

Noise-Induced Hearing Loss
Abstract
:1. Introduction
2. Epidemiology
3. Pathophysiology
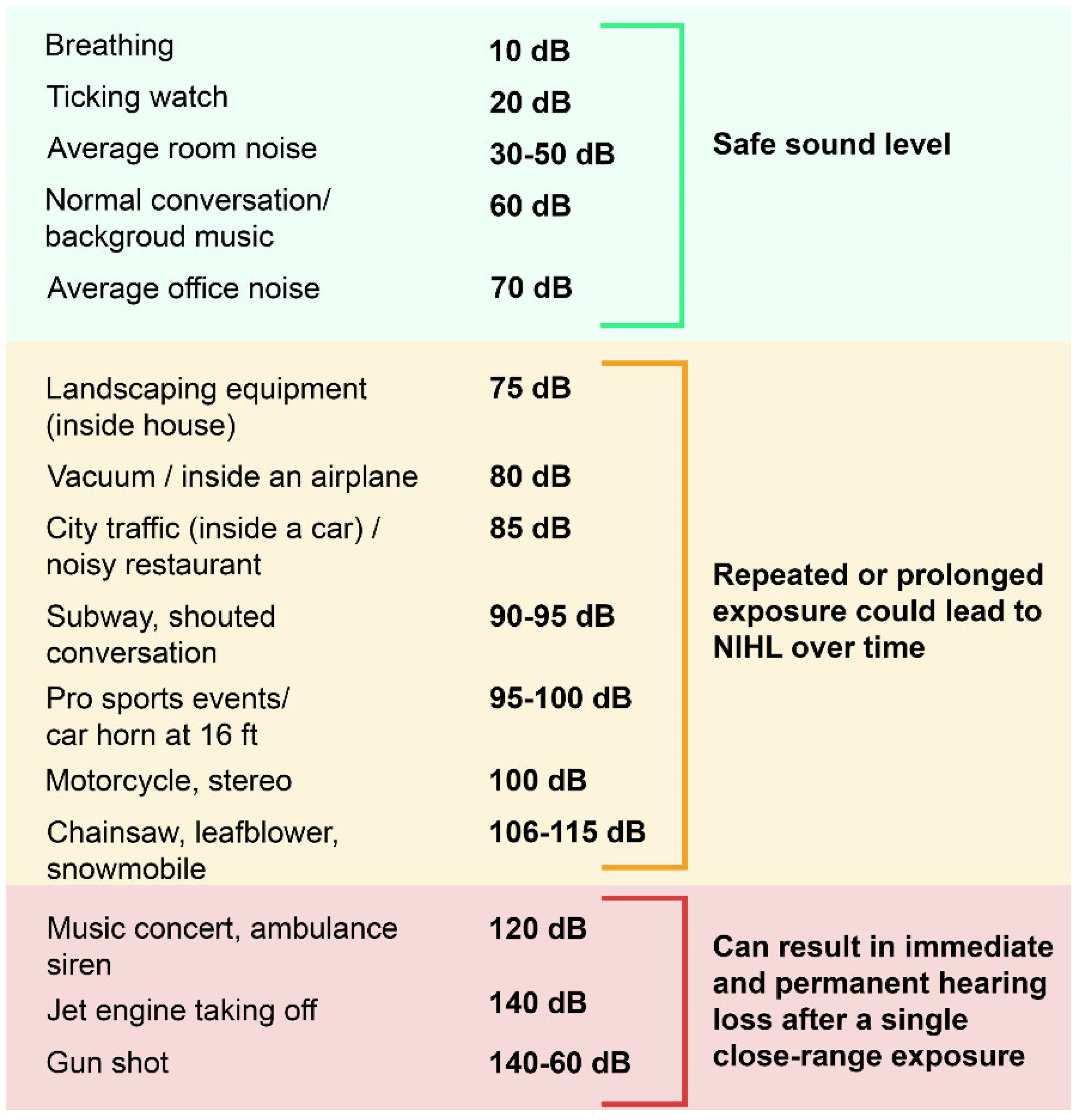
3.1. Harmful Noise Levels
3.2. Auditory Structures and Functions Impacted by Noise
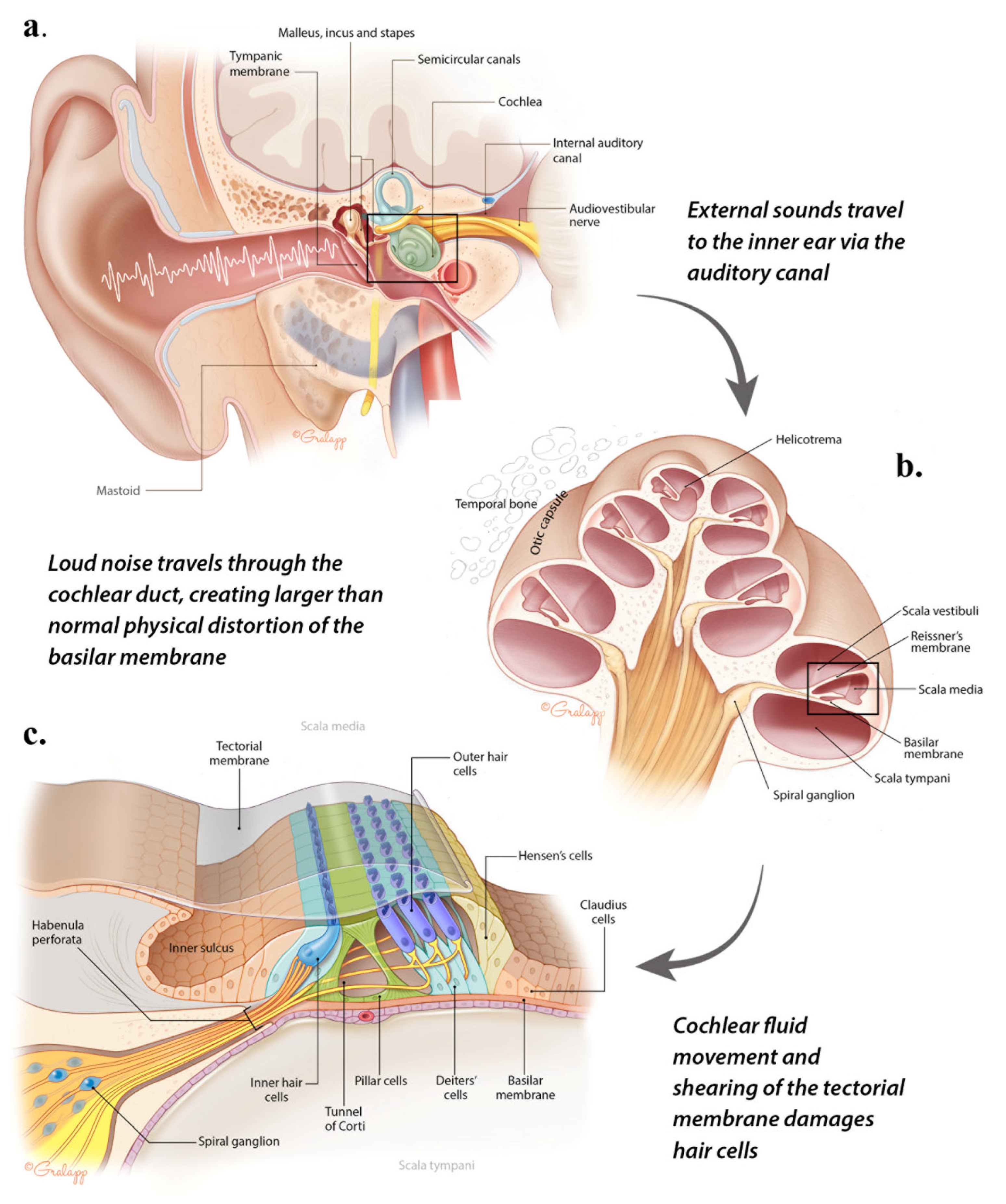
3.2.1. Sound Transmission from the Outer to the Middle and Inner Ear
3.2.2. Auditory Transduction in the Organ of Corti
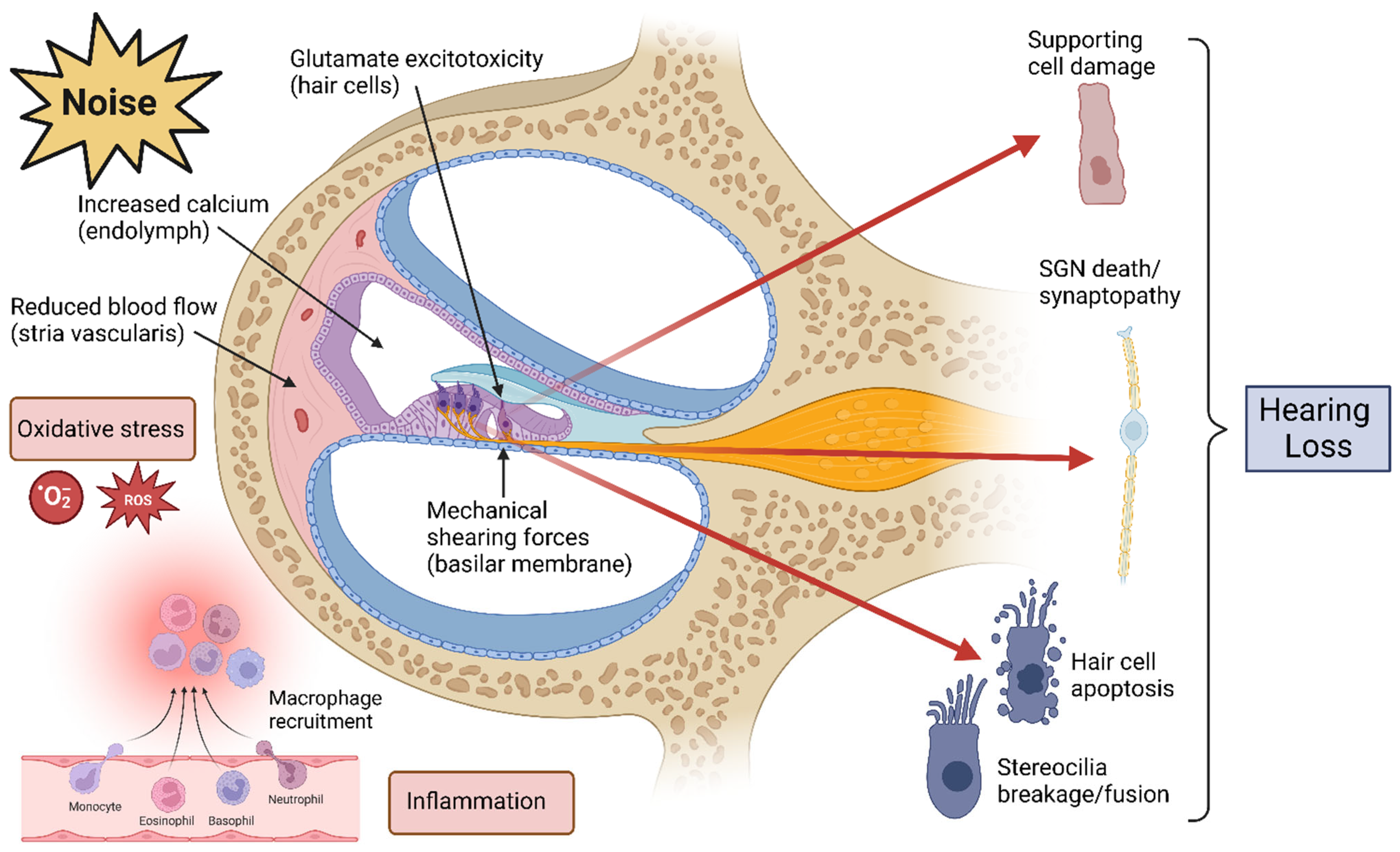
3.3. Mechanisms of Damage in NIHL
3.3.1. Mechanical Damage
3.3.2. Oxidative Stress and Reduced Blood Flow
3.3.3. Inflammation
3.3.4. Excitotoxicity and Synaptopathy
3.4. Additional Negative Effects of Noise on the Inner Ear
3.4.1. Tinnitus
3.4.2. Vestibular Dysfunction
4. Screening and Diagnosis of NIHL
4.1. Screening
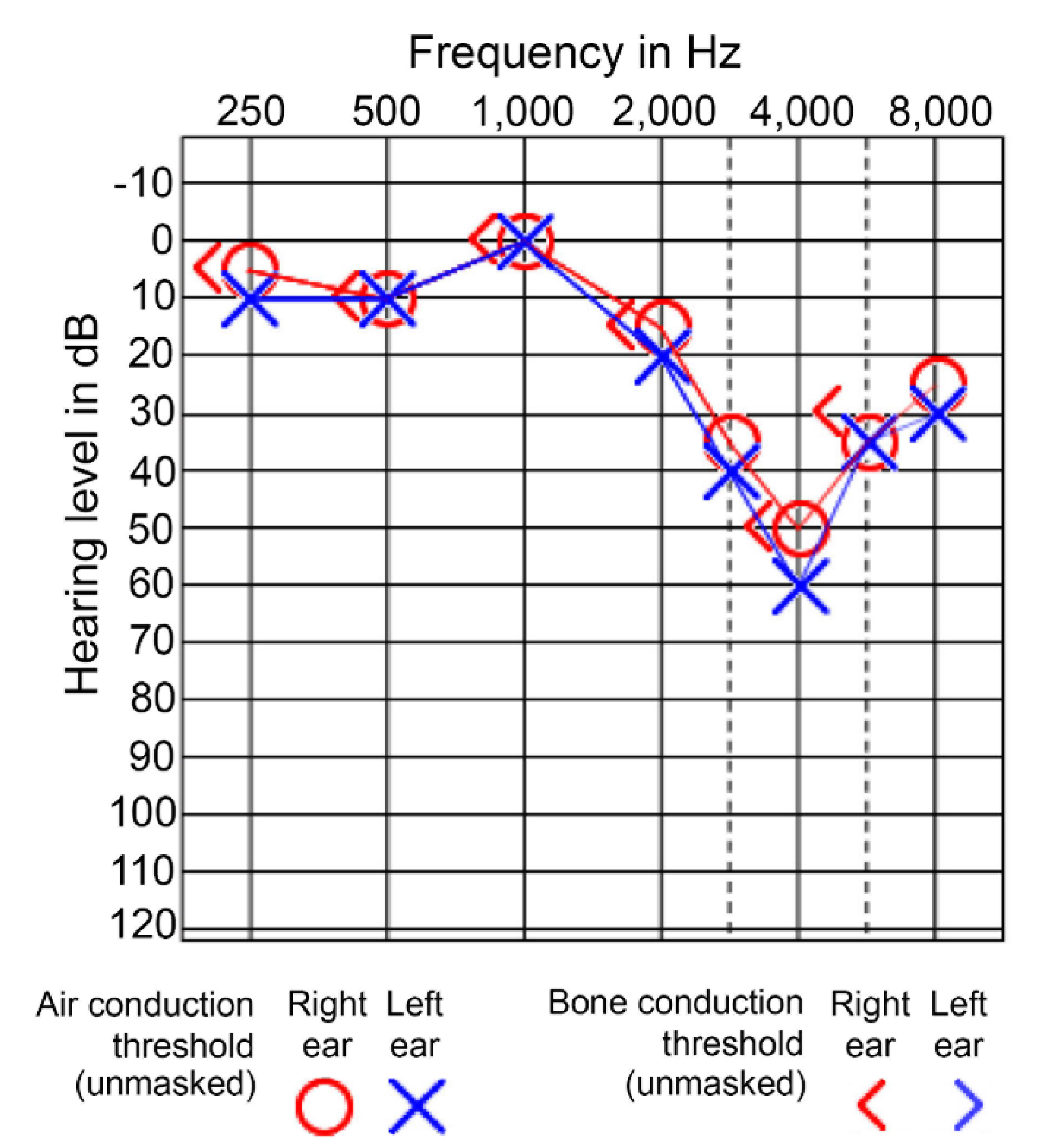
4.1.1. Audiograms
4.1.2. Speech-in-Noise Testing
4.1.3. Distortion Product Otoacoustic Emissions (DPOAE) Measurement
4.1.4. ABR Measurement
4.2. Diagnosis
5. Prevention and Management of NIHL
5.1. Prevention
5.2. Clinical Management
| Grade of impairment | Audiometric ISO value | Performance | Recommendation | Comments added to the prior classification |
| 0-None | ≥25 dB | No or very slight hearing problem. Can hear whispers. | None | 20 dB also recommended. People with 15–20 dB levels may have hearing problems. People with unilateral hearing loss may have problems even if the better ear is normal. |
| 1-Slight | 26–40 dB | Can hear and repeat words spoken in a normal voice at 1 m | Counseling. Hearing aids may be needed | Some difficulty in hearing but can usually hear normal level of conversation |
| 2-Moderate | 41–60 dB | Can hear and repeat words spoken in raised voice at 1 m | Hearing aids are usually recommended | None |
| 3-Severe | 61–80 dB | Can hear some words when shouted into better ear | Hearing aids needed. Otherwise lip-reading and signing should be taught | Discrepancies between pure-tone thresholds and speech discrimination score should be noted |
| 4-Profound | ≥81 dB | Unable to hear and understand even a shouted voice | Hearing aids may help understanding words. Additional rehabilitation needed. Lip-reading and sometimes signing are essential. | Speech is distorted, the degree depending on the age at which hearing was lost |
6. Risk Factors
- Older age, although all ages are at risk
- Repeated occupational noise exposure (construction, machine shop/factory, landscaping, mining, agriculture, musician, etc.)
- Repeated recreational noise exposure (loud music at concerts, loud volume via earphones/earbuds)
- Intense blast or explosion exposure
- Shooting firearms (recreational or military)
- Hypertension, smoking
- Lack of hearing protection
- Exposure to organic solvents, heavy metals, pesticides, asphyxiants
6.1. Occupational
6.2. Military
6.3. Environmental and Recreational
6.4. Genetic
7. Emerging Therapies
7.1. Completed and Ongoing Clinical Trials
7.2. Antioxidant Therapy
7.3. Anti-Inflammatory Therapy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ClinicalTrial.gov ID/Name | Intervention | Study Design | Population, N | Active Arm, N | Comparator Arm, N | Primary Outcome | Secondary Outcomes | Results | Publication | Sponsor |
|---|---|---|---|---|---|---|---|---|---|---|
| NCT02903355: Phase 3 Clinical Trial: D-methionine to Reduce Noise-Induced Hearing Loss (NIHL) | D-methionine to prevent NIHL or tinnitus in a military population | Phase 3 RCT | US drill sergeant instructor trainees (21–45 y) receiving weapons training, N = 266 | 18 days of oral D-methionine, n = 124 | Placebo, n = 142 | ASHA shift from baseline to day 29–36 post-drug (day 15–22 post-noise exposure) | Change in DOEHRS-HC, EWS STS, THI | D- methionine was not superior to placebo on any outcome in the interim analysis | None | Metamor, Inc., USA [discontinued development] |
| NCT00808470: Micronutrients to Prevent Noise-induced Hearing Loss | Micronutrients to reduce magnitude of TTS from 4 h of loud music in young adults | Phase 2 RCT | Adults (18–35 y) with normal hearing, N = 70 | 4 days of oral beta carotene, vitamins C and E, magnesium, n = 35 | Placebo, n = 35 | Mean threshold shift at 4 kHz in both ears 15 min post-music vs. baseline | Threshold shift at 0.25, 0.5, 1, 2, 3, 6, and 8 kHz post-music; change in DPOAE amplitude, PMTF thresholds, and tinnitus measures | Micronutrients were not superior to placebo on any outcome in the final analysis | LePrell et al., 2016 [291] | University of Michigan, USA |
| NCT00552786: Antioxidation Medication for Noise-induced Hearing Loss | NAC to prevent TTS in workers exposed to noise in Taiwan | Randomized Phase 2 crossover | Males (25–65 y) with known work noise exposure, N = 53 | 14 days of 1200 mg NAC | Glucose capsule | Threshold shift from baseline measured with PTA, four time-spaced assessments | Threshold shift from baseline measured with DPOAE, four time-spaced assessments | NAC significantly reduced TTS among men without any GSTIM1 or GSTT1 polymorphisms | Lin et al. (2010) [300] | National Taiwan University Hospital, Taiwan |
