
Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery

Abstract
:1. Coronary Revascularization Procedures
2. Total Arterial Revascularization
3. Bilateral Internal Mammary Artery Grafting
4. Radial Artery Grafting
5. Multi-Arterial Grafting
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction; Thygesen, K.; Alpert, J.S. Third universal definition of myocardial infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef] [PubMed]
- Farkouh, M.E.; Domanski, M.; Sleeper, L.A.; Siami, F.S.; Dangas, G.; Mack, M.; Yang, M.; Cohen, D.J.; Rosenberg, Y.; Solomon, S.D.; et al. Strategies for multivessel revascularization in patients with diabetes. N. Engl. J. Med. 2012, 367, 2375–2384. [Google Scholar] [CrossRef] [Green Version]
- Serruys, P.W.; Morice, M.C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Ståhle, E.; Feldman, T.E.; van den Brand, M.; Bass, E.J.; et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 360, 961–972. [Google Scholar] [CrossRef]
- Javaid, A.; Steinberg, D.H.; Buch, A.N.; Corso, P.J.; Boyce, S.W.; Pinto Slottow, T.L.; Roy, P.K.; Hill, P.; Okabe, T.; Torguson, R.; et al. Outcomes of coronary artery bypass grafting versus percutaneous coronary intervention with drug-eluting stents for patients with multivessel coronary artery disease. Circulation 2007, 116, I200–I206. [Google Scholar] [CrossRef] [Green Version]
- Caldonazo, T.; Kirov, H.; Riedel, L.L.; Gaudino, M.; Doenst, T. Comparing CABG and PCI across the globe based on current regional registry evidence. Sci. Rep. 2022, 12, 22164. [Google Scholar] [CrossRef]
- Mohr, F.W.; Morice, M.C.; Kappetein, A.P.; Feldman, T.E.; Ståhle, E.; Colombo, A.; Mack, M.J.; Holmes, D.R., Jr.; Morel, M.A.; Van Dyck, N.; et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet 2013, 381, 629–638. [Google Scholar] [CrossRef]
- Head, S.J.; Milojevic, M.; Daemen, J.; Ahn, J.M.; Boersma, E.; Christiansen, E.H.; Domanski, M.J.; Farkouh, M.E.; Flather, M.; Fuster, V.; et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: A pooled analysis of individual patient data. Lancet 2018, 391, 939–948. [Google Scholar] [CrossRef] [Green Version]
- Gould, K.L.; Johnson, N.P. Physiologic severity of diffuse coronary artery disease: Hidden high risk. Circulation 2015, 131, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Sabatine, M.S.; Bergmark, B.A.; Murphy, S.A.; O'Gara, P.T.; Smith, P.K.; Serruys, P.W.; Kappetein, A.P.; Park, S.J.; Park, D.W.; Christiansen, E.H.; et al. Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: An individual patient data meta-analysis. Lancet 2021, 398, 2247–2257. [Google Scholar] [CrossRef]
- Head, S.J.; Parasca, C.A.; Mack, M.J.; Mohr, F.W.; Morice, M.-C.; Holmes, D.R.; Feldman, T.E.; Dawkins, K.D.; Colombo, A.; Serruys, P.W.; et al. Differences in baseline characteristics, practice patterns and clinical outcomes in contemporary coronary artery bypass grafting in the United States and Europe: Insights from the SYNTAX randomized trial and registry. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2015, 47, 685–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudino, M.; Antoniades, C.; Benedetto, U.; Deb, S.; Di Franco, A.; Di Giammarco, G.; Fremes, S.; Glineur, D.; Grau, J.; He, G.W.; et al. Mechanisms, Consequences, and Prevention of Coronary Graft Failure. Circulation 2017, 136, 1749–1764. [Google Scholar] [CrossRef] [PubMed]
