
Efficacy and Safety of Coadministered Ezetimibe–Rosuvastatin plus Telmisartan in South Korean Patients with Dyslipidemia and Hypertension: A Multicenter, Randomized, Double-Blind, Active-Controlled, Phase III Trial
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Efficacy Variables
2.4. Safety Evaluation
2.5. Drug Compliance
2.6. Statistical Analysis
2.7. Sample Size
3. Results
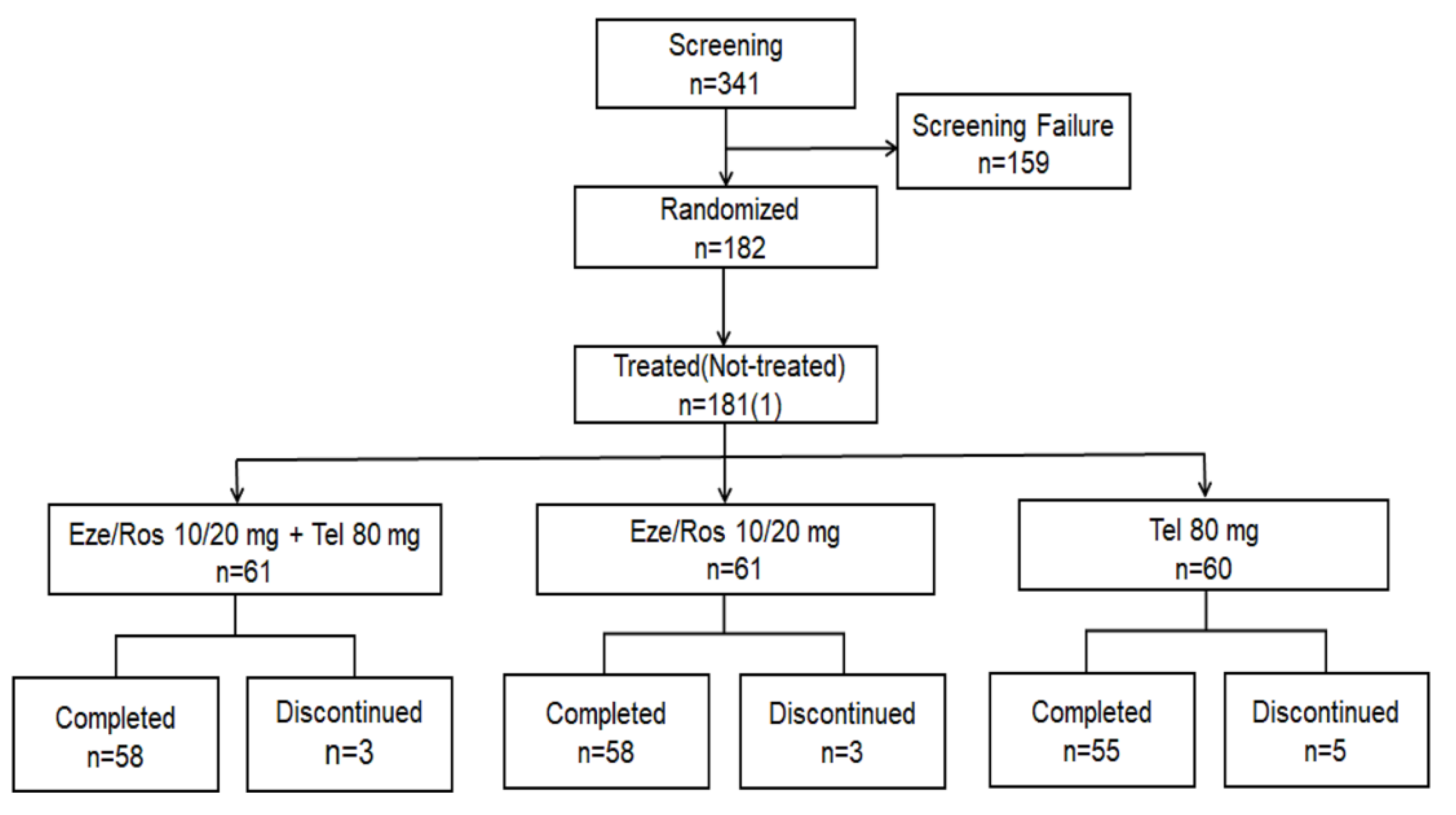
3.1. Study Population
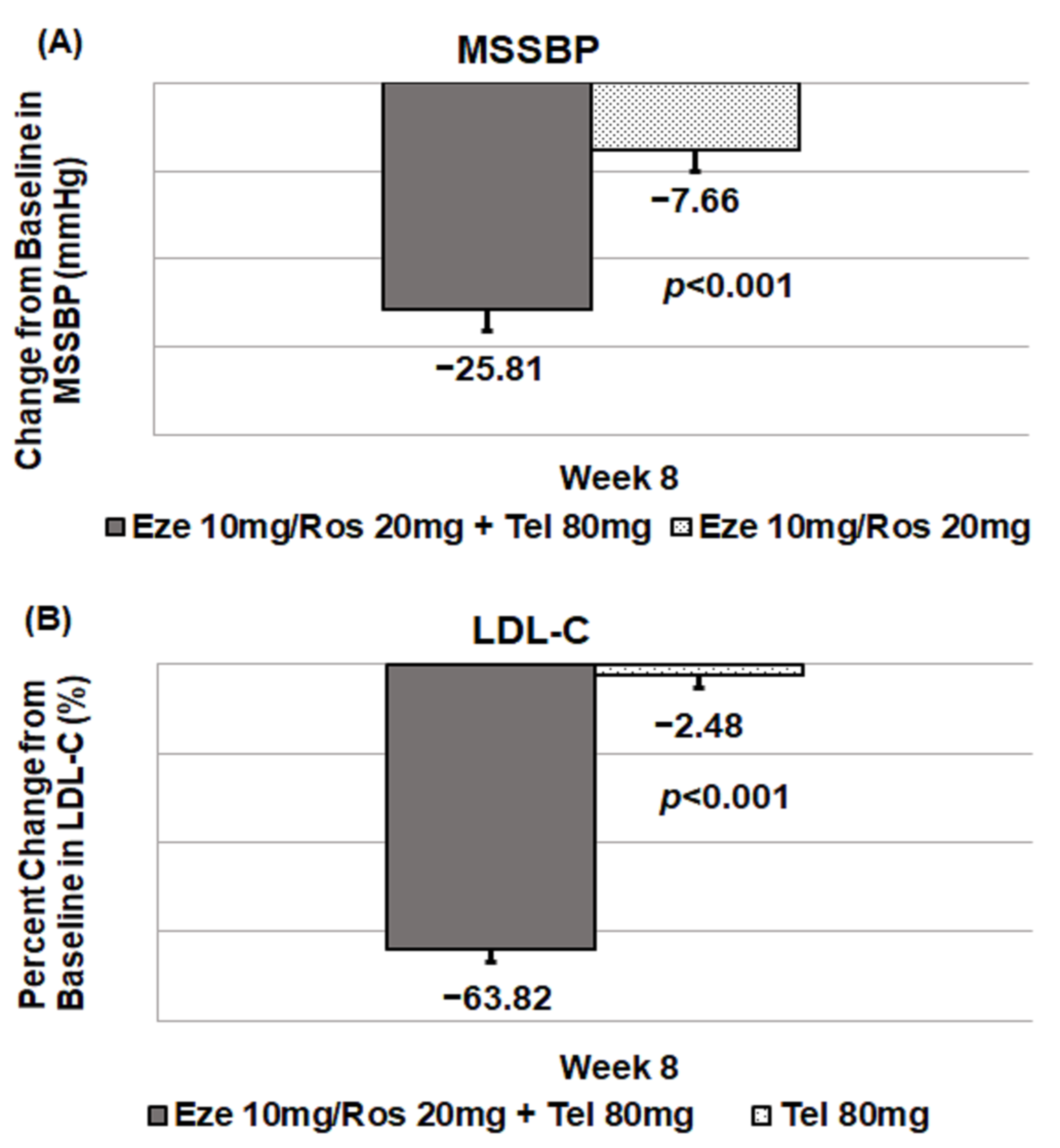
3.2. Primary Outcomes
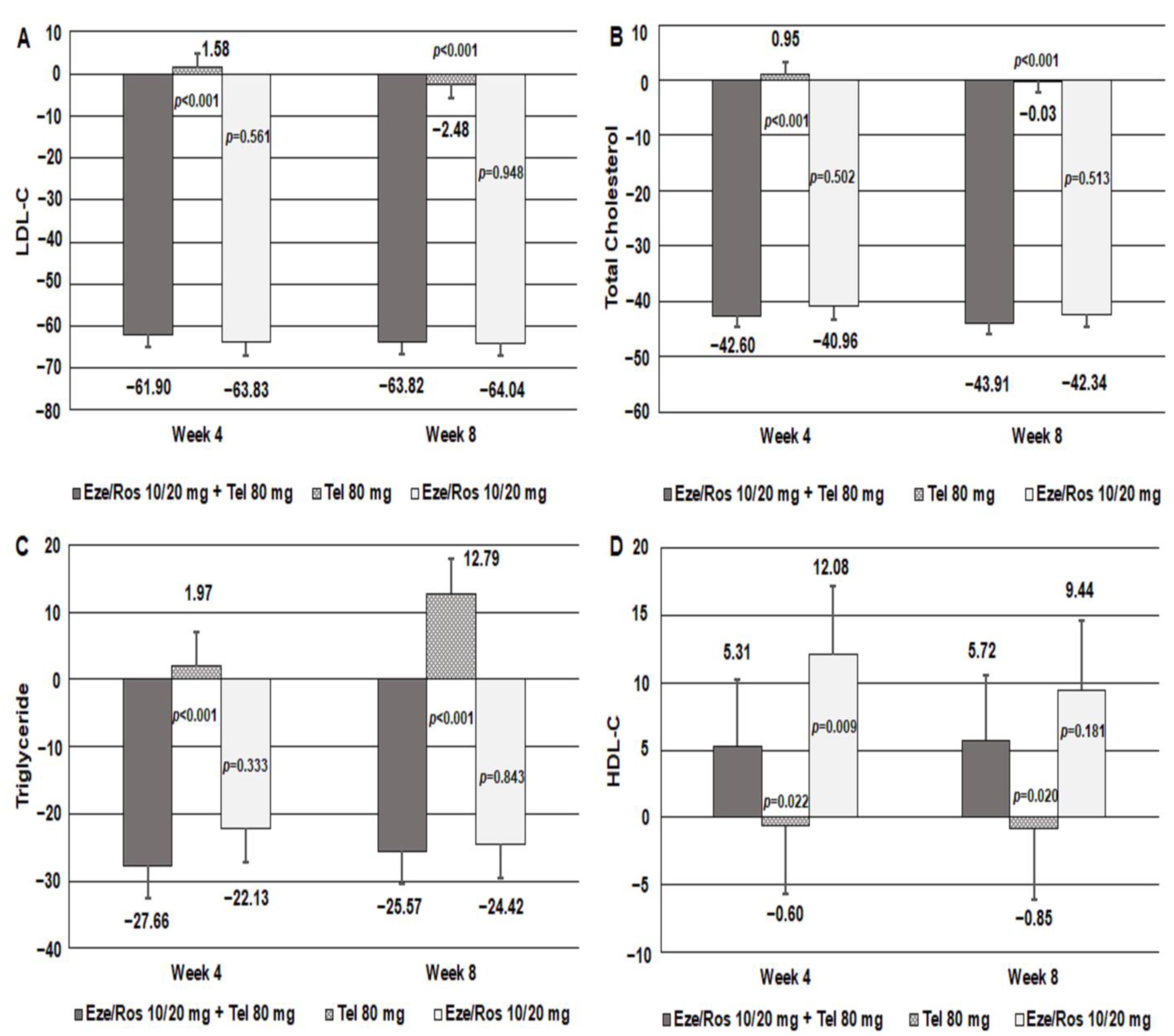
3.3. Secondary Outcomes
3.4. Safety Assessments
3.5. Adherence
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Egan, B.M.; Li, J.; Qanungo, S.; Wolfman, T.E. Blood pressure and cholesterol control in hypertensive hypercholesterolemic patients: National health and nutrition examination surveys 1988–2010. Circulation 2013, 128, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, R.; LaSalle, J.; Reeves, R.; Maroni, J.; Tarasenko, L.; Sun, F. Single-Pill Therapy in the Treatment of Concomitant Hypertension and Dyslipidemia (The Amlodipine/Atorvastatin Gemini Study). J. Clin. Hypertens. 2007, 7, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.L.; Pietz, K.; Battleman, D.S.; Beyth, R.J. Prevalence of comorbid hypertension and dyslipidemia and associated cardiovascular disease. Am. J. Manag. Care 2004, 10, 926–932. [Google Scholar]
- Dezii, C.M. A retrospective study of persistence with single-pill combination therapy vs. concurrent two-pill therapy in patients with hypertension. Manag. Care 2000, 9, 2–6. [Google Scholar]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Wang, Y.; Qiao, S.; Han, D.W.; Rong, X.R.; Wang, Y.X.; Xue, J.J.; Yang, J. Telmisartan Improves Insulin Resistance: A Meta-Analysis. Am. J. Ther. 2018, 25, e642–e651. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenney, J.M.; Jones, P.H.; Adamczyk, M.A.; Cain, V.A.; Bryzinski, B.S.; Blasetto, J.W.; Group, S.S. Comparison of the efficacy of rosuvastatin versus atorvastatin, simvastatin, and pravastatin in achieving lipid goals: Results from the STELLAR trial. Curr. Med. Res. Opin. 2003, 19, 689–698. [Google Scholar] [CrossRef]
- Waters, D.D.; Brotons, C.; Chiang, C.W.; Ferrieres, J.; Foody, J.; Jukema, J.W.; Santos, R.D.; Verdejo, J.; Messig, M.; McPherson, R.; et al. Lipid treatment assessment project 2: A multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goals. Circulation 2009, 120, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Farnier, M.; Freeman, M.W.; Macdonell, G.; Perevozskaya, I.; Davies, M.J.; Mitchel, Y.B.; Gumbiner, B.; Ezetimibe Study, G. Efficacy and safety of the coadministration of ezetimibe with fenofibrate in patients with mixed hyperlipidaemia. Eur. Heart J. 2005, 26, 897–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, G.C.; Han, J.K.; Han, K.H.; Hyon, M.S.; Doh, J.H.; Kim, M.H.; Jeong, J.O.; Bae, J.H.; Kim, S.H.; Yoo, B.S.; et al. Efficacy and Safety of Fixed-dose Combination Therapy With Telmisartan and Rosuvastatin in Korean Patients With Hypertension and Dyslipidemia: TELSTA-YU (TELmisartan-rosuvaSTAtin from YUhan), a Multicenter, Randomized, 4-arm, Double-blind, Placebo-controlled, Phase III Study. Clin. Ther. 2018, 40, 676–691.e671. [Google Scholar] [CrossRef] [PubMed]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Gupta, A.K.; Arshad, S.; Poulter, N.R. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: A meta-analysis. Hypertension 2010, 55, 399–407. [Google Scholar] [CrossRef] [Green Version]