| NCT02951715: Improvement of Tinnitus After Oral Zinc on Patients With Noise-induced Hearing Loss | Zine to improve NIHL and tinnitus symptoms | Open label, single arm | Adults with confirmed NIHL-related tinnitus, N = 20 | 2 months of 40 mg oral zinc daily | None | THI change from baseline | Threshold shift, speech discrimination, DPOAE, tinnitus pitch/loudness from baseline | Zinc did not significantly improve hearing threshold but did improve THI score from baseline | Yeh et al. (2019) [296] | Chang Gung Memorial Hospital, China |
| NCT01444846: Otoprotection With SPI-1005 for Prevention of Temporary Auditory Threshold Shift | Ebselen to prevent TTS | Phase 2 RCT | Adults (18–31 y) with normal hearing, N = 83 | 4 days of oral 200, 400, or 600 mg ebselen, total n = 63 | Placebo capsule, n = 20 | Reduction in TTS from baseline (15 min post-sound exposure) at 4 kHz | N/A | Significant reduction in TTS at 4 kHz in 400 mg ebselen vs. placebo groups | Kil et al. (2017) [309] | Sound Pharmaceuticals, Inc., USA |
| Study Nation | Author, Year | Intervention | Study Design | Population, N | Active Arm, N | Comparator arm, N | Primary Outcome | Results |
|---|---|---|---|---|---|---|---|---|
| Following AAT (attenuation) | ||||||||
| Greece | Psillas et al. (2008) [310] | Prednisone and piracetam | Randomized cohort study | Male soldiers with firearms-related AAT, N = 52 | Therapy in <1 h, n = 20 | Therapy in >1–<16 h, n = 17 Therapy in 24+ h, n = 15 | Complete or partial recovery in 1 month | Significantly higher recovery rate (65%) and better final threshold shifts if treatment at <1 h vs. with delayed treatment (13–24% recovery) |
| Belgium | Lafère et al. (2010) [318] | HBOT with or without methyl-prednisolone and piracetam (medical therapy) | Cohort study | Belgian soldiers with firearms-related AAT, N = 68 | HBOT + oral medical therapy, n = 17 HBOT + IV then oral medical therapy, n = 32 | 10 days oral medical therapy, N = 17 | Average hearing gain and average residual hearing loss 10 days post-treatment vs. baseline pre-AAT | Both regimens of HBOT + medical therapy was superior to medical therapy alone |
| China | Zhou et al. (2013) [219] | Intratympanic steroid (methyl-prednisolone) with or without oral steroid | Prospective RCT | Adults recently diagnosed with NIHL, N = 52 | Intratympanic + oral steroid 3 days after NIHL onset, n = 27 | Intratympanic placebo + oral steroid 3 days after NIHL onset, n = 26 | PTA and speech discrimination score change from baseline | Significantly more of the intratympanic group had ≥15 dB improvement in PTA and ≥15% speech discrimination vs. placebo + oral steroid only |
| Before noise exposure (prophylaxis) | ||||||||
| Israel | Attias et al, (2004) [293] | Mg | Prospective RCT | Males (16–37 y) with normal hearing, N = 20 | 10 days 122 mg oral Mg, n = 10 | Placebo, n = 10 | TTS immediately following noise exposure (90 dB for 10 min) | 12% of Mg-treated patients experienced TTS ≥ 20 dB, vs. 28% in placebo and no-intake groups; reduced magnitude of TTS was significant for all frequencies between 2 and 8 kHz |
| Israel | Attias et al, (1994) [292] | Mg | Prospective RCT | Male military recruits exposed to noise during 8 weeks of weapons training, N = 255 | 167 mg oral Mg twice daily during training, n = 125 | Placebo, n = 130 | PTS 7–10 days post-exposure vs. baseline | PTS was significantly more common and more severe in the placebo vs. Mg-treated group, and negatively correlated with red blood cell Mg level |
| Italy | Quaranta et al. (2004) [294] | Vitamin B12 | Prospective RCT | Adults (20–30 y) with normal hearing, N = 20 | 1 mg B12 daily for 7 days, then 5 mg on day 8, n = 10 | Placebo, n = 10 | TTS following 112 dB 3 kHz noise for 10 min measured 8 days post-treatment | Significant reduction in TTS at 3 at 4 kHz in B12 group vs. control |
| India | Kapoor et al. (2011) [295] | Vitamin E + inhaled carbogen (5% CO2 +95% oxygen) | Prospective RCT | Male industrial workers with exposure to intense occupational noise, N = 40 | 6 days carbogen, vitamin E only, or combination, total n = 30 (10 each) | Placebo, n = 10 | TTS from baseline following 5 h noise exposure (90–113.5 dB) | Combined carbogen + vitamin E reduced TTS by 1.6–5.1 dB across frequencies; vitamin E groups had reduced serum markers of oxidative stress |
8. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acton, W.I. History and development of hearing protection devices. J. Acoust. Soc. Am. 1987, 81, S4. [Google Scholar] [CrossRef]
- Thurston, F.E. The worker’s ear: A history of noise-induced hearing loss. Am. J. Ind. Med. 2013, 56, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Institute for Quality and Efficiency in Health Care (IQWiG). Hearing Loss and Deafness: Normal Hearing and Impaired Hearing. Available online: https://www.ncbi.nlm.nih.gov/books/NBK390300/ (accessed on 25 January 2023).
- Münzel, T.; Gori, T.; Babisch, W.; Basner, M. Cardiovascular effects of environmental noise exposure. Eur. Heart J. 2014, 35, 829–836. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Deafness and Hearing Loss. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 10 January 2022).
