

Increased Access to Immunoglobulin Replacement Therapy for Patients with Primary Immunodeficiency in Poland Based on Clinical Usage Data of Immunoglobulin G over a 5-Year Period

Abstract
:1. Introduction
Reimbursement of IgG in Poland
2. Materials and Methods
2.1. Data Collection
2.2. Ethic Statement
3. Results
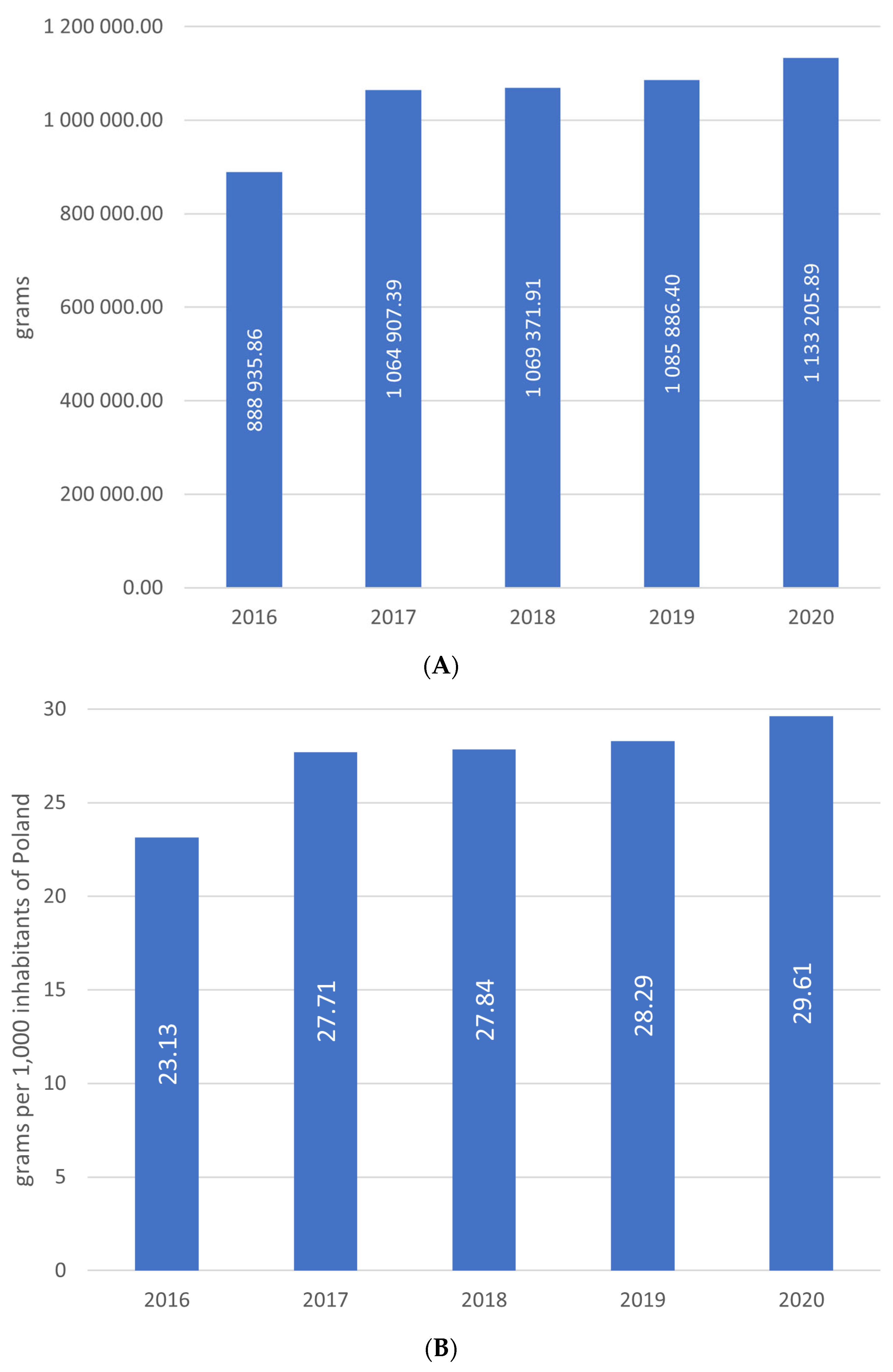
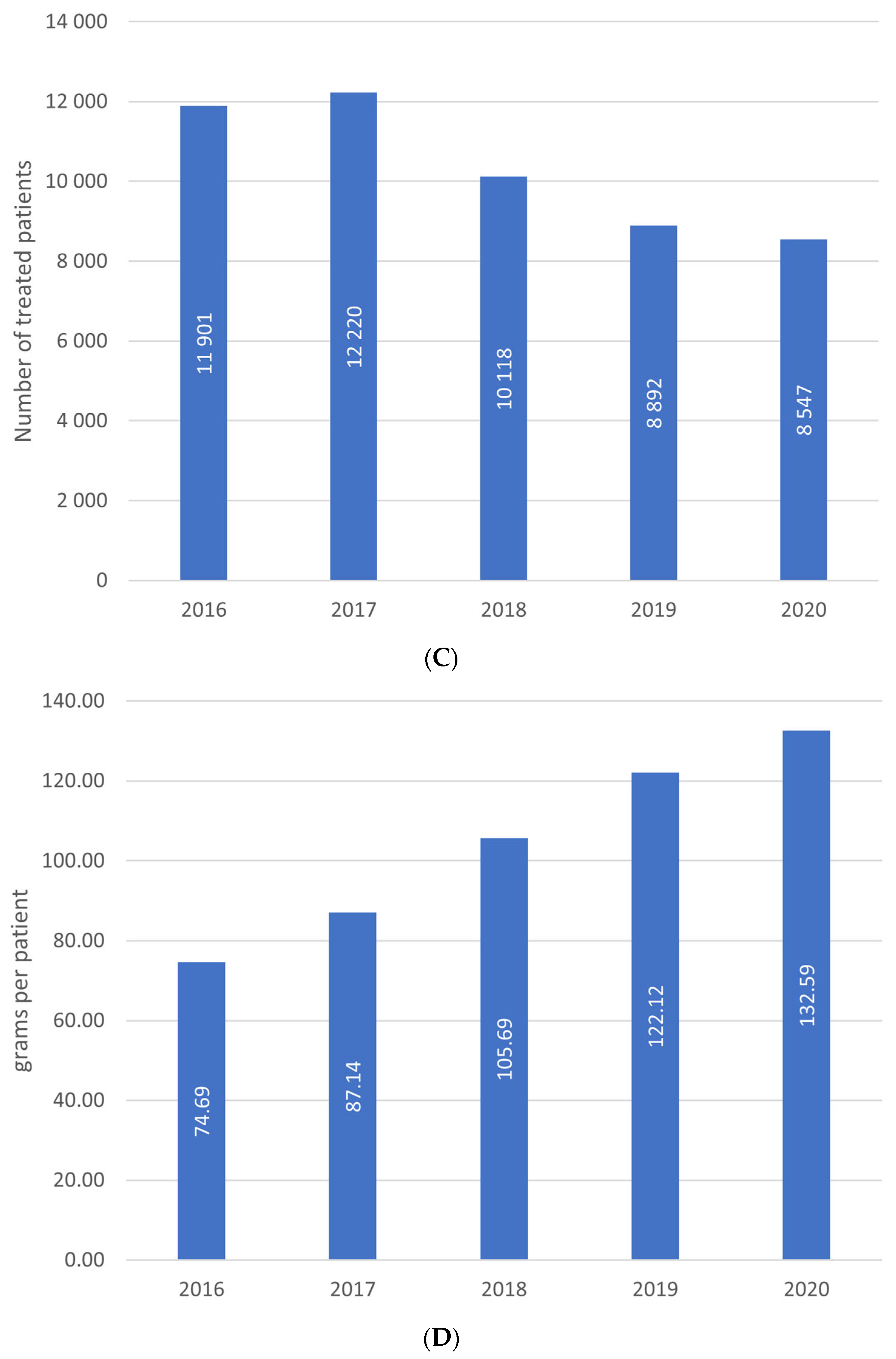
3.1. Total IgG Consumption
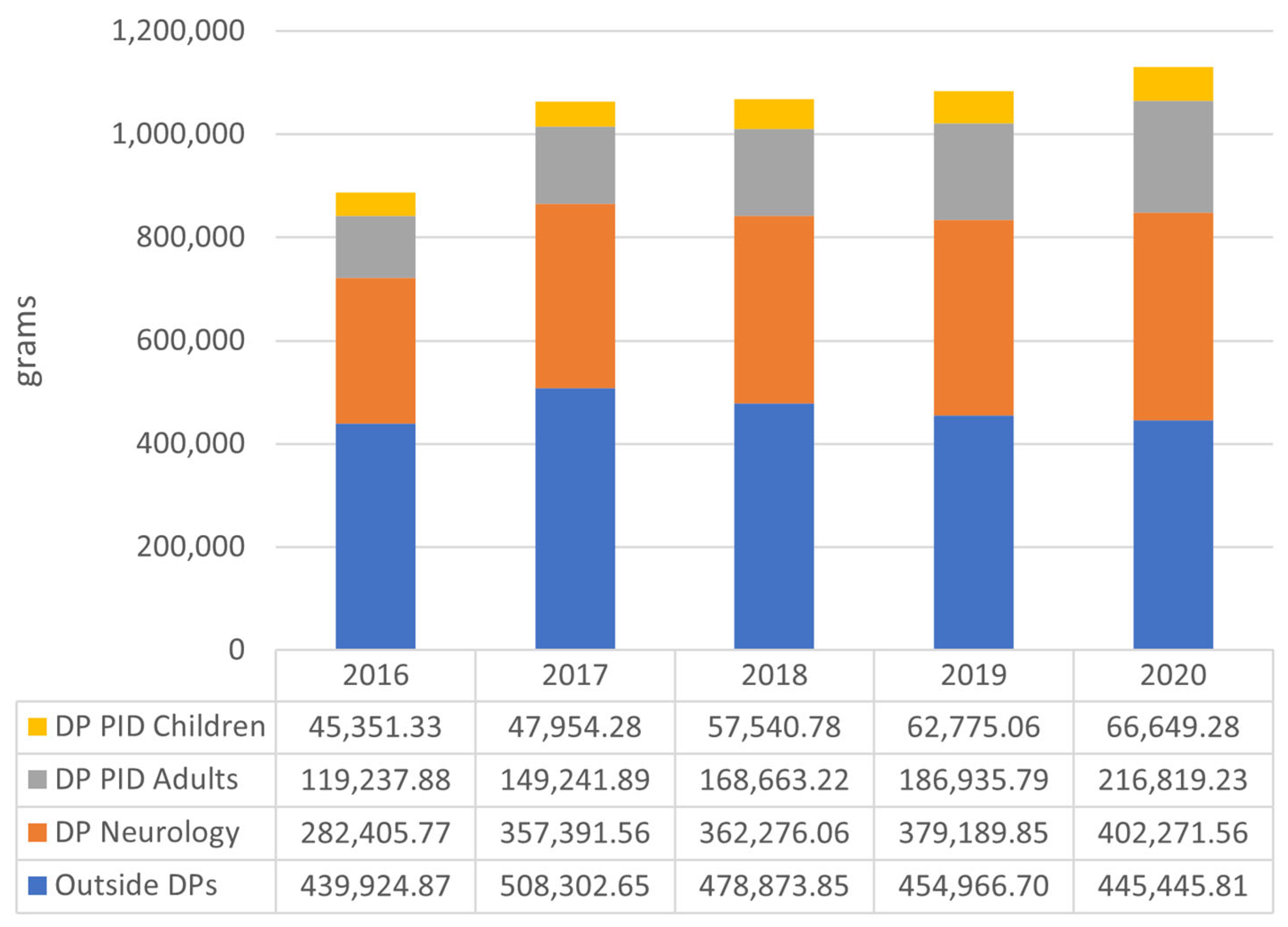
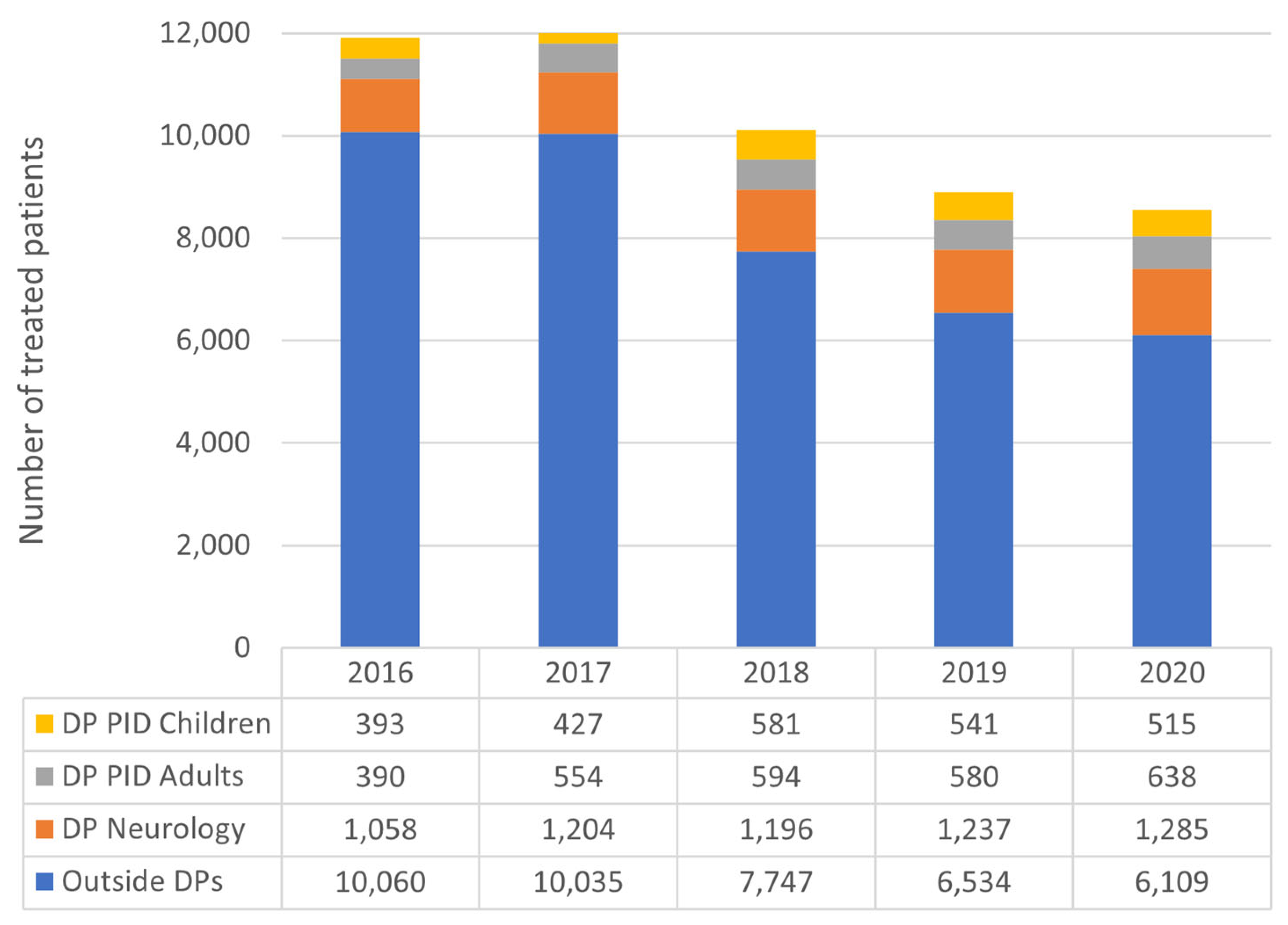
3.2. IgG Consumption in Primary Immune Deficiencies Drug Programs
3.3. IgG Consumption in Neurological Drug Program
