
Audiovisual Training in Virtual Reality Improves Auditory Spatial Adaptation in Unilateral Hearing Loss Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
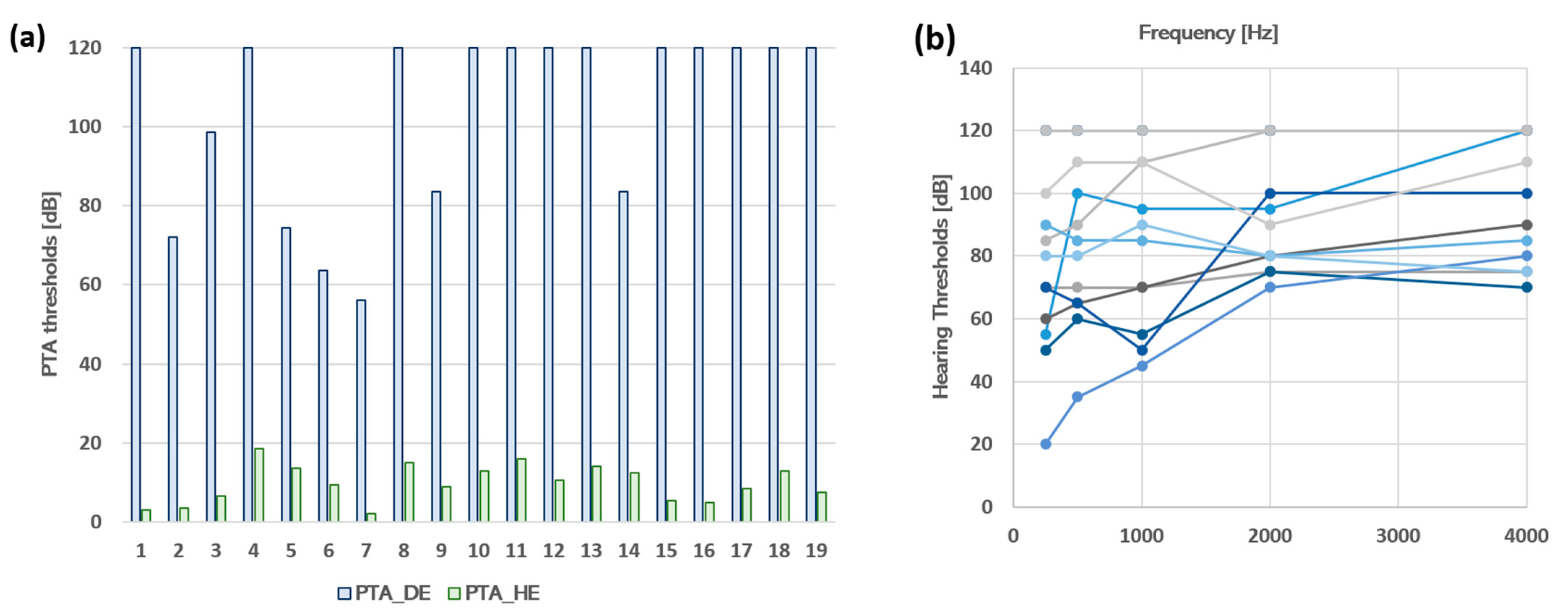
2.1. Population
2.2. Experimental Sessions
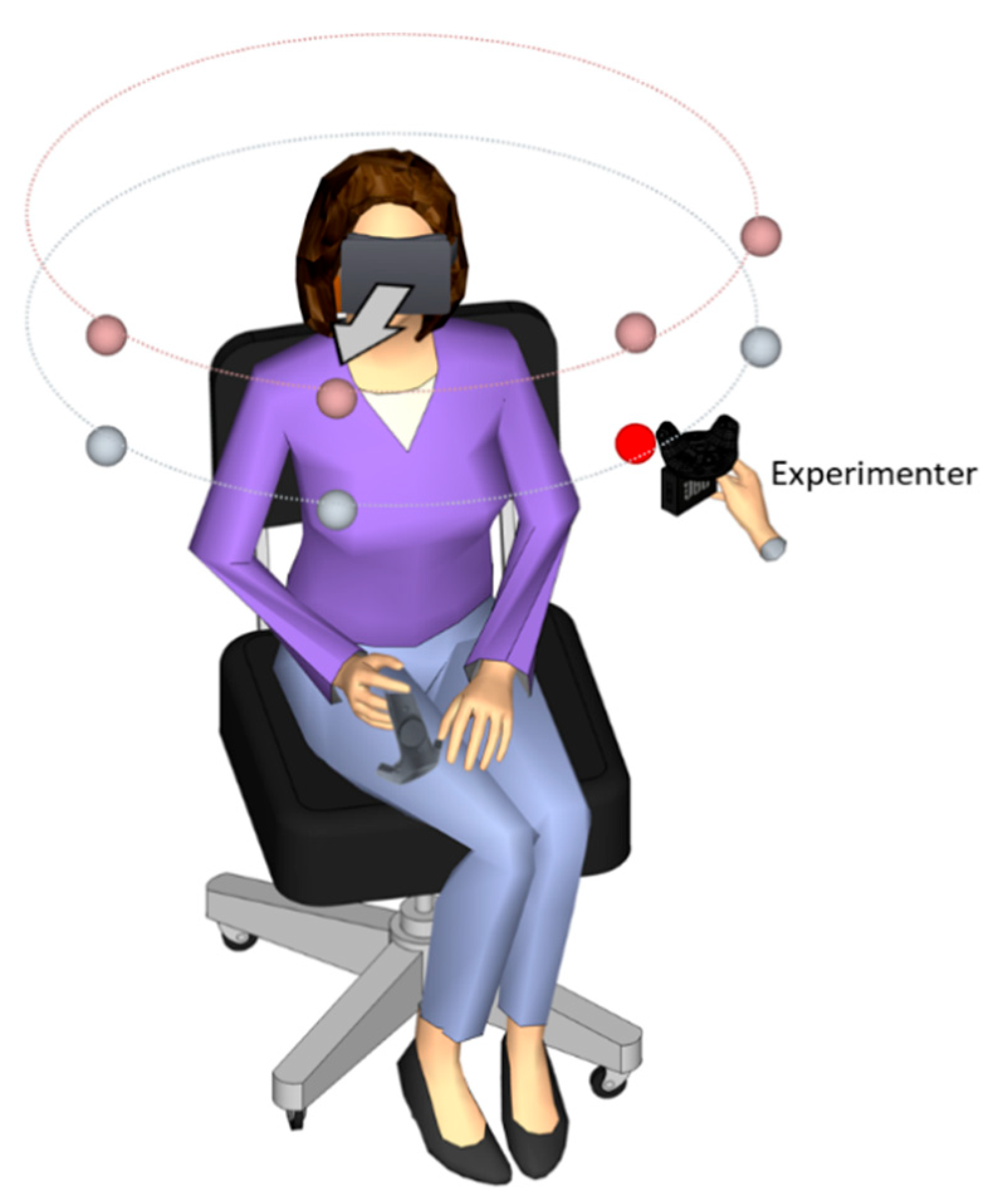
2.3. Description of the VR material
2.4. Experimental Procedure of Head-Pointing Localization Test (LOCATEST)
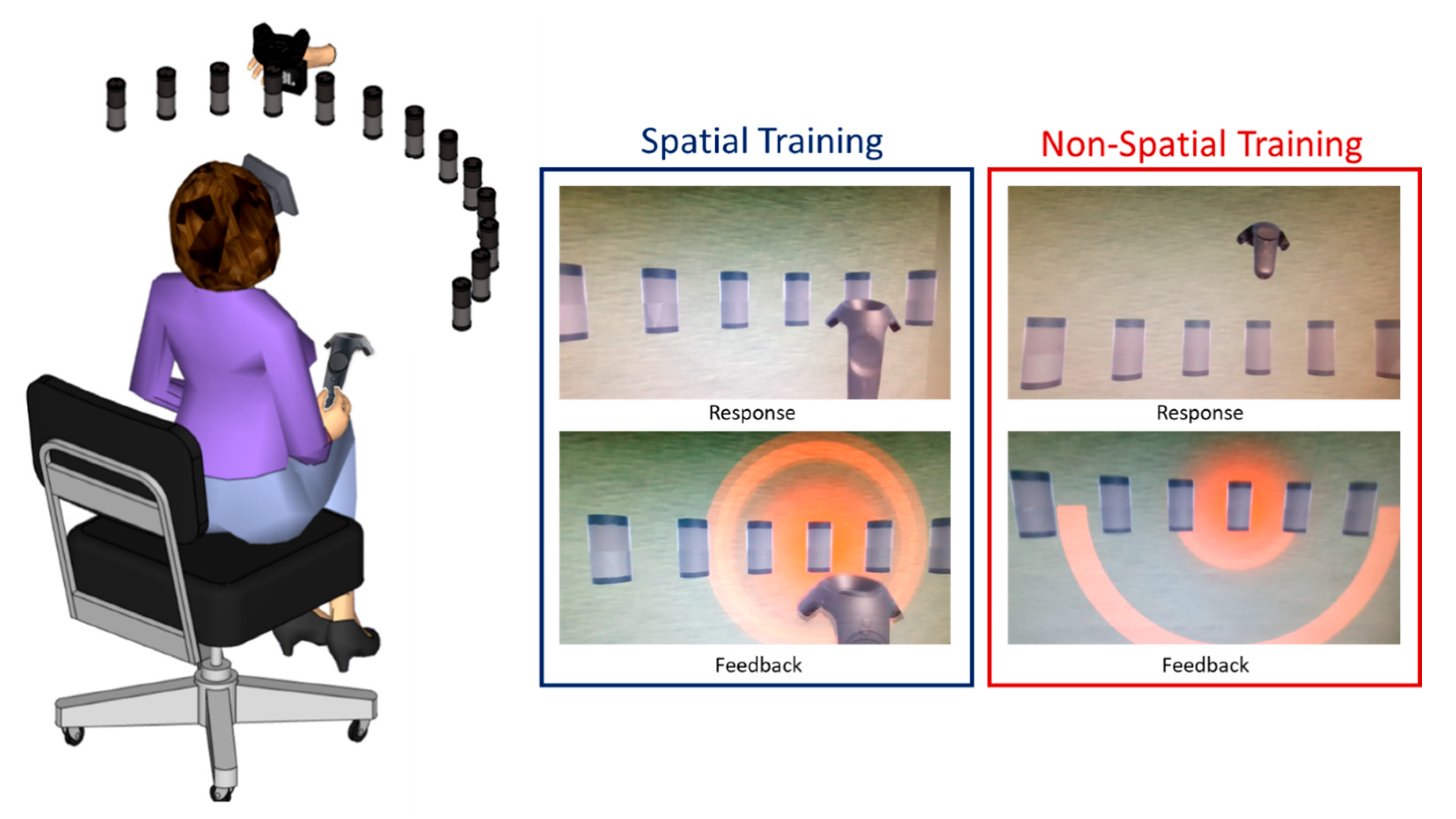
2.5. Experimental Procedure of Spatial Training
2.6. Experimental Procedure of Non-Spatial Training
2.7. Data Analysis
2.7.1. Head-Pointing Localization Performances (LOCATEST)
2.7.2. Performances during Audiovisual Training
3. Results
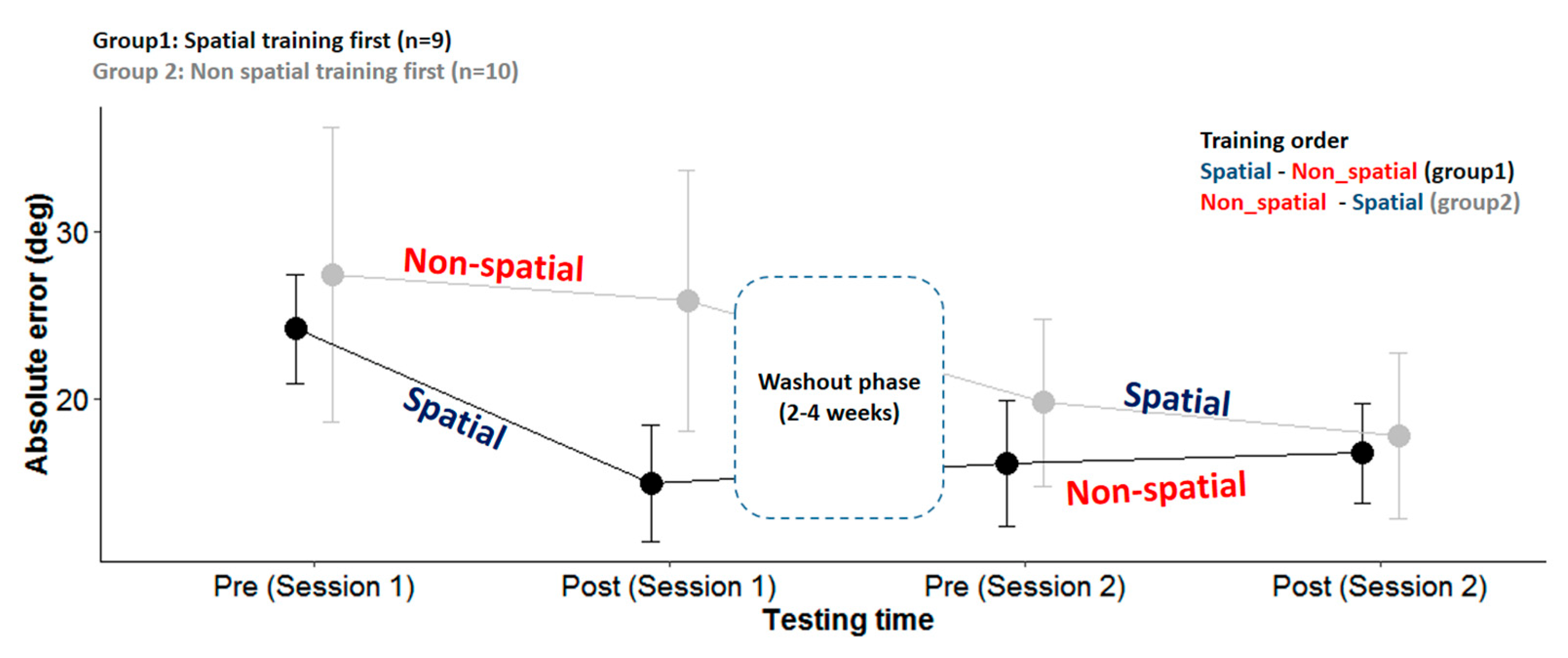
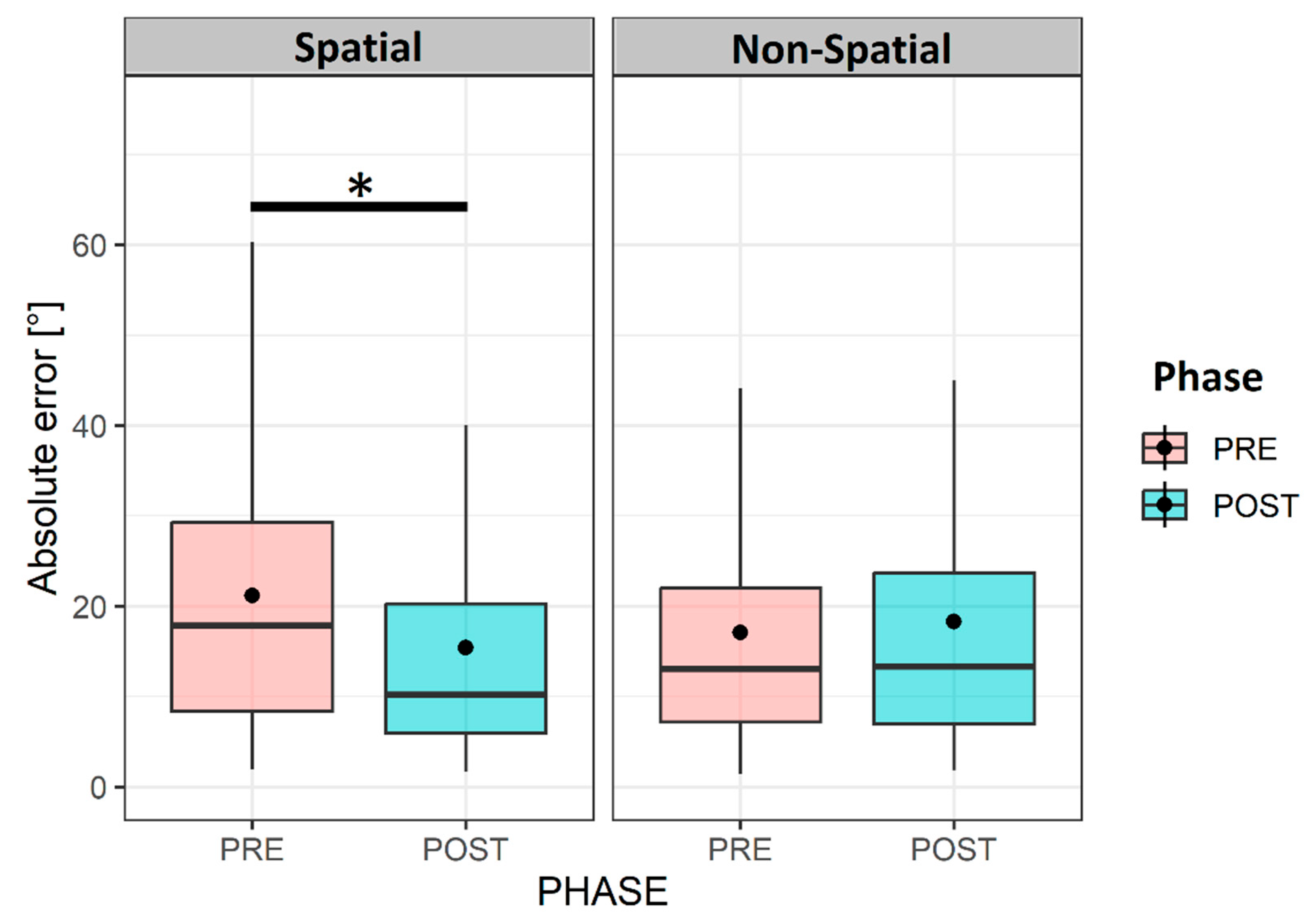
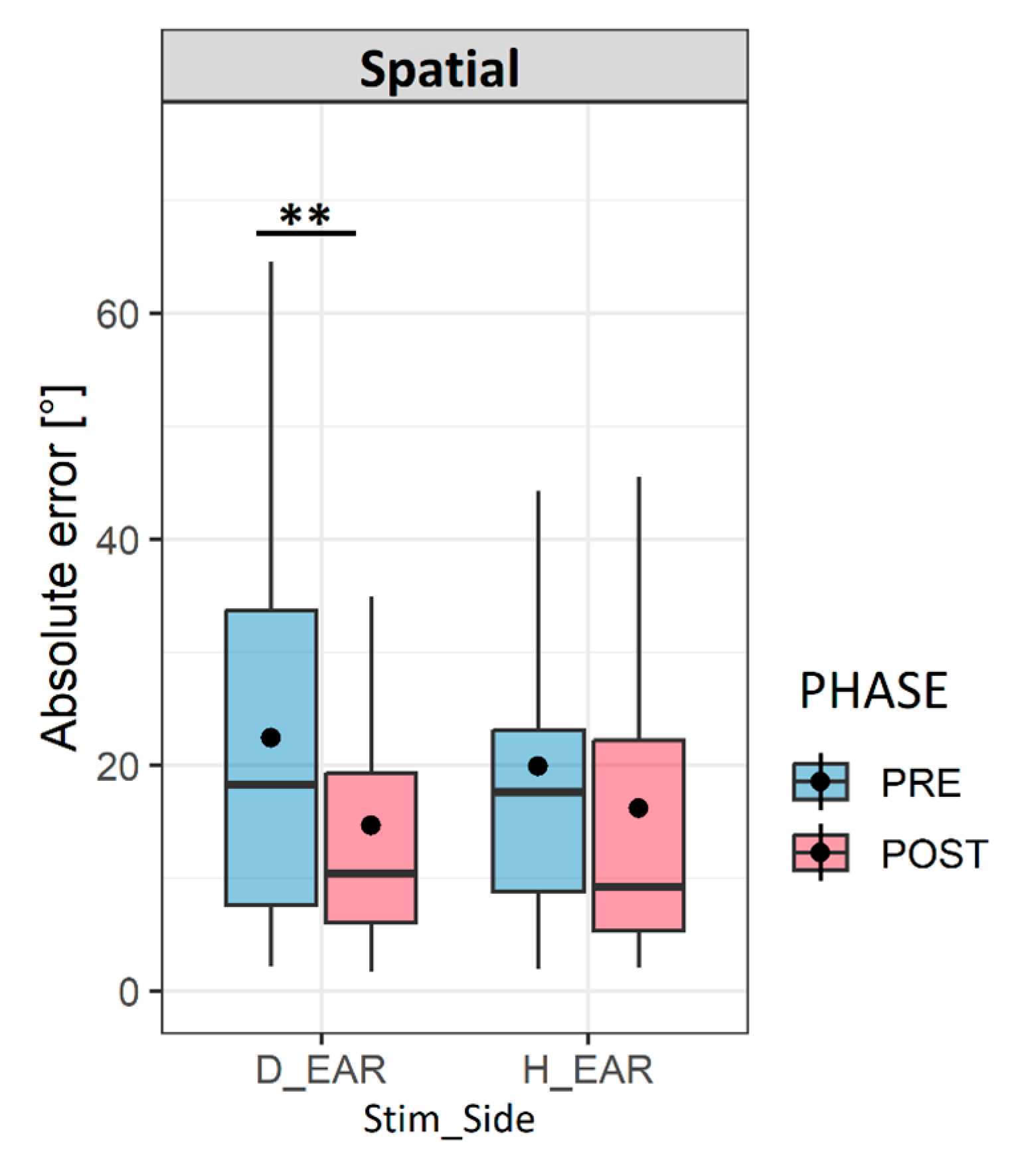
3.1. Performances in Head-Pointing Localization (LOCATEST)
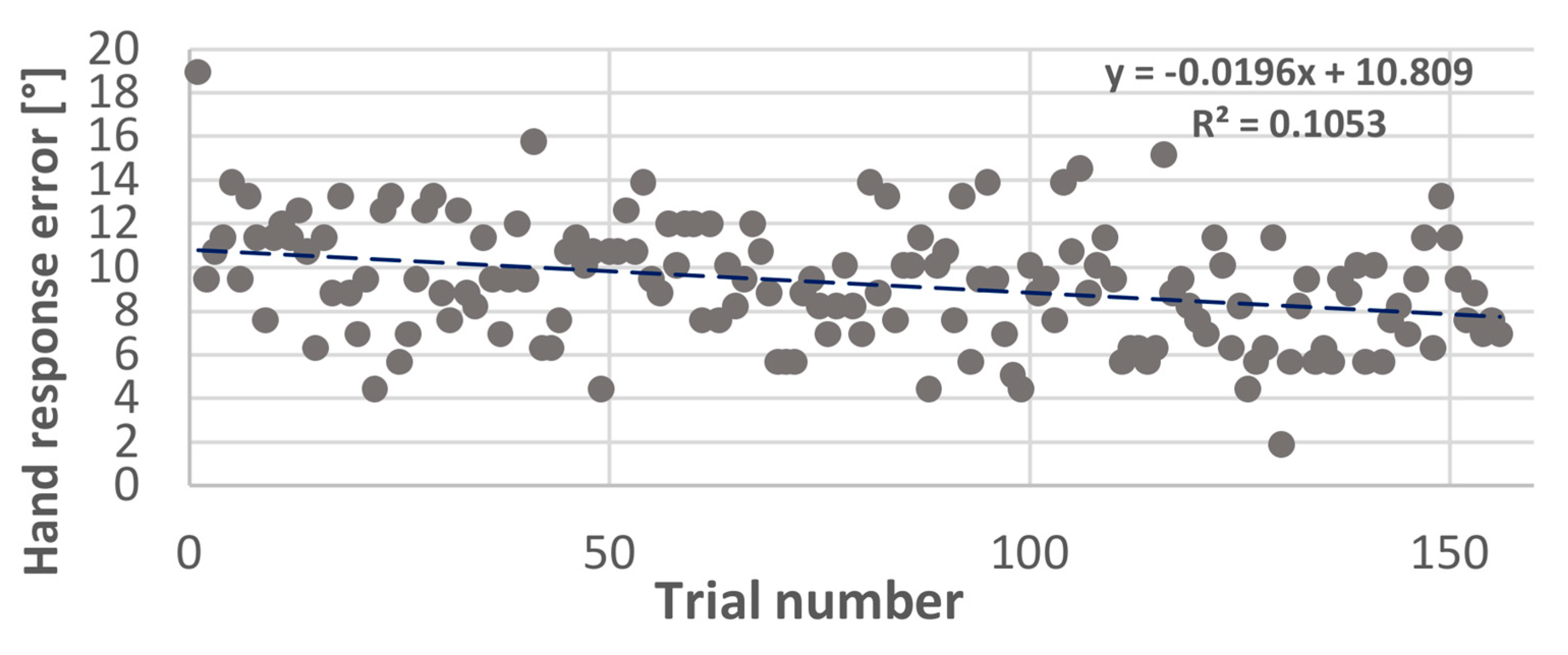
3.2. Performance during Audiovisual Training
4. Discussion
4.1. Effect of Audiovisual Training on Spatial Hearing Abilities in UHL
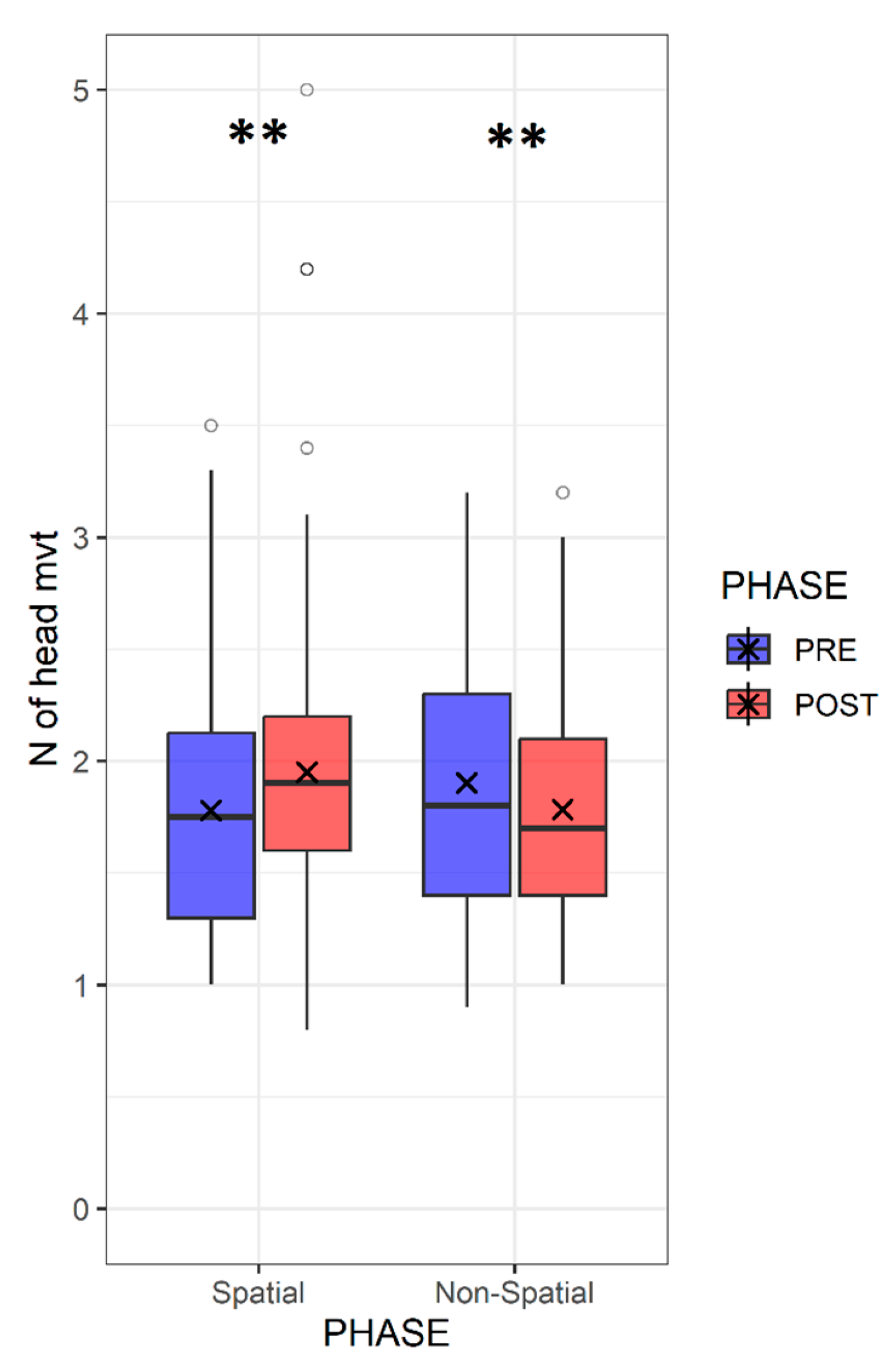
4.2. Re-Learning to Move the Head Effectively
4.3. Clinical Relevance of Motion-Tracked Virtual Reality in Treating Auditory Deficit
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bronkhorst, A.W.; Plomp, R. Binaural speech intelligibility in noise for hearing-impaired listeners. J. Acoust. Soc. Am. 1989, 86, 1374–1383. [Google Scholar] [CrossRef] [PubMed]