- Liberman, M.C. Noise-induced hearing loss: Permanent versus temporary threshold shifts and the effects of hair cell versus neuronal degeneration. Adv. Exp. Med. Biol. 2016, 875, 1–7. [Google Scholar] [PubMed]
- Mazurek, B.; Olze, H.; Haupt, H.; Szczepek, A.J. The more the worse: The grade of noise-induced hearing loss associates with the severity of tinnitus. Int. J. Environ. Res. Public. Health 2010, 7, 3071–3079. [Google Scholar] [CrossRef]
- GBD 2019 Hearing Loss Collaborators. Hearing loss prevalence and years lived with disability, 1990–2019: Findings from the Global Burden of Disease Study 2019. Lancet 2021, 397, 996–1009. [Google Scholar] [CrossRef]
- Rabinowitz, P.M. Noise-induced hearing loss. Am. Fam. Physician 2000, 61, 2749–2756, 2759–2760. [Google Scholar]
- Goines, L.; Hagler, L. Noise pollution: A modem plague. South. Med. J. 2007, 100, 287–294. [Google Scholar] [CrossRef]
- Oishi, N.; Schacht, J. Emerging treatments for noise-induced hearing loss. Expert. Opin. Emerg. Drugs 2011, 16, 235–245. [Google Scholar] [CrossRef]
- Daniel, E. Noise and hearing loss: A review. J. Sch. Health 2007, 77, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Schwela, D. Environmental noise challenges and policies in low- and middle- income countries. SFJH 2021, 2, 26–45. [Google Scholar] [CrossRef]
- Kalisa, E.; Irankunda, E.; Rugengamanzi, E.; Amani, M. Noise levels associated with urban land use types in Kigali, Rwanda. Heliyon 2022, 8, e10653. [Google Scholar] [CrossRef] [PubMed]
- King, E.A. Here, there, and everywhere: How the SDGs must include noise pollution in their development challenges. Environ. Sci. Policy 2022, 64, 17–32. [Google Scholar] [CrossRef]
- Nelson, D.I.; Nelson, R.Y.; Concha-Barrientos, M.; Fingerhut, M. The global burden of occupational noise-induced hearing loss. Am. J. Indust Med. 2005, 48, 446–458. [Google Scholar] [CrossRef] [PubMed]
- Nandi, S.S.; Dhatrak, S.V. Occupational noise-induced hearing loss in India. Indian. J. Occup. Environ. Med. 2008, 12, 53–56. [Google Scholar] [CrossRef]
- Khoza-Shangase, K.; Moroe, N.F.; Edwards, A. Occupational hearing loss in Africa: An interdisciplinary view of the current status. S. Afr. J. Commun. Disord. 2020, 67, e1–e3. [Google Scholar] [CrossRef]
- Nyarubeli, I.P.; Tungu, A.M.; Moen, B.E.; Bråtveit, M. Prevalence of noise-induced hearing loss among Tanzanian iron and steel workers: A cross-sectional study. Int. J. Environ. Res. Public. Health 2019, 16, 1367. [Google Scholar] [CrossRef]
- US Centers for Disease Control and Prevention. Noise-induced Hearing Loss. Available online: https://www.nidcd.nih.gov/health/noise-induced-hearing-loss (accessed on 28 November 2022).
- Carroll, Y.I.; Eichwald, J.; Scinicariello, F.; Hoffman, H.J.; Deitchman, S.; Radke, M.S.; Themann, C.L.; Breysse, P. Vital signs: Noise-induced hearing loss among adults—United States 2011–2012. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 139–144. [Google Scholar] [CrossRef]
- Henderson, E.; Testa, M.A.; Hartnick, C. Prevalence of noise-induced hearing-threshold shifts and hearing loss among US youths. Pediatrics 2011, 127, e39–e46. [Google Scholar] [CrossRef]
- Shield, B.; Hearing Loss: Numbers and Costs. Evaluation of the Social and Economic Costs of Hearing Impairment. A Report for Hear-It AISBL. Available online: https://www.hear-it.org/sites/default/files/2021-01/Hear-it%20Report%20Hearing%20Loss%20Numbers%20and%20Costs%202019.pdf (accessed on 28 November 2022).
- Pawlaczyk-Luszczynska, M.; Dudarewicz, A.; Zaborowski, K.; Zamojska, M.; Sliwinska-Kowalska, M. Noise induced hearing loss: Research in Central, Eastern and South-Eastern Europe and newly independent states. Noise Health 2013, 15, 55–66. [Google Scholar] [CrossRef]
- Palmer, K.T.; Griffin, M.J.; Syddall, H.E.; Davis, A.; Pannett, B.; Coggon, D. Occupational exposure to noise and the attributable burden of hearing difficulties in Great Britain. Occup. Environ. Med. 2002, 59, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Health and Safety Executive. Noise Induced Hearing Loss in Great Britain. Available online: https://www.hse.gov.uk/statistics/causdis/deafness/index.htm (accessed on 28 November 2022).
- Purves, D.; Augustine, G.; Fitzpatrick, D. (Eds.) The Audible Spectrum. In Neuroscience, 2nd ed.; Sinauer Associates: Sunderland, MA, USA, 2001. [Google Scholar]
- Stewart, C.E.; Holt, A.G.; Altschuler, R.A.; Cacace, A.T.; Hall, C.D.; Murnane, O.D.; King, W.M.; Akin, F.W. Effects of noise exposure on the vestibular system: A systematic review. Front. Neurol. 2020, 11, 593919. [Google Scholar] [CrossRef]
- US Centers for Disease Control and Prevention. What Noises Cause Hearing Loss? Available online: https://www.cdc.gov/nceh/hearing_loss/what_noises_cause_hearing_loss.html (accessed on 11 January 2023).
- US National Institute for Occupational Safety and Health (NIOSH). Noise & Hearing Loss Prevention. Available online: https://www.cdc.gov/niosh/topics/noise/default.html (accessed on 28 November 2022).
- Hearing Health Foundation. Decibel Levels. Available online: https://hearinghealthfoundation.org/decibel-levels (accessed on 28 November 2022).
- Sinyor, A.; Laszlo, C.A. Acoustic behavior of the outer ear of the guinea pig and the influence of the middle ear. J. Acoust. Soc. Am. 1973, 54, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Luers, J.C.; Hüttenbrink, K.B. Surgical anatomy and pathology of the middle ear. J. Anat. 2016, 228, 338–353. [Google Scholar] [CrossRef]
- Kujawa, S.G.; Liberman, M.C. Adding insult to injury: Cochlear nerve degeneration after “temporary” noise-induced hearing loss. J. Neurosci. 2009, 29, 14077–14085. [Google Scholar] [CrossRef] [PubMed]
- Skrzat, J.; Kozerska, M.; Wroński, S.; Tarasiu, J.; Walocha, J. Volume rendering of the tympanic cavity from micro-CT data. Folia Med. Cracov. 2015, 55, 81–89. [Google Scholar] [PubMed]
- Zdilla, M.J.; Skrzat, J.; Kozerska, M.; Leszczyński, B.; Tarasiuk, J.; Wroński, S. Oval window size and shape: A micro-CT anatomical study with considerations for stapes surgery. Otol. Neurotol. 2018, 39, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Békésy, G.V. The sound pressure difference between the round and the oval windows and the artificial window of labyrinthine fenestration. Acta Otolaryngol. 1947, 35, 301–315. [Google Scholar] [CrossRef]
- Ryan, A.F.; Kujawa, S.G.; Hammill, T.; Le Prell, C.; Kil, J. Temporary and permanent noise-induced threshold shifts: A review of basic and clinical observations. Otol. Neurotol. 2016, 37, e271–e275. [Google Scholar] [CrossRef]
- Costanzo, L. Neurophysiology. In Physiology, 6th ed.; Costanzo, L., Ed.; Elsevier: Philadelphia, PA, USA, 2018. [Google Scholar]
- Raftery AT, J.S. Head and neck. In Applied Basic Science for Basic Surgical Training, 2nd ed.; Raftery, A., Ed.; Churchill Livingstone: Edinburgh, Scotland, 2008. [Google Scholar]
- Pujol, R.; Nouvian, R.; Lenoir, M.; Irving, S. Hair Cells: Overview. Available online: http://www.cochlea.eu/en/hair-cells (accessed on 28 November 2022).
- Zetes, D.E.; Tolomeo, J.A.; Holley, M.C. Structure and mechanics of supporting cells in the guinea pig organ of Corti. PLoS ONE 2012, 7, e49338. [Google Scholar] [CrossRef]
- Sakaguchi, H.; Tokita, J.; Müller, U.; Kachar, B. Tip links in hair cells: Molecular composition and role in hearing loss. Curr. Opin. Otolaryngol. Head. Neck Surg. 2009, 17, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Hakizimana, P.; Fridberger, A. Inner hair cell stereocilia are embedded in the tectorial membrane. Nat. Commun. 2021, 12, 2604. [Google Scholar] [CrossRef] [PubMed]
- Von Bekesy, G. Resting potentials inside the cochlear partition of the guinea pig. Nature 1952, 169, 241–242. [Google Scholar] [CrossRef]
- Kurbel, S.; Borzan, V.; Golem, H.; Dinjar, K. Cochlear potential difference between endolymph fluid and the hair cell’s interior: A retold interpretation based on the Goldman equation. Med. Glas. 2017, 14, 8–15. [Google Scholar]
- Liberman, M.C.; Gao, J.; He, D.Z.Z.; Wu, X.; Jia, S.; Zuo, J. Prestin is required for electromotility of the outer hair cell and for the cochlear amplifier. Nature 2002, 419, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Gale, J.E.; Ashmore, J.F. An intrinsic frequency limit to the cochlear amplifier. Nature 1997, 389, 63–66. [Google Scholar] [CrossRef]
- Khimich, D.; Nouvian, R.; Pujol, R.; Tom Dieck, S.; Egner, A.; Gundelfinger, E.D.; Moser, T. Hair cell synaptic ribbons are essential for synchronous auditory signalling. Nature 2005, 434, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, P.A.; Glowatzki, E.; Moser, T. The afferent synapse of cochlear hair cells. Curr. Opin. Neurobiol. 2003, 13, 452–458. [Google Scholar] [CrossRef]
- Sterling, P.; Matthews, G. Structure and function of ribbon synapses. Trends Neurosci. 2005, 28, 20–29. [Google Scholar] [CrossRef]
- Lagnado, L. Ribbon synapses. Curr. Biol. 2003, 13, R631. [Google Scholar] [CrossRef]
- Johnson, D.H. The relationship between spike rate and synchrony in responses of auditory-nerve fibers to single tones. J. Acoust. Soc. Am. 1980, 68, 1115–1122. [Google Scholar] [CrossRef]
- Furness, D.N. Molecular basis of hair cell loss. Cell Tissue Res. 2015, 361, 387–399. [Google Scholar] [CrossRef]
- Salvi, R.; Sun, W.; Ding, D.; Chen, G.-D.; Lobarinas, E.; Wang, J.; Radziwon, K.; Auerbach, B.D. Inner hair cell loss disrupts hearing and cochlear function leading to sensory deprivation and enhanced central auditory gain. Front. Neurosci. 2017, 10, 621. [Google Scholar] [CrossRef] [PubMed]
- Le, T.N.; Straatman, L.V.; Lea, J.; Westerberg, B. Current insights in noise-induced hearing loss: A literature review of the underlying mechanism, pathophysiology, asymmetry, and management options. J. Otolaryngol. Head Neck Surg. 2017, 46, 41. [Google Scholar] [CrossRef]
- Wu, P.Z.; O’Malley, J.T.; de Gruttola, V.; Liberman, M.C. Primary neural degeneration in noise-exposed human cochleas: Correlations with outer hair cell loss and word-discrimination scores. J. Neurosci. 2021, 41, 4439–4447. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.; Hammill, T.; Hoffer, M.; Kil, J.; Le Prell, C. Guidelines for auditory threshold measurement for significant threshold shift. Otol. Neurotol. 2016, 37, e263–e270. [Google Scholar] [CrossRef]
- Liberman, M.C.; Dodds, L.W. Single-neuron labeling and chronic cochlear pathology. III. Stereocilia damage and alterations of threshold tuning curves. Hear. Res. 1984, 16, 55–74. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, K.J.; Rodriguez, G.P.; Hepler, E.L.; Moul, M.L. Ear canal volume and variability in the patterns of temporary threshold shifts. Ear Hear. 1987, 8, 316–321. [Google Scholar] [CrossRef]
- Wagner, E.L.; Shin, J.B. Mechanisms of hair cell damage and repair. Trends Neurosci. 2019, 42, 414–424. [Google Scholar] [CrossRef]