3.4. IgG Consumption in Indications Outside Drug Programs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prevot, J.; Jolles, S. Global immunoglobulin supply: Steaming towards the iceberg? Curr. Opin. Allergy Clin. Immunol. 2020, 20, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, A.; Grazzini, G.; Quinti, I.; Candura, F.; Profili, S.; Liumbruno, G.M. The growing importance of achieving national self-sufficiency in immunoglobulin in Italy. The emergence of a national imperative. Blood Transfus. 2019, 17, 449–458. [Google Scholar] [CrossRef]
- Solís-Díez, G.; Turu-Pedrola, M.; Roig-Izquierdo, M.; Zara, C.; Vallano, A.; Pontes, C. Dealing with Immunoglobulin Shortages: A Rationalization Plan from Evidence-Based and Data Collection. Front. Public Health 2022, 10, 893770. [Google Scholar] [CrossRef]
- Broderick, C.; Kobayashi, S.; Suto, M.; Ito, S.; Kobayashi, T. Intravenous immunoglobulin for the treatment of Kawasaki disease. Cochrane Database Syst. Rev. 2023, 1, CD014884. [Google Scholar] [PubMed]
- Lee, J.L.; Mohamed Shah, N.; Mohd Saffian, S.; Makmor-Bakry, M.; Islahudin, F.; Alias, H.; Ali, A. Prescribing Practices of Intravenous Immuno-globulin in Tertiary Care Hospitals in Malaysia: A Need for a National Guideline for Immunoglobulin Use. Front. Pharmacol. 2022, 13, 879287. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.S.; Tinmouth, A.; Goldman, M.; Chassé, M.; Colas, J.A.; Saidenberg, E.; Shehata, N.; Fergusson, D.; Forster, A.J.; Wilson, K. Trends in IVIG use at a tertiary care Canadian center and impact of provincial use mitigation strategies: 10-year retrospective study with interrupted time series analysis. Transfusion 2019, 59, 1988–1996. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02 (accessed on 18 March 2023).
