
Endogenous Opioid Imbalance as a Potential Factor Involved in the Pathogenesis of Chronic Kidney Disease-Associated Pruritus in Dialysis Patients
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Laboratory Tests
2.3. Pruritus Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
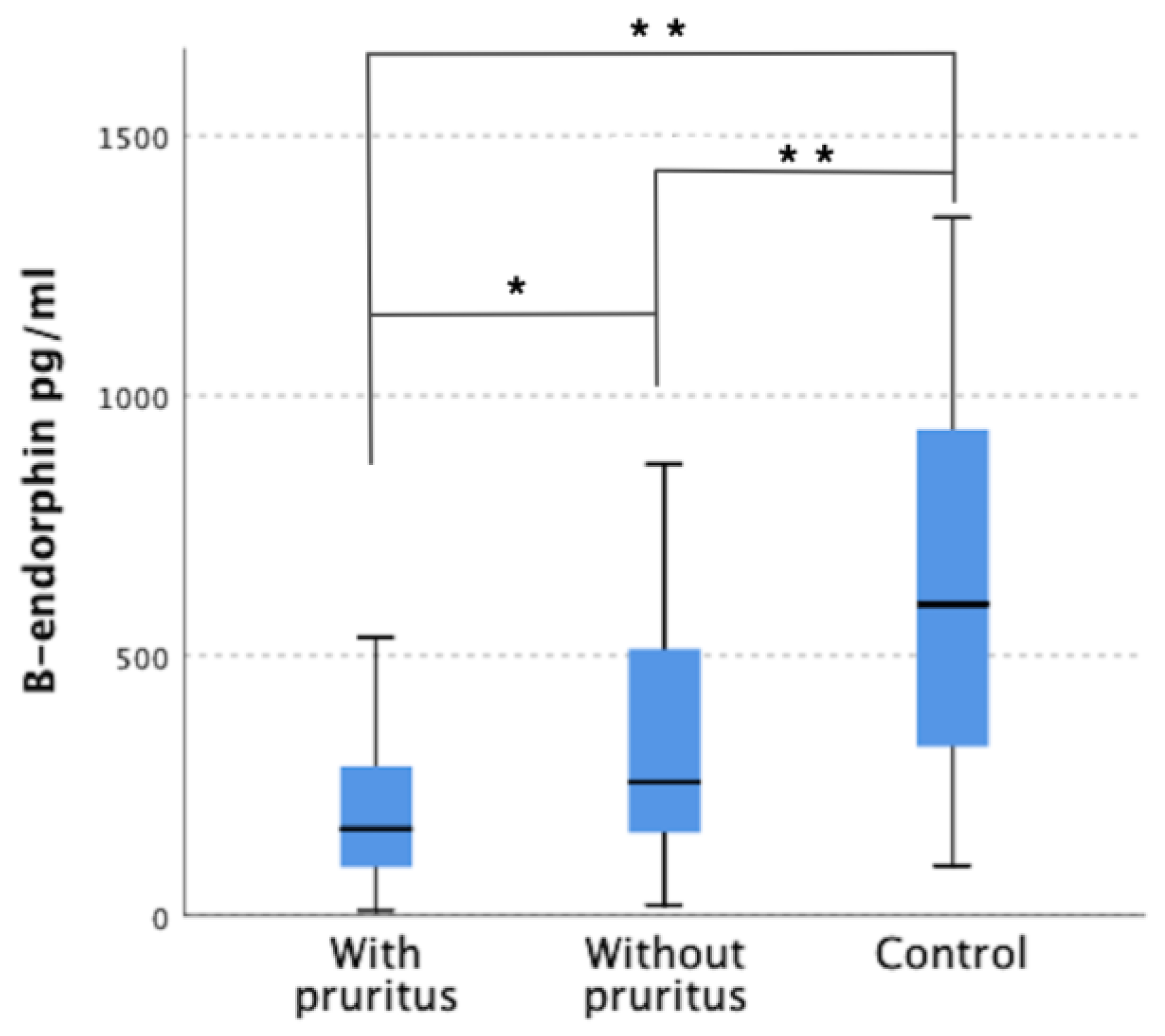
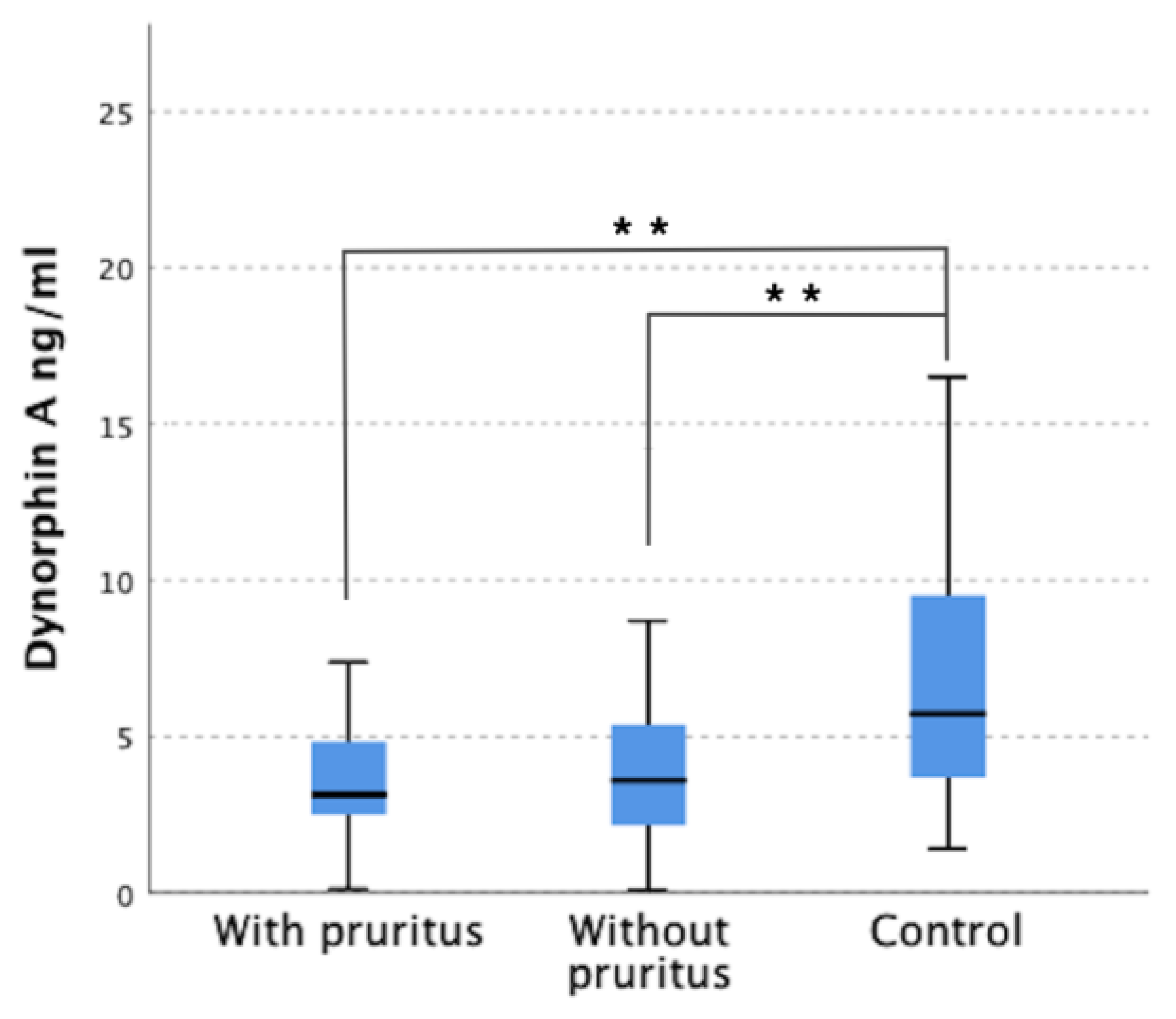
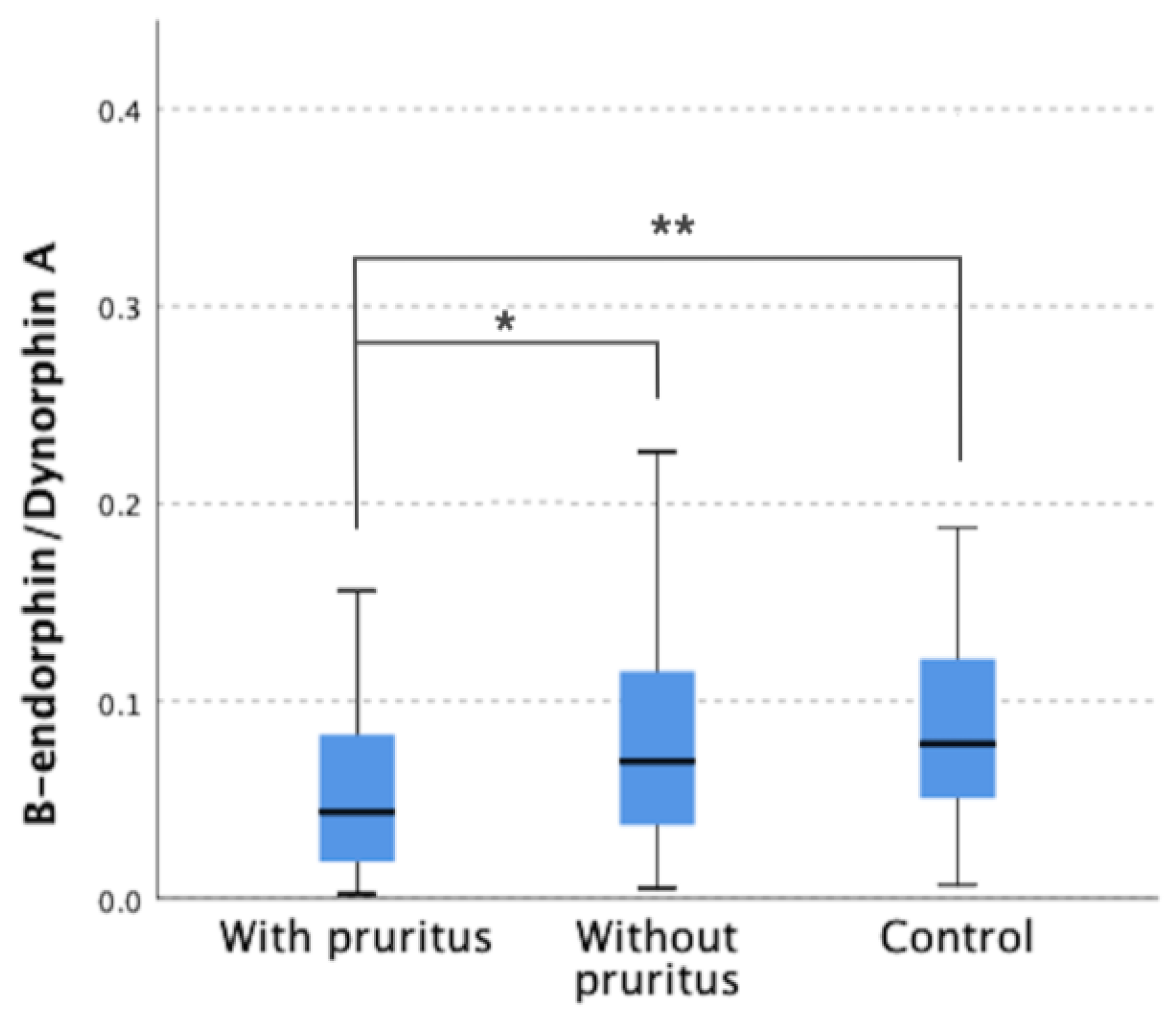
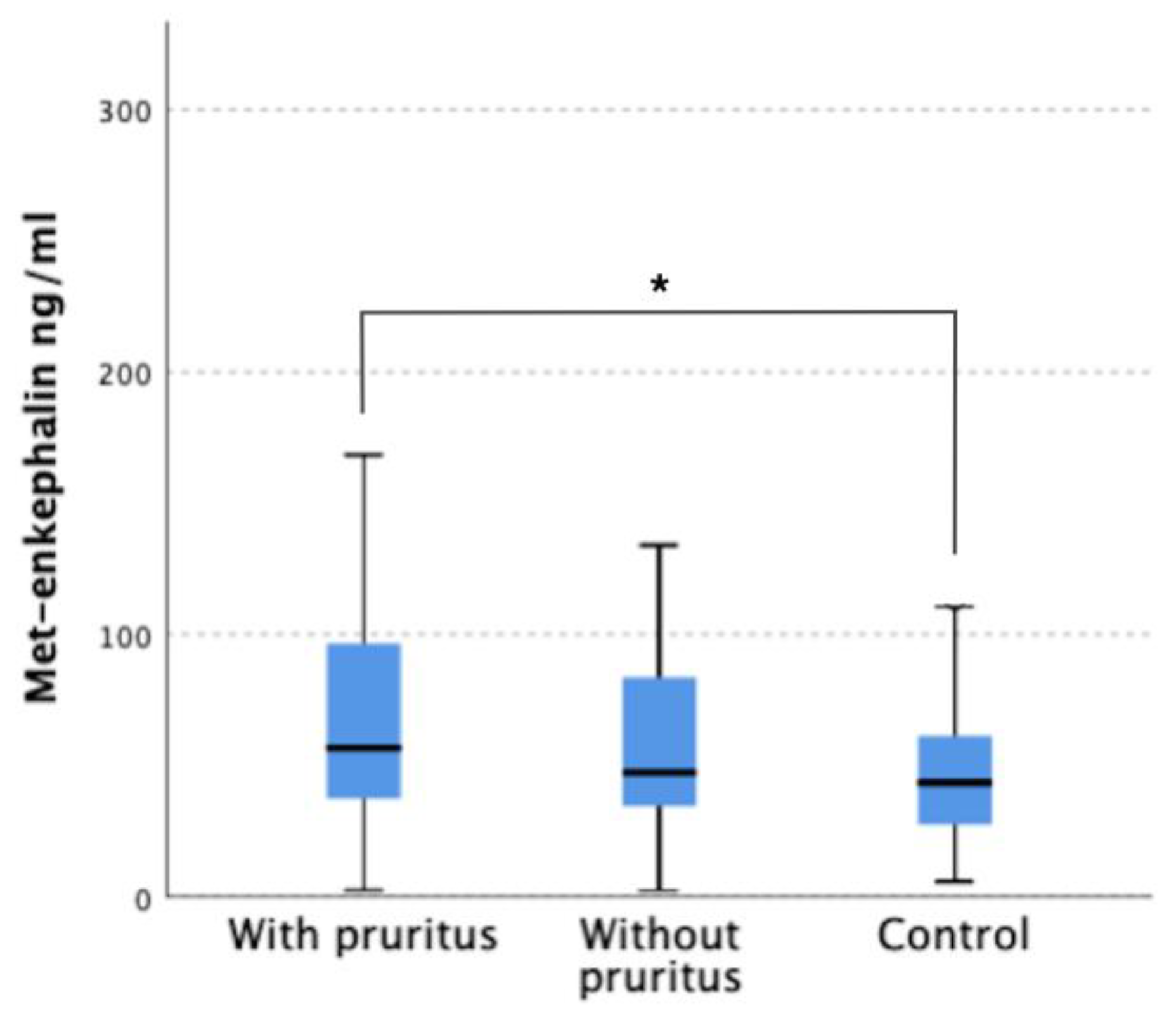
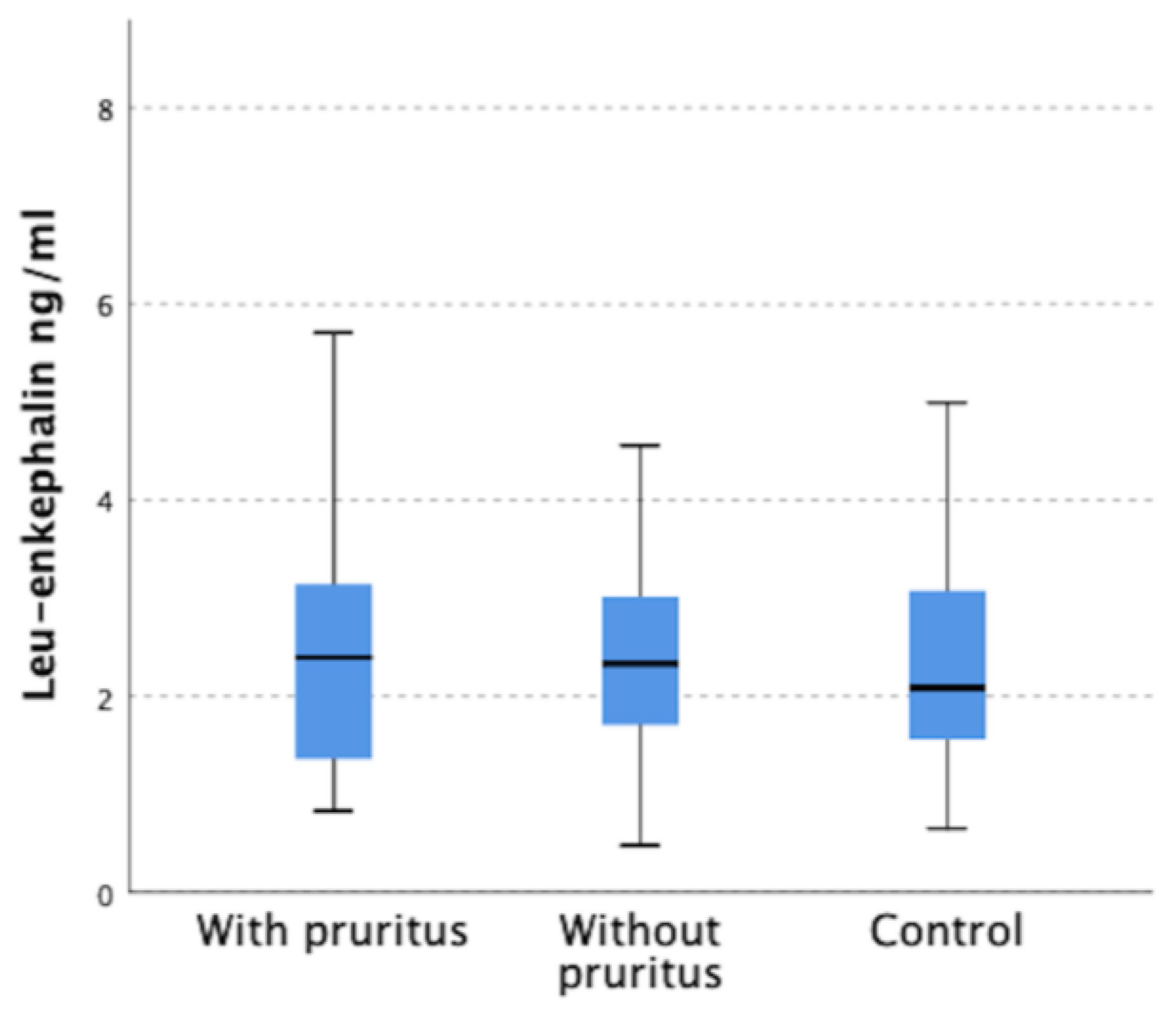
3.2. Serum Levels of Met-enkephalin, Leu-enkephalin, β-endorphin and Dynorphin A in Patients and in Control Group
3.3. Correlations of Opioids Serum Concentration with Itch Intensity and Other Clinical and Demographic Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grundmann, S.; Ständer, S. Chronic Pruritus: Clinics and Treatment. Ann. Dermatol. 2011, 23, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reszke, R.; Krajewski, P.; Szepietowski, J.C. Emerging Therapeutic Options for Chronic Pruritus. Am. J. Clin. Derm. 2020, 21, 601–618. [Google Scholar] [CrossRef] [PubMed]
- Yosipovitch, G.; Bernhard, J.D. Clinical Practice. Chronic Pruritus Item Type Journal Article. N. Engl. J. Med. 2013, 368, 1625–1659. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Pollock, C. Epidemiology and Burden of Chronic Kidney Disease-Associated Pruritus. Clin. Kidney J. 2021, 14, i1–i7. [Google Scholar] [CrossRef]
- Verduzco, H.A.; Shirazian, S. CKD-Associated Pruritus: New Insights Into Diagnosis, Pathogenesis, and Management. Kidney Int. Rep. 2020, 5, 1387. [Google Scholar] [CrossRef]
- Naldi, L.; Mercuri, S.R. Chronic Pruritus Management: A Plea for Improvement—Can Itch Clinics Be an Option? Dermatology 2010, 221, 216–218. [Google Scholar] [CrossRef]
- Weisshaar, E. Itch: A Global Problem? Front. Med. 2021, 8, 680. [Google Scholar] [CrossRef]
- Ständer, S.; Raap, U.; Weisshaar, E.; Schmelz, M.; Mettang, T.; Handwerker, H.; Luger, T.A. Pathogenesis of Pruritus. J. Dtsch. Dermatol. Ges. 2011, 9, 456–463. [Google Scholar] [CrossRef]