- Kim, J.; Koo, M. Mass and stiffness impact on the middle ear and the cochlear partition. J. Audiol. Otol. 2015, 19, 1–6. [Google Scholar] [CrossRef]
- Robles, L.; Ruggero, M.A. Mechanics of the mammalian cochlea. Physiol. Rev. 2001, 81, 1305–1352. [Google Scholar] [CrossRef]
- Prosen, C.A.; Moody, D.B.; Stebbins, W.C.; Smith, D.W.; Sommers, M.S.; Brown, J.N.; Altschuler, R.A.; Hawkins, J.E. Apical hair cells and hearing. Hear. Res. 1990, 44, 179–193. [Google Scholar] [CrossRef]
- Assad, J.A.; Shepherd, G.M.; Corey, D.P. Tip-link integrity and mechanical transduction in vertebrate hair cells. Neuron 1991, 7, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.; Yang, S.; Guo, W.; He, D.Z. Fate of mammalian cochlear hair cells and stereocilia after loss of the stereocilia. J. Neurosci. 2009, 29, 15277–15285. [Google Scholar] [CrossRef] [PubMed]
- Indzhykulian, A.A.; Stepanyan, R.; Nelina, A.; Spinelli, K.J.; Ahmed, Z.M.; Belyantseva, I.A.; Friedman, T.B.; Barr-Gillespie, P.G.; Frolenkov, G.I. Molecular remodeling of tip links underlies mechanosensory regeneration in auditory hair cells. PLoS Biol. 2013, 11, e1001583. [Google Scholar] [CrossRef]
- Liberman, M.C. Chronic ultrastructural changes in acoustic trauma: Serial-section reconstruction of stereocilia and cuticular plates. Hear. Res. 1987, 26, 65–88. [Google Scholar] [CrossRef]
- Roberto, M.; Zito, F. Scar formation following impulse noise-induced mechanical damage to the organ of Corti. J. Laryngol. Otol. 1988, 102, 2–9. [Google Scholar] [CrossRef]
- Ou, H.C.; Bohne, B.A.; Harding, G.W. Noise damage in the C57BL/CBA mouse cochlea. Hear. Res. 2000, 145, 111–122. [Google Scholar] [CrossRef]
- Flock, A.; Flock, B.; Fridberger, A.; Scarfone, E.; Ulfendahl, M. Supporting cells contribute to control of hearing sensitivity. J. Neurosci. 1999, 19, 4498–4507. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, A.S.; Bohne, B.A.; Harding, G.W. Histopathological differences between temporary and permanent threshold shift. Hear. Res. 2000, 139, 13–30. [Google Scholar] [CrossRef]
- Fetoni, A.R.; Paciello, F.; Rolesi, R.; Paludetti, G.; Troiani, D. Targeting dysregulation of redox homeostasis in noise-induced hearing loss: Oxidative stress and ROS signaling. Free. Radic. Biol. Med. 2019, 135, 46–59. [Google Scholar] [CrossRef]
- Giorgio, M.; Migliaccio, E.; Orsini, F.; Paolucci, D.; Moroni, M.; Contursi, C.; Pelliccia, G.; Luzi, L.; Minucci, S.; Marcaccio, M.; et al. Electron transfer between cytochrome C and p66Shc generates reactive oxygen species that trigger mitochondrial apoptosis. Cell 2005, 122, 221–233. [Google Scholar] [CrossRef]
- Yamashita, D.; Minami, S.B.; Kanzaki, S.; Ogawa, K.; Miller, J.M. Bcl-2 genes regulate noise-induced hearing loss. J. Neurosci. Res. 2008, 86, 920–928. [Google Scholar] [CrossRef]
- Kurabi, A.; Keithley, E.M.; Housley, G.D.; Ryan, A.F.; Wong, A.C.Y. Cellular mechanisms of noise-induced hearing loss. Hear. Res. 2017, 349, 129–137. [Google Scholar] [CrossRef]
- Yamane, H.; Nakai, Y.; Konishi, K.; Sakamoto, H.; Matsuda, Y.; Iguchi, H. Strial circulation impairment due to acoustic trauma. Acta Otolaryngol. 1991, 111, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Yamane, H.; Nakai, Y.; Takayama, M.; Iguchi, H.; Nakagawa, T.; Kojima, A. Appearance of free radicals in the guinea pig inner ear after noise-induced acoustic trauma. Eur. Arch. Otorhinolaryngol. 1995, 252, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; White, M.A.; Cobb, M.H. Stimulus-specific requirements for MAP3 kinases in activating the JNK pathway. J. Biolog. Chem. 2002, 277, 49105–49110. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Hussain, A.; Ahsan, H. Peroxynitrite: Cellular pathology and implications in autoimmunity. J. Immunoass. Immunochem. 2019, 40, 123–138. [Google Scholar] [CrossRef]
- Yamashita, D.; Jiang, H.Y.; Schacht, J.; Miller, J.M. Delayed production of free radicals following noise exposure. Brain Res. 2004, 1019, 201–209. [Google Scholar] [CrossRef]
- Mruk, D.D.; Silvestrini, B.; Mo, M.-y.; Cheng, C.Y. Antioxidant superoxide dismutase—a review: Its function, regulation in the testis, and role in male fertility. Contraception 2002, 65, 305–311. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; McFadden, S.L.; Ding, D.L.; Flood, D.G.; Reaume, A.G.; Hoffman, E.K.; Scott, R.W.; Wright, J.S.; Putcha, G.V.; Salvi, R.J. Targeted deletion of the cytosolic Cu/Zn-superoxide dismutase gene (Sod1) increases susceptibility to noise-induced hearing loss. Audiol. Neurootol. 1999, 4, 237–246. [Google Scholar] [CrossRef]
- Castaldo, A.; Linthicum, F.H. Stria vascularis hearing loss. Otol. Neurotol. 2006, 27, 285–286. [Google Scholar] [CrossRef]
- Wangemann, P. K(+) cycling and its regulation in the cochlea and the vestibular labyrinth. Audiol. Neurootol. 2002, 7, 199–205. [Google Scholar] [CrossRef]
- Hirose, K.; Liberman, M.C. Lateral wall histopathology and endocochlear potential in the noise-damaged mouse cochlea. J. Assoc. Res. Otolaryngol. 2003, 4, 339–352. [Google Scholar] [CrossRef]
- Ide, M.; Morimitsu, T. Long term effects of intense sound on endocochlear DC potential. Auris Nasus Larynx 1990, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kuokkanen, J.; Aarnisalo, A.A.; Ylikoski, J. Efficiency of hyperbaric oxygen therapy in experimental acute acoustic trauma from firearms. Acta Otolaryngol. Suppl. 2000, 543, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Le Prell, C.G.; Yamashita, D.; Minami, S.B.; Yamasoba, T.; Miller, J.M. Mechanisms of noise-induced hearing loss indicate multiple methods of prevention. Hear Res. 2007, 226, 22–43. [Google Scholar] [CrossRef] [PubMed]
- Sha, S.-H.; Taylor, R.; Forge, A.; Schacht, J. Differential vulnerability of basal and apical hair cells is based on intrinsic susceptibility to free radicals. Hear Res. 2001, 155, 1–8. [Google Scholar] [CrossRef]
- Cevette, M.J.; Vormann, J.; Franz, K. Magnesium and hearing. J. Am. Acad. Audiol. 2003, 14, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Ising, H.; Handrock, M.; Günther, T.; Fischer, R.; Dombrowski, M. Increased noise trauma in guinea pigs through magnesium deficiency. Arch. Otorhinolaryngol. 1982, 236, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Nageris, B.I.; Ulanovski, D.; Attias, J. Magnesium treatment for sudden hearing loss. Ann. Otol. Rhinol. Laryngol. 2004, 113, 672–675. [Google Scholar] [CrossRef] [PubMed]
- White, R.E.; Hartzell, H.C. Effects of intracellular free magnesium on calcium current in isolated cardiac myocytes. Science 1988, 239, 778–780. [Google Scholar] [CrossRef]
- Schanne, F.A.; Kane, A.B.; Young, E.E.; Farber, J.L. Calcium dependence of toxic cell death: A final common pathway. Science 1979, 206, 700–702. [Google Scholar] [CrossRef]
- Houston, M. The role of magnesium in hypertension and cardiovascular disease. J. Clin. Hypertens. 2011, 13, 843–847. [Google Scholar] [CrossRef] [PubMed]
- Das, U.N. Essential fatty acids: Biochemistry, physiology and pathology. Biotechnol. J. 2006, 1, 420–439. [Google Scholar] [CrossRef] [PubMed]
- Das, U.N. Nutrients, essential fatty acids and prostaglandins interact to augment immune responses and prevent genetic damage and cancer. Nutrition 1989, 5, 106–110. [Google Scholar]
- Das, U.N. Delta6 desaturase as the target of the beneficial actions of magnesium. Med. Sci. Monit. 2010, 16, LE11–LE12. [Google Scholar]
- Satoh, H.; Firestein, G.S.; Billings, P.B.; Harris, J.P.; Keithley, E.M. Tumor necrosis factor-alpha, an initiator, and etanercept, an inhibitor of cochlear inflammation. Laryngoscope 2002, 112, 1627–1634. [Google Scholar] [CrossRef]
- Wakabayashi, K.; Fujioka, M.; Kanzaki, S.; Okano, H.J.; Shibata, S.; Yamashita, D.; Masuda, M.; Mihara, M.; Ohsugi, Y.; Ogawa, K.; et al. Blockade of interleukin-6 signaling suppressed cochlear inflammatory response and improved hearing impairment in noise-damaged mice cochlea. Neurosci. Res. 2010, 66, 345–352. [Google Scholar] [CrossRef]
- Seist, R.; Landegger, L.D.; Robertson, N.G.; Vasilijic, S.; Morton, C.C.; Stankovic, K.M. Cochlin deficiency protects against noise-induced hearing loss. Front. Mol. Neurosci. 2021, 14, 670013. [Google Scholar] [CrossRef]
- Landegger, L.D.; Vasilijic, S.; Fujita, T.; Soares, V.Y.; Seist, R.; Xu, L.; Stankovic, K.M. Cytokine levels in inner ear fluid of young and aged mice as molecular biomarkers of noise-induced hearing loss. Front. Neurol. 2019, 10, 977. [Google Scholar] [CrossRef]
- Ren, Y.; Stankovic, K.M. The role of tumor necrosis factor alpha (TNFα) in hearing loss and vestibular schwannomas. Curr. Otorhinolaryngol. Rep. 2018, 6, 15–23. [Google Scholar] [CrossRef]
- Hirose, K.; Discolo, C.M.; Keasler, J.R.; Ransohoff, R. Mononuclear phagocytes migrate into the murine cochlea after acoustic trauma. J. Comp. Neurol. 2005, 489, 180–194. [Google Scholar] [CrossRef]
- Yang, W.; Vethanayagam, R.R.; Dong, Y.; Cai, Q.; Hu, B.H. Activation of the antigen presentation function of mononuclear phagocyte populations associated with the basilar membrane of the cochlea after acoustic overstimulation. Neuroscience 2015, 303, 1–15. [Google Scholar] [CrossRef]
- Frye, M.D.; Zhang, C.; Hu, B.H. Lower level noise exposure that produces only TTS modulates the immune homeostasis of cochlear macrophages. J. Neuroimmunol. 2018, 323, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Hough, K.; Verschuur, C.A.; Cunningham, C.; Newman, T.A. Macrophages in the cochlea: An immunological link between risk factors and progressive hearing loss. Glia 2022, 70, 219–238. [Google Scholar] [CrossRef] [PubMed]
- Katsumi, S.; Sahin, M.I.; Lewis, R.M.; Iyer, J.S.; Landegger, L.D.; Stankovic, K.M. Intracochlear perfusion of tumor necrosis factor-alpha induces sensorineural hearing loss and synaptic degeneration in guinea pigs. Front. Neurol. 2020, 10, 1353. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, S.G.; Liberman, M.C. Synaptopathy in the noise-exposed and aging cochlea: Primary neural degeneration in acquired sensorineural hearing loss. Hear. Res. 2015, 330, 191–199. [Google Scholar] [CrossRef]
- Jensen, J.B.; Lysaght, A.C.; Liberman, M.C.; Qvortrup, K.; Stankovic, K.M. Immediate and delayed cochlear neuropathy after noise exposure in pubescent mice. PLoS ONE 2015, 10, e0125160. [Google Scholar] [CrossRef]
- Pujol, R.; Rebillard, G.; Puel, J.L.; Lenoir, M.; Eybalin, M.; Recasens, M. Glutamate neurotoxicity in the cochlea: A possible consequence of ischaemic or anoxic conditions occurring in ageing. Acta Otolaryngol. Suppl. 1990, 476, 32–36. [Google Scholar] [CrossRef]
- Kujawa, S.G.; Liberman, M.C. Acceleration of age-related hearing loss by early noise exposure: Evidence of a misspent youth. J. Neurosci. 2006, 26, 2115–2123. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, J.J. Effects of long-term non-traumatic noise exposure on the adult central auditory system. Hearing problems without hearing loss. Hear. Res. 2017, 352, 12–22. [Google Scholar] [CrossRef]