- Benson, S.C.; Pershadsingh, H.A.; Ho, C.I.; Chittiboyina, A.; Desai, P.; Pravenec, M.; Qi, N.; Wang, J.; Avery, M.A.; Kurtz, T.W. Identification of telmisartan as a unique angiotensin II receptor antagonist with selective PPARgamma-modulating activity. Hypertension 2004, 43, 993–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruilope, L.M. Telmisartan for the management of patients at high cardiovascular risk. Curr. Med. Res. Opin. 2011, 27, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Bullano, M.F.; Wertz, D.A.; Yang, G.W.; Kamat, S.; Borok, G.M.; Gandhi, S.; McDonough, K.L.; Willey, V.J. Effect of rosuvastatin compared with other statins on lipid levels and National Cholesterol Education Program goal attainment for low-density lipoprotein cholesterol in a usual care setting. Pharmacotherapy 2006, 26, 469–478. [Google Scholar] [CrossRef]
- Phan, B.A.; Dayspring, T.D.; Toth, P.P. Ezetimibe therapy: Mechanism of action and clinical update. Vasc. Health Risk Manag. 2012, 8, 415–427. [Google Scholar] [CrossRef] [Green Version]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [Green Version]
- Bays, H.E.; Davidson, M.H.; Massaad, R.; Flaim, D.; Lowe, R.S.; Tershakovec, A.M.; Jones-Burton, C. Safety and efficacy of ezetimibe added on to rosuvastatin 5 or 10 mg versus up-titration of rosuvastatin in patients with hypercholesterolemia (the ACTE Study). Am. J. Cardiol. 2011, 108, 523–530. [Google Scholar] [CrossRef]
