless Immediate Implant Placement and Provisionalization (FIIPP) in the Aesthetic Region: Surgical Protocol of a Prospective Clinical Cohort Study on 100 Patients—Two Case Reports: Intact Socket, and Defect Socket with a Thin Gingival Phenotype. Surg. Case Rep. 2021, 4, 2–5. [Google Scholar] [CrossRef]
- Staas, T.A.; Groenendijk, E.; Bronkhorst, E.; Verhamme, L.; Raghoebar, G.M.; Meijer, G.J. Does initial buccal crest thickness affect final buccal crest thickness after flapless immediate implant placement and provisionalization: A prospective cone beam computed tomogram cohort study. Clin. Implant. Dent. Relat. Res. 2022, 24, 24–33. [Google Scholar] [CrossRef]
- Kan, J.Y.; Roe, P.; Rungcharassaeng, K.; Patel, R.D.; Waki, T.; Lozada, J.L.; Zimmerman, G. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: A cone beam computed tomography study. Int. J. Oral Maxillofac. Implant. 2011, 26, 873–876. [Google Scholar] [PubMed]
- Van der Velden, U. The Dutch periodontal screening index validation and its application in The Netherlands. J. Clin. Periodontol. 2009, 36, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Van Oort, D. Bohn Stafleu Van Loghum. In Digitale Mondfotografie: Een Praktische Handleiding; Bohn Stafleu van Loghum: Houten, The Netherlands, 2009; p. 149. ISBN 9789031368754. [Google Scholar]
- Vermylen, K.; Collaert, B.; Lindén, U.; Björn, A.-L.; De Bruyn, H. Patient satisfaction and quality of single-tooth restorations. A 7-year follow-up pilot study in private dental practices. Clin. Oral Implant. Res. 2003, 14, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Cosyn, J.; Eghbali, A.; De Bruyn, H.; Dierens, M.; De Rouck, T. Single implant treatment in healing versus healed sites of the anterior maxilla: An aesthetic evaluation. Clin. Implant. Dent. Relat. Res. 2010, 14, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Raes, F.; Cosyn, J.; Crommelinck, E.; Coessens, P.; De Bruyn, H. Immediate and conventional single implant treatment in the anterior maxilla: One-year results of a case series on hard and soft tissue remodelling and aesthetics. J. Clin. Periodontol. 2011, 38, 385–394. [Google Scholar] [CrossRef]
- Raes, S.; Cosyn, J.; Noyelle, A.; Raes, F.; De Bruyn, H. Clinical Outcome After 8 to 10 Years of Immediately Restored Single Implants Placed in Extraction Sockets and Healed Ridges. Int. J. Periodontic Restor. Dent. 2018, 38, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Seyssens, L.; Eeckhout, C.; Cosyn, J. Immediate implant placement with or without socket grafting: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2022, 24, 339–351. [Google Scholar] [CrossRef]
- Pitman, J.D.; Christiaens, V.; Callens, J.; Glibert, M.; Seyssens, L.; Blanco, J.; Cosyn, J. Immediate implant placement with flap or flapless surgery: A systematic review and meta-analysis. J. Clin. Periodontol. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Pitman, J.D.; Seyssens, L.; Christiaens, V.; Cosyn, J. Immediate implant placement with or without immediate provisionalization: A systematic review and meta-analysis. J. Clin. Periodontol. 2022, 49, 1012–1023. [Google Scholar] [CrossRef]
- Seyssens, L.; De Lat, L.; Cosyn, J. Immediate implant placement with or without connective tissue graft: A systematic review and meta-analysis. J. Clin. Periodontol. 2021, 48, 284–301. [Google Scholar] [CrossRef]
- Ferrantino, L.; Camurati, A.; Gambino, P.; Marzolo, M.; Trisciuoglio, D.; Santoro, G.; Farina, V.; Fontana, F.; Asa’ad, F.; Simion, M. Aesthetic outcomes of non-functional immediately restored single post-extraction implants with and without connective tissue graft: A multicentre randomized controlled trial. Clin. Oral Implant. Res. 2021, 32, 684–694. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Satisfaction Questionnaire | ||
