

Elevated Bile Acid Is Associated with Worsened Impaired Glucose Homeostasis in Pancreatic Ductal Adenocarcinoma Patients with Extrahepatic Cholestasis through Increased Hepatic Insulin Clearance

Abstract
:1. Introduction
2. Materials and Methods
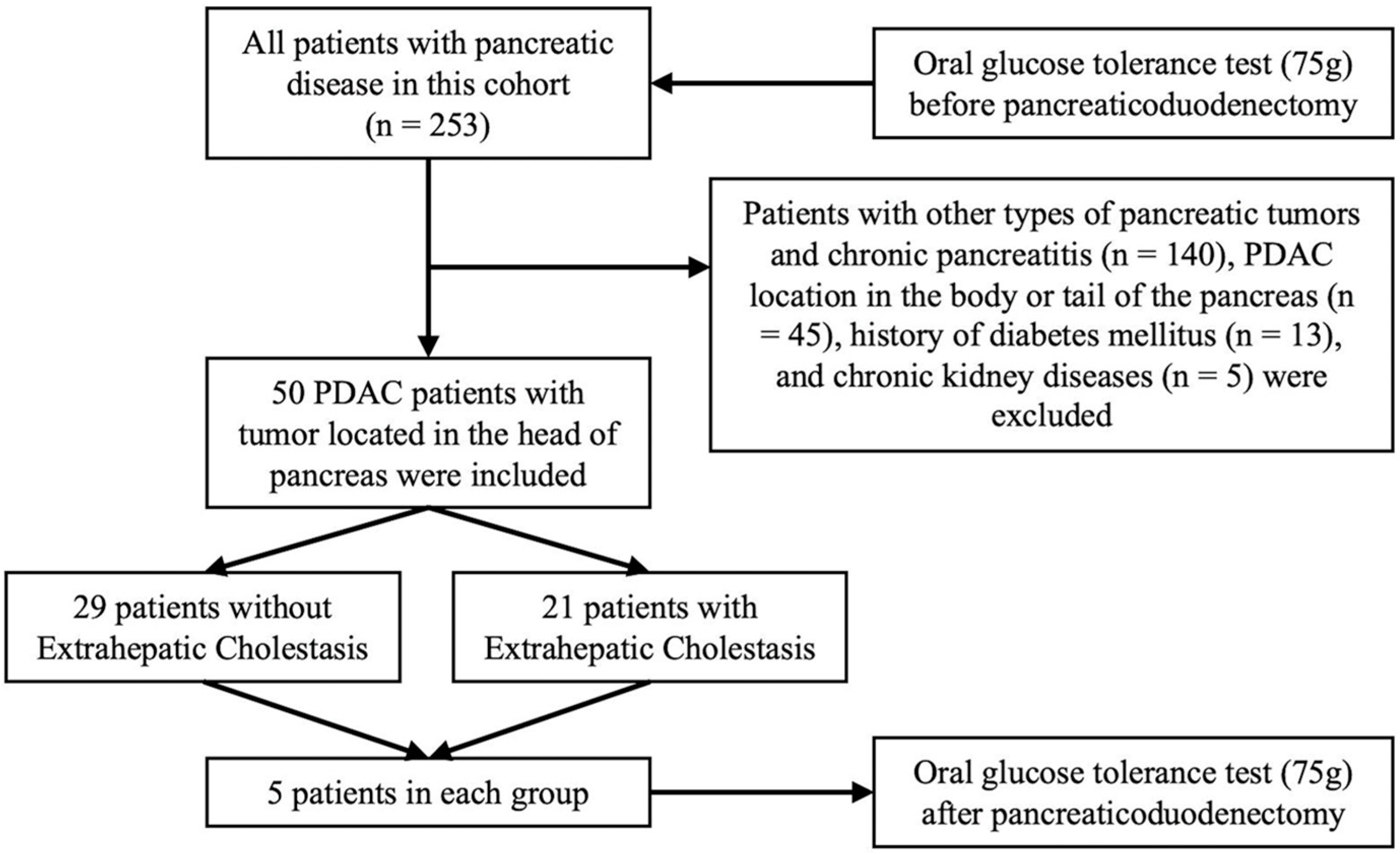
2.1. Study Design
2.2. Biochemical Parameters
2.3. Statistical Analysis
3. Results
3.1. Clinical and Metabolic Characteristics
3.2. Risk Factors for Impaired Glucose Homeostasis before PD
3.3. Glucose Metabolism Traits in Ductal Adenocarcinoma of Pancreatic Head Patients with Elevated Bile Acid
3.4. Alteration of Glycemic Traits after Bile Acid Metabolism Normalized
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hart, P.A.; Bellin, M.D.; Andersen, D.K.; Bradley, D.; Cruz-Monserrate, Z.; Forsmark, C.E.; Goodarzi, M.O.; Habtezion, A.; Korc, M.; Kudva, Y.C.; et al. Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol. Hepatol. 2016, 1, 226–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sah, R.P.; Nagpal, S.J.; Mukhopadhyay, D.; Chari, S.T. New insights into pancreatic cancer-induced paraneoplastic diabetes. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niwano, F.; Babaya, N.; Hiromine, Y.; Matsumoto, I.; Kamei, K.; Noso, S.; Taketomo, Y.; Takeyama, Y.; Kawabata, Y.; Ikegami, H. Glucose Metabolism After Pancreatectomy: Opposite Extremes Between Pancreaticoduodenectomy and Distal Pancreatectomy. J. Clin. Endocrinol. Metab. 2021, 106, e2203–e2214. [Google Scholar] [CrossRef]
- Ishida, J.; Toyama, H.; Matsumoto, I.; Shirakawa, S.; Terai, S.; Yamashita, H.; Yanagimoto, H.; Asari, S.; Kido, M.; Fukumoto, T. Glucose Tolerance after Pancreatectomy: A Prospective Observational Follow-Up Study of Pancreaticoduodenectomy and Distal Pancreatectomy. J. Am. Coll. Surg. 2021, 233, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Jung, H.S.; Jang, J.Y.; Jung, W.; Chang, J.; Shin, Y.C.; Kim, S.W. Metabolic effect of pancreatoduodenectomy: Resolution of diabetes mellitus after surgery. Pancreatology 2016, 16, 272–277. [Google Scholar] [CrossRef]
- Wu, J.M.; Kuo, T.C.; Yang, C.Y.; Chiang, P.Y.; Jeng, Y.M.; Huang, P.H.; Tien, Y.W. Resolution of diabetes after pancreaticoduodenectomy in patients with and without pancreatic ductal cell adenocarcinoma. Ann. Surg. Oncol. 2013, 20, 242–249. [Google Scholar] [CrossRef]
- Ohtsuka, T.; Kitahara, K.; Kohya, N.; Miyoshi, A.; Miyazaki, K. Improvement of glucose metabolism after a pancreatoduodenectomy. Pancreas 2009, 38, 700–705. [Google Scholar] [CrossRef]
- Permert, J.; Ihse, I.; Jorfeldt, L.; von Schenck, H.; Arnquist, H.J.; Larsson, J. Improved glucose metabolism after subtotal pancreatectomy for pancreatic cancer. Br. J. Surg. 1993, 80, 1047–1050. [Google Scholar] [CrossRef]