- Harskamp, R.E.; Williams, J.B.; Hill, R.C.; de Winter, R.J.; Alexander, J.H.; Lopes, R.D. Saphenous vein graft failure and clinical outcomes: Toward a surrogate end point in patients following coronary artery bypass surgery? Am. Heart J. 2013, 165, 639–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgibbon, G.M.; Kafka, H.P.; Leach, A.J.; Keon, W.J.; Hooper, G.D.; Burton, J.R. Coronary bypass graft fate and patient outcome: Angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J. Am. Coll. Cardiol. 1996, 28, 616–626. [Google Scholar] [CrossRef] [Green Version]
- Dimitrova, K.R.; Hoffman, D.M.; Geller, C.M.; Dincheva, G.; Ko, W.; Tranbaugh, R.F. Arterial grafts protect the native coronary vessels from atherosclerotic disease progression. Ann. Thorac. Surg. 2012, 94, 475–481. [Google Scholar] [CrossRef]
- Gaudino, M.; Benedetto, U.; Fremes, S.; Ballman, K.; Biondi-Zoccai, G.; Sedrakyan, A.; Nasso, G.; Raman, J.; Buxton, B.; Hayward, P.A.; et al. Association of Radial Artery Graft vs Saphenous Vein Graft with Long-term Cardiovascular Outcomes Among Patients Undergoing Coronary Artery Bypass Grafting. JAMA 2020, 324, 179. [Google Scholar] [CrossRef]
- Benedetto, U.; Raja, S.G.; Albanese, A.; Amrani, M.; Biondi-Zoccai, G.; Frati, G. Searching for the second best graft for coronary artery bypass surgery: A network meta-analysis of randomized controlled trials. Eur. J. Cardiothorac. Surg. 2015, 47, 59–65; discussion 65. [Google Scholar] [CrossRef]
- Cao, C.; Manganas, C.; Horton, M.; Bannon, P.; Munkholm-Larsen, S.; Ang, S.C.; Yan, T.D. Angiographic outcomes of radial artery versus saphenous vein in coronary artery bypass graft surgery: A meta-analysis of randomized controlled trials. J. Thorac. Cardiovasc. Surg. 2013, 146, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Boylan, M.J.; Lytle, B.W.; Loop, F.D.; Taylor, P.C.; Borsh, J.A.; Goormastic, M.; Cosgrove, D.M. Surgical treatment of isolated left anterior descending coronary stenosis. Comparison of left internal mammary artery and venous autograft at 18 to 20 years of follow-up. J. Thorac. Cardiovasc. Surg. 1994, 107, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.; Davis, K.B.; Green, G.; Schaff, H.V. Coronary bypass surgery with internal-thoracic-artery grafts—Effects on survival over a 15-year period. N. Engl. J. Med. 1996, 334, 216–219. [Google Scholar] [CrossRef]
- Loop, F.D.; Lytle, B.W.; Cosgrove, D.M.; Stewart, R.W.; Goormastic, M.; Williams, G.W.; Golding, L.A.; Gill, C.C.; Taylor, P.C.; Sheldon, W.C.; et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N. Engl. J. Med. 1986, 314, 1–6. [Google Scholar] [CrossRef] [PubMed]
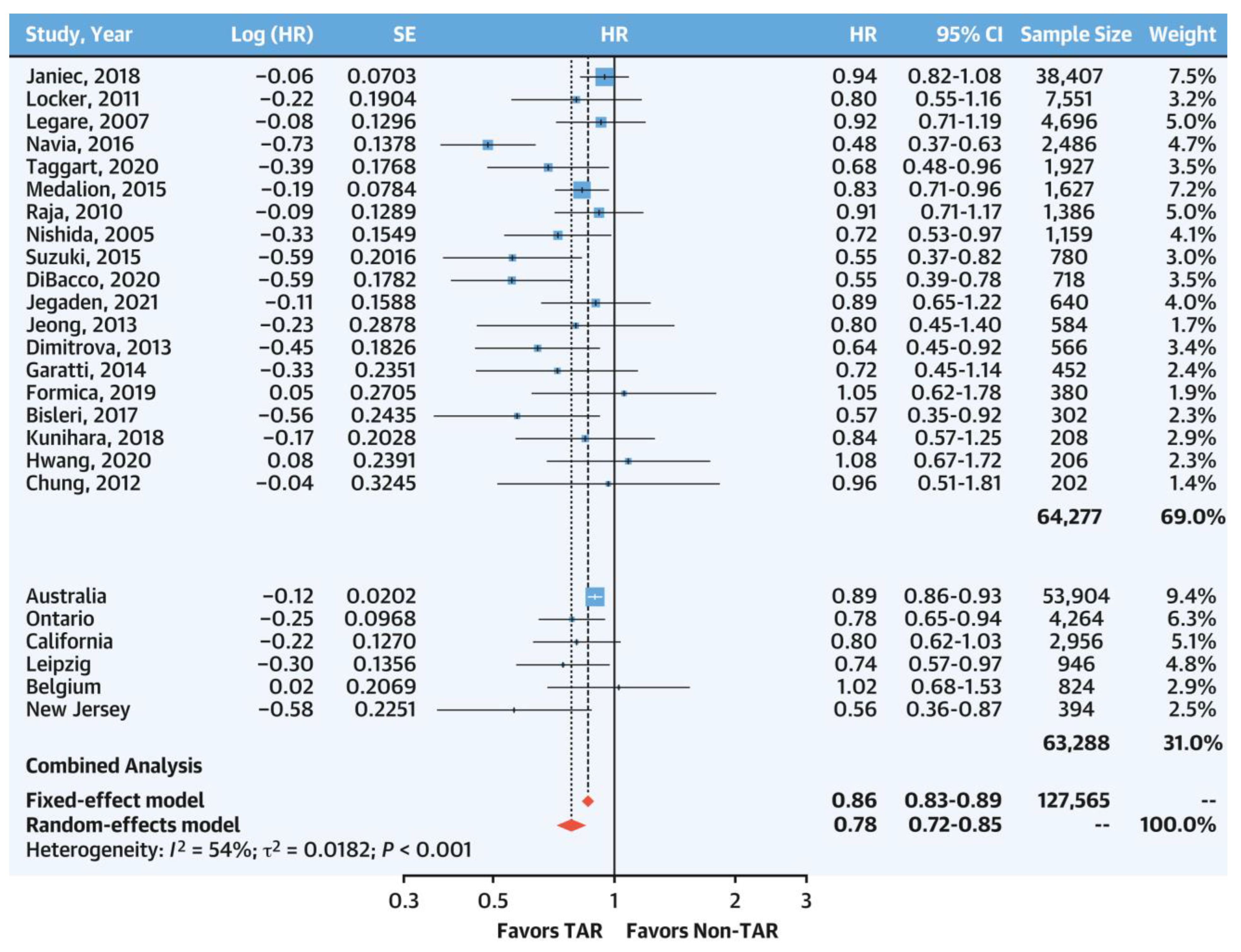
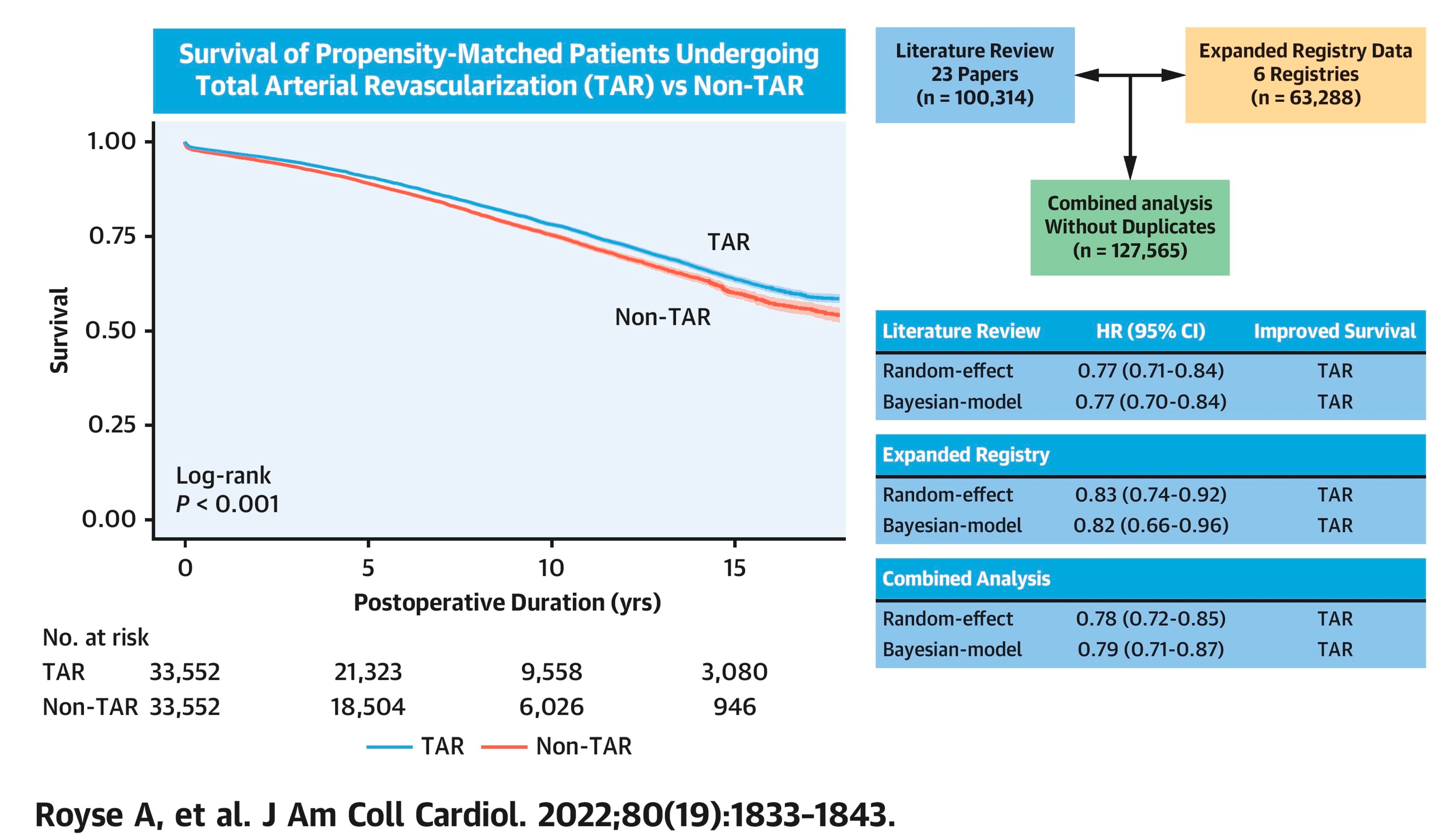
