
Aortic Stiffness: A Major Risk Factor for Multimorbidity in the Elderly
 , , , , and
, , , , and 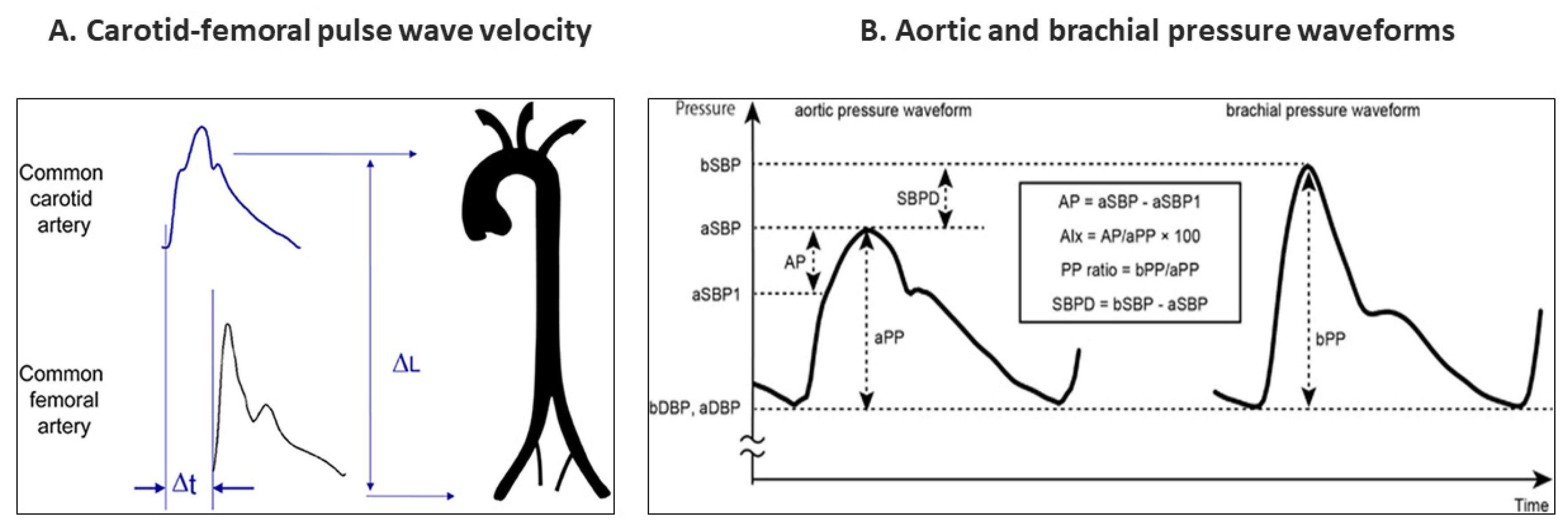{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The Normal Young Aorta
3. The Aging Aorta
3.1. Biology
3.2. Stiffness
4. Cardiovascular Disorders
4.1. Hypertension
4.2. Atrial Fibrillation
4.3. Ischemic Heart Disease
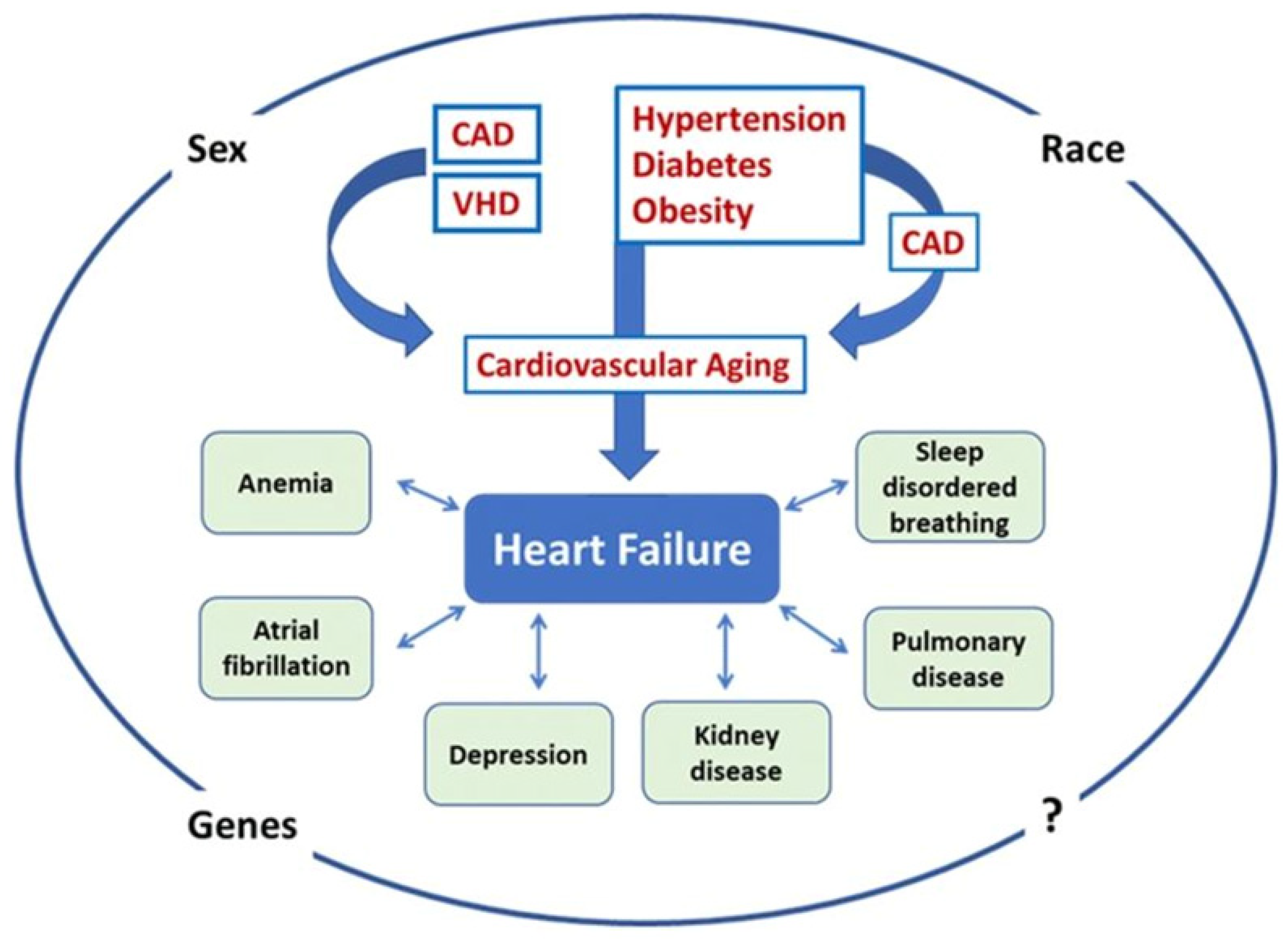
4.4. Heart Failure
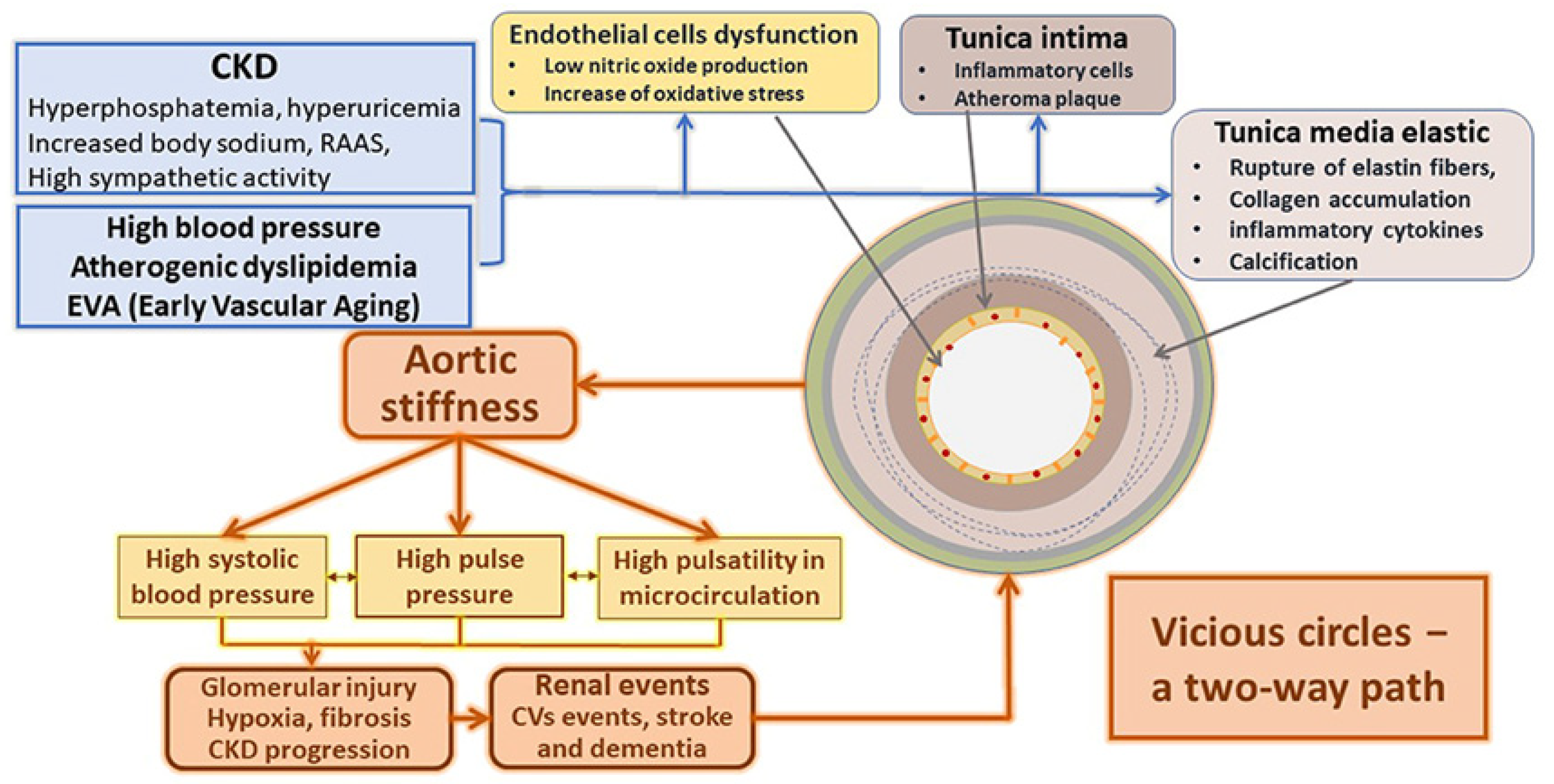
5. Chronic Kidney Disease
6. Anemia
7. Ischemic Stroke
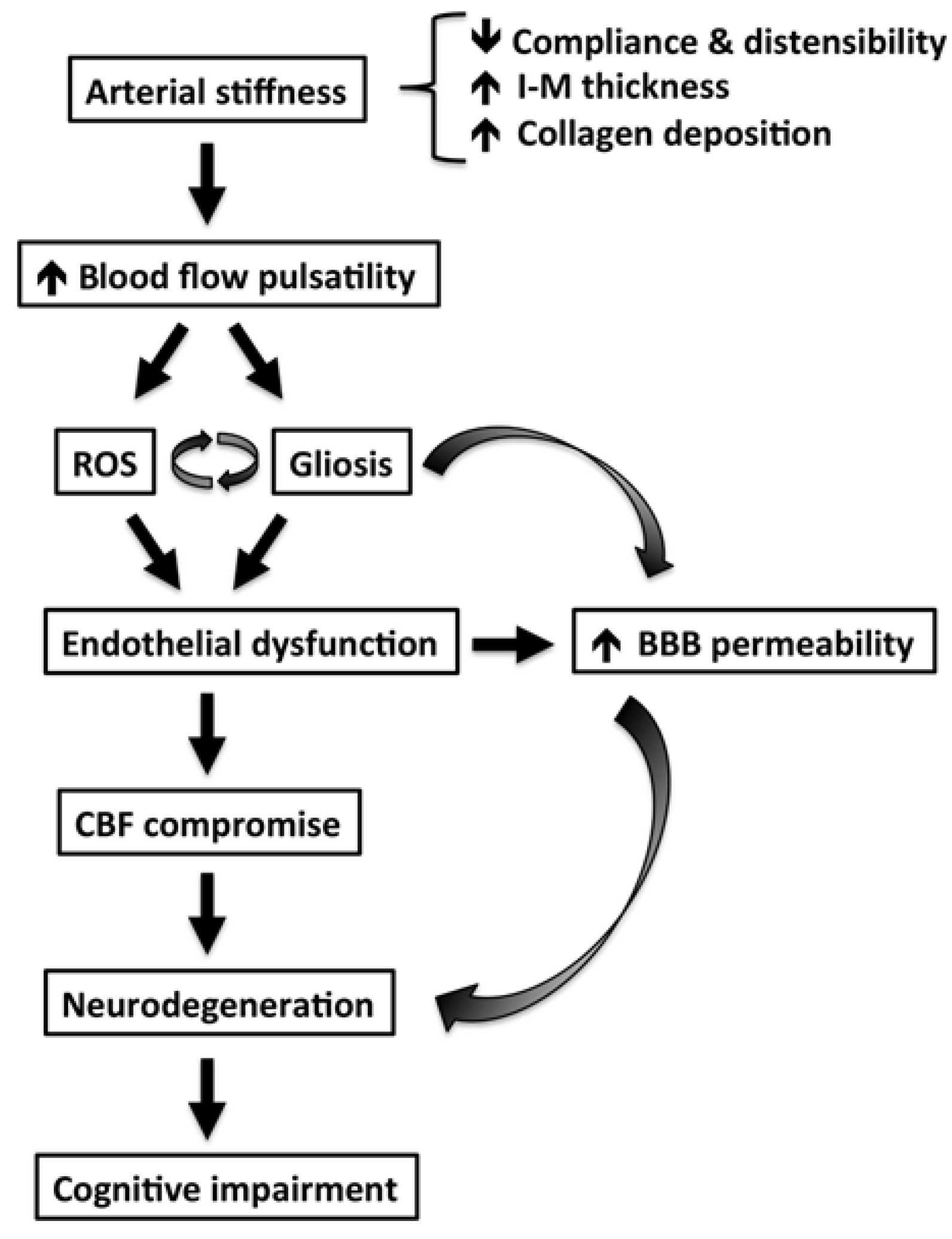
8. Dementia
9. Frailty
10. Degenerative Aortic Stenosis
11. Determinants of Multimorbidity Pattern in the Elderly
12. Clinical Implications
13. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnston, M.C.; Crilly, M.; Black, C.; Prescott, G.J.; Mercer, S.W. Defining and measuring multimorbidity: A systematic review of systematic reviews. Eur. J. Public Health 2019, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Pearson-Stuttard, J.; Ezzati, M.; Gregg, E.W. Multimorbidity-a defining challenge for health systems. Lancet Public Health 2019, 4, e599–e600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triposkiadis, F.; Xanthopoulos, A.; Butler, J. Cardiovascular Aging and Heart Failure: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 804–813. [Google Scholar] [CrossRef]
- Rodrigues, L.P.; de Oliveira Rezende, A.T.; Delpino, F.M.; Mendonca, C.R.; Noll, M.; Nunes, B.P.; de Oliviera, C.; Silveira, E.A. Association between multimorbidity and hospitalization in older adults: Systematic review and meta-analysis. Age Ageing 2022, 51, afac155. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Pan, S.; Xanthakis, V.; Beiser, A.; Larson, M.G.; Seshadri, S.; Mitchell, G.F. Arterial Stiffness and Long-Term Risk of Health Outcomes: The Framingham Heart Study. Hypertension 2022, 79, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [Green Version]
- Boudoulas, K.D.; Vlachopoulos, C.; Raman, S.V.; Sparks, E.A.; Triposciadis, F.; Stefanadis, C.; Boudoulas, H. Aortic function: From the research laboratory to the clinic. Cardiology 2012, 121, 31–42. [Google Scholar] [CrossRef]
- Fukamachi, K.; Horvath, D.J.; Karimov, J.H.; Kado, Y.; Miyamoto, T.; Kuban, B.D.; Starling, R.C. Left atrial assist device to treat patients with heart failure with preserved ejection fraction: Initial in vitro study. J. Thorac. Cardiovasc. Surg. 2021, 162, 120–126. [Google Scholar] [CrossRef]
- Lacolley, P.; Regnault, V.; Segers, P.; Laurent, S. Vascular Smooth Muscle Cells and Arterial Stiffening: Relevance in Development, Aging, and Disease. Physiol. Rev. 2017, 97, 1555–1617. [Google Scholar] [CrossRef]
- Briet, M.; Boutouyrie, P.; Laurent, S.; London, G.M. Arterial stiffness and pulse pressure in CKD and ESRD. Kidney Int. 2012, 82, 388–400. [Google Scholar] [CrossRef] [Green Version]
- Belz, G.G. Elastic properties and Windkessel function of the human aorta. Cardiovasc. Drugs Ther. 1995, 9, 73–83. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; Maki-Petaja, K.M.; Mitchell, G.F. Uses of Arterial Stiffness in Clinical Practice. Arter. Thromb. Vasc. Biol. 2020, 40, 1063–1067. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segers, P.; Rietzschel, E.R.; Chirinos, J.A. How to Measure Arterial Stiffness in Humans. Arter. Thromb. Vasc. Biol. 2020, 40, 1034–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagomi, A.; Shoji, T.; Okada, S.; Ohno, Y.; Kobayashi, Y. Validity of the augmentation index and pulse pressure amplification as determined by the SphygmoCor XCEL device: A comparison with invasive measurements. Hypertens. Res. 2018, 41, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Ito, H. Arterial stiffness in health and disease: The role of cardio-ankle vascular index. J. Cardiol. 2021, 78, 493–501. [Google Scholar] [CrossRef] [PubMed]
- McGaughey, T.J.; Fletcher, E.A.; Shah, S.A. Impact of Antihypertensive Agents on Central Systolic Blood Pressure and Augmentation Index: A Meta-Analysis. Am. J. Hypertens. 2016, 29, 448–457. [Google Scholar] [CrossRef]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef] [Green Version]