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef]
- Mezza, T.; Moffa, S.; Ferraro, P.M.; Quero, G.; Capece, U.; Carfì, A.; Cefalo, C.M.A.; Cinti, F.; Sorice, G.P.; Impronta, F.; et al. Bile Modulates Secretion of Incretins and Insulin: A Study of Human Extrahepatic Cholestasis. J. Clin. Endocrinol. Metab. 2019, 104, 2685–2694. [Google Scholar] [CrossRef]
- Martineau, M.G.; Raker, C.; Dixon, P.H.; Chambers, J.; Machirori, M.; King, N.M.; Hooks, M.L.; Manoharan, R.; Chen, K.; Powrie, R.; et al. The metabolic profile of intrahepatic cholestasis of pregnancy is associated with impaired glucose tolerance, dyslipidemia, and increased fetal growth. Diabetes Care 2015, 38, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Wikström Shemer, E.; Marschall, H.U.; Ludvigsson, J.F.; Stephansson, O. Intrahepatic cholestasis of pregnancy and associated adverse pregnancy and fetal outcomes: A 12-year population-based cohort study. Bjog 2013, 120, 717–723. [Google Scholar] [CrossRef]
- Shapiro, H.; Kolodziejczyk, A.A.; Halstuch, D.; Elinav, E. Bile acids in glucose metabolism in health and disease. J. Exp. Med. 2018, 215, 383–396. [Google Scholar] [CrossRef]
- Vítek, L.; Tiribelli, C. Bilirubin: The yellow hormone? J. Hepatol. 2021, 75, 1485–1490. [Google Scholar] [CrossRef]
- Bechmann, L.P.; Hannivoort, R.A.; Gerken, G.; Hotamisligil, G.S.; Trauner, M.; Canbay, A. The interaction of hepatic lipid and glucose metabolism in liver diseases. J. Hepatol. 2012, 56, 952–964. [Google Scholar] [CrossRef] [Green Version]
- Liao, X.; Zhang, D. The 8th Edition American Joint Committee on Cancer Staging for Hepato-pancreato-biliary Cancer: A Review and Update. Arch. Pathol. Lab. Med. 2021, 145, 543–553. [Google Scholar] [CrossRef] [Green Version]
- The American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- Defronzo, R.A.; Tripathy, D.; Schwenke, D.C.; Banerji, M.; Bray, G.A.; Buchanan, T.A.; Clement, S.C.; Henry, R.R.; Kitabchi, A.E.; Mudaliar, S.; et al. Prediction of diabetes based on baseline metabolic characteristics in individuals at high risk. Diabetes Care 2013, 36, 3607–3612. [Google Scholar] [CrossRef] [Green Version]
- Matsubayashi, Y.; Yoshida, A.; Suganami, H.; Ishiguro, H.; Yamamoto, M.; Fujihara, K.; Kodama, S.; Tanaka, S.; Kaku, K.; Sone, H. Role of fatty liver in the association between obesity and reduced hepatic insulin clearance. Diabetes Metab. 2018, 44, 135–142. [Google Scholar] [CrossRef]
