
Impact of COVID-19 Confinement on Quality of Life of Patients with Age-Related Macular Degeneration: A Two-Wave Panel Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Inclusion and Exclusion Criteria
2.3. Study Outcomes
- Clinical outcomes: visual acuity (VA), visual impairment (WHO definitions) [18], number of intravitreal injections and unilateral or bilateral disease, and cataract surgery between the two surveys.
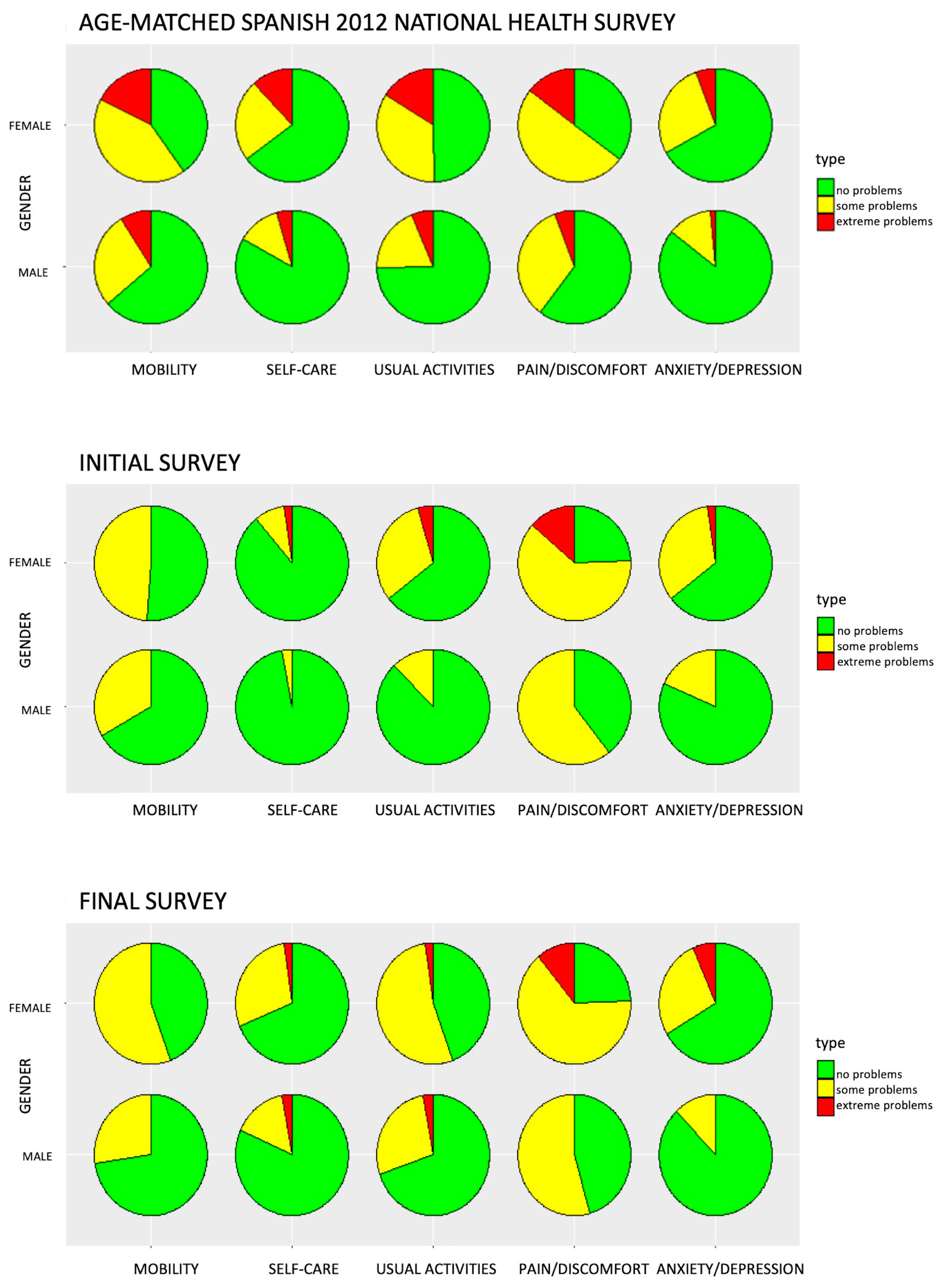
- HRQoL: Patients were asked to complete the EQ-5D-3L questionnaire [19]. The validated Spanish version of the EQ-5D-3L questionnaire, including the EQ Visual Analogue Scale (EQ VAS), was used [19]. The EQ-5D instrument is a generic instrument that provides a summary of HRQoL. The questionnaire was developed by the EuroQol Group for measuring HRQoL and consists of the EQ-5D descriptive system and the EQ VAS. The EQ descriptive system explores five health dimensions (mobility, self-care, activity, pain/discomfort, and anxiety/depression) that produce a five-digit health state profile for each patient. EQ-5D health states may be converted afterwards into a definite summary number: an index value also known as the health index. The health index reflects how good or bad a health state is, according to the preferences of the general population of a precise country/region, ensuring that the index values represent the societal perspective. The index value has a maximum value of 1 for perfect health, 0 represents death, and negative values reflect states worse than death [19]. The EQ VAS is a visual scale from 0 to 100, where 0 is the worst imagined state of health and 100 means the best [19].