- Available online: https://www.gov.pl/web/zdrowie/obwieszczenia-ministra-zdrowia-lista-lekow-refundowanych (accessed on 18 March 2023).
- Pac, M.; Bernatowska, E. Comprehensive activities to increase recognition of primary immunodeficiency and access to immu-noglobulin replacement therapy in Poland. Eur. J. Pediatr. 2016, 175, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.grifols.com/documents/3625622/90066043/IAD+2019+Grifols.pdf/e2505992-1b9c-4168-9f08-b68a75170c4c (accessed on 18 March 2023).
- Hsu, L.-I.; Chen, J.-W.; Lin, D.-T.; Hung, Y.-S.; Hou, S.-M. Clinical use of intravenous immunoglobulin in Taiwan: A 10-year population study. J. Formos. Med. Assoc. 2021, 120, 1921–1925. [Google Scholar] [CrossRef] [PubMed]
- Ziętkiewicz, M.; Więsik-Szewczyk, E.; Matyja-Bednarczyk, A.; Napiórkowska-Baran, K.; Zdrojewski, Z.; Jahnz-Różyk, K. Shorter Diagnostic Delay in Polish Adult Patients with Common Variable Immunodeficiency and Symptom Onset after 1999. Front. Immunol. 2020, 11, 982. [Google Scholar] [CrossRef]
- Nordin, J.; Solís, L.; Prévot, J.; Mahlaoui, N.; Chapel, H.; Sánchez-Ramón, S.; Ali, A.; Seymour, J.W.; Pergent, M. The PID Principles of Care: Where Are We Now? A Global Status Report Based on the PID Life Index. Front. Immunol. 2021, 12, 780140. [Google Scholar] [CrossRef]
- Więsik-Szewczyk, E.; Ziętkiewicz, M.; Matyja-Bednarczyk, A.; Napiórkowska-Baran, K.; Suchanek, H.; Jahnz-Różyk, K. The first Polish cohort of adult patients with common variable immunodeficiency from 4 specialized centers: Do we provide standards of care? Pol. Arch. Intern. Med. 2018, 128, 563–566. [Google Scholar] [CrossRef] [Green Version]
- Wiesik-Szewczyk, E.; Sołdacki, D.; Paczek, L.; Jahnz-Różyk, K. Facilitated Subcutaneous Immunoglobulin Replacement Therapy in Clinical Practice: A Two Center, Long-Term Retrospective Observation in Adults With Primary Immunodeficiencies. Front. Immunol. 2020, 11, 981. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, B.; Martins, K.J.B.; Tran, D.T.; Blain, H.; Richer, L.; Klarenbach, S.W. Economic impact of self-administered subcutaneous versus clinic-administered intravenous immunoglobulin G therapy in Alberta, Canada: A population-based cohort study. Allergy Asthma Clin. Immunol. 2022, 18, 99. [Google Scholar] [CrossRef] [PubMed]
- Perraudin, C.; Bourdin, A.; Vicino, A.; Kuntzer, T.; Bugnon, O.; Berger, J. Home-based subcutaneous immunoglobulin for chronic inflammatory demyelinating polyneuropathy patients: A Swiss cost-minimization analysis. PLoS ONE 2020, 15, e0242630. [Google Scholar] [CrossRef] [PubMed]