- Kong, M.; Lu, Z.; Zhong, C.; Gao, Q.; Zhou, X.; Chen, R.; Xiong, G.; Hao, L.; Yang, X.; Yang, N. A higher level of total bile acid in early mid-pregnancy is associated with an increased risk of gestational diabetes mellitus: A prospective cohort study in Wuhan, China. J. Endocrinol. Investig. 2020, 43, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Chávez-Talavera, O.; Tailleux, A.; Lefebvre, P.; Staels, B. Bile Acid Control of Metabolism and Inflammation in Obesity, Type 2 Diabetes, Dyslipidemia, and Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 1679–1694.e1673. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Xu, B.; Zhang, X.; Cui, Y.; Deng, L.; Shi, Z.; Shao, Y.; Ding, M. Association between serum bile acid profiles and gestational diabetes mellitus: A targeted metabolomics study. Clin. Chim. Acta 2016, 459, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huo, X.; Cao, Y.F.; Li, S.N.; Du, Z.; Shao, P.; Leng, J.; Zhang, C.; Sun, X.Y.; Ma, R.C.W.; et al. Bile acid metabolites in early pregnancy and risk of gestational diabetes in Chinese women: A nested case-control study. EBioMedicine 2018, 35, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Li, J.; Leng, J.; Li, W.; Liu, J.; Yan, X.; Yu, Z.; Hu, G.; Ma, R.C.W.; Fang, Z.; et al. The CDKAL1 rs7747752-Bile Acids Interaction Increased Risk of Gestational Diabetes Mellitus: A Nested Case-Control Study. Front. Endocrinol. 2022, 13, 808956. [Google Scholar] [CrossRef]
- Bergman, R.N.; Piccinini, F.; Kabir, M.; Kolka, C.M.; Ader, M. Hypothesis: Role of Reduced Hepatic Insulin Clearance in the Pathogenesis of Type 2 Diabetes. Diabetes 2019, 68, 1709–1716. [Google Scholar] [CrossRef]
- Duckworth, W.C.; Bennett, R.G.; Hamel, F.G. Insulin degradation: Progress and potential. Endocr. Rev. 1998, 19, 608–624. [Google Scholar] [CrossRef] [Green Version]
- Vettorazzi, J.F.; Kurauti, M.A.; Soares, G.M.; Borck, P.C.; Ferreira, S.M.; Branco, R.C.S.; Michelone, L.S.L.; Boschero, A.C.; Junior, J.M.C.; Carneiro, E.M. Bile acid TUDCA improves insulin clearance by increasing the expression of insulin-degrading enzyme in the liver of obese mice. Sci. Rep. 2017, 7, 14876. [Google Scholar] [CrossRef] [Green Version]
- Bronczek, G.A.; Vettorazzi, J.F.; Soares, G.M.; Kurauti, M.A.; Santos, C.; Bonfim, M.F.; Carneiro, E.M.; Balbo, S.L.; Boschero, A.C.; Costa Júnior, J.M. The Bile Acid TUDCA Improves Beta-Cell Mass and Reduces Insulin Degradation in Mice With Early-Stage of Type-1 Diabetes. Front. Physiol. 2019, 10, 561. [Google Scholar] [CrossRef]
- Rajani, C.; Jia, W. Bile acids and their effects on diabetes. Front. Med. 2018, 12, 608–623. [Google Scholar] [CrossRef]
