
Complement Binding Anti-HLA Antibodies and the Survival of Kidney Transplantation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Determination of DSA Complement Binding Capacity: C1q Technique
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis of the Population and Characteristics Prior to Renal Transplantation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency | Percentage (%) | ||
|---|---|---|---|
| Total Incompatibilities | 0 | 3 | 1.2 |
| 1 | 2 | 0.8 | |
| 2 | 5 | 2.0 | |
| 3 | 28 | 11.4 | |
| 4 | 61 | 24.9 | |
| 5 | 89 | 36.3 | |
| 6 | 57 | 23.3 | |
| Total | 245 | 100 | |
| Frequency | Percentage (%) | ||
| cPRA% | Negative | 192 | 78.4 |
| 1–50% | 31 | 12.7 | |
| 51–94% | 12 | 4.9 | |
| 95–100% | 10 | 4.1 | |
| Total | 245 | 100 | |
| Frequency | Percentage (%) | ||
| DSA pre-transplant | NO | 240 | 98 |
| YES | 5 | 2 | |
| Total | 245 | 100 | |
| Frequency | Percentage (%) | ||
| DSA pre-transplant complement fixers | NO | 5 | 100 |
| YES | 0 | 0 | |
| Total | 5 | 100 |
3.2. Analysis of Post-Renal Transplant Characteristics
3.3. Rejection Events
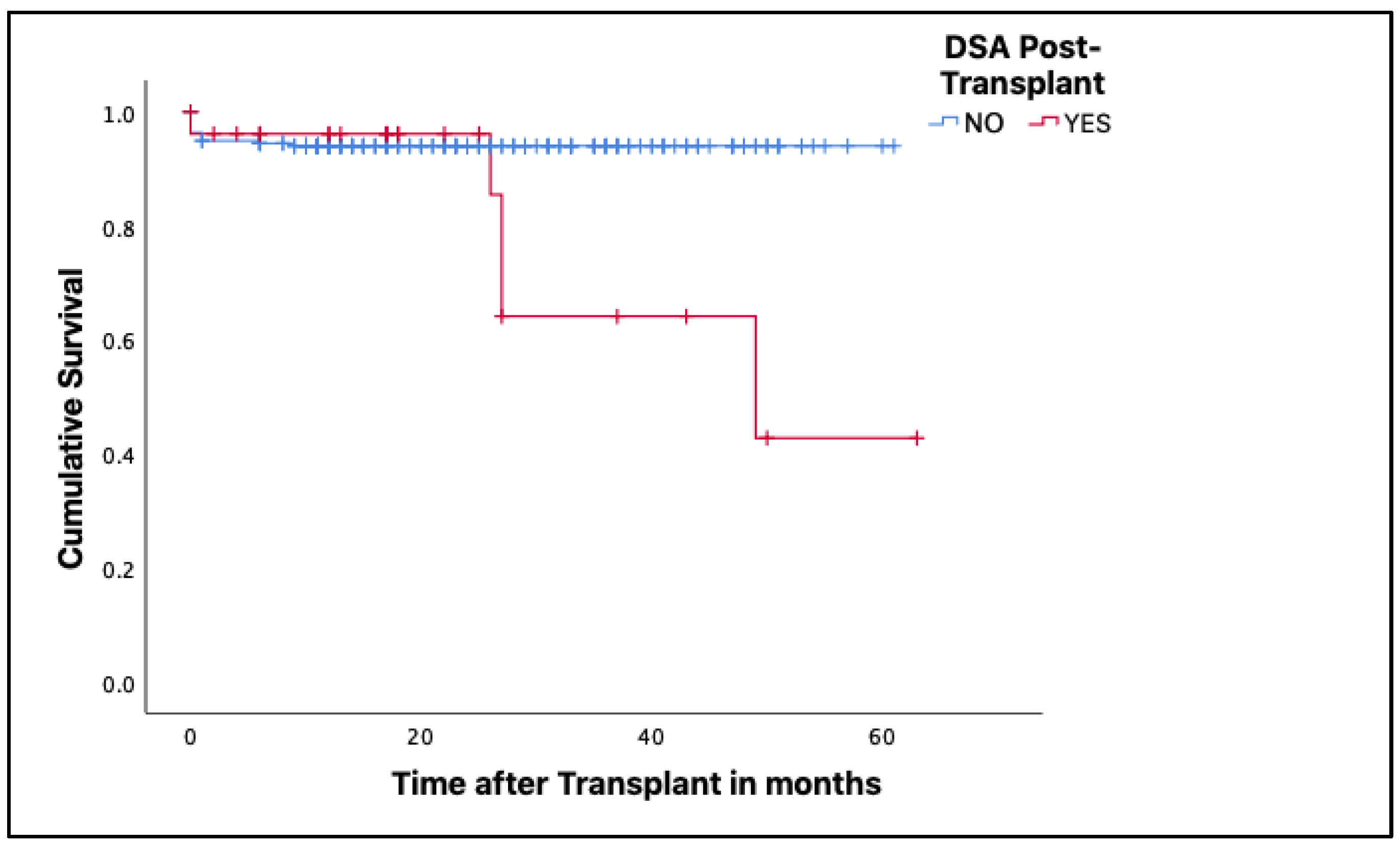
3.4. Renal Graft Survival Associated with the Presence of dnDSA
3.5. Renal Graft Loss
3.6. Relationship between MFI Values of dnDSA and Its C1q Binding Capacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hernández, D.; Alonso-Titos, J.; Armas-Padrón, A.M.; Ruiz-Esteban, P.; Cabello, M.; López, V.; Fuentes, L.; Jironda, C.; Ros, S.; Jiménez, T.; et al. Mortality in Elderly Waiting-List Patients Versus Age-Matched Kidney Transplant Recipients: Where Is the Risk? Kidney Blood Press. Res. 2018, 43, 256–275. [Google Scholar] [CrossRef]
- Kaballo, M.A.; Canney, M.; O’Kelly, P.; Williams, Y.; O’Seaghdha, C.M.; Conlon, P.J. A Comparative Analysis of Survival of Patients on Dialysis and after Kidney Transplantation. Clin. Kidney J. 2018, 11, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P. Clinical Trials in End-Stage Renal Disease—Priorities and Challenges. Nephrol. Dial. Transplant. 2019, 34, 1084–1089. [Google Scholar] [CrossRef]
- Robinson, J.; Halliwell, J.; Hayhurst, J.; Flicek, P.; Parham, P.; Marsh, S. The IPD and IMGT/HLA Database: Allele Variant Databases. Available online: http://hla.alleles.org/alleles/index.html (accessed on 20 May 2019).
- Edward, J. Moticka Transplantation Immunology. In A Historical Perspective on Evidence—Based Immunology; Elsevier: Amsterdam, The Netherlands, 2016; pp. 317–327. ISBN 978-0-12-398381-7. [Google Scholar]
- Williams, R.C.; Opelz, G.; Weil, E.J.; McGarvey, C.J.; Chakkera, H.A. The Risk of Transplant Failure With HLA Mismatch in First Adult Kidney Allografts 2. Transplant. Direct 2017, 3, e152. [Google Scholar] [CrossRef]
- Yacoub, R.; Nadkarni, G.N.; Cravedi, P.; He, J.C.; Delaney, V.B.; Kent, R.; Chauhan, K.N.; Coca, S.G.; Florman, S.S.; Heeger, P.S.; et al. Analysis of OPTN/UNOS Registry Suggests the Number of HLA Matches and Not Mismatches Is a Stronger Independent Predictor of Kidney Transplant Survival. Kidney Int. 2018, 93, 482–490. [Google Scholar] [CrossRef]