- Mehdizadeh, M.; Aguilar, M.; Thorin, E.; Ferbeyre, G.; Nattel, S. The role of cellular senescence in cardiac disease: Basic biology and clinical relevance. Nat. Rev. Cardiol. 2022, 19, 250–264. [Google Scholar] [CrossRef]
- Schmauck-Medina, T.; Moliere, A.; Lautrup, S.; Zhang, J.; Chlopicki, S.; Madsen, H.B.; Cao, S.; Soendenbroe, C.; Mansell, E.; Vestergaard, M.B.; et al. New hallmarks of ageing: A 2022 Copenhagen ageing meeting summary. Aging 2022, 14, 6829–6839. [Google Scholar] [CrossRef] [PubMed]
- Zanoli, L.; Briet, M.; Empana, J.P.; Cunha, P.G.; Maki-Petaja, K.M.; Protogerou, A.D.; Tedgui, A.; Touyz, R.M.; Schiffrin, E.L.; Spronck, B.; et al. Vascular consequences of inflammation: A position statement from the ESH Working Group on Vascular Structure and Function and the ARTERY Society. J. Hypertens. 2020, 38, 1682–1698. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, M.F.; Safar, M.E.; Dzau, V. The Cardiovascular Continuum extended: Aging effects on the aorta and microvasculature. Vasc. Med. 2010, 15, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Mammoto, A.; Matus, K.; Mammoto, T. Extracellular Matrix in Aging Aorta. Front. Cell Dev. Biol. 2022, 10, 822561. [Google Scholar] [CrossRef] [PubMed]
- Angoff, R.; Mosarla, R.C.; Tsao, C.W. Aortic Stiffness: Epidemiology, Risk Factors, and Relevant Biomarkers. Front. Cardiovasc. Med. 2021, 8, 709396. [Google Scholar] [CrossRef]
- Mitchell, G.F. Arterial Stiffness in Aging: Does It Have a Place in Clinical Practice?: Recent Advances in Hypertension. Hypertension 2021, 77, 768–780. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.W.; O’Rourke, M.F.; Avolio, A.P.; Yaginuma, T.; Murgo, J.P.; Pepine, C.J.; Conti, C.R. Effects of age on ventricular-vascular coupling. Am. J. Cardiol. 1985, 55, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Wang, N.; Palmisano, J.N.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S. Hemodynamic correlates of blood pressure across the adult age spectrum: Noninvasive evaluation in the Framingham Heart Study. Circulation 2010, 122, 1379–1386. [Google Scholar] [CrossRef] [Green Version]
- Burt, V.L.; Whelton, P.; Roccella, E.J.; Brown, C.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995, 25, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Franklin, S.S.; Gustin, W.t.; Wong, N.D.; Larson, M.G.; Weber, M.A.; Kannel, W.B.; Levy, D. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997, 96, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Pierce, G.L.; Coutinho, T.A.; DuBose, L.E.; Donato, A.J. Is It Good to Have a Stiff Aorta with Aging? Causes and Consequences. Physiology 2022, 37, 154–173. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A.; Segers, P.; Hughes, T.; Townsend, R. Large-Artery Stiffness in Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1237–1263. [Google Scholar] [CrossRef] [PubMed]
- Corda, A.; Corda, F.; Caivano, D.; Saderi, L.; Sotgiu, G.; Mollica, A.; Birettoni, F.; Porciello, F.; Pinna Parpaglia, M.L. Ultrasonographic assessment of abdominal aortic elasticity in hypertensive dogs. J. Vet. Intern. Med. 2020, 34, 2337–2344. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F. Arterial stiffness and hypertension: Chicken or egg? Hypertension 2014, 64, 210–214. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.F.; Guo, C.Y.; Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Vita, J.A.; Vasan, R.S.; Levy, D. Cross-sectional correlates of increased aortic stiffness in the community: The Framingham Heart Study. Circulation 2007, 115, 2628–2636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaess, B.M.; Rong, J.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA 2012, 308, 875–881. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P. The structural factor of hypertension: Large and small artery alterations. Circ. Res. 2015, 116, 1007–1021. [Google Scholar] [CrossRef]
- Olsen, M.H.; Angell, S.Y.; Asma, S.; Boutouyrie, P.; Burger, D.; Chirinos, J.A.; Damasceno, A.; Delles, C.; Gimenez-Roqueplo, A.P.; Hering, D.; et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: The Lancet Commission on hypertension. Lancet 2016, 388, 2665–2712. [Google Scholar] [CrossRef]
