

Development and Validation of the Life for Low Vision Questionnaire (LIFE4LVQ) Using Rasch Analysis: A Questionnaire Evaluating Ability and Independence

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design of the LIFE4LV Questionnaire
- Phase A. Content Development through a literature review and focus groups
- Phase B. Scale Refinement
- Phase C. Psychometric analysis in the LV group
2.3. Rasch Analysis
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Unidimensionality
3.3. Differential Item Functioning (DIF)
3.4. Reliability
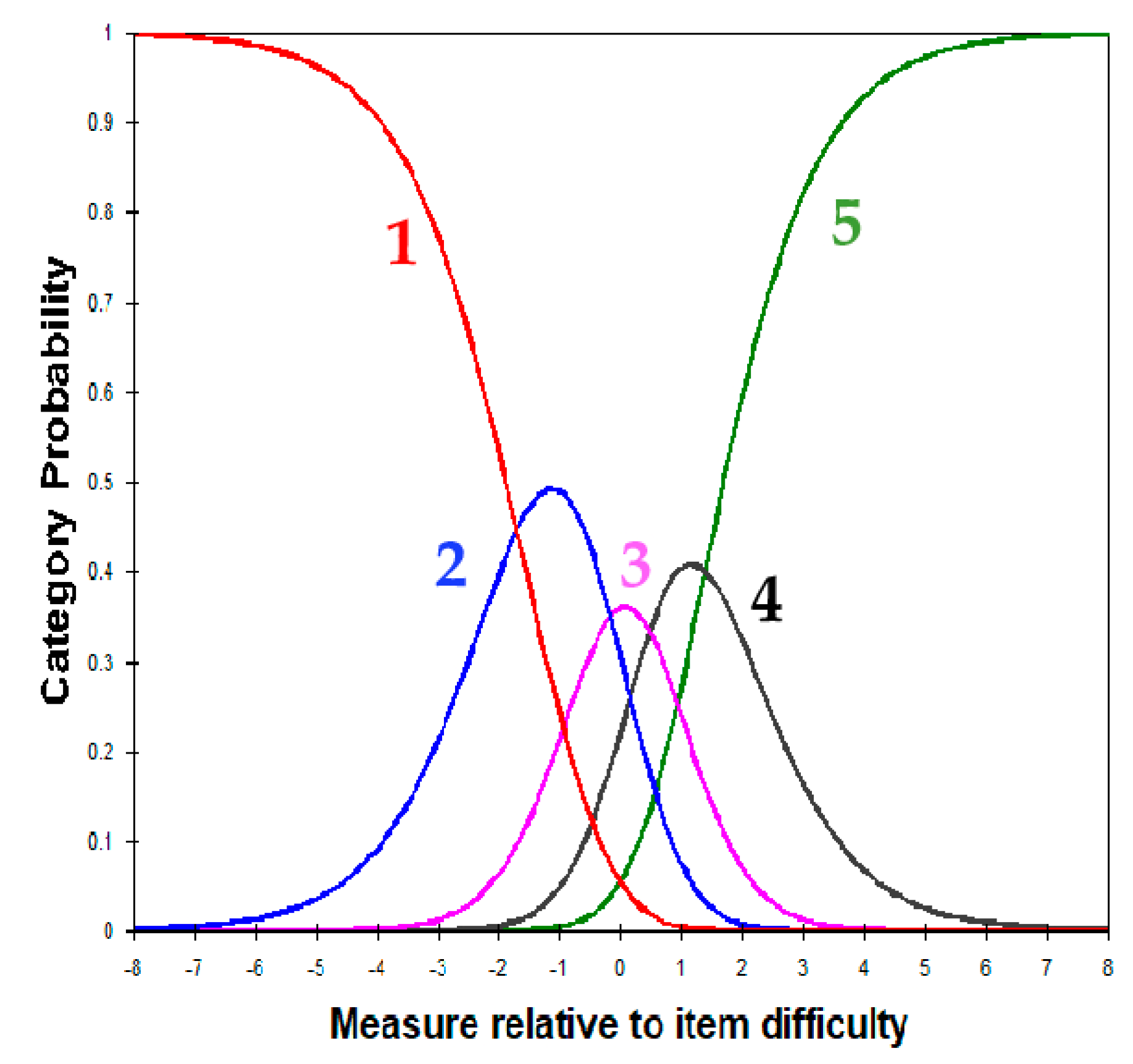
3.5. Response Category Functioning