|---|---|---|
| Q1 | What was your experience concerning duration of surgery? | 1–5: long–short |
| Q2 | What was your experience about post-surgery complaints? | 1–5: severe–limited |
| Q3 | Would you undergo this treatment again in a similar situation? | 1–5: no–certainly |
| Q4 | Would you recommend this treatment to others? | 1–5: no–certainly |
| Q5 | What is your opinion about color/gums around implant? | 1–5: ugly–beautiful |
| Q6 | What is your opinion about shape/location of gums margin? | 1–5: ugly–beautiful |
| Q7 | Do the gums look natural compared to the natural teeth? | 1–5: no–certainly |
| Q8 | What is your opinion about the form/color of the implant crown? | 1–5: ugly–beautiful |
| Q91–5 | What is your total score considering the treatment and result | 1–5: poor–excellent |
| Q91–10 | Total score (Q9: range 1–5) transformed to a scale of 1–10. | 1–10: poor–excellent |
| T4-PES | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | n |
|---|---|---|---|---|---|---|---|---|---|---|
| MBBD (mm) | ||||||||||
| 0 | 2 | 5 | 8 | 8 | 6 | 29 | ||||
| 1 | 1 | 5 | 3 | 6 | 3 | 18 | ||||
| 2 | 1 | 1 | 1 | 2 | 1 | 7 | 2 | 15 | ||
| 3 | 2 | 1 | 1 | 4 | ||||||
| 4 | 1 | 4 | 1 | 6 | ||||||
| 5 | ||||||||||
| 6 | 1 | 3 | 4 | |||||||
| 7 | 1 | 1 | 1 | 3 | ||||||
| 8 | ||||||||||
| 9 | 1 | 1 | 2 | |||||||
| 10 | ||||||||||
| 11 | 1 | 1 | ||||||||
| 12 | ||||||||||
| 13 | 1 | 1 | ||||||||
| n | 1 | 1 | 1 | 3 | 2 | 14 | 17 | 31 | 13 | 83 |
| a. Ranking of Pink Esthetic Outcomes: PES Score (Scale 0–14) N = 83 | ||||
|---|---|---|---|---|
| Excellent PES 12–14 | Acceptable PES 8–11 | Inadequate PES 0–7 | ||
| 0 year (T0) | 33% | 48% | 19% | |
| 1 year (T3) | 69% | 30% | 1% | |
| 3 year (T4) | 72% | 26% | 2% | |
| b. Overall Esthetic Outcome: Original PES Score and WES N = 83 | ||||
| Excellent PES ≥ 12/WES≥9 | Good PES ≥ 10/WES ≥ 8 | Acceptable PES ≥ 8/WES ≥ 6 | Inadequate PES < 8/WES < 6 | |
| 0 year (T0) | 8% | 5% | 20% | 67% |
| 1 year (T3) | 37% | 37% | 20% | 6% |
| 3 year (T4) | 40% | 35% | 19% | 6% |
| PES | |||
|---|---|---|---|
| Effect | 95% CI | p | |
| Intercept | 11.79 | [9.82…13.78] | 0.00 * |
| Preoperative esthetics (T0-PES) | 0.06 | [−0.03…0.15] | 0.20 |
| Smoking | −0.12 | [−0.74…0.50] | 0.73 |
| Post-extraction bone defect (mm) | 0.04 | [−0.06…0.13] | 0.44 |
| Implant location (lateral vs. central) | −0.85 | [−1.30…−0.40] | 0.00 * |
| Gap size (mm) | −0.41 | [−0.67…−0.15] | 0.01 * |
| Crown (cemented vs. screwed) | 0.19 | [−0.31…0.68] | 0.48 |
| Emergence profile (convex vs. concave) | −1.26 | [−1.76…−0.76] | 0.00 * |
| Complication | −0.59 | [−1.20…0.02] | 0.07 |
| Time | 1.93 | [1.18…2.68] | 0.00 * |
| Time2 | −0.27 | [−0.42…−0.12] | 0.00 * |
| modPES | |||
| Effect | 95% CI | p | |
| Intercept | 8.30 | [6.68…9.94] | 0.00 * |
| Preoperative esthetics (T0-modPES) | 0.11 | [0.01…0.20] | 0.05 |
| Smoking | 0.02 | [−0.50…0.54] | 0.94 |
| Post-extraction bone defect (mm) | 0.06 | [−0.02…0.13] | 0.16 |
| Implant location (lateral vs. central) | −0.57 | [−0.94…−0.20] | 0.01 * |
| Gap size (mm) | −0.29 | [−0.51…−0.08] | 0.01 * |
| Crown (cemented vs. screwed) | 0.11 | [−0.30…0.51] | 0.61 |
| Emergence profile (convex vs. concave) | −0.82 | [−1.23…−0.41] | 0.00 * |
| Complication | −0.66 | [−1.16…−0.16] | 0.02 |
| Time | 1.01 | [0.36…1.66] | 0.00 * |
| Time2 | −0.13 | [−0.26…−0.00] | 0.05 |
| WES | |||
| Effect | 95% CI | p | |
| Intercept | 4.78 | [3.20…6.36] | 0.00 * |
| Preoperative esthetics (T0-WES) | 0.09 | [0.02…0.16] | 0.02 |
| Smoking | −0.28 | [−0.85…0.29] | 0.36 |
| Post-extraction bone defect (mm) | 0.01 | [−0.08…0.09] | 0.83 |