- Lopes, D.; Barra, T.; Malheiro, J.; Tafulo, S.; Martins, L.; Almeida, M.; Pedroso, S.; Dias, L.; Castro Henriques, A.; Cabrita, A. Effect of Different Sensitization Events on HLA Alloimmunization in Kidney Transplantation Candidates. Transplant. Proc. 2015, 47, 894–897. [Google Scholar] [CrossRef]
- Phillips, B.L.; Callaghan, C. The Immunology of Organ Transplantation. Surgery 2017, 35, 333–340. [Google Scholar] [CrossRef]
- Stephen, R. Knight Ala Alasadi Marc Clancy The Immunology of Solid Organ Transplantation. Anaesth. Intensive Care Med. 2018, 19, 579–582. [Google Scholar] [CrossRef]
- Puttarajappa, C.; Shapiro, R.; Tan, H.P. Antibody-Mediated Rejection in Kidney Transplantation: A Review. J. Transplant. 2012, 2012, 193724. [Google Scholar] [CrossRef] [Green Version]
- Loupy, A.; Lefaucheur, C.; Vernerey, D.; Prugger, C.; van Huyen, J.-P.D.; Mooney, N.; Suberbielle, C.; Frémeaux-Bacchi, V.; Méjean, A.; Desgrandchamps, F.; et al. Complement-Binding Anti-HLA Antibodies and Kidney-Allograft Survival. N. Engl. J. Med. 2013, 369, 1215–1226. [Google Scholar] [CrossRef] [Green Version]
- Prieto, F.; Cabañas, C.; Villagra, V. Monitoreo de Anticuerpos Anti-HLA En Pacientes Con Insuficiencia Renal Crónica En Lista de Espera Para Trasplante. Rev. Nefrol. Diálisis Y Traspl. 2016, 36, 75–81. [Google Scholar]
- Greenspan, N.S.; Cavacini, L.A. Immunoglobulin Function. In Clinical Immunology: Principles and Practice; Elsevier Ltd.: Amsterdam, The Netherlands, 2019; pp. 223–233.e1. ISBN 978-0-7020-6896-6. [Google Scholar]
- Abbas, A.K.; Lichtman, A.H.; Pillai, S.; Baker, D.L.; Baker, A. B Cell Activation and Antibody Production. In Cellular and Molecular Immunology; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Lee, H.; Han, E.; Choi, A.R.; Ban, T.H.; Chung, B.H.; Yang, C.W.; Choi, Y.J.; Ohi, E.J. Clinical Impact of Complement (C1q, C3d) Binding de Novo Donor-Specific HLA Antibody in Kidney Transplant Recipients. PLoS ONE 2018, 13, e0207434. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castelao, A.; Górriz, J.L.; Bover, J.; Segura-De La Morena, J.; Cebollada, J.; Escalada, J.; Esmatjes, E.; Fácila, L.; Gamarra, J.; Gràcia, S.; et al. Documento de Consenso Para La Detección y Manejo de La Enfermedad Renal Crónica. Rev. Nefrol. Órgano Of. La Soc. Española Nefrol. 2014, 34, 243–262. [Google Scholar] [CrossRef]
- One Lambda, I. Product Insert: LABScreen. 2016. Available online: https://www.veritastk.co.jp/products/pdf/E-OLI-LABScreen.pdf (accessed on 20 May 2019).
- One Lambda. Antibody Mediated Rejection in Organ Transplantation. 2018. Available online: https://www.thermofisher.com/onelambda/us/en/products/_jcr_content.download?document_number=TDX-MKT-0039 (accessed on 20 May 2019).