- Damiani, G.; Cazzaniga, S.; Conic, R.R.Z.; Naldi, L.; Griseta, V.; Miracapillo, A.; Azzini, M.; Mocci, L.; Michelini, M.; Offidani, A.; et al. Pruritus Characteristics in a Large Italian Cohort of Psoriatic Patients. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1316–1324. [Google Scholar] [CrossRef]
- Jaiswal, D.; Uzans, D.; Hayden, J.; Kiberd, B.A.; Tennankore, K.K. Targeting the Opioid Pathway for Uremic Pruritus: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2016, 3, 2054358116675345. [Google Scholar] [CrossRef] [Green Version]
- Reich, A.; Szepietowski, J.C. Opioid-Induced Pruritus: An Update. Clin. Exp. Dermatol. 2010, 35, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Benson, J.L.; Campbell, H.E.; Phillips, C.N. Opioid-Induced Pruritus. Consult. Pharm. 2015, 30, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Singh, S.I. Neuraxial Opioid-Induced Pruritus: An Update. J. Anaesthesiol. Clin. Pharmacol. 2013, 29, 303. [Google Scholar] [CrossRef]
- Schricker, S.; Kimmel, M. Unravelling the Pathophysiology of Chronic Kidney Disease-Associated Pruritus. Clin. Kidney J. 2021, 14, i23–i31. [Google Scholar] [CrossRef] [PubMed]
- Stein, C. Opioid Receptors. Annu. Rev. Med. 2016, 67, 433–451. [Google Scholar] [CrossRef]
- Tominaga, M.; Takamori, K. Peripheral Itch Sensitization in Atopic Dermatitis. Allergol. Int. 2022, 71, 265–277. [Google Scholar] [CrossRef]
- Liang, X.; Liu, R.; Chen, C.; Ji, F.; Li, T. Opioid System Modulates the Immune Function: A Review. Transl. Perioper. Pain Med. 2016, 1, 5. [Google Scholar]
- Toubia, T.; Khalife, T. The Endogenous Opioid System: Role and Dysfunction Caused by Opioid Therapy. Clin. Obstet. Gynecol. 2019, 62, 3–10. [Google Scholar] [CrossRef]
- Reszke, R.; Kiliś-Pstrusińska, K.; Szepietowski, J.C. Chronic Kidney Disease-Associated Itch (CKD-AI) in Children—A Narrative Review. Toxins 2021, 13, 450. [Google Scholar] [CrossRef]