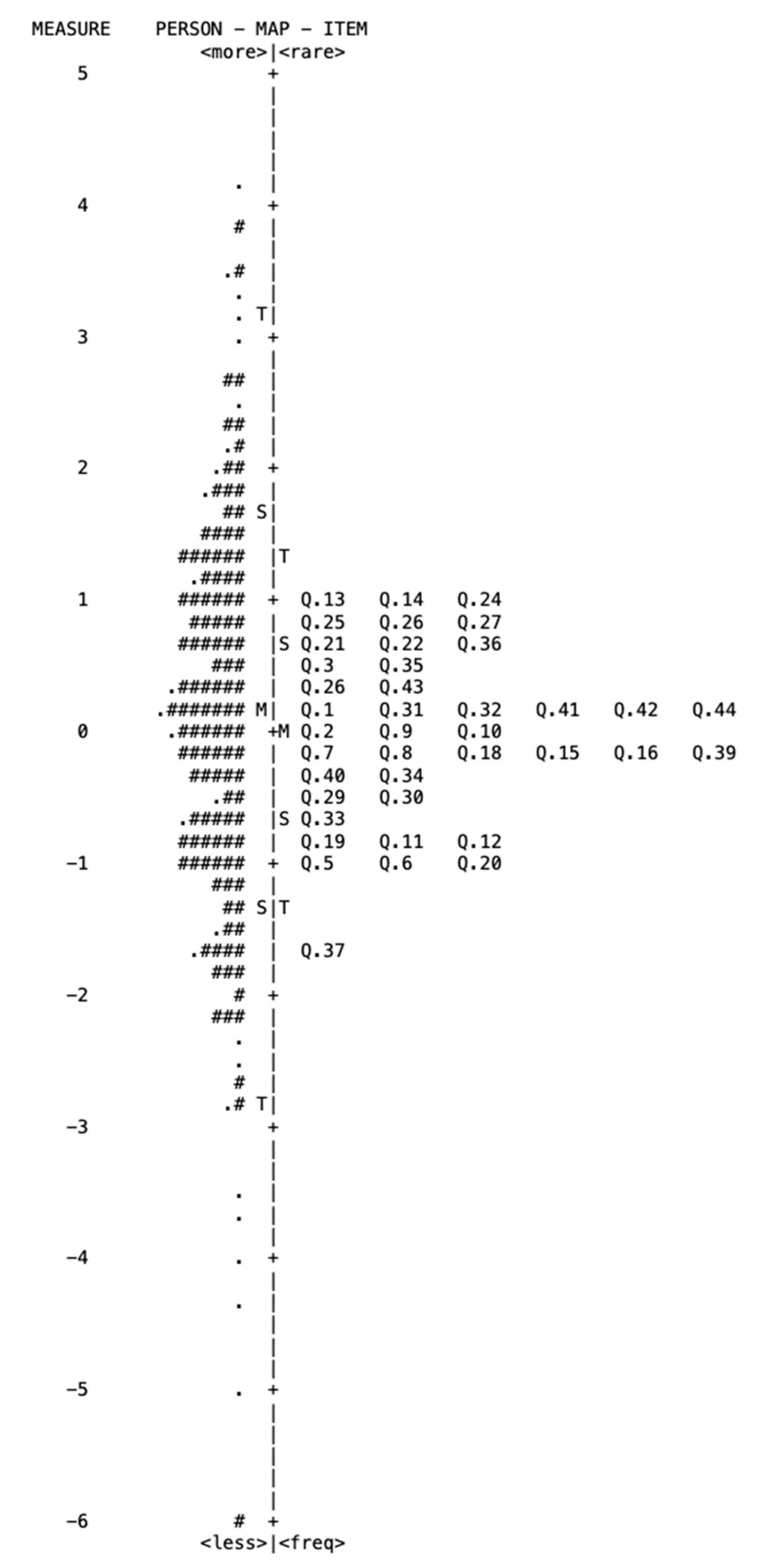
3.6. Person–Item Map
3.7. Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adigun, K.; Oluleye, T.S.; Ladipo, M.M.; Olowookere, S.A. Quality of life in patients with visual impairment in Ibadan: A clinical study in primary care. J. Multidiscip. Healthc. 2014, 7, 173–178. [Google Scholar] [PubMed] [Green Version]
- World Health Organization. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease; World Health Organization: Geneva, Switzerland, 1980; Available online: http://apps.who.int/iris/bitstream/10665/41003/1/9241541261_eng.pdf (accessed on 14 October 2021).