- Kim, B.K.; Hong, S.J.; Lee, Y.J.; Hong, S.J.; Yun, K.H.; Hong, B.K.; Heo, J.H.; Rha, S.W.; Cho, Y.H.; Lee, S.J.; et al. Long-term efficacy and safety of moderate-intensity statin with ezetimibe combination therapy versus high-intensity statin monotherapy in patients with atherosclerotic cardiovascular disease (RACING): A randomised, open-label, non-inferiority trial. Lancet 2022, 400, 380–390. [Google Scholar] [CrossRef]
- Jin, X.; Kim, M.H.; Han, K.H.; Hong, S.J.; Ahn, J.C.; Sung, J.H.; Cho, J.M.; Lee, H.C.; Choi, S.Y.; Lee, K.; et al. Efficacy and safety of co-administered telmisartan/amlodipine and rosuvastatin in subjects with hypertension and dyslipidemia. J. Clin. Hypertens. 2020, 22, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- Briasoulis, A.; Agarwal, V.; Valachis, A.; Messerli, F.H. Antihypertensive effects of statins: A meta-analysis of prospective controlled studies. J. Clin. Hypertens. 2013, 15, 310–320. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Kang, S.I.; Shin, D. Pharmacokinetic Interaction Between Telmisartan and Rosuvastatin/Ezetimibe After Multiple Oral Administration in Healthy Subjects. Adv. Ther. 2021, 38, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Huh, K.Y.; Lee, S.W.; Lee, S.B.; Kim, K.T.; Jang, I.J.; Lee, S. Pharmacokinetic Interaction Among Ezetimibe, Rosuvastatin, and Telmisartan. Clin. Pharmacol. Drug Dev. 2021, 10, 1290–1296. [Google Scholar] [CrossRef]
- Gandhi, S.K.; Jarbrink, K.; Fox, K.M.; Brandrup-Wognsen, G. Effectiveness of rosuvastatin in reducing LDL-C and target LDL-C goal attainment in real-world clinical practice. Curr. Med. Res. Opin. 2009, 25, 2817–2828. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.H.; Genest, J.; Gotto, A.M.; Kastelein, J.J.P.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Eze/Ros 10/20 mg + Tel 80 mg (n = 60) | Eze/Ros 10/20 mg (n = 60) | Tel 80 mg (n = 60) | p-Value | |
|---|---|---|---|---|