- Pienkowski, M.; Eggermont, J.J. Intermittent exposure with moderate-level sound impairs central auditory function of mature animals without concomitant hearing loss. Hear. Res. 2010, 261, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Takacs, J.D.; Forrest, T.J.; Basura, G.J. Noise exposure alters long-term neural firing rates and synchrony in primary auditory and rostral belt cortices following bimodal stimulation. Hear. Res. 2017, 356, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Seki, S.; Eggermont, J.J. Changes in spontaneous firing rate and neural synchrony in cat primary auditory cortex after localized tone-induced hearing loss. Hear Res 2003, 180, 28–38. [Google Scholar] [CrossRef]
- Agrawal, Y.; Platz, E.A.; Niparko, J.K. Prevalence of hearing loss and differences by demographic characteristics among US adults: Data from the National Health and Nutrition Examination Survey, 1999–2004. Arch. Intern. Med. 2008, 168, 1522–1530. [Google Scholar] [CrossRef]
- Shore, S.E.; Wu, C. Mechanisms of noise-induced tinnitus: Insights from cellular studies. Neuron 2019, 103, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Platz, E.A.; Niparko, J.K. Risk factors for hearing loss in US adults: Data from the National Health and Nutrition Examination Survey, 1999 to 2002. Otol. Neurotol. 2009, 30, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Moser, T.; Starr, A. Auditory neuropathy—Neural and synaptic mechanisms. Nat. Rev. Neurol. 2016, 12, 135–149. [Google Scholar] [CrossRef] [PubMed]
- Liberman, L.D.; Sukuzi, J.; Liberman, M.C. Dynamics of cochlear synaptopathy after acoustic overexposure. J. Assoc. Res. Otolaryngol. 2015, 16, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Liberman, M.C. Morphological differences among radial afferent fibers in the cat cochlea: An electron-microscopic study of serial sections. Hear. Res. 1980, 3, 45–63. [Google Scholar] [CrossRef]
- Liberman, M.C. Single-neuron labeling in the cat auditory nerve. Science 1982, 216, 1239–1241. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Liberman, L.D.; Maison, S.F.; Liberman, M.C. Olivocochlear innervation maintains the normal modiolar-pillar and habenular-cuticular gradients in cochlear synaptic morphology. J. Assoc. Res. Otolaryngol. 2014, 15, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Esmaili, A.A.; Renton, J. A review of tinnitus. Aust. J. Gen. Pract. 2018, 47, 205–208. [Google Scholar] [CrossRef]
- Shiomi, Y.; Tsuji, J.; Naito, Y.; Fujiki, N.; Yamamoto, N. Characteristics of DPOAE audiogram in tinnitus patients. Hear. Res. 1997, 108, 83–88. [Google Scholar] [CrossRef]
- Ceranic, B.J.; Prasher, D.K.; Raglan, E.; Luxon, L.M. Tinnitus after head injury: Evidence from otoacoustic emissions. J. Neurol. Neurosurg. Psychiatry 1998, 65, 523–529. [Google Scholar] [CrossRef]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef]
- Shulman, A.; Wang, W.; Luo, H.; Bao, S.; Searchfield, G.; Zhang, J. Neuroinflammation and tinnitus. Curr. Top. Behav. Neurosci. 2021, 51, 161–174. [Google Scholar]
- Jang, D.I.; Lee, A.H.; Shin, H.Y.; Song, H.R.; Park, J.H.; Kang, T.B.; Lee, S.R.; Yang, S.H. The role of tumor necrosis factor alpha (TNF-α) in autoimmune disease and current TNF-α inhibitors in therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef] [PubMed]
- Savastano, M. Tinnitus with or without hearing loss: Are its characteristics different? Eur. Arch. Otorhinolaryngol. 2008, 265, 1295–1300. [Google Scholar] [CrossRef]
- Martines, F.; Bentivegna, D.; Martines, E.; Sciacca, V.; Martinciglio, G. Assessing audiological, pathophysiological and psychological variables in tinnitus patients with or without hearing loss. Eur. Arch. Otorhinolaryngol. 2010, 267, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Yankaskas, K. Prelude: Noise-induced tinnitus and hearing loss in the military. Hear. Res. 2013, 295, 3–8. [Google Scholar] [CrossRef]
- Mrena, R.; Savolainen, S.; Pirvola, U.; Ylikoski, J. Characteristics of acute acoustical trauma in the Finnish Defence Forces. Int. J. Audiol. 2004, 43, 177–181. [Google Scholar] [CrossRef]
- Nottet, J.B.; Moulin, A.; Brossard, N.; Suc, B.; Job, A. Otoacoustic emissions and persistent tinnitus after acute acoustic trauma. Laryngoscope 2006, 116, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Day, B.L.; Fitzpatrick, R.C. The vestibular system. Curr. Biol. 2005, 15, R583–R586. [Google Scholar] [CrossRef]
- Golz, A.; Westerman, S.T.; Westerman, L.M.; Goldenberg, D.; Netzer, A.; Wiedmyer, T.; Fradis, M.; Joachims, H.Z. The effects of noise on the vestibular system. Am. J. Otolaryngol. 2001, 22, 190–196. [Google Scholar] [CrossRef]
- Oosterveld, W.J.; Polman, A.R.; Schoonheyt, J. Vestibular implications of noise-induced hearing loss. Br. J. Audiol. 1982, 16, 227–232. [Google Scholar] [CrossRef] [PubMed]
- McCue, M.P.; Guinan, J.J. Acoustically responsive fibers in the vestibular nerve of the cat. J. Neurosci. 1994, 14, 6058–6070. [Google Scholar] [CrossRef]
- Zhu, H.; Tang, X.; Wei, W.; Mustain, W.; Xu, Y.; Zhou, W. Click-evoked responses in vestibular afferents in rats. J. Neurophysiol. 2011, 106, 754–763. [Google Scholar] [CrossRef]
- Murofushi, T.; Curthoys, I.S.; Topple, A.N.; Colebatch, J.G.; Halmagyi, G.M. Responses of guinea pig primary vestibular neurons to clicks. Exp. Brain Res. 1995, 103, 174–178. [Google Scholar] [CrossRef]
- Ylikoski, J.; Juntunen, J.; Matikainen, E.; Ylikoski, M.; Ojala, M. Subclinical vestibular pathology in patients with noise-induced hearing loss from intense impulse noise. Acta Otolaryngol. 1988, 105, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Manabe, Y.; Kurokawa, T.; Saito, T.; Saito, H. Vestibular dysfunction in noise induced hearing loss. Acta Otolaryngol. Suppl. 1995, 519, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Ylikoski, J. Delayed endolymphatic hydrops syndrome after heavy exposure to impulse noise. Am. J. Otol. 1988, 9, 282–285. [Google Scholar]
- Shupak, A.; Bar-El, E.; Podoshin, L.; Spitzer, O.; Gordon, C.R.; Ben-David, J. Vestibular findings associated with chronic noise induced hearing impairment. Acta Otolaryngol. 1994, 114, 579–585. [Google Scholar] [CrossRef]
- Pyykkö, I.; Aalto, H.; Ylikoski, J. Does impulse noise induce vestibular disturbances? Acta Otolaryngol. Suppl. 1989, 468, 211–216. [Google Scholar] [CrossRef]
- Curthoys, I.S.; Vulovic, V.; Sokolic, L.; Pogson, J.; Burgess, A.M. Irregular primary otolith afferents from the guinea pig utricular and saccular maculae respond to both bone conducted vibration and to air conducted sound. Brain Res. Bull. 2012, 89, 16–21. [Google Scholar] [CrossRef]
- Dlugaiczyk, J. Ocular vestibular evoked myogenic potentials: Where are we now? Otol. Neurotol. 2017, 38, e513–e521. [Google Scholar] [CrossRef]
- Akin, F.W.; Murnane, O.D.; Tampas, J.W.; Clinard, C.; Byrd, S.; Kelly, J.K. The effect of noise exposure on the cervical vestibular evoked myogenic potential. Ear Hear. 2012, 33, 458–465. [Google Scholar] [CrossRef] [PubMed]
- McCue, M.P.; Guinan, J.J., Jr. Sound-evoked activity in primary afferent neurons of a mammalian vestibular system. Am. J. Otol. 1997, 18, 355–360. [Google Scholar]
- Stewart, C.E.; Kanicki, A.C.; Bauer, D.S.; Altschuler, R.A.; King, W.M. Exposure to intense noise causes vestibular loss. Mil. Med. 2020, 185, 454–461. [Google Scholar] [CrossRef]
- Jones, T.A.; Jones, S.M.; Vijayakumar, S.; Brugeaud, A.; Bothwell, M.; Chabbert, C. The adequate stimulus for mammalian linear vestibular evoked potentials (VsEPs). Hear. Res. 2011, 280, 133–140. [Google Scholar] [CrossRef]
- Tamura, H.; Ohgami, N.; Yajima, I.; Iida, M.; Ohgami, K.; Fujii, N.; Itabe, H.; Kusudo, T.; Yamashita, H.; Kato, M. Chronic exposure to low frequency noise at moderate levels causes impaired balance in mice. PLoS ONE 2012, 7, e39807. [Google Scholar] [CrossRef] [PubMed]
- McCabe, B.F.; Lawrence, M. The effects of intense sound on the non-auditory labyrinth. Acta Otolaryngol. 1958, 49, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Kühl, A.; Dixon, A.; Hali, M.; Apawu, A.K.; Muca, A.; Sinan, M.; Warila, J.; Braun, R.D.; Berkowitz, B.A.; Holt, A.G. Novel QUEST MRI in vivo measurement of noise-induced oxidative stress in the cochlea. Sci. Rep. 2019, 9, 16265. [Google Scholar] [CrossRef]
- Fetoni, A.R.; Ferraresi, A.; Picciotti, P.; Gaetani, E.; Paludetti, G.; Troiani, D. Noise induced hearing loss and vestibular dysfunction in the guinea pig. Int. J. Audiol. 2009, 48, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Soylemez, E.; Mujdeci, B. Dual-task performance and vestibular functions in individuals with noise induced hearing loss. Am. J. Otolaryngol. 2020, 41, 102665. [Google Scholar] [CrossRef]
- Musiek, F.E.; Shinn, J.; Chermak, G.D.; Bamiou, D.E. Perspectives on the pure-tone audiogram. J. Am. Acad. Audiol. 2017, 28, 655–671. [Google Scholar] [CrossRef]
- Kileny, P.R.; Zwolan, T.A.; Slager, H.K. Diagnostic audiology and electrophysiologic assessment of hearing. In Cummings Otolaryngology: Head and Neck Surgery; Flint, P., Ed.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 2021–2041. [Google Scholar]
- Pierson, L.L.; Gerhardt, K.J.; Rodriguez, G.P.; Yanke, R.B. Relationship between outer ear resonance and permanent noise-induced hearing loss. Am. J. Otolaryngol. 1994, 15, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, G.P.; Gerhardt, K.J. Influence of outer ear resonant frequency on patterns of temporary threshold shift. Ear Hear. 1991, 12, 110–114. [Google Scholar] [CrossRef] [PubMed]
- OSHA. 1904.10. Recording Criteria for Cases Involving Occupational Hearing Loss. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.10 (accessed on 12 December 2022).
- Kirchner, D.B.; Evenson, E.; Dobie, R.A.; Rabinowitz, P.; Crawford, J.; Kopke, R.; Hudson, T.W. Occupational noise-induced hearing loss: ACOEM Task Force on Occupational Hearing Loss. J. Occupat Environ. Med. 2012, 54, 106–108. [Google Scholar] [CrossRef]
- Moore, B.C.J.; Lowe, D.A.; Cox, G. Guidelines for diagnosing and quantifying noise-induced hearing loss. Trends Hear 2022, 26, 23312165221093156. [Google Scholar] [CrossRef]
- Moore, B.C.J. Diagnosis and quantification of military noise-induced hearing loss. J. Acoust. Soc. Am. 2020, 148, 884. [Google Scholar] [CrossRef]
- Moore, B.C. Cochlear hearing loss: Physiological, psychological and technical issues; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Liberman, M.C. Noise-induced and age-related hearing loss: New perspectives and potential therapies. F1000Res 2017, 6, 927. [Google Scholar] [CrossRef]
- Audiograms and Functional Auditory Testing to Assess Hearing Speech in Noise: A Review of the Clinical Evidence [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2015 Aug 17. Appendix 1, Functional Tests to Assess Speech in Noise. Available online: https://www.ncbi.nlm.nih.gov/books/NBK315846/ (accessed on 13 January 2023).