- Keating, P.; King, A.J. Developmental plasticity of spatial hearing following asymmetric hearing loss: Context-dependent cue integration and its clinical implications. Front. Syst. Neurosci. 2013, 7, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, P.; Rosenior-Patten, O.; Dahmen, J.C.; Bell, O.; King, A.J. Behavioral training promotes multiple adaptive processes following acute hearing loss. Elife 2016, 5, e12264. [Google Scholar] [CrossRef] [PubMed]
- Barone, P.; Lacassagne, L.; Kral, A. Reorganization of the Connectivity of Cortical Field DZ in Congenitally Deaf Cat. PLoS ONE 2013, 8, e60093. [Google Scholar] [CrossRef] [PubMed]
- Gordon, K.; Kral, A. Animal and human studies on developmental monaural hearing loss. Heart Res. 2019, 380, 60–74. [Google Scholar] [CrossRef]
- Slattery, W.H.; Middlebrooks, J.C. Monaural sound localization: Acute versus chronic unilateral impairment. Heart Res. 1994, 75, 38–46. [Google Scholar] [CrossRef]
- Hofman, P.M.; van Riswick, J.G.; van Opstal, J. Relearning sound localization with new ears. Nat. Neurosci. 1998, 1, 417–421. [Google Scholar] [CrossRef]