| Age (years) | 64.82 ± 10.07 | 62.92 ± 8.72 | 65.52 ± 10.63 | 0.1787 |
| Sex, Male, n (%) | 40 (66.67) | 40 (66.67) | 41 (68.33) | 0.9751 |
| Height (cm) | 163.20 ± 8.20 | 163.82 ± 8.54 | 163.22 ± 8.98 | 0.9053 |
| Weight (kg) | 69.39 ± 11.58 | 69.83 ± 12.42 | 69.62 ± 11.72 | 0.9736 |
| BMI (kg/m2) | 25.96 ± 3.18 | 25.91 ± 3.36 | 25.98 ± 2.70 | 0.9526 |
| CHD risk factors, n (%) | ||||
| Smoking | 12 (20.00) | 11 (18.33) | 7 (11.67) | 0.0776 |
| DBP ≥ 90 mmHg | 28 (46.67) | 30 (50.00) | 28 (46.67) | 0.9148 |
| HDL-C < 40 mg/dL | 19 (31.67) | 9 (15.00) | 13 (21.67) | 0.0907 |
| Family history of premature CHD | 4 (6.67) | 1 (1.67) | 1 (1.67) | 0.3702 |
| (−) HDL-C ≥ 60 mg/dL | 12 (20.00) | 16 (26.67) | 12 (20.00) | 0.5979 |
| Diabetes mellitus | 23 (38.33) | 25 (41.67) | 18 (30.00) | 0.3934 |
| Coronary arterial disease | 11 (18.33) | 15 (25.00) | 9 (15.00) | 0.3704 |
| 10-y risk > 20% | 12 (20.00) | 6 (10.00) | 7 (11.67) | 0.2369 |
| Duration of hypertension (months) | 112.03 ± 104.25 | 108.73 ± 71.22 | 101.66 ± 83.45 | 0.6564 |
| Duration of hyperlipidemia (months) | 87.74 ± 78.34 | 83.94 ± 54.20 | 76.35 ± 56.68 | 0.7049 |
| Baseline values | ||||
| MSSBP (mmHg) | 152.41 ± 9.69 | 154.91 ± 10.83 | 152.73 ± 9.15 | 0.3260 |
| MSDBP (mmHg) | 88.59 ± 10.59 | 89.74 ± 9.04 | 87.85 ± 9.84 | 0.5693 |
| Pulse (beats/min) | 70.62 ± 10.02 | 70.77 ± 9.49 | 72.25 ± 12.47 | 0.6124 |
| Total Cholesterol (mg/dL) | 209.45 ± 37.51 | 217.47 ± 32.27 | 217.87 ± 31.65 | 0.2739 |
| Triglyceride (mg/dL) | 162.32 ± 67.02 | 146.17 ± 61.72 | 158.07 ± 69.49 | 0.3763 |
| HDL-C (mg/dL) | 48.27 ± 12.47 | 50.97 ± 12.59 | 49.42 ± 11.57 | 0.4873 |
| LDL-C (mg/dL) | 149.28 ± 30.54 | 156.12 ± 29.99 | 156.55 ± 29.82 | 0.3894 |