- Cardoso, C.R.L.; Salles, G.F. Prognostic Value of Changes in Aortic Stiffness for Cardiovascular Outcomes and Mortality in Resistant Hypertension: A Cohort Study. Hypertension 2022, 79, 447–456. [Google Scholar] [CrossRef]
- Ma, B.; Melton, E.; Wiener, R.; Zhou, N.; Wu, W.; Lai, L.; Wang, C.; Costa, K.D.; Qiu, H. Age and Blood Pressure Contribute to Aortic Cell and Tissue Stiffness Through Distinct Mechanisms. Hypertension 2022, 79, 1777–1788. [Google Scholar] [CrossRef]
- Verdecchia, P.; Angeli, F.; Reboldi, G. Hypertension and Atrial Fibrillation: Doubts and Certainties From Basic and Clinical Studies. Circ. Res. 2018, 122, 352–368. [Google Scholar] [CrossRef] [PubMed]
- Gumprecht, J.; Domek, M.; Lip, G.Y.H.; Shantsila, A. Invited review: Hypertension and atrial fibrillation: Epidemiology, pathophysiology, and implications for management. J. Hum. Hypertens. 2019, 33, 824–836. [Google Scholar] [CrossRef] [PubMed]
- Roetker, N.S.; Chen, L.Y.; Heckbert, S.R.; Nazarian, S.; Soliman, E.Z.; Bluemke, D.A.; Lima, J.A.; Alonso, A. Relation of systolic, diastolic, and pulse pressures and aortic distensibility with atrial fibrillation (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2014, 114, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, Y.; Nakanishi, K.; Daimon, M.; Ishiwata, J.; Sawada, N.; Hirokawa, M.; Kaneko, H.; Nakao, T.; Mizuno, Y.; Morita, H.; et al. Association of arterial stiffness with left atrial structure and phasic function: A community-based cohort study. J. Hypertens. 2020, 38, 1140–1148. [Google Scholar] [CrossRef]
- Vio, R.; Giordani, A.S.; Stefil, M.; Madine, J.; Fairbairn, T.; Themistoclakis, S.; Salvi, P.; Caforio, A.L.P.; Shantsila, A.; Shantsila, E.; et al. Arterial stiffness and atrial fibrillation: Shared mechanisms, clinical implications and therapeutic options. J. Hypertens. 2022, 40, 1639–1646. [Google Scholar] [CrossRef]
- Izuhara, M.; Shioji, K.; Kadota, S.; Baba, O.; Takeuchi, Y.; Uegaito, T.; Mutsuo, S.; Matsuda, M. Relationship of cardio-ankle vascular index (CAVI) to carotid and coronary arteriosclerosis. Circ. J. 2008, 72, 1762–1767. [Google Scholar] [CrossRef] [Green Version]
- Park, J.B.; Park, H.E.; Choi, S.Y.; Kim, M.K.; Oh, B.H. Relation between cardio-ankle vascular index and coronary artery calcification or stenosis in asymptomatic subjects. J. Atheroscler. Thromb. 2013, 20, 557–567. [Google Scholar] [CrossRef] [Green Version]
- Birudaraju, D.; Cherukuri, L.; Kinninger, A.; Chaganti, B.T.; Haroun, P.; Pidikiti, S.; Lakshmanan, S.; Hamal, S.; Flores, F.; Dailing, C.; et al. Relationship between cardio-ankle vascular index and obstructive coronary artery disease. Coron. Artery Dis. 2020, 31, 550–555. [Google Scholar] [CrossRef]
- Lonnebakken, M.T.; Eskerud, I.; Larsen, T.H.; Midtbo, H.B.; Kokorina, M.V.; Gerdts, E. Impact of aortic stiffness on myocardial ischaemia in non-obstructive coronary artery disease. Open Heart 2019, 6, e000981. [Google Scholar] [CrossRef] [Green Version]
- Frak, W.; Wojtasinska, A.; Lisinska, W.; Mlynarska, E.; Franczyk, B.; Rysz, J. Pathophysiology of Cardiovascular Diseases: New Insights into Molecular Mechanisms of Atherosclerosis, Arterial Hypertension, and Coronary Artery Disease. Biomedicines 2022, 10, 1938. [Google Scholar] [CrossRef]
- Kim, H.-L. Arterial stiffness and coronary artery disease. EMJ Cardiol. 2016, 4, 84–89. [Google Scholar] [CrossRef]
- Medina-Leyte, D.J.; Zepeda-Garcia, O.; Dominguez-Perez, M.; Gonzalez-Garrido, A.; Villarreal-Molina, T.; Jacobo-Albavera, L. Endothelial Dysfunction, Inflammation and Coronary Artery Disease: Potential Biomarkers and Promising Therapeutical Approaches. Int. J. Mol. Sci. 2021, 22, 3850. [Google Scholar] [CrossRef]
- Back, M.; Yurdagul, A., Jr.; Tabas, I.; Oorni, K.; Kovanen, P.T. Inflammation and its resolution in atherosclerosis: Mediators and therapeutic opportunities. Nat. Rev. Cardiol. 2019, 16, 389–406. [Google Scholar] [CrossRef] [PubMed]
- Haider, A.W.; Larson, M.G.; Franklin, S.S.; Levy, D.; Framingham Heart, S. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann. Intern. Med. 2003, 138, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.U.; Pfeffer, M.A.; Glynn, R.J.; Mitchell, G.F.; Taylor, J.O.; Hennekens, C.H. Increased pulse pressure and risk of heart failure in the elderly. JAMA 1999, 281, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A.; Kips, J.G.; Jacobs, D.R., Jr.; Brumback, L.; Duprez, D.A.; Kronmal, R.; Bluemke, D.A.; Townsend, R.R.; Vermeersch, S.; Segers, P. Arterial wave reflections and incident cardiovascular events and heart failure: MESA (Multiethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2012, 60, 2170–2177. [Google Scholar] [CrossRef]