- Le Prell, C.G.; Brungart, D.S. Speech-in-noise tests and supra-threshold auditory evoked potentials as metrics for noise damage and clinical trial outcome measures. Otol. Neurotol. 2016, 37, e295–e302. [Google Scholar] [CrossRef]
- Killion, M.C.; Niquette, P.A.; Gudmundsen, G.I.; Revit, L.J.; Banerjee, S. Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J. Acoust. Soc. Am. 2004, 116, 2395–2405. [Google Scholar] [CrossRef]
- Wilson, R.H.; McArdle, R.A.; Smith, S.L. An evaluation of the BKB-SIN, HINT, QuickSIN, and WIN materials on listeners with normal hearing and listeners with hearing loss. J. Speech Lang. Hear. Res. 2007, 50, 844–856. [Google Scholar] [CrossRef]
- Taylor, B. Speech-in-noise tests: How and why to include them in your basic test battery. Hear. J. 2003, 56, 40, 42–46. [Google Scholar] [CrossRef]
- Anderson, S.; Kraus, N. Sensory-cognitive interaction in the neural encoding of speech in noise: A review. J. Am. Acad. Audiol. 2010, 21, 575–585. [Google Scholar] [CrossRef]
- Souza, P. Speech perception and hearing aids. In Hearing Aids; Popelka, G.R., Moore, B.C.J., Fay, R.R., Popper, A.N., Eds.; Springer Nature: Berlin, Germany, 2016; pp. 151–180. [Google Scholar]
- Davidson, A.; Marrone, N.; Wong, B.; Musiek, F. Predicting hearing aid satisfaction in adults: A systematic review of speech-in-noise tests and other behavioral measures. Ear Hear. 2021, 42, 1485–1498. [Google Scholar] [CrossRef]
- Hope, A.J.; Luxon, L.M.; Bamiou, D.E. Effects of chronic noise exposure on speech-in-noise perception in the presence of normal audiometry. J. Laryngol. Otol. 2013, 127, 233–238. [Google Scholar] [CrossRef]
- Dehghani-Ghahnaviyeh, S.; Zhao, Z.; Tajkhorshid, E. Lipid-mediated prestin organization in outer hair cell membranes and its implications in sound amplification. Nat. Commun. 2022, 13, 6877. [Google Scholar] [CrossRef]
- Brownell, W.E.; Bader, C.R.; Bertrand, D.; de Ribaupierre, Y. Evoked mechanical responses of isolated cochlear outer hair cells. Science 1985, 227, 194–196. [Google Scholar] [CrossRef]
- Fitzgerald, T.S.; Prieve, B.A. Detection of hearing loss using 2f2-f1 and 2f1-f2 distortion-product otoacoustic emissions. J. Speech Lang. Hear. Res. 2005, 48, 1165–1186. [Google Scholar] [CrossRef] [PubMed]
- Shera, C.A.; Guinan, J.J. Evoked otoacoustic emissions arise by two fundamentally different mechanisms: A taxonomy for mammalian OAEs. J. Acoust. Soc. Am. 1999, 105, 782–798. [Google Scholar] [CrossRef]
- Baiduc, R.R.; Dhar, S. Exploring optimal stimulus frequency ratio for measurement of the quadratic f2-f1 distortion product otoacoustic emission in humans. J. Speech Lang. Hear. Res. 2018, 61, 1794–1806. [Google Scholar] [CrossRef]
- Kapoor, N.; Mani, K.V.; Shukla, M. Distortion product oto-acoustic emission: A superior tool for hearing assessment than pure tone audiometry. Noise Health 2019, 21, 164–168. [Google Scholar] [PubMed]
- Abdala, C.; Dhar, S. Maturation and aging of the human cochlea: A view through the DPOAE looking glass. J. Assoc. Res. Otolaryngol. 2012, 13, 403–421. [Google Scholar] [CrossRef]
- Attias, J.; Bresloff, I.; Reshef, I.; Horowitz, G.; Furman, V. Evaluating noise induced hearing loss with distortion product otoacoustic emissions. Br. J. Audiol. 1998, 32, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Mills, D.M. Determining the cause of hearing loss: Differential diagnosis using a comparison of audiometric and otoacoustic emission responses. Ear Hear. 2006, 27, 508–525. [Google Scholar] [CrossRef]
- Petersen, L.; Wilson, W.J.; Kathard, H. Towards the preferred stimulus parameters for distortion product otoacoustic emissions in adults: A preliminary study. S. Afr. J. Commun. Disord. 2018, 65, e1–e10. [Google Scholar] [CrossRef]
- Petrova, L.D. Brainstem auditory evoked potentials. Am. J. Electroneurodiagn. Technol. 2009, 49, 317–332. [Google Scholar] [CrossRef]
- Young, A.; Cornejo, J.; Spinner, A. Auditory Brainstem Response. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564321/ (accessed on 19 January 2023).
- Møsller, A.R.; Jannetta, P.J.; Møsller, M.B. Neural generators of brainstem evoked potentials results from human intracranial recordings. Ann. Otol. Rhinol. Laryngol. 1981, 90, 591–596. [Google Scholar] [CrossRef]
- Parham, K.; Sun, X.-M.; Kim, D.O. Noninvasive assessment of auditory function in mice: Auditory brainstem response and distortion product otoacoustic emissions. In Handbook of Mouse Auditory Research; CRC Press: Boca Raton, FL, USA, 2001; pp. 51–72. [Google Scholar]
- Henry, K.R. Differential changes of auditory nerve and brain stem short latency evoked potentials in the laboratory mouse. Electroencephalogr. Clin. Neurophysiol. 1979, 46, 452–459. [Google Scholar] [CrossRef]
- Eggermont, J.J. Auditory brainstem response. Handb. Clin. Neurol. 2019, 160, 451–464. [Google Scholar]
- Alvarado, J.C.; Fuentes-Santamaría, V.; Jareño-Flores, T.; Blanco, J.L.; Juiz, J.M. Normal variations in the morphology of auditory brainstem response (ABR) waveforms: A study in Wistar rats. Neurosci. Res. 2012, 73, 302–311. [Google Scholar] [CrossRef]
- Chen, T.-J.; Chen, S.-S. Generator study of brainstem auditory evoked potentials by a radiofrequency lesion method in rats. Exp. Brain Res. 1991, 85, 537–542. [Google Scholar] [CrossRef]
- Gardi, J.N.; Berlin, C.I. Binaural interaction components. Their possible origins in guinea pig auditory brainstem response. Arch Otolaryngol 1981, 107, 164–168. [Google Scholar] [CrossRef]
- Melcher, J.R.; Kiang, N.Y.S. Generators of the brainstem auditory evoked potential in cat III: Identified cell populations. Hear. Res. 1996, 93, 52–71. [Google Scholar] [CrossRef]
- Bramhall, N.F.; Konrad-Martin, D.; McMillan, G.P.; Griest, S.E. Auditory brainstem response altered in humans with noise exposure despite normal outer hair cell function. Ear Hear. 2017, 38, e1–e12. [Google Scholar] [CrossRef]
- Coles, R.R.; Lutman, M.E.; Buffin, J.T. Guidelines on the diagnosis of noise-induced hearing loss for medicolegal purposes. Clin. Otolaryngol. Allied Sci. 2001, 25, 264–273. [Google Scholar] [CrossRef]
- Robinson, D.W. The audiogram in hearing loss due to noise: A probability test to uncover other causation. Ann. Occupat. Hyg. 1985, 29, 477–493. [Google Scholar]
- American Medical Association. Guides for the Evaluation of Permanent Impairment, 6th ed.; AMA: Chicago, IL, USA, 2021. [Google Scholar]
- Dobie, R.A. The AMA method of estimation of hearing disability: A validation study. Ear Hear. 2011, 32, 732–740. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency. Summary of the Noise Control Act-42 U.S.C. §4901 et seq. 1972. Available online: www.epa.gov/laws-regulations/summary-noise-control-act (accessed on 25 January 2023).
- OSHA. 1910.95 App A—Noise Exposure Computation. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.95AppA (accessed on 27 March 2023).
- NIOSH. Occupational Noise Exposure—Revised Criteria 1998. Available online: https://www.cdc.gov/niosh/docs/98-126/ (accessed on 27 March 2023).
- Centers for Disease Control and Prevention. Noise and Occupational Hearing Loss. Available online: https://www.cdc.gov/niosh/topics/noise/noise.html (accessed on 27 March 2023).
- OSHA. Hearing Conservation. Available online: https://www.osha.gov/sites/default/files/publications/osha3074.pdf (accessed on 19 January 2023).
- Arenas, J.P.; Suter, A.H. Comparison of occupational noise legislation in the Americas: An overview and analysis. Noise Health 2014, 16, 306–319. [Google Scholar] [CrossRef]
- NIOSH. NIOSH Sound Level Meter Application for iOS Devices. Available online: https://www.cdc.gov/niosh/topics/noise/pdfs/NIOSH-Sound-Level-Meter-Application-app-English.pdf (accessed on 19 January 2023).
- Crossley, E.; Biggs, T.; Brown, P.; Singh, T. The accuracy of iPhone applications to monitor environmental noise levels. Laryngoscope 2021, 131, E59–E62. [Google Scholar] [CrossRef]
- Smalt, C.J.; Ciccarelli, G.A.; Rodriguez, A.R.; Murphy, W.J. A deep neural-network classifier for photograph-based estimation of hearing protection attenuation and fit. J. Acoust. Soc. Am. 2021, 150, 1067. [Google Scholar] [CrossRef] [PubMed]
- Tikka, C.; Verbeek, J.H.; Kateman, E.; Morata, T.C.; Dreschler, W.A.; Ferrite, S. Interventions to prevent occupational noise-induced hearing loss. Cochrane Database Syst. Rev. 2017, 7, CD006396. [Google Scholar] [CrossRef] [PubMed]
- Salmani Nodoushan, M.; Mehrparvar, A.H.; Torab Jahromi, M.; Safaei, S.; Mollasadeghi, A. Training in using earplugs or using earplugs with a higher than necessary noise reduction rating? A randomized clinical trial. Int. J. Occup. Environ. Med. 2014, 5, 187–193. [Google Scholar]
- Smalt, C.J.; Calamia, P.T.; Dumas, A.P.; Perricone, J.P.; Patel, T.; Bobrow, J.; Collins, P.P.; Markey, M.L.; Quatieri, T.F. The effect of hearing-protection devices on auditory situational awareness and listening effort. Ear Hear. 2020, 41, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Preventing Noise-Induced Hearing Loss. Available online: https://www.cdc.gov/ncbddd/hearingloss/noise.html (accessed on 19 January 2023).
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G.; et al. Clinical practice guideline: Sudden hearing loss (update). Otolaryngol. Head. Neck Surg. 2019, 161, S1–S45. [Google Scholar] [CrossRef]
- American Academy of Audiology. Audiology Clinical Practice Algorithms and Statements. Available online: https://www.audiology.org/practice-guideline/audiology-clinical-practice-algorithms-and-statements/ (accessed on 20 January 2023).
- National Guideline Centre (UK); National Institute for Health and Care Excellence (NICE). Hearing Loss in Adults: Assessment and Management. (NICE Guideline, No. 98.) 1, Guideline Summary. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536565/ (accessed on 20 January 2023).
- Zhou, Y.; Zheng, G.; Zheng, H.; Zhou, R.; Zhu, X.; Zhang, Q. Primary observation of early transtympanic steroid injection in patients with delayed treatment of noise-induced hearing loss. Audiol. Neurotol. 2013, 18, 89–94. [Google Scholar] [CrossRef]
- Chang, Y.S.; Bang, K.H.; Jeong, B.; Lee, G.G. Effects of early intratympanic steroid injection in patients with acoustic trauma caused by gunshot noise. Acta Otolaryngol. 2017, 137, 716–719. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Davis, A.C.; Hoffman, H.J. Hearing loss grades and the International classification of functioning, disability and health. Bull. World Health Organ. 2019, 97, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.V.M.; Ribas, A.; Calleros, J. Free Field Word recognition test in the presence of noise in normal hearing adults. Braz. J. Otorhinolaryngol. 2017, 83, 665–669. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the Informal Working Group on Prevention of Deafness and Hearing Impairment Programme Planning, Geneva, 18–21 June 1991. Available online: https://apps.who.int/iris/handle/10665/58839 (accessed on 25 January 2023).
- Hapsari, A.A.; Kusmawan, D. Noise-Induced Hearing Loss (NIHL) Risk Factors Among Manufacturing Industry Workers: A Systematic Review [PREPRINT]. Available online: https://doi.org/10.21203/rs.3.rs-643998/v1 (accessed on 19 January 2023). [CrossRef]
- Toppila, E.; Pyykkö, I.I.; Starck, J.; Kaksonen, R.; Ishizaki, H. Individual risk factors in the development of noise-induced hearing loss. Noise Health 2000, 2, 59–70. [Google Scholar] [PubMed]
- Barone, J.A.; Peters, J.M.; Garabrant, D.H.; Bernstein, L.; Krebsbach, R. Smoking as a risk factor in noise-induced hearing loss. J. Occup. Med. 1987, 29, 741–745. [Google Scholar]
- Toppila, E.; Pyykkö, I.; Starck, J. Age and noise-induced hearing loss. Scand. Audiol. 2001, 30, 236–244. [Google Scholar] [CrossRef]
- Golmohammadi, R.; Darvishi, E. The combined effects of occupational exposure to noise and other risk factors—a systematic review. Noise Health 2019, 21, 125–141. [Google Scholar]
- Chen, K.H.; Su, S.B.; Chen, K.T. An overview of occupational noise-induced hearing loss among workers: Epidemiology, pathogenesis, and preventive measures. Environ. Health Prev. Med. 2020, 25, 65. [Google Scholar] [CrossRef]
- Masterson, E.A.; Bushnell, P.T.; Themann, C.L.; Morata, T.C. Hearing impairment among noise-exposed workers—United States, 2003–2012. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 389–394. [Google Scholar] [CrossRef]
- OSHA. Occupational Noise Exposure. Available online: https://www.osha.gov/noise (accessed on 25 January 2023).
- Tak, S.; Davis, R.R.; Calvert, G.M. Exposure to hazardous workplace noise and use of hearing protection devices among US workers--NHANES, 1999–2004. Am. J. Ind. Med. 2009, 52, 358–371. [Google Scholar] [CrossRef]
- Mirza, R.; Kirchner, D.B.; Dobie, R.A.; Crawford, J.; ACOEM Task Force on Occupational Hearing Loss. Occupational noise-induced hearing loss. J. Occup. Environ. Med. 2018, 60, e498–e501. [Google Scholar] [CrossRef] [PubMed]
- Yong, J.S.; Wang, D.Y. Impact of noise on hearing in the military. Mil. Med. Res. 2015, 2, 6. [Google Scholar] [CrossRef]
- Henselman, L.W.; Henderson, D.; Shadoan, J.; Subramaniam, M.; Saunders, S.; Ohlin, D. Effects of noise exposure, race, and years of service on hearing in US Army soldiers. Ear Hear. 1995, 16, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Collee, A.; Legrand, C.; Govaerts, B.; Veken, P.; De Boodt, F.; Degrave, E. Occupational exposure to noise and the prevalence of hearing loss in a Belgian military population: A cross-sectional study. Noise Health 2011, 13, 64–70. [Google Scholar] [PubMed]
- Hughes, H.; Hunting, K.L. Evaluation of the effects of exposure to organic solvents and hazardous noise among US Air Force Reserve personnel. Noise Health 2013, 15, 379–387. [Google Scholar] [CrossRef]
- US Veteran’s Administration. 2021 Annual Benefits Report: Service-Connected Disability or Death Benefits. Available online: https://www.benefits.va.gov/REPORTS/abr/docs/2021_compensation.pdf (accessed on 30 January 2023).