| HbA1c (%) | 6.21 ± 0.83 | 6.13 ± 0.70 | 6.06 ± 0.68 | 0.7075 |
| Risk group classification, n (%) | ||||
| Group 1 (risk factor 0–1) | 4 (6.67) | 2 (3.33) | 3 (5.00) | |
| Group 2 (risk factor ≥ 2 and 10-year risk ≤ 20%) | 8 (13.33) | 9 (15.00) | 9 (15.00) | |
| Group 3 (CHD or CHD equivalence or 10-year risk >20%) | 46 (76.67) | 47 (78.33) | 47 (78.33) |
| Eze/Ros 10/20 mg + Tel 80 mg (n = 60) | Eze/Ros 10/20 mg (n = 60) | Tel 80 mg (n = 60) | |
|---|---|---|---|
| MSSBP (mmHg) | |||
| Baseline | 152.41 ± 9.69 | 154.91 ± 10.83 | 152.73 ± 9.15 |
| Week 4 | 129.62 ± 13.22 | 148.43 ± 14.17 | 137.98 ± 14.31 |
| MMRM | |||
| LS Means (SE) | −22.93 (2.11) | −5.85 (2.18) | −14.44 (2.20) |
| LS Mean Difference (SE) | −17.08 (2.37) | −8.49 (2.37) | |
| 95%CI | [−21.75, −12.41] | [−13.17, −3.81] | |
| p-value | <0.0001 | 0.0004 | |
| Week 8 | 126.43 ± 15.13 | 146.53 ± 16.73 | 136.95 ± 16.81 |
| MMRM | |||
| LS Means (SE) | −25.81 (2.34) | −7.66 (2.45) | −14.78 (2.49) |
| LS Mean Difference (SE) | −18.15 (2.83) | −11.03 (2.86) | |
| 95%CI | [−23.75, −12.56] | [−16.68, −5.38] | |
| p-value | <0.0001 | 0.0002 | |
| LDL-C (mg/dL) | |||
| Baseline | 149.28 ± 30.54 | 156.12 ± 29.99 | 156.55 ± 29.82 |
| Week 4 | 54.16 ± 30.19 | 52.57 ± 22.29 | 153.51 ± 36.12 |
| MMRM | |||
| LS Means (SE) | −61.90 (2.92) | −63.83 (3.07) | 1.58 (3.13) |
| LS Mean Difference (SE) | 1.93 (3.32) | −63.48 (3.35) | |
| 95%CI | [−4.62, 8.48] | [−70.09, −56.88] | |
| p-value | 0.5612 | <0.0001 | |
| Week 8 | 51.75 ± 23.49 | 52.62 ± 24.01 | 149.69 ± 41.34 |
| MMRM | |||
| LS Means (SE) | −63.82 (2.87) | −64.04 (3.07) | −2.48 (3.12) |
| LS Mean Difference (SE) | 0.21 (3.29) | −61.34 (3.33) | |
| 95%CI | [−6.28, 6.71] | [−67.91, −54.78] | |
| p-value | 0.9484 | <0.0001 |