- Pascolini, D.; Mariotti, S.P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 2012, 96, 614–618. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.; Friedman, D.S.; Bradley, C.; Massof, R. Estimates of Incidence and Prevalence of Visual Impairment, Low Vision, and Blindness in the United States. JAMA Ophthalmol. 2018, 136, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Khoo, K.; Man, R.E.K.; Rees, G.; Gupta, P.; Lamoureux, E.L.; Fenwick, E.K. The relationship between diabetic retinopathy and psychosocial functioning: A systematic review. Qual. Life Res. 2019, 28, 2017–2039. [Google Scholar] [CrossRef]
- Mitchell, J.; Bradley, C. Quality of life in age-related macular degeneration: A review of the literature. Health Qual. Life Outcomes 2006, 4, 97. [Google Scholar] [CrossRef] [Green Version]
- Forshaw, T.R.J.; Parpounas, A.K.; Sørensen, T.L. Correlation of macular sensitivity measures and visual acuity to vision-related quality of life in patients with age-related macular degeneration. BMC Ophthalmol. 2021, 21, 149. [Google Scholar] [CrossRef]
- Colenbrander, A. Assessment of functional vision and its rehabilitation. Acta Ophthalmol. 2010, 88, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Colenbrander, A. Visual functions and functional vision. Int. Congr. Ser. 2005, 1282, 482–486. [Google Scholar] [CrossRef]
- Haymes, S.A.; Johnston, A.W.; Heyes, A.D. A weighted version of the Melbourne Low-Vision ADL Index: A measure of disability impact. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2001, 78, 565–579. [Google Scholar] [CrossRef]
- Sørensen, M.S.; Andersen, S.; Henningsen, G.O.; Larsen, C.T.; Sørensen, T.L. Danish version of visual function Questionnaire-25 and its use in age-related macular degeneration. Dan. Med. Bull. 2011, 58, A4290. [Google Scholar]
- Pesudovs, K.; Burr, J.M.; Harley, C.; Elliott, D.B. The development, assessment, and selection of questionnaires. Optom. Vis. Sci. 2007, 84, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Whitcomb, J.J. Functional Status Versus Quality of Life. Adv. Nurs. Sci. 2011, 34, 97–105. [Google Scholar] [CrossRef]
- World Health Organization. Division of Mental Health and Prevention of Substance Abuse. WHOQOL Measuring Quality of Life. Available online: https://apps.who.int/iris/handle/10665/63482 (accessed on 24 November 2021).
- Wan, Y.; Zhao, L.; Huang, C.; Xu, Y.; Sun, M.; Yang, Y.; An, L.; Lv, S.; Yu, Y.; Chen, D.; et al. Validation and comparison of the National Eye Institute Visual Functioning Questionnaire-25 (NEI VFQ-25) and the Visual Function Index-14 (VF-14) in patients with cataracts: A multicentre study. Acta Ophthalmol. 2021, 99, e480–e488. [Google Scholar] [CrossRef] [PubMed]
- de Boer, M.R.; Moll, A.C.; de Vet, H.C.; Terwee, C.B.; Völker-Dieben, H.J.; van Rens, G.H. Psychometric properties of vision-related quality of life questionnaires: A systematic review. Ophthalmic Physiol. Opt. 2004, 24, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Revicki, D.A.; Rentz, A.M.; Harnam, N.; Thomas, V.S.; Lanzetta, P. Reliability and validity of the National Eye Institute Visual Function Questionnaire-25 in patients with age-related macular degeneration. Investg. Ophthalmol. Vis. Sci. 2010, 51, 712–717. [Google Scholar] [CrossRef] [Green Version]
- Chiang, P.P.; Fenwick, E.; Marella, M.; Finger, R.; Lamoureux, E. Validation and reliability of the VF-14 questionnaire in a German population. Investg. Ophthalmol. Vis. Sci. 2011, 52, 8919–8926. [Google Scholar] [CrossRef] [Green Version]