- Gubata, M.E.; Packnett, E.R.; Feng, X.; Cowan, D.N.; Niebuhr, D.W. Pre-enlistment hearing loss and hearing loss disability among US soldiers and marines. Noise Health 2013, 15, 289–295. [Google Scholar] [CrossRef]
- Chandrasekhar, S.S.; Rubinstein, R.Y.; Kwartler, J.A.; Gatz, M.; Connelly, P.E.; Huang, E.; Baredes, S. Dexamethasone pharmacokinetics in the inner ear: Comparison of route of administration and use of facilitating agents. Otolaryngol. Head. Neck Surg. 2000, 122, 521–528. [Google Scholar]
- Leong, S.T.; Laortanakul, P. Monitoring and assessment of daily exposure of roadside workers to traffic noise levels in an Asian city: A case study of Bangkok streets. Environ. Monit. Assess. 2003, 85, 69–85. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for, E. Burden of Disease from Environmental Noise: Quantification of Healthy Life Years Lost in Europe; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Dillard, L.K.; Arunda, M.O.; Lopez-Perez, L.; Martinez, R.X.; Jiménez, L.; Chadha, S. Prevalence and global estimates of unsafe listening practices in adolescents and young adults: A systematic review and meta-analysis. BMJ Glob. Health 2022, 7, e010501. [Google Scholar] [CrossRef]
- English, W. 2021 National Firearms Survey (14 July 2021). Georgetown McDonough School of Business Research Paper No. 3887145. Available online: https://ssrn.com/abstract=3887145 (accessed on 25 January 2023).
- Bielefeld, E.C.; Harrison, R.T.; Riley DeBacker, J. Pharmaceutical otoprotection strategies to prevent impulse noise-induced hearing loss. J. Acoust. Soc. Am. 2019, 146, 3790. [Google Scholar] [CrossRef]
- Ohlemiller, K.K. Recent findings and emerging questions in cochlear noise injury. Hear. Res. 2008, 245, 5–17. [Google Scholar] [CrossRef]
- Watkins-Chow, D.E.; Pavan, W.J. Genomic copy number and expression variation within the C57BL/6J inbred mouse strain. Genome Res. 2008, 18, 60–66. [Google Scholar] [CrossRef]
- Heinonen-Guzejev, M.; Vuorinen, H.S.; Mussalo-Rauhamaa, H.; Heikkilä, K.; Koskenvuo, M.; Kaprio, J. Genetic component of noise sensitivity. Twin Res. Hum. Genet. 2005, 8, 245–249. [Google Scholar] [CrossRef]
- Konings, A.; Van Laer, L.; Van Camp, G. Genetic studies on noise-induced hearing loss: A review. Ear Hear. 2009, 30, 151–159. [Google Scholar] [CrossRef]
- Candreia, C.; Martin, G.K.; Stagner, B.B.; Lonsbury-Martin, B.L. Distortion product otoacoustic emissions show exceptional resistance to noise exposure in MOLF/Ei mice. Hear. Res. 2004, 194, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, A.E.; Jimenez, A.M.; Martin, G.K.; Luebke, A.E.; Lonsbury-Martin, B.L. Evaluating cochlear function and the effects of noise exposure in the B6.CAST+Ahl mouse with distortion product otoacoustic emissions. Hear. Res. 2004, 194, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Hequembourg, S.J.; Atencio, C.A.; Rosowski, J.J.; Liberman, M.C. Acoustic injury in mice: 129/SvEv is exceptionally resistant to noise-induced hearing loss. Hear. Res. 2000, 141, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Sugahara, K.; Inouye, S.; Izu, H.; Katoh, Y.; Katsuki, K.; Takemoto, T.; Shimogori, H.; Yamashita, H.; Nakai, A. Heat shock transcription factor HSF1 is required for survival of sensory hair cells against acoustic overexposure. Hear. Res. 2003, 182, 88–96. [Google Scholar] [CrossRef]
- Tan, J.; Kaiserman, D.; O’Leary, S.J.; Bird, P.I. Increased susceptibility to acoustic trauma in a mouse model of non-syndromic sensorineural deafness, DFNB91. Eur. J. Neurosci. 2021, 53, 1638–1651. [Google Scholar] [CrossRef]
- Kozel, P.J.; Davis, R.R.; Krieg, E.F.; Shull, G.E.; Erway, L.C. Deficiency in plasma membrane calcium ATPase isoform 2 increases susceptibility to noise-induced hearing loss in mice. Hear. Res. 2002, 164, 231–239. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; McFadden, S.L.; Ding, D.L.; Lear, P.M.; Ho, Y.S. Targeted mutation of the gene for cellular glutathione peroxidase (Gpx1) increases noise-induced hearing loss in mice. J. Assoc. Res. Otolaryngol. 2000, 1, 243–254. [Google Scholar] [CrossRef]
- Tabuchi, K.; Suzuki, M.; Mizuno, A.; Hara, A. Hearing impairment in TRPV4 knockout mice. Neurosci. Lett. 2005, 382, 304–308. [Google Scholar] [CrossRef]
- Schick, B.; Praetorius, M.; Eigenthaler, M.; Jung, V.; Müller, M.; Walter, U.; Knipper, M. Increased noise sensitivity and altered inner ear MENA distribution in VASP-/- mice. Cell. Tissue Res. 2004, 318, 493–502. [Google Scholar] [CrossRef]
- Fairfield, D.A.; Lomax, M.I.; Dootz, G.A.; Chen, S.; Galecki, A.T.; Benjamin, I.J.; Dolan, D.F.; Altschuler, R.A. Heat shock factor 1-deficient mice exhibit decreased recovery of hearing following noise overstimulation. J. Neurosci. Res. 2005, 81, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Duan, H.; Zhang, D.; Liang, Y.; Xu, C.; Wu, Y.; Tian, X.; Pang, Z.; Tan, Q.; Li, S.; Qiu, C. Heritability of age-related hearing loss in middle-aged and elderly chinese: A population-based twin study. Ear Hear. 2019, 40, 253–259. [Google Scholar] [CrossRef]
- Kvestad, E.; Czajkowski, N.; Krog, N.H.; Engdahl, B.; Tambs, K. Heritability of hearing loss. Epidemiology 2012, 23, 328–331. [Google Scholar] [CrossRef]
- Chen, X.-M.; Xue, X.-M.; Yu, N.; Guo, W.-W.; Yuan, S.-L.; Jiang, Q.-Q.; Yang, S.-M. The role of genetic variants in the susceptibility of noise-induced hearing loss. Front. Cell. Neurosci. 2022, 16, 946206. [Google Scholar] [CrossRef]
- Konings, A.; Van Laer, L.; Pawelczyk, M.; Carlsson, P.I.; Bondeson, M.L.; Rajkowska, E.; Dudarewicz, A.; Vandevelde, A.; Fransen, E.; Huyghe, J.; et al. Association between variations in CAT and noise-induced hearing loss in two independent noise-exposed populations. Hum. Mol. Genet. 2007, 16, 1872–1883. [Google Scholar] [CrossRef]
- Rabinowitz, P.M.; Pierce Wise, J.; Hur Mobo, B.; Antonucci, P.G.; Powell, C.; Slade, M. Antioxidant status and hearing function in noise-exposed workers. Hear. Res. 2002, 173, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, G.; Marciano, E.; Zarrilli, F.; Mazzaccara, C.; Intrieri, M.; Calcagno, G.; Vitale, D.F.; La Manna, P.; Saulino, C.; Marcelli, V.; et al. Paraoxonase and superoxide dismutase gene polymorphisms and noise-induced hearing loss. Clin. Chem. 2004, 50, 2012–2018. [Google Scholar] [CrossRef] [PubMed]
- Van Laer, L.; Carlsson, P.I.; Ottschytsch, N.; Bondeson, M.L.; Konings, A.; Vandevelde, A.; Dieltjens, N.; Fransen, E.; Snyders, D.; Borg, E.; et al. The contribution of genes involved in potassium-recycling in the inner ear to noise-induced hearing loss. Hum. Mutat. 2006, 27, 786–795. [Google Scholar] [CrossRef]
- Pawelczyk, M.; Van Laer, L.; Fransen, E.; Rajkowska, E.; Konings, A.; Carlsson, P.I.; Borg, E.; Van Camp, G.; Sliwinska-Kowalska, M. Analysis of gene polymorphisms associated with K ion circulation in the inner ear of patients susceptible and resistant to noise-induced hearing loss. Ann. Hum. Genet. 2009, 73, 411–421. [Google Scholar] [CrossRef]
- Sliwinska-Kowalska, M.; Pawelczyk, M. Contribution of genetic factors to noise-induced hearing loss: A human studies review. Mutat. Res. 2013, 752, 61–65. [Google Scholar] [CrossRef]
- Yoshida, N.; Kristiansen, A.; Liberman, M.C. Heat stress and protection from permanent acoustic injury in mice. J. Neurosci. 1999, 19, 10116–10124. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Tan, H.; Yang, Q.; Wang, F.; Yao, H.; Wei, Q.; Tanguay, R.M.; Wu, T. Association of hsp70 polymorphisms with risk of noise-induced hearing loss in Chinese automobile workers. Cell. Stress. Chaperones 2006, 11, 233–239. [Google Scholar] [CrossRef]
- Konings, A.; Van Laer, L.; Michel, S.; Pawelczyk, M.; Carlsson, P.I.; Bondeson, M.L.; Rajkowska, E.; Dudarewicz, A.; Vandevelde, A.; Fransen, E.; et al. Variations in HSP70 genes associated with noise-induced hearing loss in two independent populations. Eur. J. Hum. Genet. 2009, 17, 329–335. [Google Scholar] [CrossRef]
- Konings, A.; Van Laer, L.; Wiktorek-Smagur, A.; Rajkowska, E.; Pawelczyk, M.; Carlsson, P.I.; Bondeson, M.L.; Dudarewicz, A.; Vandevelde, A.; Fransen, E.; et al. Candidate gene association study for noise-induced hearing loss in two independent noise-exposed populations. Ann. Hum. Genet. 2009, 73, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wilson, C.M.; Mendelev, N.; Ge, Y.; Galfalvy, H.; Elder, G.; Ahlers, S.; Yarnell, A.M.; LoPresti, M.L.; Kamimori, G.H.; et al. Acute and chronic molecular signatures and associated symptoms of blast exposure in military breachers. J. Neurotrauma 2020, 37, 1221–1232. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Li, P.H.; Li, H.; Colicino, E.; Colicino, S.; Wen, Y.; Zhang, R.; Feng, X.; Barrow, T.M.; Cayir, A.; et al. Effects of environmental noise exposure on DNA methylation in the brain and metabolic health. Environ. Res. 2017, 153, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.T.; Wang, J.; Wang, Y.; Chen, F.Q. Association between histone deacetylases and the loss of cochlear hair cells: Role of the former in noise-induced hearing loss. Int. J. Mol. Med. 2015, 36, 534–540. [Google Scholar] [CrossRef]
- Chen, J.; Hill, K.; Sha, S.H. Inhibitors of histone deacetylases attenuate noise-induced hearing loss. J. Assoc. Res. Otolaryngol. 2016, 17, 289–302. [Google Scholar] [CrossRef]
- Yang, D.H.; Xie, J.; Liu, K.; Peng, Z.; Guo, J.Y.; Yu, S.K.; Wang, G.P.; Gong, S.S. The histone deacetylase inhibitor sodium butyrate protects against noise-induced hearing loss in Guinea pigs. Neurosci. Lett. 2017, 660, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.; Long, H.; Pan, S.; Lai, R.; Wang, X.; Zhu, Y.; Hill, K.; Fang, Q.; Zheng, Y.; Sha, S.H. Inhibition of histone methyltransferase G9a attenuates noise-induced cochlear synaptopathy and hearing loss. J. Assoc. Res. Otolaryngol. 2019, 20, 217–232. [Google Scholar] [CrossRef]
- Ding, L.; Liu, J.; Shen, H.X.; Pan, L.P.; Liu, Q.D.; Zhang, H.D.; Han, L.; Shuai, L.G.; Ding, E.M.; Zhao, Q.N.; et al. Analysis of plasma microRNA expression profiles in male textile workers with noise-induced hearing loss. Hear. Res. 2016, 333, 275–282. [Google Scholar] [CrossRef]
- Li, Y.H.; Yang, Y.; Yan, Y.T.; Xu, L.W.; Ma, H.Y.; Shao, Y.X.; Cao, C.J.; Wu, X.; Qi, M.J.; Wu, Y.Y.; et al. Analysis of serum microRNA expression in male workers with occupational noise-induced hearing loss. Braz. J. Med. Biol. Res. 2018, 51, e6426. [Google Scholar] [CrossRef]
- Patel, M.; Cai, Q.; Ding, D.; Salvi, R.; Hu, Z.; Hu, B.H. The miR-183/Taok1 target pair is implicated in cochlear responses to acoustic trauma. PLoS ONE 2013, 8, e58471. [Google Scholar] [CrossRef]