| Eze/Ros 10/20 mg + Tel 80 mg (n = 61) | Eze/Ros 10/20 mg (n = 60) | Tel 80 mg (n = 60) | |
|---|---|---|---|
| Subjects with TEAEs | 9 (14.75) | 7 (11.67) | 7 (11.67) |
| Subjects with ADRs | 1 (1.64) | 3 (5.00) | 6 (10.00) |
| Asthenia | 0 | 0 | 1 (1.67) |
| Chest pain | 0 | 0 | 1 (1.67) |
| Ear pain | 0 | 0 | 1 (1.67) |
| Duodenal ulcer | 0 | 0 | 1 (1.67) |
| Neck pain | 0 | 0 | 1 (1.67) |
| Dizziness | 0 | 0 | 1 (1.67) |
| Hematuria | 1 (1.64) | 0 | 0 |
| Hypertension | 0 | 1 (1.67) | 0 |
| Atrial fibrillation | 0 | 0 | 1 (1.67) |
| Supraventricular tachycardia | 0 | 0 | 1 (1.67) |
| Alanine aminotransferase increased | 1 (1.64) | 2 (3.33) | 0 |
| Aspartate aminotransferase increased | 1 (1.64) | 2 (3.33) | 0 |
| Gamma-glutamyltransferase increased | 1 (1.64) | 1 (1.67) | 0 |
| Blood alkaline phosphatase increased | 1 (1.64) | 0 | 0 |
| Subjects with SAEs | 1 (1.64) | 0 | 0 |
| Subjects with Serious ADRs | 0 | 0 | 0 |
| Subjects with TEAEs Leading to Drug Interruption | 0 | 0 | 1 (1.67) |
| Subjects with TEAEs Leading to Drug Withdrawn | 0 | 0 | 1 (1.67) |
| Subjects with TEAEs Leading to Death | 0 | 0 | 0 |
| Subjects with ADRs Leading to Drug Interruption | 0 | 0 | 1 (1.67) |
| Subjects with ADRs Leading to Drug Withdrawn | 0 | 0 | 1 (1.67) |
| Subjects with ADRs Leading to Death | 0 | 0 | 0 |
| Variables | Eze/Ros 10/20 mg + Tel 80 mg (n = 60) | Eze/Ros 10/20 mg (n = 60) | Tel 80 mg (n = 60) | Total (n = 180) | p-Value |
|---|---|---|---|---|---|
| Compliance at week 4 (week 0~week 4) | 97.50 ± 7.09 | 97.28 ± 3.59 | 97.93 ± 4.18 | 97.56 ± 5.18 | 0.3059 |
| Subjects with Compliance ≥ 80% at week 4, n (%) | 59 (98.33) | 59 (98.33) | 55 (91.67) | 173 (96.11) | NC |