- King, A.J.; Parsons, C.H.; Moore, D.R. Plasticity in the neural coding of auditory space in the mammalian brain. Proc. Natl. Acad. Sci. USA 2000, 97, 11821–11828. [Google Scholar] [CrossRef] [Green Version]
- Hendrikse, M.M.E.; Grimm, G.; Hohmann, V. Evaluation of the Influence of Head Movement on Hearing Aid Algorithm Performance Using Acoustic Simulations. Trends Heart 2020, 24. [Google Scholar] [CrossRef]
- Ausili, S.A.; Agterberg, M.J.H.; Engel, A.; Voelter, C.; Thomas, J.P.; Brill, S.; Snik, A.F.M.; Dazert, S.; Van Opstal, A.J.; Mylanus, E.A.M. Spatial Hearing by Bilateral Cochlear Implant Users with Temporal Fine-Structure Processing. Front. Neurol. 2020, 11, 915. [Google Scholar] [CrossRef]
- Perrett, S.; Noble, W. The contribution of head motion cues to localization of low-pass noise. Percept. Psychophys. 1997, 59, 1018–1026. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, E.; Knudsen, P. Vision calibrates sound localization in developing barn owls. J. Neurosci. 1989, 9, 3306–3313. [Google Scholar] [CrossRef]
- Kacelnik, O.; Nodal, F.R.; Parsons, C.H.; King, A.J. Training-Induced Plasticity of Auditory Localization in Adult Mammals. PLoS Biol. 2006, 4, e71. [Google Scholar] [CrossRef]
- Valzolgher, C.; Alzhaler, M.; Gessa, E.; Todeschini, M.; Nieto, P.; Verdelet, G.; Salemme, R.; Gaveau, V.; Marx, M.; Truy, E.; et al. The impact of a visual spatial frame on real sound-source localization in virtual reality. Curr. Res. Behav. Sci. 2020, 1, 100003. [Google Scholar] [CrossRef]