- Social support: To assess the caregiver support and social network that the patient can have if needed, four questions concerning tangible support from the Medical Outcomes Study (MOS) Social Support questionnaire were used [20]. The MOS Social Support Survey (MOS SSS) Instrument consists of four separate social support subscales or dimensions (emotional/informational support, tangible support, affectionate support, and positive social interaction). A higher score on the scale or for overall support indicates more support. The instrumental or tangible support subscale qualifies the type of material or assistance aid, which can be measured in some way. This includes economic or financial support, material help in obtaining goods or services, collaboration with housework, and caring for the patient [20]. Responses range from 1 (none of the time) to 5 (all of the time). Higher scores indicate a higher level of social support. The maximum possible tangible scale score is 20. Scale scores were transformed to a 0–100-scale tangible support index for better comparison [21].
- Changes in living conditions and medical visits due to the COVID-19 pandemic. A specific questionnaire was designed and offered to the patients to determine pandemic-related questions.
2.4. Variables
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Study Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Velez-Montoya, R.; Oliver, S.C.; Olson, J.L.; Fine, S.L.; Quiroz-Mercado, H.; Mandava, N. Current knowledge and trends in age related macular degeneration: Genetics, epidemiology, and prevention. Retina 2014, 34, 423–441. [Google Scholar] [CrossRef]
- Kim, L.A.; D’Amore, P.A. A brief history of anti-VEGF for the treatment of ocular angiogenesis. Am. J. Pathol. 2012, 181, 376–379. [Google Scholar] [CrossRef] [Green Version]
- Finger, R.P.; Daien, V.; Eldem, B.M.; Talks, J.S.; Korobelnik, J.-F.; Mitchell, P.; Sakamoto, T.; Wong, T.Y.; Pantiri, K.; Carrasco, J. Anti-vascular endothelial growth factor in neovascular age-related macular degeneration—A systematic review of the impact of anti-VEGF on patient outcomes and healthcare systems. BMC Ophthalmol. 2020, 20, 294. [Google Scholar] [CrossRef]
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020, the right to sight: An analysis for the global burden of disease study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Ciulla, T.A.; Hussain, R.M.; Pollack, J.S.; Williams, D.F. Visual acuity outcomes and anti-vascular endothelial growth factor therapy intensity in neovascular age-related macular degeneration patients: A real-world analysis of 49 485 eyes. Ophthalmol Retina 2020, 4, 19–30. [Google Scholar] [CrossRef]
- Taylor, D.J.; Hobby, A.E.; Binns, A.M.; Crabb, D.P. How does age-related macular degeneration affect real-world visual ability and quality of life? A systematic review. BMJ Open 2016, 6, e011504. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline#event-76 (accessed on 15 October 2021).
- Agencia Estatal Boletin Oficial del Estado. Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Available online: https://www.boe.es/eli/es/rd/2020/03/14/463 (accessed on 15 October 2021).