- Perraudin, C.; Bourdin, A.; Spertini, F.; Berger, J.; Bugnon, O. Switching Patients to Home-Based Subcutaneous Immunoglobulin: An Economic Evaluation of an Interprofessional Drug Therapy Management Program. J. Clin. Immunol. 2016, 36, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.W.; Song, C.; Isaranuwatchai, W.; Betschel, S. Home-based subcutaneous immunoglobulin therapy vs hospital-based intra-venous immunoglobulin therapy: A prospective economic analysis. Ann. Allergy Asthma Immunol. 2018, 120, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Romberg, N. High cost of immunoglobulin replacement therapy. Ann. Allergy Asthma Immunol. 2022, 129, 645. [Google Scholar] [CrossRef]
- Alsina, L.; Montoro, J.B.; Moral, P.M.; Neth, O.; Pica, M.O.; Sánchez-Ramón, S.; Presa, M.; Oyagüez, I.; Casado, M.; González-Granado, L.I. Cost-minimization analysis of immunoglobulin treatment of primary immunodeficiency diseases in Spain. Eur. J. Health Econ. 2022, 23, 551–558. [Google Scholar] [CrossRef]
- Burakgazi, A.Z. Immunoglobulin Treatment in Neuromuscular Medicine. J. Clin. Neuromuscul. Dis. 2019, 20, 182–193. [Google Scholar] [CrossRef]
- Available online: https://www.criteria.blood.gov.au/CheckEligibility (accessed on 18 March 2023).
- Oaklander, A.L.; Gimigliano, F. Are the treatments for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) effective and safe?—A Cochrane Overview summary with commentary. Neurorehabilitation 2019, 44, 609–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahnz-Różyk, K.; Więsik-Szewczyk, E.; Roliński, J.; Siedlar, M.; Jędrzejczak, W.; Sydor, W.; Tomaszewska, A. Secondary immunodeficiencies with predominant antibody deficiency: Multidisciplinary perspectives of Polish experts. Cent. Eur. J. Immunol. 2020, 45, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Link, H.; Kerkmann, M.; Holtmann, L.; Working Groups Supportive Care (AGSMO); Medical Oncology (AIO) of the German Cancer Society (DKG). Immunoglobulin substitution in patients with secondary antibody deficiency in chronic lymphocytic leukemia and multiple myeloma: A representative analysis of guideline adherence and infections. Support. Care Cancer 2022, 30, 5187–5200. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SPECIALTY | 2016 | 2017 | 2018 | 2019 | 2020 | TOTAL AMOUNT | CHANGE 2016 vs. 2020 |
|---|---|---|---|---|---|---|---|
| HEMATOLOGY | 183,776.60 | 222,100.00 | 195,407.00 | 178,641.75 | 162,866.00 | 942,791.35 | −11.38% |
| PEDIATRIC ONCOHEMATOLOGY | 36,619.00 | 42,090.35 | 44,060.45 | 32,015.50 | 31,870.50 | 186,655.80 | −12.97% |
| CLINICAL IMMUNOLOGY | 22,875.85 | 27,698.55 | 29,515.15 | 31,456.65 | 42,223.50 | 153,769.70 | 84.58% |
| PEDIATRICS | 26,672.00 | 28,055.50 | 25,518.00 | 28,044.00 | 34,471.00 | 142,760.50 | 29.24% |
| REUMATOLOGY | 15,337.00 | 27,770.50 | 21,864.00 | 27,871.00 | 31,129.50 | 123,972.00 | 102.97% |