- Royse, A.; Ren, J.; Royse, C.; Tian, D.H.; Fremes, S.; Gaudino, M.; Benedetto, U.; Woo, J.S.; Goldstone, A.B.; Davierwala, P.; et al. Coronary Artery Bypass Surgery without Saphenous Vein Grafting: JACC: Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 80, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- Urso, S.; Sadaba, R.; González, J.M.; Nogales, E.; Pettinari, M.; Tena, M.; Paredes, F.; Portela, F. Total arterial revascularization strategies: A meta-analysis of propensity score-matched observational studies. J. Card. Surg. 2019, 34, 837–845. [Google Scholar] [CrossRef]
- Yanagawa, B.; Verma, S.; Mazine, A.; Tam, D.Y.; Jüni, P.; Puskas, J.D.; Murugavel, S.; Friedrich, J.O. Impact of total arterial revascularization on long term survival: A systematic review and meta-analysis of 130,305 patients. Int. J. Cardiol. 2017, 233, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Klima, U.; Elsebay, A.A.; Gantri, M.R.; Bangardt, J.; Miller, G.; Emery, R.W. Computerized tomographic angiography in patients having eSVS Mesh(R) supported coronary saphenous vein grafts: Intermediate term results. J. Cardiothorac. Surg. 2014, 9, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, D. A new no-touch preparation technique. Technical notes. Scand. J. Thorac. Cardiovasc. Surg. 1996, 30, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Wang, X.; Sun, H.; Feng, W.; Song, Y.; Lu, F.; Wang, L.; Wang, Y.; Xu, B.; Wang, H.; et al. No-Touch Versus Conventional Vein Harvesting Techniques at 12 Months After Coronary Artery Bypass Grafting Surgery: Multicenter Randomized, Controlled Trial. Circulation 2021, 144, 1120–1129. [Google Scholar] [CrossRef]
- Deb, S.; Singh, S.K.; de Souza, D.; Chu, M.W.A.; Whitlock, R.; Meyer, S.R.; Verma, S.; Jeppsson, A.; Al-Saleh, A.; Brady, K.; et al. SUPERIOR SVG: No touch saphenous harvesting to improve patency following coronary bypass grafting (a multi-Centre randomized control trial, NCT01047449). J. Cardiothorac. Surg. 2019, 14, 85. [Google Scholar] [CrossRef] [Green Version]
- Muneretto, C.; Bisleri, G.; Negri, A.; Manfredi, J.; Metra, M.; Nodari, S.; Culot, L.; Dei Cas, L. Total arterial myocardial revascularization with composite grafts improves results of coronary surgery in elderly: A prospective randomized comparison with conventional coronary artery bypass surgery. Circulation 2003, 108 (Suppl. 1), Ii29–Ii33. [Google Scholar] [CrossRef] [Green Version]
- Le, J.; Baskett, R.J.F.; Buth, K.J.; Hirsch, G.M.; Brydie, A.; Gayner, R.; Legare, J.-F. A pilot randomized controlled trial comparing CABG surgery performed with total arterial grafts or without. J. Cardiothorac. Surg. 2015, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, R.V.; Tam, D.Y.; Karkhanis, R.; Wang, X.; Austin, P.C.; Ko, D.T.; Gaudino, M.; Royse, A.; Fremes, S.E. Long-term Outcomes Associated with Total Arterial Revascularization vs Non–Total Arterial Revascularization. JAMA Cardiol. 2020, 5, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Buxton, B.F.; Hayward, P.A.; Raman, J.; Moten, S.C.; Rosalion, A.; Gordon, I.; Seevanayagam, S.; Matalanis, G.; Benedetto, U.; Gaudino, M.; et al. Long-Term Results of the RAPCO Trials. Circulation 2020, 142, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