- Umeuchi, H.; Togashi, Y.; Honda, T.; Nakao, K.; Okano, K.; Tanaka, T.; Nagase, H. Involvement of Central μ-Opioid System in the Scratching Behavior in Mice, and the Suppression of It by the Activation of κ-Opioid System. Eur. J. Pharmacol. 2003, 477, 29–35. [Google Scholar] [CrossRef]
- Sakakihara, M.; Imamachi, N.; Saito, Y. Effects of Intrathecal κ-Opioid Receptor Agonist on Morphine-Induced Itch and Antinociception in Mice. Reg. Anesth. Pain Med. 2016, 41, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.M.; Nguyen, E.; Ross, S.E. The Delta-Opioid Receptor Bidirectionally Modulates Itch. Reg. Anesth. Pain Med. 2023, 24, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Hägermark, Ö. Itch and Endorphins. In New Trends in Allergy; Ring, J., Burg, G., Eds.; Springer: Berlin/Heidelberg, Germany, 1986; pp. 128–134. [Google Scholar]
- Kardon, A.P.; Polgár, E.; Hachisuka, J.; Snyder, L.M.; Cameron, D.; Savage, S.; Cai, X.; Karnup, S.; Fan, C.R.; Hemenway, G.M.; et al. Dynorphin Acts as a Neuromodulator to Inhibit Itch in the Dorsal Horn of the Spinal Cord. Neuron 2014, 82, 573–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, A. Enkephalin. In Handbook of Hormones: Comparative Endocrinology for Basic and Clinical Research; Ando, H., Ukena, K., Nagata, S., Eds.; Academic Press: London, UK, 2021; Volume 1, pp. 91–94. ISBN 9780128206492. [Google Scholar]
- Lee, H.; Ko, M.-C. Distinct Functions of Opioid-Related Peptides and Gastrin-Releasing Peptide in Regulating Itch and Pain in the Spinal Cord of Primates OPEN. Sci. Rep. 2015, 5, 11676. [Google Scholar] [CrossRef] [Green Version]
- Hägermark, Ö. Peripheral and Central Mediators of Itch. Skin Pharmacol. Physiol. 1992, 5, 1–8. [Google Scholar] [CrossRef]
- Sandyk, R. The Endogenous Opioid System in Neurological Disorders of the Basal Ganglia. Life Sci. 1985, 37, 1655–1663. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Reich, A. Pruritus in Psoriasis: An Update. Eur. J. Pain 2016, 20, 41–46. [Google Scholar] [CrossRef]