| NEUROLOGY | 22,552.00 | 20,574.00 | 26,527.00 | 27,448.00 | 21,571.00 | 118,672.00 | −4.35% |
| ANESTHESIOLOGY AND INTENSIVE THERAPY | 25,145.50 | 23,485.00 | 25,138.50 | 20,509.00 | 13,578.00 | 107,856.00 | −46.00% |
| ONCOLOGY | 16,502.40 | 19,339.00 | 19,342.00 | 16,154.00 | 13,551.00 | 84,888.40 | −17.88% |
| INTERNAL MEDICINE | 19,369.50 | 18,313.00 | 19,517.00 | 15,781.00 | 8775.00 | 81,755.50 | −54.70% |
| OBSTETRICS AND GYNECOLOGY | 17,168.00 | 17,534.00 | 8872.00 | 9582.00 | 8961.86 | 62,117.86 | −47.80% |
| DERMATOLOGY AND VENEROLOGY | 7141.00 | 8712.00 | 9974.00 | 15,254.00 | 19,882.00 | 60,963.00 | 178.42% |
| PEDIATRIC NEUROLOGY | 6687.00 | 8852.00 | 9011.50 | 12,597.50 | 13,927.00 | 51,075.00 | 108.27% |
| ALERGOLOGY | 6609.50 | 7520.00 | 5984.00 | 6721.00 | 7590.00 | 34,424.50 | 14.83% |
| NEFROLOGY | 5741.00 | 7835.00 | 8978.00 | 5410.00 | 5954.00 | 33,918.00 | 3.71% |
| PEDIATRIC ANESTHESIOLOGY AND INTENSIVE THERAPY | 5018.90 | 4057.55 | 4441.25 | 4650.70 | 5979.95 | 24,148.35 | 19.15% |
| PEDIATRIC REUMATOLOGY | 3131.50 | 4502.00 | 4224.00 | 4595.00 | 4732.50 | 21,185.00 | 51.13% |
| LUNG DISEASES | 4692.20 | 4113.00 | 4897.20 | 4312.00 | 2332.00 | 20,346.40 | −50.30% |
| PEDIATRIC CLINICAL IMMUNOLOGY | 4503.00 | 3547.20 | 3672.80 | 2806.60 | 2001.00 | 16,530.60 | −55.56% |
| TRANSPLANTOLOGY | 2351.00 | 1694.00 | 3042.00 | 3246.00 | 4269.00 | 14,602.00 | 81.58% |
| PEDIATRIC INFECTIOUS DISEASES | 1911.50 | 2826.50 | 2259.00 | 2600.50 | 3305.50 | 12,903.00 | 72.93% |
| PEDIATRIC CARDILOGY | 1233.50 | 1412.00 | 1085.00 | 1117.50 | 1991.50 | 6839.50 | 61.45% |
| PEDIATRIC ALLERGOLOGY | 1638.00 | 2018.50 | 976.50 | 340.00 | 495.00 | 5468.00 | −69.78% |
| INFECTIOUS DISEASES | 788.20 | 1498.00 | 1249.00 | 1228.00 | 200.00 | 4963.20 | −74.63% |
| PEDIATRIC TRANSPLANTOLOGY | 564.50 | 725.00 | 1269.50 | 1082.50 | 895.00 | 4536.50 | 58.55% |
| PEDIATRIC LUNG DISEASES | 786.70 | 432.50 | 542.50 | 1054.50 | 1218.50 | 4034.70 | 54.89% |
| PEDIATRIC NEFROLOGY | 974.52 | 942.50 | 729.50 | 274.00 | 457.50 | 3378.02 | −53.05% |
| CARDIOLOGY | 120.00 | 605.00 | 727.00 | 174.00 | 309.00 | 1935.00 | 157.50% |
| GERIATRICS | 15.00 | 50.00 | 50.00 | NR | 865.00 | 980.00 | 5666.67% |
| CARDIAC SURGERY | NR | NR | NR | NR | 44.00 | 44.00 |
| SPECIALTY | 2016 | 2017 | 2018 | 2019 | 2020 | Mean Over 5-Years |
|---|---|---|---|---|---|---|
| HEMATOLOGY | 102.27 | 98.84 | 96.40 | 105.58 | 95.52 | 99.58 |
| PEDIATRIC ONCOHEMATOLOGY | 48.37 | 51.96 | 51.53 | 38.62 | 43.96 | 46.95 |
| CLINICAL IMMUNOLOGY | 97.34 | 109.91 | 119.49 | 116.94 | 150.80 | 119.85 |
| PEDIATRICS | 38.49 | 44.04 | 35.64 | 41.18 | 45.42 | 40.95 |
| REUMATOLOGY | 125.71 | 169.33 | 155.06 | 207.99 | 213.22 | 175.35 |
| NEUROLOGY | 145.50 | 162.00 | 158.84 | 180.58 | 163.42 | 161.90 |