- Tsao, C.W.; Lyass, A.; Larson, M.G.; Levy, D.; Hamburg, N.M.; Vita, J.A.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Relation of Central Arterial Stiffness to Incident Heart Failure in the Community. J. Am. Heart Assoc. 2015, 4, 2189. [Google Scholar] [CrossRef] [Green Version]
- Chirinos, J.A.; Khan, A.; Bansal, N.; Dries, D.L.; Feldman, H.I.; Ford, V.; Anderson, A.H.; Kallem, R.; Lash, J.P.; Ojo, A.; et al. Arterial stiffness, central pressures, and incident hospitalized heart failure in the chronic renal insufficiency cohort study. Circ. Heart Fail. 2014, 7, 709–716. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A.; Khan, H.; Newman, A.B.; Lakatta, E.G.; Forman, D.E.; Butler, J.; Berry, J.D. Arterial Stiffness and Risk of Overall Heart Failure, Heart Failure With Preserved Ejection Fraction, and Heart Failure With Reduced Ejection Fraction: The Health ABC Study (Health, Aging, and Body Composition). Hypertension 2017, 69, 267–274. [Google Scholar] [CrossRef]
- Aisu, H.; Saito, M.; Inaba, S.; Morofuji, T.; Takahashi, K.; Sumimoto, T.; Okura, T.; Higaki, J. Association of worsening arterial stiffness with incident heart failure in asymptomatic patients with cardiovascular risk factors. Hypertens. Res. 2017, 40, 173–180. [Google Scholar] [CrossRef]
- Watanabe, K.; Yoshihisa, A.; Sato, Y.; Hotsuki, Y.; Anzai, F.; Ichijo, Y.; Kimishima, Y.; Yokokawa, T.; Misaka, T.; Sato, T.; et al. Cardio-Ankle Vascular Index Reflects Impaired Exercise Capacity and Predicts Adverse Prognosis in Patients With Heart Failure. Front. Cardiovasc. Med. 2021, 8, 631807. [Google Scholar] [CrossRef] [PubMed]
- Triposkiadis, F.; Xanthopoulos, A.; Parissis, J.; Butler, J.; Farmakis, D. Pathogenesis of chronic heart failure: Cardiovascular aging, risk factors, comorbidities, and disease modifiers. Heart Fail. Rev. 2022, 27, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Chirinos, J.A. Pulsatile arterial haemodynamics in heart failure. Eur. Heart J. 2018, 39, 3847–3854. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.L.; Zambanini, A.; Mayet, J.; Mc, G.T.S.A.; Foale, R.; Parker, K.H.; Hughes, A.D. Reduced systolic wave generation and increased peripheral wave reflection in chronic heart failure. Am. J. Physiol. Circ. Physiol. 2007, 293, H557–H562. [Google Scholar] [CrossRef] [Green Version]
- Lazzeroni, D.; Villatore, A.; Souryal, G.; Pili, G.; Peretto, G. The Aging Heart: A Molecular and Clinical Challenge. Int. J. Mol. Sci. 2022, 23, 16033. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.E.; Ahmed, A.; Fleg, J.L. Heart failure in very old adults. Curr. Heart Fail. Rep. 2013, 10, 387–400. [Google Scholar] [CrossRef]
- Bidani, A.K.; Griffin, K.A.; Williamson, G.; Wang, X.; Loutzenhiser, R. Protective importance of the myogenic response in the renal circulation. Hypertension 2009, 54, 393–398. [Google Scholar] [CrossRef]
- Mitchell, G.F. Aortic stiffness, pressure and flow pulsatility, and target organ damage. J. Appl. Physiol. (1985) 2018, 125, 1871–1880. [Google Scholar] [CrossRef]
- Christensen, P.K.; Hansen, H.P.; Parving, H.H. Impaired autoregulation of GFR in hypertensive non-insulin dependent diabetic patients. Kidney Int. 1997, 52, 1369–1374. [Google Scholar] [CrossRef] [Green Version]
- Hill, G.S.; Heudes, D.; Bariety, J. Morphometric study of arterioles and glomeruli in the aging kidney suggests focal loss of autoregulation. Kidney Int. 2003, 63, 1027–1036. [Google Scholar] [CrossRef] [Green Version]