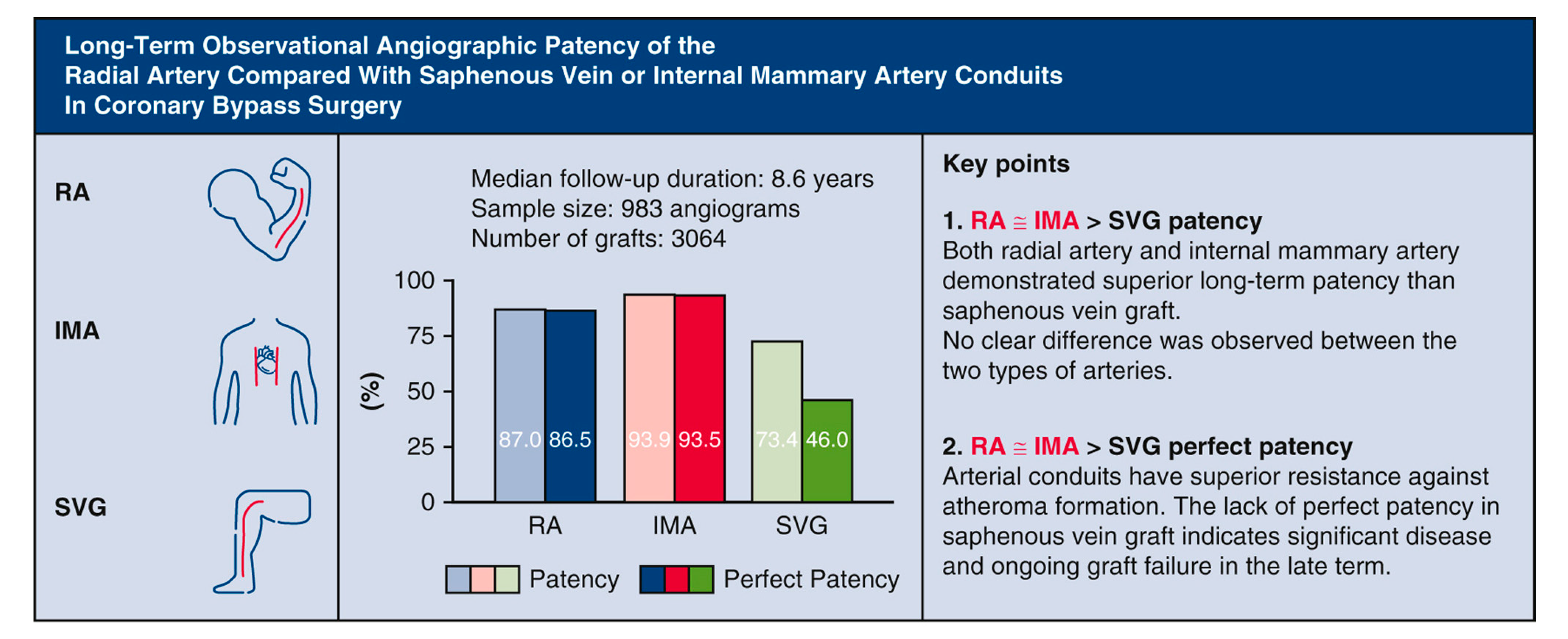
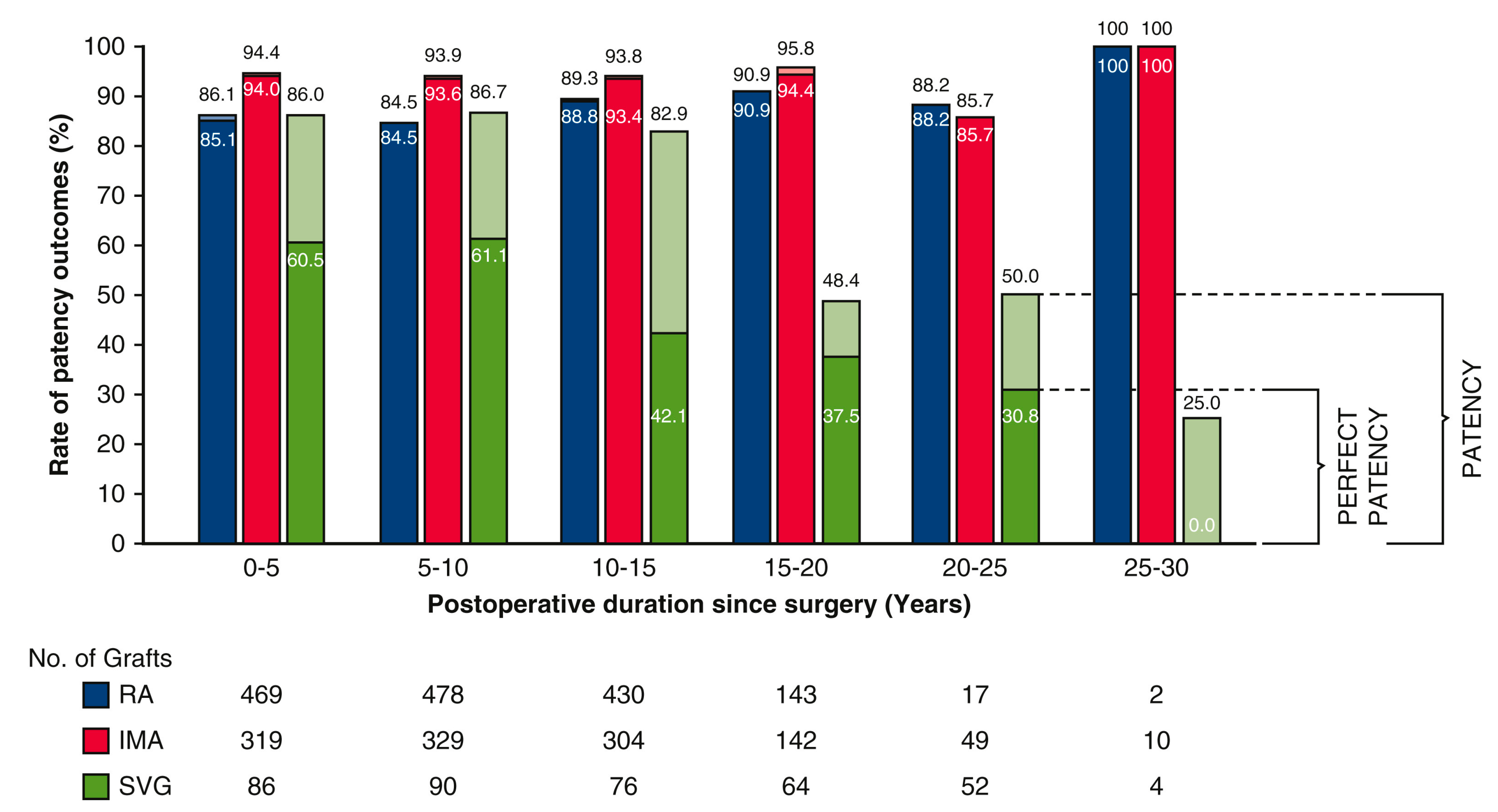
- Ren, J.; Royse, C.; Siderakis, C.; Srivastav, N.; Royse, A. Long-term observational angiographic patency and perfect patency of radial artery compared with saphenous vein or internal mammary artery in coronary bypass surgery. J. Thorac. Cardiovasc. Surg. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Taggart, D.P.; Altman, D.G.; Gray, A.M.; Lees, B.; Gerry, S.; Benedetto, U.; Flather, M. Randomized Trial of Bilateral versus Single Internal-Thoracic-Artery Grafts. N. Engl. J. Med. 2016, 375, 2540–2549. [Google Scholar] [CrossRef] [Green Version]
- Gaudino, M.; Lorusso, R.; Rahouma, M.; Abouarab, A.; Tam, D.Y.; Spadaccio, C.; Saint-Hilary, G.; Leonard, J.; Iannaccone, M.; D'Ascenzo, F.; et al. Radial Artery Versus Right Internal Thoracic Artery Versus Saphenous Vein as the Second Conduit for Coronary Artery Bypass Surgery: A Network Meta-Analysis of Clinical Outcomes. J. Am. Heart Assoc. 2019, 8, e010839. [Google Scholar] [CrossRef] [Green Version]
- Gaudino, M.; Di Franco, A.; Rahouma, M.; Tam, D.Y.; Iannaccone, M.; Deb, S.; D'Ascenzo, F.; Abouarab, A.A.; Girardi, L.N.; Taggart, D.P.; et al. Unmeasured Confounders in Observational Studies Comparing Bilateral Versus Single Internal Thoracic Artery for Coronary Artery Bypass Grafting: A Meta-Analysis. J. Am. Heart Assoc. 2018, 7, e008010. [Google Scholar] [CrossRef] [Green Version]
- Takagi, H.; Goto, S.N.; Watanabe, T.; Mizuno, Y.; Kawai, N.; Umemoto, T. A meta-analysis of adjusted hazard ratios from 20 observational studies of bilateral versus single internal thoracic artery coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2014, 148, 1282–1290. [Google Scholar] [CrossRef] [Green Version]
- Yi, G.; Shine, B.; Rehman, S.M.; Altman, D.G.; Taggart, D.P. Effect of bilateral internal mammary artery grafts on long-term survival: A meta-analysis approach. Circulation 2014, 130, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Taggart, D.P.; Benedetto, U.; Gerry, S.; Altman, D.G.; Gray, A.M.; Lees, B.; Gaudino, M.; Zamvar, V.; Bochenek, A.; Buxton, B.; et al. Bilateral versus Single Internal-Thoracic-Artery Grafts at 10 Years. N. Engl. J. Med. 2019, 380, 437–446. [Google Scholar] [CrossRef]
- Taggart, D.P.; Gaudino, M.F.; Gerry, S.; Gray, A.; Lees, B.; Dimagli, A.; Puskas, J.D.; Zamvar, V.; Pawlaczyk, R.; Royse, A.G.; et al. Effect of total arterial grafting in the Arterial Revascularization Trial. J. Thorac. Cardiovasc. Surg. 2022, 163, 1002–1009.e1006. [Google Scholar] [CrossRef] [PubMed]
- Aldea, G.S.; Bakaeen, F.G.; Pal, J.; Fremes, S.; Head, S.J.; Sabik, J.; Rosengart, T.; Kappetein, A.P.; Thourani, V.H.; Firestone, S.; et al. The Society of Thoracic Surgeons Clinical Practice Guidelines on Arterial Conduits for Coronary Artery Bypass Grafting. Ann. Thorac. Surg. 2016, 101, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. J. Cardiothorac. Surg. 2019, 55, 4–90. [Google Scholar] [CrossRef] [Green Version]