- Strelnikov, K.; Rosito, M.; Barone, P. Effect of Audiovisual Training on Monaural Spatial Hearing in Horizontal Plane. PLoS ONE 2011, 6, e18344. [Google Scholar] [CrossRef] [Green Version]
- Valzolgher, C.; Todeschini, M.; Verdelet, G.; Gatel, J.; Salemme, R.; Gaveau, V.; Truy, E.; Farnè, A.; Pavani, F. Adapting to altered auditory cues: Generalization from manual reaching to head pointing. PLoS ONE 2022, 17, e0263509. [Google Scholar] [CrossRef]
- Valzolgher, C.; Gatel, J.; Bouzaid, S.; Grenouillet, S.; Todeschini, M.; Verdelet, G.; Salemme, R.; Gaveau, V.; Truy, E.; Farnè, A.; et al. Reaching to Sounds Improves Spatial Hearing in Bilateral Cochlear Implant Users. Ear Heart 2022, 44, 189–198. [Google Scholar] [CrossRef]
- Valzolgher, C.; Verdelet, G.; Salemme, R.; Lombardi, L.; Gaveau, V.; Farné, A.; Pavani, F. Reaching to sounds in virtual reality: A multisensory-motor approach to promote adaptation to altered auditory cues. Neuropsychologia 2020, 149, 107665. [Google Scholar] [CrossRef]
- Nodal, F.R.; Kacelnik, O.; Bajo, V.M.; Bizley, J.K.; Moore, D.R.; King, A.J. Lesions of the Auditory Cortex Impair Azimuthal Sound Localization and Its Recalibration in Ferrets. J. Neurophysiol. 2010, 103, 1209–1225. [Google Scholar] [CrossRef] [Green Version]