- Georgianos, P.I.; Sarafidis, P.A.; Liakopoulos, V. Arterial Stiffness: A Novel Risk Factor for Kidney Injury Progression? Am. J. Hypertens. 2015, 28, 958–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedaghat, S.; Mattace-Raso, F.U.; Hoorn, E.J.; Uitterlinden, A.G.; Hofman, A.; Ikram, M.A.; Franco, O.H.; Dehghan, A. Arterial Stiffness and Decline in Kidney Function. Clin. J. Am. Soc. Nephrol. 2015, 10, 2190–2197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Varik, B.J.; Vossen, L.M.; Rennenberg, R.J.; Stoffers, H.E.; Kessels, A.G.; de Leeuw, P.W.; Kroon, A.A. Arterial stiffness and decline of renal function in a primary care population. Hypertens. Res. 2017, 40, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Denic, A.; Rule, A.D.; Glassock, R.J. Healthy and unhealthy aging on kidney structure and function: Human studies. Curr. Opin. Nephrol. Hypertens. 2022, 31, 228–234. [Google Scholar] [CrossRef]
- Townsend, R.R.; Anderson, A.H.; Chirinos, J.A.; Feldman, H.I.; Grunwald, J.E.; Nessel, L.; Roy, J.; Weir, M.R.; Wright, J.T., Jr.; Bansal, N.; et al. Association of Pulse Wave Velocity With Chronic Kidney Disease Progression and Mortality: Findings From the CRIC Study (Chronic Renal Insufficiency Cohort). Hypertension 2018, 71, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Inserra, F.; Forcada, P.; Castellaro, A.; Castellaro, C. Chronic Kidney Disease and Arterial Stiffness: A Two-Way Path. Front. Med. 2021, 8, 765924. [Google Scholar] [CrossRef]
- Cannata-Andia, J.B.; Martin-Carro, B.; Martin-Virgala, J.; Rodriguez-Carrio, J.; Bande-Fernandez, J.J.; Alonso-Montes, C.; Carrillo-Lopez, N. Chronic Kidney Disease-Mineral and Bone Disorders: Pathogenesis and Management. Calcif. Tissue Int. 2021, 108, 410–422. [Google Scholar] [CrossRef]
- Rodriguez Garcia, M.; Naves Diaz, M.; Cannata Andia, J.B. Bone metabolism, vascular calcifications and mortality: Associations beyond mere coincidence. J. Nephrol. 2005, 18, 458–463. [Google Scholar]
- Rodriguez-Garcia, M.; Gomez-Alonso, C.; Naves-Diaz, M.; Diaz-Lopez, J.B.; Diaz-Corte, C.; Cannata-Andia, J.B.; Asturias Study, G. Vascular calcifications, vertebral fractures and mortality in haemodialysis patients. Nephrol. Dial. Transpl. 2009, 24, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Blacher, J.; Guerin, A.P.; Pannier, B.; Marchais, S.J.; Safar, M.E.; London, G.M. Impact of aortic stiffness on survival in end-stage renal disease. Circulation 1999, 99, 2434–2439. [Google Scholar] [CrossRef] [Green Version]
- Guerin, A.P.; Blacher, J.; Pannier, B.; Marchais, S.J.; Safar, M.E.; London, G.M. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation 2001, 103, 987–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarafidis, P.A.; Loutradis, C.; Karpetas, A.; Tzanis, G.; Piperidou, A.; Koutroumpas, G.; Raptis, V.; Syrgkanis, C.; Liakopoulos, V.; Efstratiadis, G.; et al. Ambulatory Pulse Wave Velocity Is a Stronger Predictor of Cardiovascular Events and All-Cause Mortality Than Office and Ambulatory Blood Pressure in Hemodialysis Patients. Hypertension 2017, 70, 148–157. [Google Scholar] [CrossRef]
- Sarafidis, P.A.; Loutradis, C.; Mayer, C.C.; Karpetas, A.; Pagkopoulou, E.; Bikos, A.; Faitatzidou, D.; Wassertheurer, S.; Schmaderer, C.; Liakopoulos, V.; et al. Weak within-individual association of blood pressure and pulse wave velocity in hemodialysis is related to adverse outcomes. J. Hypertens. 2019, 37, 2200–2208. [Google Scholar] [CrossRef] [PubMed]
- Bach, V.; Schruckmayer, G.; Sam, I.; Kemmler, G.; Stauder, R. Prevalence and possible causes of anemia in the elderly: A cross-sectional analysis of a large European university hospital cohort. Clin. Interv. Aging 2014, 9, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Stauder, R.; Valent, P.; Theurl, I. Anemia at older age: Etiologies, clinical implications, and management. Blood 2018, 131, 505–514. [Google Scholar] [CrossRef] [Green Version]
- Montero, D.; Diaz-Canestro, C.; Keiser, S.; Lundby, C. Arterial stiffness is strongly and negatively associated with the total volume of red blood cells. Int. J. Cardiol. 2016, 221, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Tiwaskar, M.; Kalra, S.; Bantwal, G.; Bhattacharya, A.; Sahay, M.; Jadhav, U.; Joshi, A.; Das, A.K.; Khullar, D.; Baruah, M.; et al. SGLT2-inhibition and Vascular Euphoria a Reconciliation of Vascular Health and Disease Homeostasis. J. Assoc. Physicians India 2021, 69, 11–12. [Google Scholar]