- Iribarne, A.; Goodney, P.P.; Flores, A.M.; DeSimone, J.; DiScipio, A.W.; Austin, A.; McCullough, J.N. National Trends and Geographic Variation in Bilateral Internal Mammary Artery Use in the United States. Ann. Thorac. Surg. 2017, 104, 1902–1907. [Google Scholar] [CrossRef] [Green Version]
- Yan, B.P.; Clark, D.J.; Buxton, B.; Ajani, A.E.; Smith, J.A.; Duffy, S.J.; Shardey, G.C.; Skillington, P.D.; Farouque, O.; Yii, M.; et al. Clinical characteristics and early mortality of patients undergoing coronary artery bypass grafting compared to percutaneous coronary intervention: Insights from the Australasian Society of Cardiac and Thoracic Surgeons (ASCTS) and the Melbourne Interventional Group (MIG) Registries. Heart Lung Circ. 2009, 18, 184–190. [Google Scholar] [CrossRef]
- Kamiya, H.; Akhyari, P.; Martens, A.; Karck, M.; Haverich, A.; Lichtenberg, A. Sternal microcirculation after skeletonized versus pedicled harvesting of the internal thoracic artery: A randomized study. J. Thorac. Cardiovasc. Surg. 2008, 135, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parish, M.A.; Asai, T.; Grossi, E.A.; Esposito, R.; Galloway, A.C.; Colvin, S.B.; Spencer, F.C. The effects of different techniques of internal mammary artery harvesting on sternal blood flow. J. Thorac. Cardiovasc. Surg. 1992, 104, 1303–1307. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Lockman, J.; Lorberboym, M.; Bder, O.; Cohen, N.; Medalion, B.; Schachner, A. Assessment of sternal vascularity with single photon emission computed tomography after harvesting of the internal thoracic artery. J. Thorac. Cardiovasc. Surg. 1999, 118, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Sá, M.P.B.O.; Cavalcanti, P.E.F.; de Andrade Costa Santos, H.J.; Soares, A.F.; Albuquerque Miranda, R.G.; Araújo, M.L.; Lima, R.C. Skeletonized versus pedicled bilateral internal mammary artery grafting: Outcomes and concerns analyzed through a meta-analytical approach. Int. J. Surg. 2015, 16, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, A.; Guermonprez, J.; Deloche, A.; Frechette, C.; DuBost, C. The aorta-to-coronary radial artery bypass graft: A technique avoiding pathological changes in grafts. Ann. Thorac. Surg. 1973, 16, 111–121. [Google Scholar] [CrossRef]
- Fisk, R.L.; Brooks, C.H.; Callaghan, J.C.; Dvorkin, J. Experience with the radial artery graft for coronary artery bypass. Ann. Thorac. Surg. 1976, 21, 513–518. [Google Scholar] [CrossRef]
- Curtis, J.J.; Stoney, W.S.; Alford, W.C., Jr.; Burrus, G.R.; Thomas, C.S., Jr. Intimal hyperplasia: A cause of radial artery aortocoronary bypass graft failure. Ann. Thorac. Surg. 1975, 20, 628–635. [Google Scholar] [CrossRef]