- Falchier, A.; Schroeder, C.E.; Hackett, T.A.; Lakatos, P.; Nascimento-Silva, S.; Ulbert, I.; Karmos, G.; Smiley, J.F. Projection from Visual Areas V2 and Prostriata to Caudal Auditory Cortex in the Monkey. Cereb. Cortex 2009, 20, 1529–1538. [Google Scholar] [CrossRef] [Green Version]
- Rauschecker, J.P.; Tian, B. Mechanisms and streams for processing of “what” and “where” in auditory cortex. Proc. Natl. Acad. Sci. USA 2000, 97, 11800–11806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coudert, A.; Verdelet, G.; Reilly, K.T.; Truy, E.; Gaveau, V. Intensive Training of Spatial Hearing Promotes Auditory Abilities of Bilateral Cochlear Implant Adults: A Pilot Study. Ear Heart 2022, 44, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Coudert, A.; Gaveau, V.; Gatel, J.; Verdelet, G.; Salemme, R.; Farne, A.; Pavani, F.; Truy, E. Spatial Hearing Difficulties in Reaching Space in Bilateral Cochlear Implant Children Improve with Head Movements. Ear Heart 2021, 43, 192–205. [Google Scholar] [CrossRef] [PubMed]
- Heffner, R.S.; Heffner, H.E. Visual Factors in Sound Localization in Mammals. J. Comp. Neurol. 1992, 317, 219–232. [Google Scholar] [CrossRef]
- Bulkin, D.A.; Groh, J.M. Seeing sounds: Visual and auditory interactions in the brain. Curr. Opin. Neurobiol. 2006, 16, 415–419. [Google Scholar] [CrossRef]