- Montero, D.; Diaz-Canestro, C.; Flammer, A.; Lundby, C. Unexplained Anemia in the Elderly: Potential Role of Arterial Stiffness. Front. Physiol. 2016, 7, 485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerna, C.; Thomalla, G.; Campbell, B.C.V.; Rha, J.H.; Hill, M.D. Current practice and future directions in the diagnosis and acute treatment of ischaemic stroke. Lancet 2018, 392, 1247–1256. [Google Scholar] [CrossRef]
- Laurent, S.; Katsahian, S.; Fassot, C.; Tropeano, A.I.; Gautier, I.; Laloux, B.; Boutouyrie, P. Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. Stroke 2003, 34, 1203–1206. [Google Scholar] [CrossRef] [Green Version]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.G.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.H.; Cruickshank, J.K.; et al. Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, Y.; Wang, Y.; Niu, W.; Zhang, Y.; Gao, P.; Zhang, L.; Lin, H.; Chen, K.; Zhu, D. Arterial stiffness and asymptomatic intracranial large arterial stenosis and calcification in hypertensive chinese. Am. J. Hypertens. 2011, 24, 304–309. [Google Scholar] [CrossRef] [Green Version]
- De Silva, D.A.; Woon, F.P.; Gan, H.Y.; Chen, C.P.; Chang, H.M.; Koh, T.H.; Kingwell, B.A.; Cameron, J.D.; Wong, M.C. Arterial stiffness is associated with intracranial large artery disease among ethnic Chinese and South Asian ischemic stroke patients. J. Hypertens. 2009, 27, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Shen, F.; Liu, J.; Yang, G.Y. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc. Neurol. 2017, 2, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fico, B.G.; Miller, K.B.; Rivera-Rivera, L.A.; Corkery, A.T.; Pearson, A.G.; Eisenmann, N.A.; Howery, A.J.; Rowley, H.A.; Johnson, K.M.; Johnson, S.C.; et al. The Impact of Aging on the Association Between Aortic Stiffness and Cerebral Pulsatility Index. Front. Cardiovasc. Med. 2022, 9, 821151. [Google Scholar] [CrossRef] [PubMed]
- Jaminon, A.; Reesink, K.; Kroon, A.; Schurgers, L. The Role of Vascular Smooth Muscle Cells in Arterial Remodeling: Focus on Calcification-Related Processes. Int. J. Mol. Sci. 2019, 20, 5694. [Google Scholar] [CrossRef] [Green Version]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Am Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); Am Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Decourt, B.; Noorda, K.; Noorda, K.; Shi, J.; Sabbagh, M.N. Review of Advanced Drug Trials Focusing on the Reduction of Brain Beta-Amyloid to Prevent and Treat Dementia. J. Exp. Pharm. 2022, 14, 331–352. [Google Scholar] [CrossRef]
- Niotis, K.; Akiyoshi, K.; Carlton, C.; Isaacson, R. Dementia Prevention in Clinical Practice. Semin. Neurol. 2022, 42, 525–548. [Google Scholar] [CrossRef]
- Biessels, G.J. Diagnosis and treatment of vascular damage in dementia. Biochim. Biophys. Acta. 2016, 1862, 869–877. [Google Scholar] [CrossRef]
- Kalaria, R.N. The pathology and pathophysiology of vascular dementia. Neuropharmacology 2018, 134, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Iulita, M.F.; Noriega de la Colina, A.; Girouard, H. Arterial stiffness, cognitive impairment and dementia: Confounding factor or real risk? J. Neurochem. 2018, 144, 527–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poels, M.M.; Zaccai, K.; Verwoert, G.C.; Vernooij, M.W.; Hofman, A.; van der Lugt, A.; Witteman, J.C.; Breteler, M.M.; Mattace-Raso, F.U.; Ikram, M.A. Arterial stiffness and cerebral small vessel disease: The Rotterdam Scan Study. Stroke 2012, 43, 2637–2642. [Google Scholar] [CrossRef] [Green Version]
- Zhai, F.F.; Ye, Y.C.; Chen, S.Y.; Ding, F.M.; Han, F.; Yang, X.L.; Wang, Q.; Zhou, L.X.; Ni, J.; Yao, M.; et al. Arterial Stiffness and Cerebral Small Vessel Disease. Front. Neurol. 2018, 9, 723. [Google Scholar] [CrossRef] [PubMed]
- Saji, N.; Toba, K.; Sakurai, T. Cerebral Small Vessel Disease and Arterial Stiffness: Tsunami Effect in the Brain? Pulse 2016, 3, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Hughes, T.M.; Kuller, L.H.; Barinas-Mitchell, E.J.; McDade, E.M.; Klunk, W.E.; Cohen, A.D.; Mathis, C.A.; Dekosky, S.T.; Price, J.C.; Lopez, O.L. Arterial stiffness and beta-amyloid progression in nondemented elderly adults. JAMA Neurol. 2014, 71, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Wong, A.; Au, L.; Yang, J.; Wang, Z.; Leung, E.Y.; Chen, S.; Ho, C.L.; Mok, V.C. Influence of Amyloid-beta on Cognitive Decline After Stroke/Transient Ischemic Attack: Three-Year Longitudinal Study. Stroke 2015, 46, 3074–3080. [Google Scholar] [CrossRef] [Green Version]