- Acar, C.; Jebara, V.A.; Portoghese, M.; Beyssen, B.; Pagny, J.Y.; Grare, P.; Chachques, J.C.; Fabiani, J.-N.; Deloche, A.; Guermonprez, J.L. Revival of the radial artery for coronary artery bypass grafting. Ann. Thorac. Surg. 1992, 54, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Benedetto, U.; Fremes, S.; Biondi-Zoccai, G.; Sedrakyan, A.; Puskas, J.D.; Angelini, G.D.; Buxton, B.; Frati, G.; Hare, D.L.; et al. Radial-Artery or Saphenous-Vein Grafts in Coronary-Artery Bypass Surgery. N. Engl. J. Med. 2018, 378, 2069–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hare, D.L. Radial Artery Patency and Clinical Outcomes Study–RAPCO: The 15-Year RCT Clinical Outcomes Comparing Radial Artery with Right Internal Thoracic Artery or with Saphenous Vein; AHA: Chicago, IL, USA, 2022. [Google Scholar]
- Schwann, T.A.; Habib, R.H.; Wallace, A.; Shahian, D.M.; O'Brien, S.; Jacobs, J.P.; Puskas, J.D.; Kurlansky, P.A.; Engoren, M.C.; Tranbaugh, R.F.; et al. Operative Outcomes of Multiple-Arterial Versus Single-Arterial Coronary Bypass Grafting. Ann. Thorac. Surg. 2018, 105, 1109–1119. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Bellomo, F.; Nappi, P.; Chello, C.; Iervolino, A.; Chello, M.; Acar, C. The Use of Radial Artery for CABG: An Update. Biomed. Res. Int. 2021, 2021, 5528006. [Google Scholar] [CrossRef]
- Nezic, D.G.; Knezevic, A.M.; Milojevic, P.S.; Dukanovic, B.P.; Jovic, M.D.; Borzanovic, M.D.; Neskovic, A.N. The fate of the radial artery conduit in coronary artery bypass grafting surgery. Eur. J. Cardio-Thorac. Surg. 2006, 30, 341–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, C.; Lu, Z.; Zhu, H.; Xue, S.; Lian, F. Bilateral internal mammary artery grafting and risk of sternal wound infection: Evidence from observational studies. Ann. Thorac. Surg. 2013, 95, 1938–1945. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.Y.; Hayward, P.A.; Hadinata, I.E.; Matalanis, G.; Buxton, B.F.; Stewart, A.G.; Hare, D.L. Long-term impact of radial artery harvest on forearm function and symptoms: A comparison with leg vein. J. Thorac. Cardiovasc. Surg. 2013, 145, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knobloch, K.; Lichtenberg, A.; Tomaszek, S.; Hagl, C.; Khaladj, N.; Klima, U.; Haverich, A. Long-term physical activity and neurologic function after harvesting of the radial artery as T-graft or free graft in coronary revascularization. Ann. Thorac. Surg. 2005, 80, 918–921. [Google Scholar] [CrossRef] [PubMed]
- Holman, W.L.; Davies, J.E.; Lin, J.Y.; Wang, Y.; Goldman, S.; Bakaeen, F.G.; Kelly, R.; Fremes, S.E.; Lee, K.K.; Wagner, T.H.; et al. Consequences of radial artery harvest: Results of a prospective, randomized, multicenter trial. JAMA Surg. 2013, 148, 1020–1023. [Google Scholar] [CrossRef] [Green Version]
- Royse, A.G.; Royse, C.F.; Shah, P.; Williams, A.; Kaushik, S.; Tatoulis, J. Radial artery harvest technique, use and functional outcome. Eur. J. Cardiothorac. Surg. 1999, 15, 186–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pola, P.; Serricchio, M.; Flore, R.; Manasse, E.; Favuzzi, A.; Possati, G.F. Safe removal of the radial artery for myocardial revascularization: A doppler study to prevent ischemic complications to the hand. J. Thorac. Cardiovasc. Surg. 1996, 112, 737–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glineur, D.; Hanet, C. Competitive flow in coronary bypass surgery: Is it a problem? Curr. Opin. Cardiol. 2012, 27, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Myers, M.G.; Fremes, S.E. Prevention of radial artery graft spasm: A survey of Canadian surgical centres. Can. J. Cardiol. 2003, 19, 677–681. [Google Scholar]