- Leso, V.; Fontana, L.; Finiello, F.; De Cicco, L.; Luigia Ercolano, M.; Iavicoli, I. Noise induced epigenetic effects: A systematic review. Noise Health 2020, 22, 77–89. [Google Scholar]
- Tahera, Y.; Meltser, I.; Johansson, P.; Bian, Z.; Stierna, P.; Hansson, A.C.; Canlon, B. NF-kappaB mediated glucocorticoid response in the inner ear after acoustic trauma. J. Neurosci. Res. 2006, 83, 1066–1076. [Google Scholar] [CrossRef]
- Terunuma, T.; Hara, A.; Senarita, M.; Motohashi, H.; Kusakari, J. Effect of acoustic overstimulation on regulation of glucocorticoid receptor mRNA in the cochlea of the guinea pig. Hear. Res. 2001, 151, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.M.; Rarey, K.E. Effect of stress on cochlear glucocorticoid protein. II. Restraint. Hear. Res. 1995, 92, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Scheibe, F.; Haupt, H.; Vlastos, G.A. Preventive magnesium supplement reduces ischemia-induced hearing loss and blood viscosity in the guinea pig. Eur. Arch. Otorhinolaryngol. 2000, 257, 355–361. [Google Scholar] [CrossRef]
- Altura, B.M.; Altura, B.T.; Gebrewold, A.; Ising, H.; Günther, T. Noise-induced hypertension and magnesium in rats: Relationship to microcirculation and calcium. J. Appl. Physiol. 1992, 72, 194–202. [Google Scholar] [CrossRef]
- Choi, Y.H.; Miller, J.M.; Tucker, K.L.; Hu, H.; Park, S.K. Antioxidant vitamins and magnesium and the risk of hearing loss in the US general population. Am. J. Clin. Nutr. 2014, 99, 148–155. [Google Scholar] [CrossRef]
- Alvarado, J.C.; Fuentes-Santamaría, V.; Melgar-Rojas, P.; Gabaldón-Ull, M.C.; Cabanes-Sanchis, J.J.; Juiz, J.M. Oral antioxidant vitamins and magnesium limit noise-induced hearing loss by promoting sensory hair cell survival: Role of antioxidant enzymes and apoptosis genes. Antioxidants 2020, 9, 1177. [Google Scholar] [CrossRef]
- Abbasi, M.; Pourrajab, B.; Tokhi, M.O. Protective effects of vitamins/antioxidants on occupational noise-induced hearing loss: A systematic review. J. Occupat Health 2021, 63, e12217. [Google Scholar] [CrossRef]
- Le Prell, C.G.; Fulbright, A.; Spankovich, C.; Griffiths, S.K.; Lobarinas, E.; Campbell, K.C.; Antonelli, P.J.; Green, G.E.; Guire, K.; Miller, J.M. Dietary supplement comprised of β-carotene, vitamin C, vitamin E, and magnesium: Failure to prevent music-induced temporary threshold shift. Audiol. Neurotol. Extra 2016, 6, 20–39. [Google Scholar] [CrossRef] [PubMed]
- Attias, J.; Weisz, G.; Almog, S.; Shahar, A.; Wiener, M.; Joachims, Z.; Netzer, A.; Ising, H.; Rebentisch, E.; Guenther, T. Oral magnesium intake reduces permanent hearing loss induced by noise exposure. Am. J. Otolaryngol. 1994, 15, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Attias, J.; Sapir, S.; Bresloff, I.; Reshef-Haran, I.; Ising, H. Reduction in noise-induced temporary threshold shift in humans following oral magnesium intake. Clin. Otolaryngol. Allied Sci. 2004, 29, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, A.; Scaringi, A.; Bartoli, R.; Margarito, M.A.; Quaranta, N. The effects of ’supra-physiological’ vitamin B12 administration on temporary threshold shift. Int. J. Audiol. 2004, 43, 162–165. [Google Scholar] [CrossRef]
- Kapoor, N.; Mani, K.V.; Shyam, R.; Sharma, R.K.; Singh, A.P.; Selvamurthy, W. Effect of vitamin E supplementation on carbogen-induced amelioration of noise induced hearing loss in man. Noise Health 2011, 13, 452–458. [Google Scholar] [CrossRef]
- Yeh, C.W.; Tseng, L.H.; Yang, C.H.; Hwang, C.F. Effects of oral zinc supplementation on patients with noise-induced hearing loss associated tinnitus: A clinical trial. Biomed. J. 2019, 42, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kopke, R.; Allen, K.A.; Henderson, D.; Hoffer, M.; Frenz, D.; Van de Water, T. A radical demise. Toxins and trauma share common pathways in hair cell death. Ann. NY Acad. Sci. 1999, 884, 171–191. [Google Scholar] [CrossRef]
- Coleman, J.K.; Kopke, R.D.; Liu, J.; Ge, X.; Harper, E.A.; Jones, G.E.; Cater, T.L.; Jackson, R.L. Pharmacological rescue of noise induced hearing loss using N-acetylcysteine and acetyl-L-carnitine. Hear. Res. 2007, 226, 104–113. [Google Scholar] [CrossRef]
- Aruoma, O.I.; Halliwell, B.; Hoey, B.M.; Butler, J. The antioxidant action of N-acetylcysteine: Its reaction with hydrogen peroxide, hydroxyl radical, superoxide, and hypochlorous acid. Free. Radic. Biol. Med. 1989, 6, 593–597. [Google Scholar] [CrossRef]
- Lin, C.Y.; Wu, J.L.; Shih, T.S.; Tsai, P.J.; Sun, Y.M.; Ma, M.C.; Guo, Y.L. N-Acetyl-cysteine against noise-induced temporary threshold shift in male workers. Hear. Res. 2010, 269, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Kopke, R.; Slade, M.D.; Jackson, R.; Hammill, T.; Fausti, S.; Lonsbury-Martin, B.; Sanderson, A.; Dreisbach, L.; Rabinowitz, P.; Torre, P.; et al. Efficacy and safety of N-acetylcysteine in prevention of noise induced hearing loss: A randomized clinical trial. Hear. Res. 2015, 323, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Canlon, B. Protective mechanisms of sound conditioning. Adv. Otorhinolaryngol. 2002, 59, 96–105. [Google Scholar]
- Henderson, D.; McFadden, S.L.; Liu, C.C.; Hight, N.; Zheng, X.Y. The role of antioxidants in protection from impulse noise. Ann. NY Acad. Sci. 1999, 884, 368–380. [Google Scholar] [CrossRef]
- Jacono, A.A.; Hu, B.; Kopke, R.D.; Henderson, D.; Van De Water, T.R.; Steinman, H.M. Changes in cochlear antioxidant enzyme activity after sound conditioning and noise exposure in the chinchilla. Hear. Res. 1998, 117, 31–38. [Google Scholar] [CrossRef]
- Harris, K.C.; Bielefeld, E.; Hu, B.H.; Henderson, D. Increased resistance to free radical damage induced by low-level sound conditioning. Hear. Res. 2006, 213, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Kil, J.; Harruff, E.E.; Longenecker, R.J. Development of ebselen for the treatment of sensorineural hearing loss and tinnitus. Hear. Res. 2022, 413, 108209. [Google Scholar] [CrossRef]
- Kil, J.; Pierce, C.; Tran, H.; Gu, R.; Lynch, E.D. Ebselen treatment reduces noise induced hearing loss via the mimicry and induction of glutathione peroxidase. Hear. Res. 2007, 226, 44–51. [Google Scholar] [CrossRef]
- Lynch, E.D.; Gu, R.; Pierce, C.; Kil, J. Ebselen-mediated protection from single and repeated noise exposure in rat. Laryngoscope 2004, 114, 333–337. [Google Scholar] [CrossRef]
- Kil, J.; Lobarinas, E.; Spankovich, C.; Griffiths, S.K.; Antonelli, P.J.; Lynch, E.D.; Le Prell, C.G. Safety and efficacy of ebselen for the prevention of noise-induced hearing loss: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2017, 390, 969–979. [Google Scholar] [CrossRef]
- Psillas, G.; Pavlidis, P.; Karvelis, I.; Kekes, G.; Vital, V.; Constantinidis, J. Potential efficacy of early treatment of acute acoustic trauma with steroids and piracetam after gunshot noise. Eur. Arch. Otorhinolaryngol. 2008, 265, 1465–1469. [Google Scholar] [CrossRef] [PubMed]
- Zloczower, E.; Tsur, N.; Hershkovich, S.; Fink, N.; Marom, T. Efficacy of oral steroids for acute acoustic trauma. Audiol. Neurotol. 2022, 27, 312–320. [Google Scholar] [CrossRef]
- Rhee, T.M.; Hwang, D.; Lee, J.S.; Park, J.; Lee, J.M. Addition of hyperbaric oxygen therapy vs medical therapy alone for idiopathic sudden sensorineural hearing loss: A systematic review and meta-analysis. JAMA Otolaryngol. Head. Neck Surg. 2018, 144, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Hashida, K.; Nguyen, K.-H.; Hohchi, N.; Katoh, A.; Koizumi, H.; Ohbuchi, T. Efficacy of intratympanic steroid administration on idiopathic sudden sensorineural hearing loss in comparison with hyperbaric oxygen therapy. Laryngoscope 2012, 122, 1154–1157. [Google Scholar] [CrossRef]
- Oya, M.; Tadano, Y.; Takihata, Y.; Ikomi, F.; Tokunaga, T. Utility of hyperbaric oxygen therapy for acute acoustic trauma: 20 years’ experience at the japan maritime self-defense force undersea medical center. Int. Arch. Otorhinolaryngol. 2019, 23, e408–e414. [Google Scholar] [CrossRef] [PubMed]
- Ylikoski, J.; Mrena, R.; Makitie, A.; Kuokkanen, J.; Pirvola, U.; Savolainen, S. Hyperbaric oxygen therapy seems to enhance recovery from acute acoustic trauma. Acta Otolaryngol. 2008, 128, 1110–1115. [Google Scholar] [CrossRef]
- Salihoğlu, M.; Ay, H.; Cincik, H.; Cekin, E.; Cesmeci, E.; Memis, A.; Uzun, G.; Altundag, A.; Simsek, K. Efficiency of hyperbaric oxygen and steroid therapy in treatment of hearing loss following acoustic trauma. Undersea Hyperb. Med. 2015, 42, 539–546. [Google Scholar] [PubMed]
- Fakhry, N.; Rostain, J.C.; Cazals, Y. Hyperbaric oxygenation with corticoid in experimental acoustic trauma. Hear. Res. 2007, 230, 88–92. [Google Scholar] [CrossRef]
- Lafère, P.; Vanhoutte, D.; Germonprè, P. Hyperbaric oxygen therapy for acute noise-induced hearing loss: Evaluation of different treatment regimens. Diving Hyperb. Med. 2010, 40, 63–67. [Google Scholar]
- Bayoumy, A.B.; van der Veen, E.L.; van Ooij, P.A.M.; Besseling-Hansen, F.S.; Koch, D.A.A.; Stegeman, I.; de Ru, J.A. Effect of hyperbaric oxygen therapy and corticosteroid therapy in military personnel with acute acoustic trauma. BMJ Mil. Health 2020, 166, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.L.; Smith, K.J.; Palmer, C. Cost-effectiveness analysis of a military hearing conservation program. Mil. Med. 2018, 183, e547–e553. [Google Scholar] [CrossRef] [PubMed]




| Sound Pressure Level (dB) | Permissible Exposure Time | |
|---|---|---|
| NIOSH | OSHA | |
| 120 | 9 s | 7 min 30 s |
| 115 | 28 s | 15 min |
| 112 | 56 s | 22 min 48 s |
| 110 | 1 min 29 s | 30 min |
| 109 | 1 min 53 s | 34 min 12 s |
| 106 | 3 min 45 s | 52 min 12 s |
| 105 | 4 min 43 s | 1 h |
| 103 | 7 min 30 s | 1 h 18 min |
| 100 | 15 min | 2 h |
| 97 | 30 min | 3 h |
| 95 | 47 min 37 s | 4 h |
| 94 | 1 h | 4 h 36 min |
| 91 | 2 h | 7 h |
| 90 | 2 h 31 min | 8 h |
| 88 | 4 h | 10 h 36 min |
| 85 | 8 h | 16 h |
| 82 | 16 h | 24 h 18 min |
| 81 | 20 h 10 min | 27 h 54 min |
| 80 | 25 h 24 min | 32 h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natarajan, N.; Batts, S.; Stankovic, K.M. Noise-Induced Hearing Loss. J. Clin. Med. 2023, 12, 2347. https://doi.org/10.3390/jcm12062347
Natarajan N, Batts S, Stankovic KM. Noise-Induced Hearing Loss. Journal of Clinical Medicine. 2023; 12(6):2347. https://doi.org/10.3390/jcm12062347
Chicago/Turabian StyleNatarajan, Nirvikalpa, Shelley Batts, and Konstantina M. Stankovic. 2023. "Noise-Induced Hearing Loss" Journal of Clinical Medicine 12, no. 6: 2347. https://doi.org/10.3390/jcm12062347