- Khadka, J.; McAlinden, C.; Pesudovs, K. Quality assessment of ophthalmic questionnaires: Review and recommendations. Optom. Vis. Sci. 2013, 90, 720–744. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Brost, M.A.; Horton, V.E.; Kenyon, S.B.; Mears, K.E. Occupational therapy interventions to improve performance of daily activities at home for older adults with low vision: A systematic review. Am. J. Occup. Ther. 2013, 67, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Pesudovs, K.; Gothwal, V.K.; Wright, T.; Lamoureux, E.L. Remediating serious flaws in the National Eye Institute Visual Function Questionnaire. J. Cataract. Refract. Surg. 2010, 36, 718–732. [Google Scholar] [CrossRef]
- Wu, Y.H.; Granquist, C.; Gage, R.; Crossland, M.D.; Legge, G.E. Online Survey of Digital Reading by Adults with Low Vision. Optom. Vis. Sci. 2020, 97, 249–256. [Google Scholar] [CrossRef]
- Massof, R.W.; Hsu, C.T.; Baker, F.H.; Barnett, G.D.; Park, W.L.; Deremeik, J.T.; Rainey, C.; Epstein, C. Visual disability variables. I: The importance and difficulty of activity goals for a sample of low-vision patients. Arch. Phys. Med. Rehabil. 2005, 86, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Sloane, M.E.; Ball, K.; Owsley, C.; Bruni, J.R.; Roenker, D.L. The visual activities questionnaire: Developing an instrument for assessing problems in everyday visual tasks. Tech. Dig. Noninvasive Assess. Vis. Syst. 1992, 1, 26–29. [Google Scholar]
- Andrich, D.A. A rating scale formulation for ordered response categories. Psychometrika 1978, 43, 561–573. [Google Scholar] [CrossRef]
- Boone, W.J. Rasch Analysis for Instrument Development: Why, When, and How? CBE Life Sci. Educ. 2016, 15, rm4. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, D.W. Comparing Rasch measurement and factor analysis. Struct. Equ. Model. A Multidiscip. J. 1996, 3, 3–24. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini Mental State Examination (MMSE): A validation study in Greece. Am. J. Alzheimer’s Dis. Other Dement. 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Paz, S.H.; Slotkin, J.; McKean-Cowdin, R.; Lee, P.; Owsley, C.; Vitale, S.; Varma, R.; Gershon, R.; Hays, R.D. Development of a vision-targeted health-related quality of life item measure. Qual. Life Res. 2013, 22, 2477–2487. [Google Scholar] [CrossRef] [Green Version]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Brown, J.C.; Goldstein, J.E.; Chan, T.L.; Massof, R.; Ramulu, P.; Low Vision Research Network Study Group. Characterizing functional complaints in patients seeking outpatient low-vision services in the United States. Ophthalmology 2014, 121, 1655–1662.e1. [Google Scholar] [CrossRef]
- Owsley, C.; McGwin, G., Jr. Vision-targeted health related quality of life in older adults: Patient-reported visibility problems in low luminance activities are more likely to decline than daytime activities. BMC Ophthalmol. 2016, 16, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangione, C.M.; Berry, S.; Spritzer, K.; Janz, N.K.; Klein, R.; Owsley, C.; Lee, P.P. Identifying the content area for the 51-item National Eye Institute Visual Function Questionnaire: Results from focus groups with visually impaired persons. Arch. Ophthalmol. 1998, 116, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Mangione, C.M.; Lee, P.P.; Pitts, J.; Gutierrez, P.; Berry, S.; Hays, R.D. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). NEI-VFQ Field Test Investigators. Arch. Ophthalmol. 1998, 116, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Mangione, C.M.; Lee, P.P.; Gutierrez, P.R.; Spritzer, K.; Berry, S.; Hays, R.D.; National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch. Ophthalmol. 2001, 119, 1050–1058. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Cochrane, A.L. Design of the low vision quality-of-life questionnaire (LVQOL) and measuring the outcome of low-vision rehabilitation. Am. J. Ophthalmol. 2000, 130, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.; Bradley, C. Design of an individualised measure of the impact of macular disease on quality of life (the MacDQoL). Qual. Life Res. 2004, 13, 1163–1175. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, E.P.; Tielsch, J.M.; Schein, O.D.; Javitt, J.C.; Sharkey, P.; Cassard, S.D.; Legro, M.W.; Diener-West, M.; Bass, E.B.; Damiano, A.M.; et al. The VF-14. An index of functional impairment in patients with cataract. Arch. Ophthalmol. 1994, 112, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Linder, M.; Chang, T.S.; Scott, I.U.; Hay, D.; Chambers, K.; Sibley, L.M.; Weis, E. Validity of the visual function index (VF-14) in patients with retinal disease. Arch. Ophthalmol. 1999, 117, 1611–1616. [Google Scholar] [CrossRef] [Green Version]
- Mangione, C.M.; Phillips, R.S.; Seddon, J.M.; Lawrence, M.G.; Cook, E.F.; Dailey, R.; Goldman, L. Development of the ‘Activities of Daily Vision Scale’. A measure of visual functional status. Med. Care 1992, 30, 1111–1126. [Google Scholar] [CrossRef]
- Pesudovs, K.; Garamendi, E.; Keeves, J.P.; Elliott, D.B. The Activities of Daily Vision Scale for cataract surgery outcomes: Re-evaluating validity with Rasch analysis. Investg. Ophthalmol. Vis. Sci. 2003, 44, 2892–2899. [Google Scholar] [CrossRef] [Green Version]
- Owsley, C.; McGwin, G., Jr.; Scilley, K.; Kallies, K. Development of a questionnaire to assess vision problems under low luminance in age-related maculopathy. Investg. Ophthalmol. Vis. Sci. 2006, 47, 528–535. [Google Scholar] [CrossRef] [Green Version]
- Lamoureux, E.L.; Hassell, J.B.; Keeffe, J.E. The determinants of participation in activities of daily living in people with impaired vision. Am. J. Ophthalmol. 2004, 137, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, E.L.; Hassell, J.B.; Keeffe, J.E. The impact of diabetic retinopathy on participation in daily living. Arch. Ophthalmol. 2004, 122, 84–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassell, J.B.; Lamoureux, E.L.; Keeffe, J.E. Impact of age-related macular degeneration on quality of life. Br. J. Ophthalmol. 2006, 90, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A practical Guide to Their Development and Use, 5th ed.; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Jobe, J.B.; Mingay, D.J. Cognitive research improves questionnaires. Am. J. Public Health 1989, 79, 1053–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasch, G. Probabilistic Models for Some Intelligence and Attainment Tests; University of Chicago Press: Chicago, IL, USA, 1960. [Google Scholar]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Sciences, 2nd ed.; Routledge: New York, NY, USA, 2007. [Google Scholar]
- Prieto, L.; Alonso, J.; Lamarca, R. Classical Test Theory versus Rasch analysis for quality of life questionnaire reduction. Health Qual. Life Outcomes 2003, 1, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linacre, J.M. Optimizing rating scale category effectiveness. J. Appl. Meas. 2002, 3, 85–106. [Google Scholar] [PubMed]
- Linacre, J. What do Infit and Outfit, meansquare and standardized mean? Rasch Meas. Trans. 2002, 16, 878. [Google Scholar]
- Cacho-Martínez, P.; Cantó-Cerdán, M.; Lara-Lacárcel, F.; García-Muñoz, Á. Validation of the symptom questionnaire for visual dysfunctions (SQVD): A questionnaire to evaluate symptoms of any type of visual dysfunctions. Transl. Vis. Sci. Technol. 2022, 11, 7. [Google Scholar] [CrossRef]
- Linacre, J.M. Winsteps® Rasch Measurement Computer Program (Version 5.1.7). Portland, Oregon. 2021. Available online: Winsteps.com (accessed on 10 January 2022).
- Holland, P.W.; Wainer, H. Differential item functioning. In Differential Item Functioning; Holland, P.W., Weiner, H., Eds.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1993. [Google Scholar]
- Available online: https://www.rasch.org/rmt/rmt131a.htm (accessed on 20 January 2022).