- Umehara, Y.; Kiatsurayanon, C.; Trujillo-Paez, J.V.; Chieosilapatham, P.; Peng, G.; Yue, H.; Le, H.; Nguyen, T.; Song, P.; Okumura, K.; et al. Intractable Itch in Atopic Dermatitis: Causes and Treatments. Biomedicines 2021, 9, 229. [Google Scholar] [CrossRef]
- Lipman, Z.M.; Yosipovitch, G. An Evaluation of Difelikefalin as a Treatment Option for Moderate-to-Severe Pruritus in End Stage Renal Disease. Expert Opin. Pharmacother. 2021, 22, 549–555. [Google Scholar] [CrossRef]
- Wieczorek, A.; Krajewski, P.; Kozioł-Gałczyńska, M.; Szepietowski, J.C. Opioid Receptors Expression in the Skin of Haemodialysis Patients Suffering from Uraemic Pruritus. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2368–2372. [Google Scholar] [CrossRef]
- Hwang, J.C.; Hsu, K.T.; Tsai, H.C.; Lam, K.K.; Wang, P.W. Serum Endorphin Levels in Uremic Patients under Maintenance Hemodialysis. Taiwan Yi Xue Hui Za Zhi JFMA 1989, 88, 360–365. [Google Scholar]
- Mettang, T.; Fischer, F.P.; Dollenbacher, U.; Kuhlman, U. Uraemic Pruritus Is Not Related to β-Endorphin Serum Levels in Haemodialysis Patients. Nephrol. Dial. Transplant. 1998, 13, 231–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odou, P.; Azar, R.; Luyckx, M.; Brunet, C.; Dine, T. A Hypothesis for Endogenous Opioid Peptides in Uraemic Pruritus: Role of Enkephalin. Nephrol. Dial. Transplant. 2001, 16, 1953–1954. [Google Scholar] [CrossRef] [Green Version]
- Fowler, E.; Yosipovitch, G. A New Generation of Treatments for Itch. Acta Derm. Venereol. 2020, 100, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Damiani, G.; Kridin, K.; Pacifico, A.; Malagoli, P.; Pigatto, P.D.M.; Finelli, R.; Taccone, F.S.; Peluso, L.; Conic, R.R.Z.; Bragazzi, N.L.; et al. Antihistamines-Refractory Chronic Pruritus in Psoriatic Patients Undergoing Biologics: Aprepitant vs Antihistamine Double Dosage, a Real-World Data. J. Dermatol. Treat. 2022, 33, 1554–1557. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, H.; Ebata, T.; Takamori, K.; Muramatsu, T.; Nakamoto, H.; Suzuki, H. Effect of a Novel Kappa-Receptor Agonist, Nalfurafine Hydrochloride, on Severe Itch in 337 Haemodialysis Patients: A Phase III, Randomized, Double-Blind, Placebo-Controlled Study. Nephrol. Dial. Transpl. 2010, 25, 1251–1257. [Google Scholar] [CrossRef] [Green Version]