- Agencia Estatal Boletin Oficial del Estado. Real Decreto 537/2020, de 22 de Mayo, por el que se Prorroga el Estado de Alarma Declarado por el Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Available online: https://www.boe.es/eli/es/rd/2020/05/22/537/con (accessed on 15 October 2021).
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: A meta-analysis of 59 studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Korobelnik, J.F.; Loewenstein, A.; Eldem, B.; Joussen, A.M.; Koh, A.; Lambrou, G.N.; Lanzetta, P.; Li, X.; Lövestam-Adrian, M.; Navarro, R.; et al. Guidance for anti-VEGF intravitreal injections during the COVID-19 pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Espanola de Retina y Vitreo. Recomendaciones Para la Atención a Pacientes Oftalmológicos en Relación con Emergencia COVID-19. Available online: https://serv.es/oftalmologia-COVID19/ (accessed on 22 March 2020).
- Lindeke-Myers, A.; Zhao, P.Y.C.; Meyer, B.I.; Liu, E.A.; Levine, D.A.; Bennett, O.M.; Ji, S.; Newman-Casey, P.A.; Rao, R.C.; Jain, N. Patient perceptions of SARS-CoV-2 exposure risk and association with continuity of ophthalmic care. JAMA Ophthalmol. 2021, 139, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística. Cifras Oficiales de Población Resultantes de la Revisión del Padrón Municipal a 1 de Enero. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=2852 (accessed on 15 October 2021).
- Instituto Nacional de Estadística. Indicadores de Estructura de la Población: Palencia. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=1488 (accessed on 15 October 2021).
- Evolución de Los Indicadores de Riesgo Por Provincias. Situación Epidemiológica del Coronavirus (COVID-19) en Castilla y León. Available online: https://analisis.datosabiertos.jcyl.es/pages/coronavirus/ (accessed on 1 December 2021).
- World Health Organization. Blindness and Vision Impairment. Available online: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment (accessed on 1 December 2021).
- EQ-5D. EQ-5D-3L|about. Available online: https://euroqol.org/eq-5d-instruments/eq-5d-3l-about/ (accessed on 1 December 2021).
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- MOS Social Support Survey. Description and Scoring Instructions: MOS Social Support Survey. Available online: https://cadc.ucsf.edu/sites/g/files/tkssra881/f/Description%20and%20Scoring%20Instructions%20MOS%20Social%20Support%20Survey.pdf (accessed on 1 December 2021).
- Holladay, J.T. Visual acuity measurements. J. Cataract. Refract. Surg. 2004, 30, 287–290. [Google Scholar] [CrossRef]
- Corazza, P.; D’Alterio, F.M.; Kabbani, J.; Alam, M.M.R.; Mercuri, S.; Orlans, H.O.; Younis, S. Long-term outcomes of intravitreal anti-VEGF therapies in patients affected by neovascular age-related macular degeneration: A real-life study. BMC Ophthalmol. 2021, 21, 300. [Google Scholar] [CrossRef]
- Upasani, D.; Dhingra, N. Ten-year outcome of anti-vascular endothelial growth factor treatment for neovascular age-related macular degeneration. Indian J. Ophthalmol. 2021, 69, 2350–2354. [Google Scholar] [CrossRef]