- Hughes, T.M.; Wagenknecht, L.E.; Craft, S.; Mintz, A.; Heiss, G.; Palta, P.; Wong, D.; Zhou, Y.; Knopman, D.; Mosley, T.H.; et al. Arterial stiffness and dementia pathology: Atherosclerosis Risk in Communities (ARIC)-PET Study. Neurology 2018, 90, e1248–e1256. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- O’Caoimh, R.; Sezgin, D.; O’Donovan, M.R.; Molloy, D.W.; Clegg, A.; Rockwood, K.; Liew, A. Prevalence of frailty in 62 countries across the world: A systematic review and meta-analysis of population-level studies. Age Ageing 2021, 50, 96–104. [Google Scholar] [CrossRef]
- Piotrowicz, K.; Gasowski, J. Risk Factors for Frailty and Cardiovascular Diseases: Are They the Same? Adv. Exp. Med. Biol. 2020, 1216, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, M.S.; Ramirez, J.L.; Gasper, W.J.; Zahner, G.J.; Hills, N.K.; Grenon, S.M. Frailty Is Associated with an Increased Risk of Major Adverse Cardiac Events in Patients with Stable Claudication. Ann. Vasc. Surg. 2018, 50, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ewe, S.H.; Ajmone Marsan, N.; Pepi, M.; Delgado, V.; Tamborini, G.; Muratori, M.; Ng, A.C.; van der Kley, F.; de Weger, A.; Schalij, M.J.; et al. Impact of left ventricular systolic function on clinical and echocardiographic outcomes following transcatheter aortic valve implantation for severe aortic stenosis. Am. Heart J. 2010, 160, 1113–1120. [Google Scholar] [CrossRef]
- Arnold, S.V.; Zhao, Y.; Leon, M.B.; Sathananthan, J.; Alu, M.; Thourani, V.H.; Smith, C.R.; Mack, M.J.; Cohen, D.J. Impact of Frailty and Prefrailty on Outcomes of Transcatheter or Surgical Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2022, 15, e011375. [Google Scholar] [CrossRef]
- Campo, G.; Maietti, E.; Tonet, E.; Biscaglia, S.; Ariza-Sole, A.; Pavasini, R.; Tebaldi, M.; Cimaglia, P.; Bugani, G.; Serenelli, M.; et al. The Assessment of Scales of Frailty and Physical Performance Improves Prediction of Major Adverse Cardiac Events in Older Adults with Acute Coronary Syndrome. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1113–1119. [Google Scholar] [CrossRef]
- Damluji, A.A.; Chung, S.E.; Xue, Q.L.; Hasan, R.K.; Moscucci, M.; Forman, D.E.; Bandeen-Roche, K.; Batchelor, W.; Walston, J.D.; Resar, J.R.; et al. Frailty and cardiovascular outcomes in the National Health and Aging Trends Study. Eur. Heart J. 2021, 42, 3856–3865. [Google Scholar] [CrossRef]
- Piotrowicz, K.; Gryglewska, B.; Grodzicki, T.; Gasowski, J. Arterial stiffness and frailty—A systematic review and metaanalysis. Exp. Gerontol. 2021, 153, 111480. [Google Scholar] [CrossRef]
- Alvarez-Bueno, C.; Cunha, P.G.; Martinez-Vizcaino, V.; Pozuelo-Carrascosa, D.P.; Visier-Alfonso, M.E.; Jimenez-Lopez, E.; Cavero-Redondo, I. Arterial Stiffness and Cognition Among Adults: A Systematic Review and Meta-Analysis of Observational and Longitudinal Studies. J. Am. Heart Assoc. 2020, 9, e014621. [Google Scholar] [CrossRef]
- Zhang, Y.; Miyai, N.; Abe, K.; Utsumi, M.; Uematsu, Y.; Terada, K.; Nakatani, T.; Takeshita, T.; Arita, M. Muscle mass reduction, low muscle strength, and their combination are associated with arterial stiffness in community-dwelling elderly population: The Wakayama Study. J. Hum. Hypertens. 2021, 35, 446–454. [Google Scholar] [CrossRef]
- Plunde, O.; Back, M. Arterial Stiffness in Aortic Stenosis and the Impact of Aortic Valve Replacement. Vasc. Health Risk Manag. 2022, 18, 117–122. [Google Scholar] [CrossRef]
- Tanaka, T.; Asami, M.; Yahagi, K.; Ninomiya, K.; Okuno, T.; Horiuchi, Y.; Komiyama, K.; Tanaka, J.; Yokozuka, M.; Miura, S.; et al. Prognostic impact of arterial stiffness following transcatheter aortic valve replacement. J. Cardiol. 2021, 78, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Broyd, C.J.; Patel, K.; Pugliese, F.; Chehab, O.; Mathur, A.; Baumbach, A.; Ozkor, M.; Kennon, S.; Mullen, M. Pulse wave velocity can be accurately measured during transcatheter aortic valve implantation and used for post-procedure risk stratification. J. Hypertens. 2019, 37, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Baran, J.; Kablak-Ziembicka, A.; Kleczynski, P.; Alfieri, O.; Niewiara, L.; Badacz, R.; Pieniazek, P.; Legutko, J.; Zmudka, K.; Przewlocki, T.; et al. Association of Increased Vascular Stiffness with Cardiovascular Death and Heart Failure Episodes Following Intervention on Symptomatic Degenerative Aortic Stenosis. J. Clin. Med. 2022, 11, 2078. [Google Scholar] [CrossRef] [PubMed]