- Wala, K.; Szepietowski, J. Difelikefalin in the Treatment of Chronic Kidney Disease-Associated Pruritus: A Systematic Review. Pharmaceuticals 2022, 15, 934. [Google Scholar]
- Reich, A.; Mcglone, F. Tailoring the Cut-off Values of the Visual Analogue Scale and Numeric Rating Scale in Itch Assessment. Acta Derm. Venereol. 2017, 97, 759–760. [Google Scholar] [CrossRef] [Green Version]
- Świerczyńska, K.; Krajewski, P.; Reszke, R.; Krajewska, M.; Nochaiwong, S.; Białynicki-Birula, R.; Szepietowski, J.C.; Dermatol Allergol, A. Uraemic Pruritus in Dialysis Patient (UP-Dial) Questionnaire: Creation and validation of the Polish Language Version. Adv. Dermatol. Allergol. 2021, 39, 538–544. [Google Scholar] [CrossRef]
- Jang, Y.H.; Kim, S.M.; Eun, D.H.; Park, K.D.; Park, G.H.; Kim, B.S.; Li, K.; Park, C.O.; Kim, H.O.; Kim, H.S.; et al. Validity and Reliability of Itch Assessment Scales for Chronic Pruritus in Adults: A Prospective Multicenter Study. J. Am. Acad. Dermatol. 2020, 82, 80–86. [Google Scholar] [CrossRef]
- Narita, I.; Tsubakihara, Y.; Uchiyama, T.; Okamura, S.; Oya, N.; Takahashi, N.; Gejyo, F.; Yamamoto, A.; Ichikawa, A.; Ohishi, A.; et al. Efficacy and Safety of Difelikefalin in Japanese Patients With Moderate to Severe Pruritus Receiving Hemodialysis: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2210339. [Google Scholar] [CrossRef] [PubMed]
- Fishbane, S.; Wen, W.; Munera, C.; Menzaghi, F.; McCafferty, K. Long-Term Safety and Efficacy of Difelikefalin in Subjects With Chronic Kidney Disease–Associated Pruritus: Analysis From KALM-1 and KALM-2. SKIN J. Cutan. Med. 2021, 5, s75. [Google Scholar] [CrossRef]