- Evans, R.N.; Reeves, B.C.; Phillips, D.; Muldrew, K.A.; Rogers, C.; Harding, S.P.; Chakravarthy, U.; IVAN Study Group. Long-term Visual Outcomes after Release from Protocol in Patients who Participated in the Inhibition of VEGF in Age-related Choroidal Neovascularisation (IVAN) Trial. Ophthalmology 2020, 127, 1191–1200. [Google Scholar] [CrossRef]
- Fasler, K.; Fu, D.J.; Moraes, G.; Wagner, S.; Gokhale, E.; Kortuem, K.; Chopra, R.; Faes, L.; Preston, G.; Pontikos, N.; et al. Moorfields AMD database report 2, fellow eye involvement with neovascular age-related macular degeneration. Br. J. Ophthalmol. 2020, 104, 684–690. [Google Scholar] [CrossRef]
- Longworth, L.; Yang, Y.; Young, T.; Mulhern, B.; Alava, M.H.; Mukuria, C.; Rowen, D.; Tosh, J.; Tsuchiya, A.; Evans, P.; et al. Use of generic and condition-specific measures of health-related quality of life in NICE decision-making: A systematic review, statistical modelling and survey. Health Technol. Assess. 2014, 18, 1–224. [Google Scholar] [CrossRef] [Green Version]
- Seland, J.H.; Vingerling, J.R.; Augood, C.A.; Bentham, G.; Chakravarthy, U.; DeJong, P.T.V.M.; Rahu, M.; Soubrane, G.; Tomazzoli, L.; Topouzis, F.; et al. Visual impairment and quality of life in the older European population, the EUREYE study. Acta Ophthalmol. 2011, 89, 608–613. [Google Scholar] [CrossRef] [Green Version]
- Mehta, H.; Kim, L.N.; Mathis, T.; Zalmay, P.; Ghanchi, F.; Amoaku, W.M.; Kodjikian, L. Trends in real-world neovascular AMD treatment outcomes in the UK. Clin. Ophthalmol. 2020, 14, 3331–3342. [Google Scholar] [CrossRef]
- Gillies, M.C.; Campain, A.; Barthelmes, D.; Simpson, J.M.; Arnold, J.J.; Guymer, R.H.; McAllister, I.L.; Essex, R.W.; Morlet, N.; Hunyor, A.P.; et al. Long-term outcomes of treatment of neovascular age-related macular degeneration: Data from an observational study. Ophthalmology 2015, 122, 1837–1845. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Estado de Salud Percibido por Estado de Salud Percibido por Edad y Periodo. Available online: https://www.ine.es/jaxi/Tabla.htm?path=/t00/ICV/dim3/&file=31304.px (accessed on 1 December 2021).
- Instituto Nacional de Estadística. National Health Survey. Available online: https://www.ine.es/CDINEbase/consultar.do?mes=&operacion=Encuesta+nacional+de+salud&id_oper=Ir (accessed on 15 October 2021).
- Instituto Nacional de Estadística. Available online: https://www.ine.es/prensa/experimental_ind_multi_calidad_vida.pdf (accessed on 8 March 2023).
- Péntek, M.; Brodszky, V.; Biró, Z.; Kölkedi, Z.; Dunai, Á.; Németh, J.; Baji, P.; Rencz, F.; Gulácsi, L.; Resch, M.D. Subjective health expectations of patients with age-related macular degeneration treated with antiVEGF drugs. BMC Geriatr. 2017, 17, 233. [Google Scholar] [CrossRef] [Green Version]
- Emrani, Z.; Akbari Sari, A.; Zeraati, H.; Olyaeemanesh, A.; Daroudi, R. Health-related quality of life measured using the EQ-5D-5L: Population norms for the capital of Iran. Health Qual. Life Outcomes 2020, 18, 108. [Google Scholar] [CrossRef]