- Isaiah, A.; Hartley, D.E. Can training extend current guidelines for cochlear implant candidacy? Neural Regen. Res. 2015, 10, 718–720. [Google Scholar] [CrossRef]
- Blauert, J. Spatial Hearing: The Psychophysics of Human Sound Localization; MIT Press: Cambridge, MA, USA, 2001. [Google Scholar]
- Middlebrooks, J.C.; Green, D.M. Sound Localization by Human Listeners. Annu. Rev. Psychol. 1991, 42, 135–159. [Google Scholar] [CrossRef]
- Gessa, E.; Giovanelli, E.; Spinella, D.; Verdelet, G.; Farnè, A.; Frau, G.N.; Pavani, F.; Valzolgher, C. Spontaneous head-movements improve sound localization in aging adults with hearing loss. Front. Hum. Neurosci. 2022, 16. [Google Scholar] [CrossRef]
- Kumpik, D.P.; King, A.J. A review of the effects of unilateral hearing loss on spatial hearing. Heart Res. 2018, 372, 17–28. [Google Scholar] [CrossRef]
- Makous, J.C.; Middlebrooks, J.C. Two-dimensional sound localization by human listeners. J. Acoust. Soc. Am. 1990, 87, 2188–2200. [Google Scholar] [CrossRef]
- Alzaher, M.; Vannson, N.; Deguine, O.; Marx, M.; Barone, P.; Strelnikov, K. Brain plasticity and hearing disorders. Rev. Neurol. 2021, 177, 1121–1132. [Google Scholar] [CrossRef]