- Zecher, D.; Bach, C.; Preiss, A.; Staudner, C.; Utpatel, K.; Evert, M.; Jung, B.; Bergler, T.; Böger, C.A.; Spriewald, B.M.; et al. Analysis of Luminex-Based Algorithms to Define Unacceptable HLA Antibodies in CDC-Crossmatch Negative Kidney Transplant Recipients. Transplantation 2018, 102, 969–977. [Google Scholar] [CrossRef]
- Thurman, J.M.; Panzer, S.E.; Quintrec, M. Le The Role of Complement in Antibody Mediated Transplant Rejection. Mol. Immunol. 2019, 112, 240–246. [Google Scholar] [CrossRef]
- Zhang, R. Donor-Specific Antibodies in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2018, 13, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Malheiro, J.; Tafulo, S.; Dias, L.; Martins, L.S.; Fonseca, I.; Beirão, I.; Castro-Henriques, A.; Cabrita, A. Determining Donor-Specific Antibody C1q-Binding Ability Improves the Prediction of Antibody-Mediated Rejection in Human Leucocyte Antigen-Incompatible Kidney Transplantation. Transpl. Int. 2017, 30, 347–359. [Google Scholar] [CrossRef]
- Wehmeier, C.; Amico, P.; Sidler, D.; Wirthmüller, U.; Hadaya, K.; Ferrari-Lacraz, S.; Golshayan, D.; Aubert, V.; Schnyder, A.; Sunic, K.; et al. Pre-Transplant Donor-Specific HLA Antibodies and Risk for Poor First-Year Renal Transplant Outcomes: Results from the Swiss Transplant Cohort Study. Transpl. Int. 2021, 34, 2755–2768. [Google Scholar] [CrossRef]
- Crespo, M.; Torio, A.; Mas, V.; Redondo, D.; Pérez-Sáez, M.J.; Mir, M.; Faura, A.; Guerra, R.; Montes-Ares, O.; Checa, M.D.; et al. Clinical Relevance of Pretransplant Anti-HLA Donor-Specific Antibodies: Does C1q-Fixation Matter? Transpl. Immunol. 2013, 29, 28–33. [Google Scholar] [CrossRef]
- Aubert, O.; Loupy, A.; Hidalgo, L.; Duong van Huyen, J.-P.; Higgins, S.; Viglietti, D.; Jouven, X.; Glotz, D.; Legendre, C.; Lefaucheur, C.; et al. Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients. J. Am. Soc. Nephrol. 2017, 28, 1912–1923. [Google Scholar] [CrossRef] [Green Version]
- Tyan, D.B. Application, Technical Issues, and Interpretation of C1q for Graft Outcome. Curr. Opin. Organ Transplant. 2017, 22, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Itabashi, Y.; Aikawa, A.; Muramatsu, M.; Hyoudou, Y.; Shinoda, K.; Takahashi, Y.; Sakurabayashi, K.; Mizutani, T.; Oguchi, H.; Arai, T.; et al. Living-Donor Kidney Transplant With Preformed Donor-Specific Antibodies. Exp. Clin. Transplant. 2019, 17, 43–49. [Google Scholar] [CrossRef]
- Gebel, H.M.; Bray, R.A.; Nickerson, P. Pre-Transplant Assessment of Donor-Reactive, HLA-Specific Antibodies in Renal Transplantation: Contraindication vs. Risk. Am. J. Transplant. 2003, 3, 1488–1500. [Google Scholar] [CrossRef]
- Loupy, A.; Lefaucheur, C. Antibody-Mediated Rejection of Solid-Organ Allografts. N. Engl. J. Med. 2018, 379, 1150–1160. [Google Scholar] [CrossRef]