| Compliance at week 8 (week 4~week 8) | 97.20 ± 4.26 | 98.39 ± 3.08 | 97.78 ± 4.06 | 97.79 ± 3.84 | 0.3701 |
| Subjects with Compliance ≥ 80% at week 8, n (%) | 58 (96.67) | 58 (96.67) | 55 (91.67) | 171 (95.00) | NC |
| Overall Compliance | 97.16 ± 4.55 | 97.87 ± 2.48 | 96.62 ± 8.21 | 97.21 ± 5.60 | 0.4567 |
| Subjects with Compliance ≥ 80%, n (%) | 60 (100.00) | 60 (100.00) | 58 (96.67) | 178 (98.89) | 0.3296 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Z.-Y.; Kim, M.-H.; Lee, H.-C.; Park, S.-J.; Rhee, M.-Y.; Choi, J.-I.; Kim, S.-H.; Chae, I.-H.; Hong, Y.-J.; Lee, N.-H.; et al. Efficacy and Safety of Coadministered Ezetimibe–Rosuvastatin plus Telmisartan in South Korean Patients with Dyslipidemia and Hypertension: A Multicenter, Randomized, Double-Blind, Active-Controlled, Phase III Trial. J. Clin. Med. 2023, 12, 2377. https://doi.org/10.3390/jcm12062377
Song Z-Y, Kim M-H, Lee H-C, Park S-J, Rhee M-Y, Choi J-I, Kim S-H, Chae I-H, Hong Y-J, Lee N-H, et al. Efficacy and Safety of Coadministered Ezetimibe–Rosuvastatin plus Telmisartan in South Korean Patients with Dyslipidemia and Hypertension: A Multicenter, Randomized, Double-Blind, Active-Controlled, Phase III Trial. Journal of Clinical Medicine. 2023; 12(6):2377. https://doi.org/10.3390/jcm12062377
Chicago/Turabian StyleSong, Zhao-Yan, Moo-Hyun Kim, Han-Cheol Lee, Sung-Ji Park, Moo-Yong Rhee, Jong-Il Choi, Sang-Hyun Kim, In-Ho Chae, Young-Joon Hong, Nam-Ho Lee, and et al. 2023. "Efficacy and Safety of Coadministered Ezetimibe–Rosuvastatin plus Telmisartan in South Korean Patients with Dyslipidemia and Hypertension: A Multicenter, Randomized, Double-Blind, Active-Controlled, Phase III Trial" Journal of Clinical Medicine 12, no. 6: 2377. https://doi.org/10.3390/jcm12062377