- Sharma, A.; Smyrk, T.C.; Levy, M.J.; Topazian, M.A.; Chari, S.T. Fasting Blood Glucose Levels Provide Estimate of Duration and Progression of Pancreatic Cancer Before Diagnosis. Gastroenterology 2018, 155, 490–500.e492. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Thompson, M.L.; Filipp, S.L.; Grajo, J.R.; Nambam, B.; Beegle, R.; Middlebrooks, E.H.; Gurka, M.J.; Atkinson, M.A.; Schatz, D.A.; Haller, M.J. Relative Pancreas Volume Is Reduced in First-Degree Relatives of Patients With Type 1 Diabetes. Diabetes Care 2019, 42, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virostko, J.; Williams, J.; Hilmes, M.; Bowman, C.; Wright, J.J.; Du, L.; Kang, H.; Russell, W.E.; Powers, A.C.; Moore, D.J. Pancreas Volume Declines During the First Year After Diagnosis of Type 1 Diabetes and Exhibits Altered Diffusion at Disease Onset. Diabetes Care 2019, 42, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.; Sorokin, E.P.; Thomas, E.L.; Sattar, N.; Cule, M.; Bell, J.D.; Yaghootkar, H. Estimating the Effect of Liver and Pancreas Volume and Fat Content on Risk of Diabetes: A Mendelian Randomization Study. Diabetes Care 2022, 45, 460–468. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Extrahepatic Cholestasis n = 21 | No-Extrahepatic Cholestasis n = 29 | p Value |
|---|---|---|---|
| Sex (Male) | 18 (85.7) | 18 (62.1) | 0.110 |
| Age (years) | 62.9 ± 10.5 | 59.8 ± 11.6 | 0.340 |
| BMI (kg/m2) | 21.9 ± 2.1 | 22.3 ± 2.8 | 0.625 |
| Dilation of MPD | 16 (76.2) | 22 (75.9) | >0.999 |
| Tumor diameter | 3.3 ± 1.1 | 2.9 ± 1.0 | 0.206 |
| Tumor stage | 0.551 | ||
| I–II | 12 (57.1) | 20 (69.0) | |
| III–IV | 9 (42.9) | 9 (31.0) | |
| Total bilirubin (μmol/L) | 174.4 ± 140.3 | 12.2 ± 6.1 | <0.001 |
| Conjugated bilirubin (μmol/L) | 150.5 ± 120.6 | 5.2 ± 3.7 | <0.001 |
| Unconjugated bilirubin (μmol/L) | 23.9 ± 22.0 | 7.0 ± 3.2 | 0.002 |
| Albumin (g/L) | 37.9 ± 5.9 | 43.8 ± 4.3 | <0.001 |
| ALT (IU/L) | 144.1 ± 158.3 | 24.3 ± 28.8 | <0.001 |
| ALP (IU/L) | 378.0 ± 190.8 | 90.9 ± 59.6 | <0.001 |
| GGT (IU/L) | 458.1 ± 500.8 | 41.23 ± 78.0 | 0.001 |
| Total bile acid (μmol/L) | 93.8 ± 93.0 | 5.1 ± 5.9 | <0.001 |
| Triglyceride (mmol/L) | 2.1 ± 1.2 | 1.3 ± 0.5 | 0.009 |
| Total cholesterol (mmol/L) | 4.4 ± 1.5 | 4.1 ± 0.8 | 0.401 |
| HDL (mmol/L) | 0.5 ± 0.4 | 1.2 ± 0.4 | <0.001 |
| LDL (mmol/L) | 1.9 ± 1.0 | 2.4 ± 0.7 | 0.033 |
| Urea (mmol/L) | 4.2 ± 1.5 | 4.3 ± 1.2 | 0.795 |
| Creatine (μmol/L) | 72.8 ± 17.4 | 68.1 ± 17.2 | 0.347 |
| Fasting glucose levels (mmol/L) | 7.0 ± 2.1 | 5.6 ± 0.9 | 0.007 |
| 2 h postprandial plasma glucose (mmol/L) | 12.7 ± 5.4 | 8.9 ± 2.8 | 0.008 |
| HbA1c (%) | 6.4 ± 1.4 | 5.9 ± 0.8 | 0.173 |
| Glucose tolerance status | 0.004 * | ||
| Normal glucose tolerance | 1 (4.8) | 12 (31.0) | |
| Prediabetes mellitus | 9 (42.8) | 9 (44.8) | |
| New-onset diabetes | 11 (52.4) | 8 (27.6) |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| p Value | OR (95% CI) | p Value | OR (95% CI) | |