- Zeevi, A.; Lunz, J.; Feingold, B.; Shullo, M.; Bermudez, C.; Teuteberg, J.; Webber, S. Persistent Strong Anti-HLA Antibody at High Titer Is Complement Binding and Associated with Increased Risk of Antibody-Mediated Rejection in Heart Transplant Recipients. J. Heart Lung Transplant. 2013, 32, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Llorente, S.; Boix, F.; Eguia, J.; López, M.; Bosch, A.; Martinez, H.; Gonzalez, M.J.; López-Hernández, R.; Salgado, G.; Moya-Quiles, M.R.; et al. C1q-Fixing Human Leukocyte Antigen Assay in Immunized Renal Patients: Correlation between Luminex SAB-C1q and SAB-IgG. Transplant. Proc. 2012, 44, 2535–2537. [Google Scholar] [CrossRef]
- Lan, J.H.; Tinckam, K. Clinical Utility of Complement Dependent Assays in Kidney Transplantation. Transplantation 2018, 102, S14–S22. [Google Scholar] [CrossRef]
- Wiebe, C.; Gareau, A.J.; Pochinco, D.; Gibson, I.W.; Ho, J.; Birk, P.E.; Blydt-Hansen, T.; Karpinski, M.; Goldberg, A.; Storsley, L.; et al. Evaluation of C1q Status and Titer of de novo Donor-Specific Antibodies as Predictors of Allograft Survival. Am. J. Transplant. 2017, 17, 703–711. [Google Scholar] [CrossRef]
- Yell, M.; Muth, B.L.; Kaufman, D.B.; Djamali, A.; Ellis, T.M. C1q Binding Activity of De Novo Donor-Specific HLA Antibodies in Renal Transplant Recipients With and Without Antibody-Mediated Rejection. Transplantation 2015, 99, 1151–1155. [Google Scholar] [CrossRef]
- Visentin, J.; Vigata, M.; Daburon, S.; Contin-Bordes, C.; Fremeaux-Bacchi, V.; Dromer, C.; Billes, M.-A.; Neau-Cransac, M.; Guidicelli, G.; Taupin, J.-L. Deciphering Complement Interference in Anti-Human Leukocyte Antigen Antibody Detection with Flow Beads Assays. Transplantation 2014, 98, 625–631. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Viglietti, D.; Hidalgo, L.G.; Ratner, L.E.; Bagnasco, S.M.; Batal, I.; Aubert, O.; Orandi, B.J.; Oppenheimer, F.; Bestard, O.; et al. Complement-Activating Anti-HLA Antibodies in Kidney Transplantation: Allograft Gene Expression Profiling and Response to Treatment. J. Am. Soc. Nephrol. 2018, 29, 620–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arreola-Guerra, J.M.; Morales-Buenrostro, L.E.; Granados, J.; Castelán, N.; de Santiago, A.; Arvizu, A.; Gonzalez-Tableros, N.; López, M.; Vilatobá, M.; Alberú, J. Anti-HLA-DQ Antibodies Are Highly and Independently Related to the C1q-Binding Capacity of HLA Antibodies. Transpl. Immunol. 2017, 41, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Freitas, M.C.S.; Rebellato, L.M.; Ozawa, M.; Nguyen, A.; Sasaki, N.; Everly, M.; Briley, K.P.; Haisch, C.E.; Bolin, P.; Parker, K.; et al. The Role of Immunoglobulin-G Subclasses and C1q in de Novo HLA-DQ Donor-Specific Antibody Kidney Transplantation Outcomes. Transplantation 2013, 95, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Willicombe, M.; Brookes, P.; Sergeant, R.; Santos-Nunez, E.; Steggar, C.; Galliford, J.; McLean, A.; Cook, T.H.; Cairns, T.; Roufosse, C.; et al. De Novo DQ Donor-Specific Antibodies Are Associated with a Significant Risk of Antibody-Mediated Rejection and Transplant Glomerulopathy. Transplantation 2012, 94, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Devos, J.M.; Gaber, A.O.; Knight, R.J.; Land, G.A.; Suki, W.N.; Gaber, L.W.; Patel, S.J. Donor-Specific HLA-DQ Antibodies May Contribute to Poor Graft Outcome after Renal Transplantation. Kidney Int. 2012, 82, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Iniotaki-Theodoraki, A.G.; Boletis, J.N.; Trigas, G.C.; Kalogeropoulou, H.G.; Kostakis, A.G.; Stavropoulos-Giokas, C.G. Humoral Immune Reactivity against Human Leukocyte Antigen (HLA)-DQ Graft Molecules in the Early Posttransplantation Period. Transplantation 2003, 75, 1601–1603. [Google Scholar] [CrossRef]
- Tambur, A.R.; Kosmoliaptsis, V.; Claas, F.H.J.; Mannon, R.B.; Nickerson, P.; Naesens, M. Significance of HLA-DQ in Kidney Transplantation: Time to Reevaluate Human Leukocyte Antigen–Matching Priorities to Improve Transplant Outcomes? An Expert Review and Recommendations. Kidney Int. 2021, 100, 1012–1022. [Google Scholar] [CrossRef]
- Okabe, Y.; Noguchi, H.; Miyamoto, K.; Kaku, K.; Tsuchimoto, A.; Masutani, K.; Nakamura, M. Preformed C1q-Binding Donor-Specific Anti-HLA Antibodies and Graft Function After Kidney Transplantation. Transplant. Proc. 2018, 50, 3460–3466. [Google Scholar] [CrossRef]





| Features | Total Patients | No DSA | DSA | |
|---|---|---|---|---|
| Non-Complement Fixers | Complement Fixers | |||
| Recipient | 245 | 219 | 17 | 9 |
| Age | 53.9 ± 12.4 | 54.2 ± 12.4 | 55.0 ± 11.9 | 46.1 ± 10.9 |
| Sex | 174 men | 158 men | 11 men | 5 men |
| 71 women | 61 women | 6 women | 4 women | |
| Donors | ||||
| Age * | 50.4 ± 14.7 | 51.2 ± 14.5 | 43.3 ± 16.7 | 46.0 ± 13.3 |
| Sex * | 166 men | 147 men | 12 men | 7 men |
| 68 women | 61 women | 5 women | 2 women | |
| Type of Donors | 233 deceased | 207 deceased | 17 deceased | 9 deceased |
| 12 alive | 12 alive | 0 alive | 0 alive | |
| Immunological data | ||||
| HLA Incompatibilities | 4.6 ± 1.1 | 4.6 ± 1.1 | 4.5 ± 1.5 | 4.5 ± 1.1 |
| Blood Group Recipient | ||||
| A | 105 | 98 | 7 | 0 |
| B | 30 | 30 | 0 | 0 |
| AB | 6 | 5 | 0 | 1 |
| 0 | 104 | 86 | 10 | 8 |
| dnDSA | ||||
| HLA class I | 9 | - | 8 | 1 |
| HLA class II | 11 | - | 7 | 4 |
| HLA class I and II | 6 | - | 2 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Herrera, C.M.; Gutiérrez-Bautista, J.F.; López-Nevot, M.Á. Complement Binding Anti-HLA Antibodies and the Survival of Kidney Transplantation. J. Clin. Med. 2023, 12, 2335. https://doi.org/10.3390/jcm12062335
Muñoz-Herrera CM, Gutiérrez-Bautista JF, López-Nevot MÁ. Complement Binding Anti-HLA Antibodies and the Survival of Kidney Transplantation. Journal of Clinical Medicine. 2023; 12(6):2335. https://doi.org/10.3390/jcm12062335
Chicago/Turabian StyleMuñoz-Herrera, Claudia M., Juan Francisco Gutiérrez-Bautista, and Miguel Ángel López-Nevot. 2023. "Complement Binding Anti-HLA Antibodies and the Survival of Kidney Transplantation" Journal of Clinical Medicine 12, no. 6: 2335. https://doi.org/10.3390/jcm12062335