- Labiris, G.; Katsanos, A.; Fanariotis, M.; Tsirouki, T.; Pefkianaki, M.; Chatzoulis, D.; Tsironi, E. Psychometric properties of the Greek version of the NEI-VFQ 25. BMC Ophthalmol. 2008, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163, Erratum in: J. Chiropr. Med. 2017, 16, 346. [Google Scholar] [CrossRef] [Green Version]
- Almpanidou, S.; Almaliotis, D.; Karamitopoulos, L.; Topouzis, F.; Labiris, G.; Karampatakis, V. Causes of low vision in a Greek population. Acta Ophthalmol. 2021, 99, S265. [Google Scholar] [CrossRef]
- Zheng, Y.; Lamoureux, E.L.; Chiang, P.P.; Cheng, C.Y.; Anuar, A.R.; Saw, S.M.; Aung, T.; Wong, T.Y. Literacy is an independent risk factor for vision impairment and poor visual functioning. Investg. Ophthalmol. Vis. Sci. 2011, 52, 7634–7639. [Google Scholar] [CrossRef]
- Stelmack, J.A.; Stelmack, T.R.; Massof, R.W. Measuring low-vision rehabilitation outcomes with the NEI VFQ-25. Investg. Ophthalmol. Vis. Sci. 2002, 43, 2859–2868. [Google Scholar]
- Stelmack, J.A.; Szlyk, J.P.; Stelmack, T.R.; Demers-Turco, P.; Williams, R.T.; D’Anna, M.; Massof, R.W. Psychometric Properties of the Veterans Affairs Low-Vision Visual Functioning Questionnaire. Investg. Ophthalmol. Vis. Sci. 2004, 45, 3919–3928. [Google Scholar] [CrossRef]
- Marella, M.; Pesudovs, K.; Keeffe, J.E.; O’Connor, P.M.; Rees, G.; Lamoureux, E.L. The Psychometric Validity of the NEI VFQ-25 for Use in a Low-Vision Population. Investg. Ophthalmol. Vis. Sci. 2010, 51, 2878–2884. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, J.; Bressler, N.M.; Lamoureux, E.; Ferreira, A.; Cano, S. Development of a new Rasch-based scoring algorithm for the National Eye Institute Visual Functioning Questionnaire to improve its interpretability. Health Qual. Life Outcomes 2017, 15, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finger, R.P.; Fenwick, E.; Pesudovs, K.; Marella, M.; Lamoureux, E.L.; Holz, F.G. Rasch analysis reveals problems with multiplicative scoring in the macular disease quality of life questionnaire. Ophthalmology 2012, 119, 2351–2357. [Google Scholar] [CrossRef] [PubMed]
- van Nispen, R.M.; Knol, D.L.; Langelaan, M.; van Rens, G.H. Re-evaluating a vision-related quality of life questionnaire with item response theory (IRT) and differential item functioning (DIF) analyses. BMC Med. Res. Methodol. 2011, 11, 125. [Google Scholar] [CrossRef] [Green Version]
- Berndt, A.E. Sampling Methods. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2020, 36, 224–226. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Daily Activities | Ν (%) |
|---|---|
| Technology-Communication | 32 (29.1) |
| Cooking | 43 (39.1) |
| Watching Television (TV) | 27 (24.5) |
| Self-care | 27 (24.5) |
| Social functioning | 38 (34.5) |
| Housekeeping | 39 (35.5) |
| Reading ‡ | 47 (42.3) |
| Books/Hardcopies | 32 (68.1) |
| Digital Texts | 29 (61.7) |
| Labels | 22 (46.8) |
| Prices | 19 (40.4) |
| Bills | 12 (25.5) |
| Subtitles | 11 (23.4) |
| Going out/Walking | 39 (35.5) |
| Public Transport use | 24 (21.8) |
| Sex life | 2 (1.8) |
| Travelling | 12 (10.1) |
| Spirituality-Praying | 3 (2.7) |
| Shopping | 22 (20) |