- Hołownia-Voloskova, M.; Tarbastaev, A.; Golicki, D. Population norms of health-related quality of life in Moscow, Russia: The EQ-5D-5L-based survey. Qual. Life Res. 2021, 30, 831–840. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Czeisler, M.; Kennedy, J.L.; Wiley, J.F.; Facer-Childs, E.R.; Robbins, R.; Barger, L.K.; Czeisler, C.A.; Rajaratnam, S.M.W.; Howard, M.E. Delay or avoidance of routine, urgent and emergency medical care due to concerns about COVID-19 in a region with low COVID-19 prevalence: Victoria, Australia. Respirology 2021, 26, 707–712. [Google Scholar] [CrossRef]
- Gonzalez, D.; Karpman, M.; Haley, J.M. Coronavirus Concerns Led More Than 1 in 10 Nonelderly Adults to Delay or Forgo Health Care in Spring 2021; Coronavirus Pandemic (COVID-19) an RWJF Collection. Robert Wood Johson Fundation; Urban Institute: Washington, DC, USA, 2021. [Google Scholar]
- Borrelli, E.; Grosso, D.; Vella, G.; Sacconi, R.; Battista, M.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. Short-term outcomes of patients with neovascular exudative AMD: The effect of COVID-19 pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2621–2628. [Google Scholar] [CrossRef]


{kind=link}
| Mean ± SD [%] (95% CI) | ||
|---|---|---|
| Initial Survey | Final Survey | |
| Age (years) | 81.2 ± 7.1 (79.6–82.8) | 83.2 ± 7.1 (81.6–84.8) |
| Sex | ||
| Male | 33 [42.3%] (31.2–54.0) | |
| Female | 45 [57.7%] (46–68.8) | |
| Living conditions: | ||
| The patient lives alone | 23 [29.5%] (19.7–40.9) | 20 [25.6%] (16.4–36.8) |
| The patient lives with his or her family | 54 [69.2%] (57.8–79.2) | 55 [70.5%] (59.1–80.3) |
| The patient lives in a nursing home | 0 [0%] (0–4.6) | 2 [2.6%] (0.3–9.0) |
| Other (the patient lives with a friend) | 1 [1.3%] (0–6.9) | 1 [1.3%] (0.0–6.9) |
| Time from the beginning of the treatment (months) | 44.6 ± 26.6 [38.7–50.6] | 74.6 ± 27.1 [67.9–81.3] |
| Number of intravitreal injections applied per patient | 23.4 ± 13.3 [20.4–26.4] | 38.5 ± 17.3 [34.6–42.4] |
| BCVA of treated eyes—LogMAR | 0.66 ± 0.61 [0.55–0.77] | 0.77 ± 0.83 [0.63–0.92] |
| Visual impairment * | ||
| No impairment (≤0.3) | 52 [66.7%] (55.1–76.9) | 52 [66.7%] (55.1–76.9) |
| Mild impairment (>0.3–≤0.5) | 18 [23.1%] (14.3–34) | 13 [16.7%] (9.2–26.8) |
| Moderate impairment (>0.5–≤1) | 6 [7.7%] (2.9–16) | 9 [11.5%] (5.4–20.8) |
| Severe impairment (1–1.3) | 2 [2.6%] (0.3–9) | 2 [2.6%] (0.3–9) |
| Blindness (>1.3) | 0 [0%] (0–4.6) | 2 [2.6%] (0.3–9) |
| BCVA changes after treatment (eyes): | ||
| Improvement | 45 [38.5%] 29.6–47.9 | 57 [43.5%] 34.9–52.4 |
| No change | 26 [22.2%] 15.1–30.8 | 16 [12.2%] 7.1–19.1 |
| Worsening | 46 [39.3%] 30.4–48.8 | 58 [44.3%] 35.6–53.2 |
| EQ-5D-3L | Mobility Problems | Self-Care | Problems with Usual Activities | Pain/Discomfort | Anxiety/Depression | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Initial | Final | Initial | Final | Initial | Final | |
| Level 1 (no problems) | 48 [61.53%] | 44 [56.41%] | 72 [92.3%] | 58 [74.36%] | 58 [74.45%] | 43 [55.12%] | 24 [30.76%] | 26 [33.33%] | 56 [71.79%] | 59 [75.64%] |