| ANESTHESIOLOGY AND INTENSIVE THERAPY | 60.01 | 61.16 | 59.85 | 63.69 | 64.05 | 61.39 |
| ONCOLOGY | 63.96 | 50.89 | 56.72 | 60.28 | 69.14 | 58.83 |
| INTERNAL MEDICINE | 84.58 | 84.00 | 79.66 | 76.61 | 79.77 | 81.11 |
| OBSTETRICS AND GYNECOLOGY | 5.14 | 5.25 | 8.56 | 15.58 | 14.64 | 6.94 |
| DERMATOLOGY AND VENEROLOGY | 285.64 | 290.40 | 343.93 | 526.00 | 473.38 | 393.31 |
| PEDIATRIC NEUROLOGY | 79.61 | 85.12 | 72.67 | 91.29 | 94.10 | 85.41 |
| ALERGOLOGY | 101.68 | 115.69 | 213.71 | 231.76 | 210.83 | 154.37 |
| NEFROLOGY | 55.74 | 66.97 | 72.40 | 77.29 | 106.32 | 72.17 |
| PEDIATRIC ANESTHESIOLOGY AND INTENSIVE THERAPY | 11.13 | 10.19 | 9.74 | 10.82 | 17.43 | 11.62 |
| PEDIATRIC REUMATOLOGY | 54.94 | 91.88 | 100.57 | 135.15 | 115.43 | 95.00 |
| LUNG DISEASES | 111.72 | 117.51 | 106.46 | 100.28 | 86.37 | 105.42 |
| PEDIATRIC CLINICAL IMMUNOLOGY | 45.48 | 45.48 | 48.33 | 43.85 | 50.03 | 46.30 |
| TRANSPLANTOLOGY | 31.77 | 30.80 | 26.22 | 36.89 | 40.27 | 33.26 |
| PEDIATRIC INFECTIOUS DISEASES | 15.93 | 25.93 | 28.24 | 26.54 | 45.28 | 26.88 |
| PEDIATRIC CARDILOGY | 18.98 | 25.21 | 22.60 | 26.61 | 31.12 | 24.87 |
| PEDIATRIC ALLERGOLOGY | 40.95 | 36.04 | 17.44 | 17.89 | 24.75 | 28.63 |
| INFECTIOUS DISEASES | 20.74 | 42.80 | 32.87 | 30.70 | 40.00 | 31.82 |
| PEDIATRIC TRANSPLANTOLOGY | 22.58 | 31.52 | 45.34 | 36.08 | 44.75 | 36.00 |
| PEDIATRIC LUNG DISEASES | 13.11 | 8.16 | 9.86 | 15.51 | 21.76 | 13.82 |
| PEDIATRIC NEFROLOGY | 12.34 | 17.45 | 15.20 | 10.54 | 16.94 | 14.44 |
| CARDIOLOGY | 30.00 | 55.00 | 90.88 | 43.50 | 38.63 | 55.29 |
| GERIATRICS | 15.00 | 50.00 | 50.00 | NR | 216.25 | 140.00 |
| CARDIAC SURGERY | NR | NR | NR | NR | 7.33 | 7.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Więsik-Szewczyk, E.; Ziętkiewicz, M.; Radziwilska-Muc, A.; Jahnz-Różyk, K. Increased Access to Immunoglobulin Replacement Therapy for Patients with Primary Immunodeficiency in Poland Based on Clinical Usage Data of Immunoglobulin G over a 5-Year Period. J. Clin. Med. 2023, 12, 2431. https://doi.org/10.3390/jcm12062431
Więsik-Szewczyk E, Ziętkiewicz M, Radziwilska-Muc A, Jahnz-Różyk K. Increased Access to Immunoglobulin Replacement Therapy for Patients with Primary Immunodeficiency in Poland Based on Clinical Usage Data of Immunoglobulin G over a 5-Year Period. Journal of Clinical Medicine. 2023; 12(6):2431. https://doi.org/10.3390/jcm12062431
Chicago/Turabian StyleWięsik-Szewczyk, Ewa, Marcin Ziętkiewicz, Anna Radziwilska-Muc, and Karina Jahnz-Różyk. 2023. "Increased Access to Immunoglobulin Replacement Therapy for Patients with Primary Immunodeficiency in Poland Based on Clinical Usage Data of Immunoglobulin G over a 5-Year Period" Journal of Clinical Medicine 12, no. 6: 2431. https://doi.org/10.3390/jcm12062431