| Family | 12 (10.1) |
| Gardening | 12 (10.1) |
| Work/Education | 28 (25.5) |
| Pets | 4 (3.6) |
| Needlecraft | 4 (3.6) |
| Driving | 6 (5.5) |
| Watching Theater | 2 (1.8) |
| Volunteering | 2 (1.8) |
| Flirting | 12 (10.1) |
| Low Vision N = 252 (%) | Legally Blind N = 22 (%) | Mild Visual Impairment N = 20 (%) | p * | |
|---|---|---|---|---|
| Age group, N (%) | 0.005 | |||
| <55 | 35 (13.5) | 8 (36.4) | 1 (5) | |
| 55–74 | 92 (38.5) | 6 (27.2) | 9 (45) | |
| ≥75 | 125 (48) | 8 (36.4) | 10 (50) | |
| Gender, females, N (%) | 129 (50.4) | 10 (45.5) | 11 (61.1) | 0.676 |
| Educational level, Ν (%) | 0.816 | |||
| Primary | 150 (59.5) | 12 (54.5) | 7 (46.7) | |
| Lower and upper secondary | 53 (21) | 7 (31.8) | 11 (40) | |
| Higher | 49 (19.4) | 3 (13.6) | 2 (13.3) | |
| General health (mean (SD), range) | 6.31 (2.16), 0–10 | 5.86 (2.76), 1–10 | 6.30 (1.92), 2–9 | 0.652 |
| General vision (mean (SD), range) | 4.88 (1.89), 0–9 | 2.68 (2.23), 0–8 | 6.10 (1.62), 2–8 | <0.001 |
| BCVA of the better-seeing eye (logMAR, mean (SD), range) | 0.70 (0.27), 0.5–1.3 | 1.53 (0.09), 1.3–1.6 | 0.16 (0.13), 0.0–0.4 | |
| Ocular disease, Ν (%) | ||||
| Age-related Macular Degeneration (AMD) | 106 (42) | |||
| Diabetic Retinopathy (DR) | 62 (24.6) | |||
| Glaucoma | 29 (11.5) | |||
| Retinitis Pigmentosa (RP) | 13 (5.2) | |||
| Other | 42 (16.6) |
| Items | Measure | SE | Infit MNSQ | Outfit MNSQ | Age DIF Contrast a * | Gender DIF Contrast a |
|---|---|---|---|---|---|---|
| Shopping (A) | 0.21 | 0.07 | 0.85 | 0.96 | −0.05 | 0.08 |
| Shopping (I) | 0.03 | 0.07 | 1.01 | 0.99 | 0.00 | 0.14 |
| Product recognition (A) | 0.51 | 0.07 | 0.81 | 0.92 | −0.31 | −0.22 |
| Product recognition (I) | 0.38 | 0.07 | 1.04 | 0.97 | −0.32 | −0.24 |
| Price identification (A) | −0.91 | 0.08 | 0.92 | 0.92 | 0.21 | 0.02 |
| Price identification (I) | −0.96 | 0.08 | 1.07 | 0.92 | 0.17 | 0.09 |
| Use of electronic devices (A) | −0.21 | 0.08 | 1.07 | 1.07 | 0.35 | −0.24 |
| Use of electronic devices (I) | −0.14 | 0.08 | 1.28 | 1.19 | 0.37 | −0.20 |
| Use of public transport—daytime (A) | 0.09 | 0.08 | 0.81 | 0.78 | 0.04 | 0.24 |
| Use of public transport—daytime (I) | 0.09 | 0.08 | 1.02 | 0.89 | 0.11 | 0.34 |
| Use of public transport—night (A) | −0.84 | 0.08 | 0.87 | 0.83 | 0.20 | 0.42 |
| Use of public transport—night (I) | −0.77 | 0.08 | 1.24 | 1.08 | 0.22 | 0.36 |
| Walking in familiar places—daytime (A) | 1.02 | 0.08 | 0.73 | 0.73 | 0.15 | 0.20 |
| Walking in familiar places—daytime (I) | 0.98 | 0.08 | 1.06 | 0.99 | 0.02 | 0.27 |
| Walking in familiar places—night (A) | −0.2 | 0.07 | 1.03 | 1.02 | −0.06 | 0.23 |
| Walking in familiar places—night (I) | −0.18 | 0.07 | 1.3 | 1.17 | 0.00 | 0.47 |
| Walking in unfamiliar places—daytime (I) | −0.15 | 0.07 | 0.87 | 0.77 | 0.00 | 0.19 |
| Walking in unfamiliar places—night (A) | −0.9 | 0.08 | 0.99 | 1.03 | −0.24 | 0.23 |
| Walking in unfamiliar places—night (I) | −0.98 | 0.08 | 1.24 | 1.17 | −0.10 | 0.44 |
| Noticing objects around (A) | 0.72 | 0.07 | 1.1 | 1.17 | −0.49 | −0.11 |
| Noticing objects around (I) | 0.73 | 0.07 | 1.17 | 1.06 | −0.60 | −0.10 |