| Implant location (lateral vs. central) | −0.27 | [−0.69…0.16] | 0.24 |
| Gap size (mm) | 0.01 | [−0.24…0.25] | 0.97 |
| Final crown (cemented vs. screwed) | 0.57 | [0.12…1.01] | 0.02 |
| Emergence profile (convex vs. concave) | −0.68 | [−1.14…−0.23] | 0.01 * |
| Complication | −0.19 | [−0.74…0.37] | 0.53 |
| Time is >1 | 3.44 | [3.10…3.77] | 0.00 * |
| a. Comparable IIP Studies | ||||||
|---|---|---|---|---|---|---|
| Study | N | Socket | Implant | Implant Position | Esthetic Outcome | Other |
| Cosyn et al. [26] | 25 | Intact | Nobel Replace | H: 1 mm P V: 1 mm A | 3-year results: PES = 10.5/WES = 8.2 | PES: 16% inadequate |
| Cosyn et al. [29] | 17 | Intact | Nobel Active | H: 1 mm P V: 1 mm A | 1-year: PES = 12.2 5-year: PES = 11.2 | MB recession: 47% |
| Seyssens et al. [37] | 18 | Intact | Nobel Active | H: 1 mm P V: 1 mm A | 10-year results: PES = 10.6 | MB recession: 33% advanced |
| Slagter et al. [24] | 20 | Intact | Nobel Active | H: 1 mm P V: ≥3 mm A | 5-year results: PES = 7.8/WES = 7.5 | MB recession: mean 1.44 mm |
| b. Comparable Studies with Different Treatment Timing | ||||||
| Study | N + Timing | Implant Position | Healing Protocol | Esthetic Outcome | ||
| Raes et al. [46] | 15 IIP 23 DIP | H: 1 mm P V: 1 mm A | temp crown | 1-year results: IIP: PES = 10.3 DIP: PES = 9.7 | ||
| Buser et al. [17] | 20 EIP | H: 1 mm P V: 1 mm A | submerged | 3-year results: modPES = 8.1 WES = 8.7 | ||
| Buser et al. [19] | 41 EIP | H: 1 mm P V: 1 mm A | submerged | 5-year results: modPES = 7.8/WES = 7 9-year results: modPES = 7.5/WES = 6.9 | ||
| Felice et al. [30] | 25 IIP 25 RP and DIP | H: 1.5 mm P V: 4–5 mm MB | temp crown | 1-year results: IIP: PES = 12.8/ DIP: PES = 12.2 | ||
| Tonetti et al. [25] | 58 IIP 57 DIP | not reported | submerged IIP: 62% DIP: 82% | 1-year IIP: modPES ≈ 7 42% inadequate 1-year DIP: modPES ≈ 8 19% inadequate | ||
| Arora and Ivanovski [35] | 15 IIP 15 EIP | H: 1 mm P V: 1 mm | healing abutment | 1-year post crown: IIP: PES = 9.4 EIP: PES = 9.3 | ||
| Raes et al. [47] | 11 IIP 18 DIP | H: 1 mm P V: 1 mm | temp crown | >8-year results: IIP: PES = 10.4 DIP: PES = 9.2 | ||
| Meijndert et al. [20] | 50 DIP | H: 1 mm PV: 1 mm | submerged | 1- and 5-year results: modPES = 6.9 and 6.6 WES = 7.5 and 7.8 | ||
| T0 | T4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frequency | Mean | SD | Frequency | Mean | SD | |||||
| Score | 0 | 1 | 2 | 0 | 1 | 2 | ||||
| PES-3: soft-tissue level | 16 | 29 | 38 | 1.27 | 0.76 | 6 | 20 | 57 | 1.61 | 0.62 |
| PES-5: alveolar process contour | 2 | 16 | 65 | 1.76 | 0.48 | 4 | 24 | 55 | 1.61 | 0.58 |
| Total | 83 | 83 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groenendijk, E.; Staas, T.A.; Bronkhorst, E.M.; Raghoebar, G.M.; Meijer, G.J. Factors Associated with Esthetic Outcomes of Flapless Immediate Placed and Loaded Implants in the Maxillary Incisor Region—Three-Year Results of a Prospective Case Series. J. Clin. Med. 2023, 12, 2625. https://doi.org/10.3390/jcm12072625
Groenendijk E, Staas TA, Bronkhorst EM, Raghoebar GM, Meijer GJ. Factors Associated with Esthetic Outcomes of Flapless Immediate Placed and Loaded Implants in the Maxillary Incisor Region—Three-Year Results of a Prospective Case Series. Journal of Clinical Medicine. 2023; 12(7):2625. https://doi.org/10.3390/jcm12072625
Chicago/Turabian StyleGroenendijk, Edith, Tristan Ariaan Staas, Ewald Maria Bronkhorst, Gerry Max Raghoebar, and Gert Jacobus Meijer. 2023. "Factors Associated with Esthetic Outcomes of Flapless Immediate Placed and Loaded Implants in the Maxillary Incisor Region—Three-Year Results of a Prospective Case Series" Journal of Clinical Medicine 12, no. 7: 2625. https://doi.org/10.3390/jcm12072625