| Sex | ||||
| Female | Reference | - | - | |
| Male | 0.796 | 1.20 (0.30–4.79) | - | - |
| Age (years) | ||||
| <69 | Reference | - | - | |
| ≥69 | 0.426 | 1.81 (0.42–7.74) | - | - |
| BMI (kg/m2) | ||||
| <23.9 | Reference | Reference | ||
| ≥23.9 | 0.098 | 0.32 (0.08–1.23) | 0.159 | 0.08 (0.08–1.50) |
| Dilation of MPD | ||||
| No | Reference | |||
| Yes | 0.928 | 0.93 (0.21–4.15) | ||
| Tumor diameter (cm) | 0.219 | 1.53 (0.78–2.99) | ||
| Tumor stage | ||||
| I–II | Reference | - | - | |
| III–IV | 0.266 | 2.27 (0.53–9.67) | - | - |
| Unconjugated bilirubin (μmol/L) | ||||
| <17.0 | Reference | |||
| ≥17.0 | >0.999 | - | ||
| Bile acid (μmol/L) | ||||
| <10.0 | Reference | Reference | ||
| ≥10.0 | 0.018 | 7.22 (1.34–37.25) | 0.024 | 6.85 (1.29–36.25) |
| Triglyceride (mmol/L) | ||||
| <1.88 | Reference | - | - | |
| ≥1.88 | 0.944 | 0.95 (0.24–3.76) | - | - |
| HDL (mmol/L) | ||||
| ≥0.9 | Reference | - | - | |
| <0.9 | 0.269 | 2.13 (0.56–8.16) | - | - |
| ALT (IU/L) | ||||
| <40 | Reference | - | - | |
| ≥40 | 0.118 | 3.16 (0.75–13.36) | - | - |
| Characteristics | Elevated Bile Acids n = 21 | Normal Bile Acids n = 29 | p Value |
|---|---|---|---|
| Glucose AUC0–180 min | 40.4 ± 14.3 | 29.9 ± 7.0 | 0.005 |
| Insulin AUC0–180 min | 68.1 ± 47.4 | 121.9 ± 78.3 | 0.007 |
| C-peptide AUC0–180 min | 4.72 ± 2.92 | 5.55 ± 2.57 | 0.298 |
| Matsuda index | 163.8 ± 98.9 | 147.1 ± 127.6 | 0.619 |
| Insulinogenic index | 3.3 ± 3.2 | 8.7 ± 8.9 | 0.005 |
| ISSI-2 | 4.4 ± 2.9 | 6.9 ± 3.5 | 0.010 |
| HIC | 16.7 ± 5.3 | 11.7 ± 3.0 | 0.001 |
| 3 h postprandial HIC | 10.6 ± 2.4 | 7.9 ± 3.1 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Tan, C.; Zheng, Z.; Wang, X.; Liu, X.; Chen, Y. Elevated Bile Acid Is Associated with Worsened Impaired Glucose Homeostasis in Pancreatic Ductal Adenocarcinoma Patients with Extrahepatic Cholestasis through Increased Hepatic Insulin Clearance. J. Clin. Med. 2023, 12, 2352. https://doi.org/10.3390/jcm12062352
Yang J, Tan C, Zheng Z, Wang X, Liu X, Chen Y. Elevated Bile Acid Is Associated with Worsened Impaired Glucose Homeostasis in Pancreatic Ductal Adenocarcinoma Patients with Extrahepatic Cholestasis through Increased Hepatic Insulin Clearance. Journal of Clinical Medicine. 2023; 12(6):2352. https://doi.org/10.3390/jcm12062352
Chicago/Turabian StyleYang, Jie, Chunlu Tan, Zhenjiang Zheng, Xing Wang, Xubao Liu, and Yonghua Chen. 2023. "Elevated Bile Acid Is Associated with Worsened Impaired Glucose Homeostasis in Pancreatic Ductal Adenocarcinoma Patients with Extrahepatic Cholestasis through Increased Hepatic Insulin Clearance" Journal of Clinical Medicine 12, no. 6: 2352. https://doi.org/10.3390/jcm12062352