| Level 2 (some problems) | 30 [38.46%] | 34 [43.58%] | 5 [6.41%] | 18 [23.08%] | 17 [21.79%] | 33 [42.31%] | 48 [61.53%] | 47 [60.26%] | 21 [26.92%] | 16 [20.51%] |
| Level 3 (severe problems) | 0 [0%] | 0 [0%] | 1 [1.28%] | 2 [2.56%] | 2 [2.56%] | 2 [2.56%] | 6 [7.69%] | 5 [6.41%] | 1 [1.28%] | 3 [3.85%] |
| Total | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] | 78 [100%] |
| Any problem | 30 [38.46%] | 34 [43.58%] | 6 [7.69%] | 20 [25.64%] | 19 [24.36%] | 35 [48.87%] | 54 [69.23%] | 52 [66.67%] | 22 [28.20%] | 19 [24.36%] |
| Change in any problem | p = 0.63 | p = 0.005 | p = 0.01 | p = 0.86 | p = 0.72 | |||||
| Any problem: Spanish 2012-NHS | 49.27% | 27.39% | 39.27% | 53.85% | 24.81% | |||||
| * Comparison of our sample with the Spanish 2012-NHS population (p value) | 0.072 | 0.374 | <0.001 | 0.841 | 0.008 | 0.369 | 0.008 | 0.029 | 0.563 | 1 |
| Initial Survey | Final Survey | |||
|---|---|---|---|---|
| VAS | Health Index | VAS | Health Index | |
| Sex | ||||
| Male | 82.090 | 0.810 | 73.180 | 0.790 |
| Female | 68.910 | 0.670 | 67.780 | 0.650 |
| p value | 0.002 | 0.001 | 0.155 | 0.009 |
| Age (years) | ||||
| Q1: 64–77 | 82.380 | 0.850 | 78.120 | 0.870 |
| Q2: 78–82 | 74.090 | 0.700 | 70.430 | 0.710 |
| Q3: 82–86 | 70.210 | 0.780 | 69.290 | 0.690 |
| Q4: 87–97 | 72.200 | 0.660 | 65.000 | 0.610 |
| p value | 0.114 | 0.014 | 0.017 | 0.000 |
| Receipt of treatment | ||||
| One eye | 79.670 | 0.770 | 72.820 | 0.730 |
| Both eyes | 69.310 | 0.690 | 67.310 | 0.690 |
| p value | 0.015 | 0.041 | 0.142 | 0.431 |
| Visual impairment | ||||
| No impairment (≤0.3) | 75.560 | 0.770 | 72.880 | 0.740 |
| Mild impairment (>0.3–≤0.5) | 72.440 | 0.660 | 65.380 | 0.660 |
| Moderate impairment (>0.5–≤1) | 67.000 | 0.600 | 65.450 | 0.680 |
| Severe impairment (1–1.3) | 87.500 | 0.720 | 52.500 | 0.430 |
| p value | 0.700 | 0.022 | 0.026 | 0.077 |
| Bilateral BCVA | ||||
| Q1: 0–0.1 | 87.250 | 0.880 | 76.670 | 0.860 |
| Q2: 0.2 | 73.000 | 0.760 | 76.110 | 0.760 |
| Q3: 0.3–0.4 | 73.630 | 0.750 | 70.320 | 0.690 |
| Q4: 0.5–1.3 | 72.350 | 0.650 | 61.250 | 0.620 |
| p value | 0.138 | 0.002 | 0.003 | 0.004 |
| n [%] (95% CI) | ||
|---|---|---|
| Initial Survey | Final Survey | |
| Availability of someone to help you if you are confined to bed | Mean score *: 4.3 ± 1.3 | Mean score *: 4.6 ± 0.9 |
| 1 None of the time | 5 [6.4%] (2.1–14.3) | 1 [1.3%] (0.0–6.9) |
| 2 A little of the time | 7 [9.0%] (3.7–17.6) | 5 [6.4%] (2.1–14.3) |
| 3 Some of the time | 5 [6.4%] (2.1–14.3) | 2 [2.6%] (0.3–9.9) |
| 4 Most of the time | 6 [7.7%] (2.9–16.0) | 7 [9.0%] (3.7–17.6) |
| 5 All the time | 55 [70.5%] (59.1–80.3) | 63 [80.8%] (70.3–88.8) |
| p value | 0.009 | |
| Availability of someone to take you to the doctor if you need it | Mean score *: 4.7 ± 0.7 | Mean score *: 4.6 ± 0.9 |
| None of the time | 0 [0%] (0–4.6) | 2 [2.6%] (0.3–9.0) |
| A little of the time | 3 [3.8%] (0.8–10.8) | 2 [2.6%] (0.3–9.0) |
| Some of the time | 3 [3.8%] (0.8–10.8) | 3 [3.8%] (0.8–10.8) |
| Most of the time | 5 [6.4%] (2.1–14.3) | 8 [10.3%] (4.5–19.2) |
| All the time | 67 [85.9%] (76.2–92.7) | 63 [80.8%] (70.3–88.8) |
| p value | 0.288 | |