- Van Wanrooij, M.M.; Van Opstal, A.J. Contribution of Head Shadow and Pinna Cues to Chronic Monaural Sound Localization. J. Neurosci. 2004, 24, 4163–4171. [Google Scholar] [CrossRef] [Green Version]
- Freigang, C.; Schmiedchen, K.; Nitsche, I.; Rübsamen, R. Free-field study on auditory localization and discrimination performance in older adults. Exp. Brain Res. 2014, 232, 1157–1172. [Google Scholar] [CrossRef]
- Brimijoin, W.O.; Akeroyd, M. The moving minimum audible angle is smaller during self motion than during source motion. Front. Neurosci. 2014, 8, 273. [Google Scholar] [CrossRef] [Green Version]
- Brimijoin, W.O.; McShefferty, D.; Akeroyd, M.A. Undirected head movements of listeners with asymmetrical hearing impairment during a speech-in-noise task. Heart Res. 2012, 283, 162–168. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Gender | Age | D. Onset | Side of Deafness | Etiology of Deafness |
|---|---|---|---|---|---|
| UHL 01 | M | 37 | 5 | R | Sudden |
| UHL 02 | M | 20 | 16 | R | Congenital |
| UHL 03 | F | 43 | 12 | R | Granulome |
| UHL 04 | F | 56 | 7 | L | Facial paralysia |
| UHL 05 | F | 55 | 21 | L | Unknown |
| UHL 06 | M | 44 | 2 | R | Unknown |
| UHL 07 | F | 47 | 8 | R | Sudden |
| UHL 08 | F | 70 | 64 | L | Tympanic lesion |
| UHL 09 | M | 60 | 13 | L | Unknown |
| UHL 10 | F | 65 | 5 | L | Vestibular schwanoma |
| UHL 11 | M | 69 | 3 | L | Vestibular schwanoma |