- Sutaria, N.; Adawi, W.; Goldberg, R.; Roh, Y.S.; Choi, J.; Kwatra, S.G. Itch: Pathogenesis and Treatment. J. Am. Acad. Dermatol. 2022, 86, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Langedijk, J.A.G.M.; Beuers, U.H.; Oude Elferink, R.P.J. Cholestasis-Associated Pruritus and Its Pruritogens. Front. Med. 2021, 8, 224. [Google Scholar] [CrossRef]
- Bailey, A.J.M.; Li, H.O.Y.; Kirchhof, M.G. Novel Kappa-Opioid Receptor Agonist for the Treatment of Cholestatic Pruritus: Systematic Review. JMIR Dermatol. 2022, 5, e30737. [Google Scholar] [CrossRef]
- Komiya, E.; Tominaga, M.; Kamata, Y.; Suga, Y.; Takamori, K. Molecular and Cellular Mechanisms of Itch in Psoriasis. Int. J. Mol. Sci. 2020, 21, 8406. [Google Scholar] [CrossRef]
- Georgala, S.; Schulpis, K.H.; Papaconstantinou, E.D.; Stratigos, J. Raised β-Endorphin Serum Levels in Children with Atopic Dermatitis and Pruritus. J. Dermatol. Sci. 1994, 8, 125–128. [Google Scholar] [CrossRef]
- Glinski, W.; Brodecka, H.; Glinska-Ferenz, M.; Kowalski, D. Increased Concentration of Beta-endorphin in Sera of Patients with Psoriasis and Other Inflammatory Dermatoses. Br. J. Dermatol. 1994, 131, 260–264. [Google Scholar] [CrossRef]
- Takahashi, N.; Tominaga, M.; Kosaka, R.; Kamata, Y.; Umehara, Y.; Matsuda, H.; Sakaguchi, A.; Ogawa, H.; Takamori, K. Involvement of Μ-Opioid Receptors and κ-Opioid Receptors in Itch-Related Scratching Behaviour of Imiquimod-Induced Psoriasis-like Dermatitis in Mice. Acta Derm. Venereol. 2017, 97, 928–933. [Google Scholar] [CrossRef] [Green Version]
- Nakasone, T.; Sato, T.; Matsushima, Y.; Inoue, T.; Kamei, C. Characteristics of Scratching Behavior in ADJM Mice (Atopic Dermatitis from Japanese Mice). Immunopharmacol. Immunotoxicol. 2015, 37, 202–206. [Google Scholar] [CrossRef]
- Sagita Moniaga, C.; Iwamoto, S.; Kitamura, T.; Fujishiro, M.; Takahashi, N.; Kina, K.; Ogawa, H.; Tominaga, M.; Takamori, K. Plasma Dynorphin A Concentration Reflects the Degree of Pruritus in Chronic Liver Disease: A Preliminary Report. Acta Derm. Venereol. 