| Availability of someone to prepare your meals if you are unable to do it yourself | Mean score *: 4.4 ± 1.1 | Mean score *: 4.7 ± 0.9 |
| None of the time | 3 [3.8%] (0.8–10.8) | 1 [1.3%] (0.0–6.9) |
| A little of the time | 4 [5.1%] (1.4–12.6) | 5 [6.4%] (2.1–14.3) |
| Some of the time | 7 [9.0%] (3.7–17.6) | 1 [1.3%] (0.0–6.9) |
| Most of the time | 7 [9.0%] (3.7–17.6) | 5 [6.4%] (2.1–14.3) |
| All the time | 57 [73.1%] (61.8–82.5) | 66 [84.6%] (74.7–91.8) |
| p value | 0.019 | |
| Availability of someone to help with daily chores if you were sick | Mean score *: 4.5 ± 1.1 | Mean score *: 4.7 ± 0.9 |
| None of the time | 1 [1.3%] (0.0–6.9) | 1 [1.3%] (0.0–6.9) |
| A little of the time | 7 [9.0%] (3.7–17.6) | 5 [6.4%] (2.1–14.3) |
| Some of the time | 6 [7.7%] (2.9–16.0) | 1 [1.3%] (0.0–6.9) |
| Most of the time | 5 [6.4%] (2.1–14.3) | 5 [6.4%] (2.1–14.3) |
| All the time | 59 [75.6%] (64.6–84.7) | 66 [84.6%] (74.7–91.8) |
| p value | 0.114 | |
| Initial Survey | Final Survey | |
|---|---|---|
| Subscale score (index) | ||
| Sex | ||
| Male | 19.09 (94.31) | 19.24 (95.25) |
| Female | 17.02 (81.37) | 18.11 (88.19) |
| p value | 0.009 | 0.136 |
| p value * | 0.207 | |
| The patient lives | ||
| Alone | 16.22 (76.38) | 16.35 (77.19) |
| With his or her family | 18.57 (91.06) | 19.52 (97) |
| In a nursing home | 20.00 (100) | |
| With friends | 20.00 (100) | |
| p value | 0.007 | 0.000 |
| p value * | 0.442 | |
| Situation | ||
| Keep on treatment | 18.18 (88.63) | 18.80 (92.5) |
| Keep on visiting, with no need of treatment | 17.12 (82) | 18.50 (90.63) |
| Keep on visiting, without treatment | 14.75 (67.19) | 15.25 (70.32) |
| p value | 0.049 | 0.067 |
| p value * | 0.791 | |
| Receive treatment | ||
| One eye | 17.95 (87.18) | 17.94 (87.12) |
| Both eyes | 17.85 (86.56) | 19.12 (94.50) |
| p value | 0.898 | 0.166 |
| p value * | 0.007 | |
| Bilateral BCVA | ||
| Q1 0–0.1 | 18.00 (87.50) | 17.57 (84.82) |
| Q2 0.2 | 18.29 (89.31) | 17.33 (83.32) |
| Q3 0.3–0.4 | 18.33 (89.56) | 19.62 (97.63) |
| Q4 0.5–1.3 | 17.15 (82.19) | 19.46 (97.63) |
| p value | 0.337 | 0.013 |
| p value * | 0.018 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanabria, M.R.; Calles-Monar, P.S.; Alonso-Tarancón, A.M.; Coco-Martín, R.M.; Mayo-Iscar, A. Impact of COVID-19 Confinement on Quality of Life of Patients with Age-Related Macular Degeneration: A Two-Wave Panel Study. J. Clin. Med. 2023, 12, 2394. https://doi.org/10.3390/jcm12062394
Sanabria MR, Calles-Monar PS, Alonso-Tarancón AM, Coco-Martín RM, Mayo-Iscar A. Impact of COVID-19 Confinement on Quality of Life of Patients with Age-Related Macular Degeneration: A Two-Wave Panel Study. Journal of Clinical Medicine. 2023; 12(6):2394. https://doi.org/10.3390/jcm12062394
Chicago/Turabian StyleSanabria, María R., Paola S. Calles-Monar, Ana M. Alonso-Tarancón, Rosa M. Coco-Martín, and Agustín Mayo-Iscar. 2023. "Impact of COVID-19 Confinement on Quality of Life of Patients with Age-Related Macular Degeneration: A Two-Wave Panel Study" Journal of Clinical Medicine 12, no. 6: 2394. https://doi.org/10.3390/jcm12062394