| Preparing meals and drinks (I) | 0.96 | 0.08 | 0.99 | 0.86 | −0.06 | −0.06 |
| Matching clothes according to color (A) | 0.9 | 0.08 | 0.91 | 0.95 | 0.00 | −0.41 |
| Matching clothes according to color (I) | 0.88 | 0.08 | 1.21 | 1.12 | 0.05 | −0.65 |
| Self-care (A) | 0.79 | 0.07 | 1.22 | 1.3 | −0.29 | −0.43 |
| Reading relatively large letters in formal texts (A) | −0.42 | 0.07 | 1.09 | 0.97 | 0.38 | 0.08 |
| Reading relatively large letters in formal texts (I) | −0.48 | 0.07 | 1.3 | 1.13 | 0.41 | 0.00 |
| Working/Studying (A) | 0.1 | 0.08 | 0.86 | 0.91 | −0.22 | −0.28 |
| Working/Studying (I) | 0.09 | 0.08 | 0.92 | 1.08 | −0.24 | −0.16 |
| Reading relatively large letters in magazines etc. (A) | −0.58 | 0.08 | 1.11 | 1.08 | 0.56 | 0.06 |
| Reading relatively large letters in magazines etc. (I) | −0.36 | 0.08 | 1.22 | 1.02 | 0.44 | 0.13 |
| Watching television (A) | 0.46 | 0.07 | 1.04 | 1.06 | 0.15 | −0.11 |
| Watching television (I) | 0.71 | 0.08 | 1.03 | 0.97 | 0.15 | 0.00 |
| Reading subtitles (A) | −1.72 | 0.09 | 1.13 | 0.92 | 0.00 | −0.02 |
| Traveling (A) | −0.14 | 0.08 | 0.74 | 0.75 | 0.26 | −0.18 |
| Traveling (I) | −0.3 | 0.08 | 1.01 | 0.9 | 0.08 | 0.06 |
| Recognizing faces/reactions (A) | 0.08 | 0.07 | 0.91 | 0.94 | −0.08 | −0.38 |
| Recognizing faces/reactions (I) | 0.12 | 0.07 | 0.94 | 1.0 | −0.20 | −0.33 |
| Social life (A) | 0.25 | 0.07 | 0.75 | 0.7 | −0.25 | 0.00 |
| Social life (I) | 0.14 | 0.07 | 1.03 | 0.89 | −0.45 | 0.18 |
| LIFE4LVQ Response Categories | Count | Average Measure | Infit MNSQ | Outfit MNSQ | Andrich Threshold |
|---|---|---|---|---|---|
| 1 | 2112 | −1.73 | 1.20 | 1.19 | None |
| 2 | 1963 | −0.80 | 0.88 | 0.87 | −1.18 |
| 3 | 1570 | 0.04 | 0.88 | 0.78 | −0.11 |
| 4 | 1866 | 0.85 | 0.93 | 0.90 | 0.26 |
| 5 | 2418 | 1.81 | 1.11 | 1.12 | 1.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almpanidou, S.; Almaliotis, D.; Karamitopoulos, L.; Topouzis, F.; Konstas, A.-G.; Labiris, G.; Dardavesis, T.; Fountoulakis, K.N.; Chatzisavvas, K.C.; Karampatakis, V. Development and Validation of the Life for Low Vision Questionnaire (LIFE4LVQ) Using Rasch Analysis: A Questionnaire Evaluating Ability and Independence. J. Clin. Med. 2023, 12, 2549. https://doi.org/10.3390/jcm12072549
Almpanidou S, Almaliotis D, Karamitopoulos L, Topouzis F, Konstas A-G, Labiris G, Dardavesis T, Fountoulakis KN, Chatzisavvas KC, Karampatakis V. Development and Validation of the Life for Low Vision Questionnaire (LIFE4LVQ) Using Rasch Analysis: A Questionnaire Evaluating Ability and Independence. Journal of Clinical Medicine. 2023; 12(7):2549. https://doi.org/10.3390/jcm12072549
Chicago/Turabian StyleAlmpanidou, Stavroula, Diamantis Almaliotis, Leonidas Karamitopoulos, Fotios Topouzis, Anastasios-Georgios Konstas, Georgios Labiris, Theodoros Dardavesis, Konstantinos N. Fountoulakis, Konstantinos Ch. Chatzisavvas, and Vasileios Karampatakis. 2023. "Development and Validation of the Life for Low Vision Questionnaire (LIFE4LVQ) Using Rasch Analysis: A Questionnaire Evaluating Ability and Independence" Journal of Clinical Medicine 12, no. 7: 2549. https://doi.org/10.3390/jcm12072549