| UHL 12 | F | 56 | 3 | L | Vestibular schwanoma |
| UHL 13 | F | 59 | 4 | L | Congenital |
| UHL 14 | M | 48 | 10 | L | Neurinoma |
| UHL 15 | M | 55 | 5 | R | Vestibular schwanoma |
| UHL 16 | M | 55 | 11 | R | Intracochlear schwanoma |
| UHL 17 | F | 47 | 8 | R | Unknown |
| UHL 18 | F | 59 | 59 | L | Congenital |
| UHL 19 | F | 43 | 1 | R | Cholestéatome |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzaher, M.; Valzolgher, C.; Verdelet, G.; Pavani, F.; Farnè, A.; Barone, P.; Marx, M. Audiovisual Training in Virtual Reality Improves Auditory Spatial Adaptation in Unilateral Hearing Loss Patients. J. Clin. Med. 2023, 12, 2357. https://doi.org/10.3390/jcm12062357
Alzaher M, Valzolgher C, Verdelet G, Pavani F, Farnè A, Barone P, Marx M. Audiovisual Training in Virtual Reality Improves Auditory Spatial Adaptation in Unilateral Hearing Loss Patients. Journal of Clinical Medicine. 2023; 12(6):2357. https://doi.org/10.3390/jcm12062357
Chicago/Turabian StyleAlzaher, Mariam, Chiara Valzolgher, Grégoire Verdelet, Francesco Pavani, Alessandro Farnè, Pascal Barone, and Mathieu Marx. 2023. "Audiovisual Training in Virtual Reality Improves Auditory Spatial Adaptation in Unilateral Hearing Loss Patients" Journal of Clinical Medicine 12, no. 6: 2357. https://doi.org/10.3390/jcm12062357