2019, 99, 442–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Düll, M.M.; Wolf, K.; Vetter, M.; Dietrich, P.; Neurath, M.F.; Kremer, A.E. Endogenous Opioid Levels Do Not Correlate With Itch Intensity and Therapeutic Interventions in Hepatic Pruritus. Front. Med. 2021, 8, 454. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Ciccarelli, M.; Mallamaci, F.; Maggiore, Q.; Lotti, M.; Zucchelli, G.C. Plasma Met-Enkephalin and Leu-Enkephalin in Chronic Renal Failure. Nephrol. Dial. Transplant. 1987, 1, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Danno, K.; Nishiura, K.; Tanaka, M. Increased Met-Enkephalin Plasma Levels in Hemodialysis Patients with or without Pruritus. J. Dermatol. Sci. 1995, 10, 238–240. [Google Scholar] [CrossRef]
- Klin, M.; Waluga, M.; Rudka, R.; Madej, A.; Janiszewska, M.; Grzebieniak, E.; Wesolowsky, A. Plasma Catecholamines, Neuropeptide Y and Leucine-Enkephalin in Uremic Patients before and after Dialysis during Rest and Handgrip. Boll. Chim. Farm. 1998, 137, 306–313. [Google Scholar] [PubMed]
- Spivey, J.R.; Jorgensen, R.A.; Gores, G.J.; Lindor, K.D. Methionine-Enkephalin Concentrations Correlate with Stage of Disease but Not Pruritus in Patients with Primary Biliary Cirrhosis. Am. J. Gastroenterol. Suppl. 1994, 89, 2028–2032. [Google Scholar] [CrossRef]
- Taneda, K.; Tominaga, M.; Negi, O.; Tengara, S.; Kamo, A.; Ogawa, H.; Takamori, K. Evaluation of Epidermal Nerve Density and Opioid Receptor Levels in Psoriatic Itch. Br. J. Dermatol. 2011, 165, 277–284. [Google Scholar] [CrossRef]
- Kupczyk, P.; Reich, A.; Hołysz, M.; Gajda, M.; Wysokińska, E.; Kobuszewska, A.; Nevozhay, D.; Nowakowska, B.; Strządała, L.; Jagodziński, P.P.; et al. Opioid Receptors in Psoriatic Skin: Relationship with Itch. Acta Derm. Venereol. 2017, 97, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Velenosi, T.J.; Urquhart, B.L. Pharmacokinetic Considerations in Chronic Kidney Disease and Patients Requiring Dialysis. Expert Opin. Drug Metab. Toxicol. 2014, 10, 1131–1143. [Google Scholar] [CrossRef]