- Gaudino, M.; Glieca, F.; Luciani, N.; Alessandrini, F.; Possati, G. Clinical and angiographic effects of chronic calcium channel blocker therapy continued beyond first postoperative year in patients with radial artery grafts: Results of a prospective randomized investigation. Circulation 2001, 104, I64–I67. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Luciani, N.; Nasso, G.; Salica, A.; Canosa, C.; Possati, G. Is postoperative calcium channel blocker therapy needed in patients with radial artery grafts? J. Thorac. Cardiovasc. Surg. 2005, 129, 532–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabik, J.F.; Lytle, B.W.; Blackstone, E.H.; Houghtaling, P.L.; Cosgrove, D.M. Comparison of Saphenous Vein and Internal Thoracic Artery Graft Patency by Coronary System. Ann. Thorac. Surg. 2005, 79, 544–551. [Google Scholar] [CrossRef]
- Robinson, B.M.; Paterson, H.S.; Naidoo, R.; Dhurandhar, V.; Denniss, A.R. Bilateral Internal Thoracic Artery Composite Y Grafts: Analysis of 464 Angiograms in 296 Patients. Ann. Thorac. Surg. 2016, 101, 974–980. [Google Scholar] [CrossRef]
- Abu-Omar, Y.; Mussa, S.; Anastasiadis, K.; Steel, S.; Hands, L.; Taggart, D.P. Duplex ultrasonography predicts safety of radial artery harvest in the presence of an abnormal Allen test. Ann. Thorac. Surg. 2004, 77, 116–119. [Google Scholar] [CrossRef]
- Maniar, H.S.; Sundt, T.M.; Barner, H.B.; Prasad, S.M.; Peterson, L.; Absi, T.; Moustakidis, P. Effect of target stenosis and location on radial artery graft patency. J. Thorac. Cardiovasc. Surg. 2002, 123, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudino, M.; Alessandrini, F.; Pragliola, C.; Cellini, C.; Glieca, F.; Luciani, N.; Girola, F.; Possati, G. Effect of target artery location and severity of stenosis on mid-term patency of aorta-anastomosed vs. internal thoracic artery-anastomosed radial artery grafts. Eur. J. Cardio-Thorac. Surg. 2004, 25, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Royse, A.G.; Brennan, A.P.; Pawanis, Z.; Canty, D.; Royse, C.F. Patency When Grafted to Coronary Stenosis More Than 50% in LIMA-RA-Y Grafts. Heart Lung Circ. 2020, 29, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Mounsey, C.A.; Mawhinney, J.A.; Werner, R.S.; Taggart, D.P. Does Previous Transradial Catheterization Preclude Use of the Radial Artery as a Conduit in Coronary Artery Bypass Surgery? Circulation 2016, 134, 681–688. [Google Scholar] [CrossRef]
- Rocha, R.V.; Tam, D.Y.; Karkhanis, R.; Nedadur, R.; Fang, J.; Tu, J.V.; Gaudino, M.; Royse, A.; Fremes, S.E. Multiple Arterial Grafting Is Associated With Better Outcomes for Coronary Artery Bypass Grafting Patients. Circulation 2018, 138, 2081–2090. [Google Scholar] [CrossRef]
- Chikwe, J.; Sun, E.; Hannan, E.L.; Itagaki, S.; Lee, T.; Adams, D.H.; Egorova, N.N. Outcomes of Second Arterial Conduits in Patients Undergoing Multivessel Coronary Artery Bypass Graft Surgery. J. Am. Coll. Cardiol. 2019, 74, 2238–2248. [Google Scholar] [CrossRef]
- Gaudino, M.; Alexander, J.H.; Bakaeen, F.G.; Ballman, K.; Barili, F.; Calafiore, A.M.; Davierwala, P.; Goldman, S.; Kappetein, P.; Lorusso, R.; et al. Randomized comparison of the clinical outcome of single versus multiple arterial grafts: The ROMA trial-rationale and study protocol. Eur. J. Cardiothorac. Surg. 2017, 52, 1031–1040. [Google Scholar] [CrossRef]
- Gaudino, M.; Di Franco, A.; Alexander, J.H.; Bakaeen, F.; Egorova, N.; Kurlansky, P.; Boening, A.; Chikwe, J.; Demetres, M.; Devereaux, P.J.; et al. Sex differences in outcomes after coronary artery bypass grafting: A pooled analysis of individual patient data. Eur. Heart J. 2022, 43, 18–28. [Google Scholar] [CrossRef]
- Alam, M.; Bandeali, S.J.; Kayani, W.T.; Ahmad, W.; Shahzad, S.A.; Jneid, H.; Birnbaum, Y.; Kleiman, N.S.; Coselli, J.S.; Ballantyne, C.M.; et al. Comparison by meta-analysis of mortality after isolated coronary artery bypass grafting in women versus men. Am. J. Cardiol. 2013, 112, 309–317. [Google Scholar] [CrossRef]
- Abramov, D.; Tamariz, M.G.; Sever, J.Y.; Christakis, G.T.; Bhatnagar, G.; Heenan, A.L.; Goldman, B.S.; Fremes, S.E. The influence of gender on the outcome of coronary artery bypass surgery. Ann. Thorac. Surg. 2000, 70, 800–805; discussion 806. [Google Scholar] [CrossRef]
- Tam, D.Y.; Rocha, R.V.; Fang, J.; Ouzounian, M.; Chikwe, J.; Lawton, J.; Ko, D.T.; Austin, P.C.; Gaudino, M.; Fremes, S.E. Multiple arterial coronary bypass grafting is associated with greater survival in women. Heart 2021, 107, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Samadashvili, Z.; Hameed, I.; Chikwe, J.; Girardi, L.N.; Hannan, E.L. Differences in Long-term Outcomes After Coronary Artery Bypass Grafting Using Single vs Multiple Arterial Grafts and the Association with Sex. JAMA Cardiol. 2021, 6, 401–409. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparative Analysis | Patency | Perfect Patency | ||
|---|---|---|---|---|
| Odds Ratio (CI) | p | Odds Ratio (CI) | p | |
| Overall effect of conduit type | - | <0.001 | - | <0.001 |
| RA vs. SVG | 3.37 (2.23, 5.08) | <0.001 | 17.57 (11.39, 27.08) | <0.001 |
| IMA vs. SVG | 4.72 (2.74, 8.15) | <0.001 | 20.11 (11.64, 34.74) | <0.001 |
| IMA vs. RA | 1.40 (0.85, 2.33) | 0.189 | 1.14 (0.71, 1.84) | 0.578 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, J.; Royse, C.; Royse, A. Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery. J. Clin. Med. 2023, 12, 2516. https://doi.org/10.3390/jcm12072516
Ren J, Royse C, Royse A. Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery. Journal of Clinical Medicine. 2023; 12(7):2516. https://doi.org/10.3390/jcm12072516
Chicago/Turabian StyleRen, Justin, Colin Royse, and Alistair Royse. 2023. "Late Clinical Outcomes of Total Arterial Revascularization or Multiple Arterial Grafting Compared to Conventional Single Arterial with Saphenous Vein Grafting for Coronary Surgery" Journal of Clinical Medicine 12, no. 7: 2516. https://doi.org/10.3390/jcm12072516