- Böger, R.H. Renal Impairment: A Challenge for Opioid Treatment? The Role of Buprenorphine. Palliat. Med. 2016, 20, 17–23. [Google Scholar] [CrossRef]
- Mercadante, S. Opioid Metabolism and Clinical Aspects. Eur. J. Pharmacol. 2015, 769, 71–78. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group 1—With Pruritus | Group 2—Without Pruritus | Group 3—Controls | p-Value | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Mean ± SD | Median | Mean ± SD | Median | ||
| Met-enkephalin (ng/mL) | 75.98 ± 65.48 | 58.6 | 61.37 ± 44.92 | 47.3 | 48.06 ± 92.09 | 43.3 | 0.033 |
| Leu-enkephalin (ng/mL) | 2.9 ± 2.15 | 2.5 | 2.79 ± 2.1 | 2.3 | 2.42 ± 1.22 | 2.1 | NS |
| β-endorphin (pg/mL) | 216.25 ± 171.21 | 166.4 | 344.84 ± 268.3 | 256.6 | 658.51 ± 377.66 | 596.2 | <0.001 |
| Dynorphin A (ng/mL) | 4.32 ± 3.95 | 3.1 | 4.62 ± 3.87 | 3.6 | 8.1 ± 6.2 | 5.8 | <0.001 |
| β-endorphin/Dynorphin A | 0.16 ± 0.64 | 0.047 | 0.16 ± 0.34 | 0.076 | 0.13 ± 0.14 | 0.086 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wala-Zielińska, K.; Świerczyńska-Mróz, K.; Krajewski, P.K.; Nowicka-Suszko, D.; Krajewska, M.; Szepietowski, J.C. Endogenous Opioid Imbalance as a Potential Factor Involved in the Pathogenesis of Chronic Kidney Disease-Associated Pruritus in Dialysis Patients. J. Clin. Med. 2023, 12, 2474. https://doi.org/10.3390/jcm12072474
Wala-Zielińska K, Świerczyńska-Mróz K, Krajewski PK, Nowicka-Suszko D, Krajewska M, Szepietowski JC. Endogenous Opioid Imbalance as a Potential Factor Involved in the Pathogenesis of Chronic Kidney Disease-Associated Pruritus in Dialysis Patients. Journal of Clinical Medicine. 2023; 12(7):2474. https://doi.org/10.3390/jcm12072474
Chicago/Turabian StyleWala-Zielińska, Kamila, Karolina Świerczyńska-Mróz, Piotr K. Krajewski, Danuta Nowicka-Suszko, Magdalena Krajewska, and Jacek C. Szepietowski. 2023. "Endogenous Opioid Imbalance as a Potential Factor Involved in the Pathogenesis of Chronic Kidney Disease-Associated Pruritus in Dialysis Patients" Journal of Clinical Medicine 12, no. 7: 2474. https://doi.org/10.3390/jcm12072474