- Velek, P.; Luik, A.I.; Brusselle, G.G.O.; Stricker, B.C.; Bindels, P.J.E.; Kavousi, M.; Kieboom, B.C.T.; Voortman, T.; Ruiter, R.; Ikram, M.A.; et al. Sex-specific patterns and lifetime risk of multimorbidity in the general population: A 23-year prospective cohort study. BMC Med. 2022, 20, 304. [Google Scholar] [CrossRef]
- Rippo, M.R.; Olivieri, F.; Monsurro, V.; Prattichizzo, F.; Albertini, M.C.; Procopio, A.D. MitomiRs in human inflamm-aging: A hypothesis involving miR-181a, miR-34a and miR-146a. Exp. Gerontol. 2014, 56, 154–163. [Google Scholar] [CrossRef]
- Iannone, F.; Crocco, P.; Dato, S.; Passarino, G.; Rose, G. Circulating miR-181a as a novel potential plasma biomarker for multimorbidity burden in the older population. BMC Geriatr. 2022, 22, 772. [Google Scholar] [CrossRef]
- Garin, N.; Koyanagi, A.; Chatterji, S.; Tyrovolas, S.; Olaya, B.; Leonardi, M.; Lara, E.; Koskinen, S.; Tobiasz-Adamczyk, B.; Ayuso-Mateos, J.L.; et al. Global Multimorbidity Patterns: A Cross-Sectional, Population-Based, Multi-Country Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 205–214. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J. Mechanisms of development of multimorbidity in the elderly. Eur. Respir. J. 2015, 45, 790–806. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, E.D.; Hughes, J.; Ferenbach, D.A. Renal Aging: Causes and Consequences. J. Am. Soc. Nephrol. 2017, 28, 407–420. [Google Scholar] [CrossRef] [Green Version]
- Lacolley, P.; Regnault, V.; Laurent, S. Mechanisms of Arterial Stiffening: From Mechanotransduction to Epigenetics. Arter. Thromb. Vasc. Biol. 2020, 40, 1055–1062. [Google Scholar] [CrossRef]
- Sheridan, P.E.; Mair, C.A.; Quinones, A.R. Associations between prevalent multimorbidity combinations and prospective disability and self-rated health among older adults in Europe. BMC Geriatr. 2019, 19, 198. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, B.; Reilly, R.B.; Kenny, R.A. Investigation of multimorbidity and prevalent disease combinations in older Irish adults using network analysis and association rules. Sci. Rep. 2019, 9, 14567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Wang, Y.; Hou, L.; Zuo, Z.; Zhang, N.; Wei, A. Multimorbidity patterns in old adults and their associated multi-layered factors: A cross-sectional study. BMC Geriatr. 2021, 21, 372. [Google Scholar] [CrossRef] [PubMed]
- Masoli, J.A.H.; Pilling, L.C.; Frayling, T.M. Genomics and multimorbidity. Age Ageing 2022, 51, afac285. [Google Scholar] [CrossRef] [PubMed]
- Melzer, D.; Pilling, L.C.; Ferrucci, L. The genetics of human ageing. Nat. Rev. Genet. 2020, 21, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.; Feng, J.; Sun, F.; Chen, J.; Zhao, X.M. A global overview of genetically interpretable multimorbidities among common diseases in the UK Biobank. Genome Med. 2021, 13, 110. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Jia, G.; Wen, W.; Long, J.; Zheng, W. Evaluating polygenic risk scores in assessing risk of nine solid and hematologic cancers in European descendants. Int. J. Cancer 2020, 147, 3416–3423. [Google Scholar] [CrossRef]
- Littlejohns, T.J.; Collister, J.A.; Liu, X.; Clifton, L.; Tapela, N.M.; Hunter, D.J. Hypertension, a dementia polygenic risk score, APOE genotype, and incident dementia. Alzheimers Dement. 2022, 19, 467–476. [Google Scholar] [CrossRef]
- Budoff, M.J.; Alpert, B.; Chirinos, J.A.; Fernhall, B.; Hamburg, N.; Kario, K.; Kullo, I.; Matsushita, K.; Miyoshi, T.; Tanaka, H.; et al. Clinical Applications Measuring Arterial Stiffness: An Expert Consensus for the Application of Cardio-Ankle Vascular Index. Am. J. Hypertens. 2022, 35, 441–453. [Google Scholar] [CrossRef]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [Green Version]
- D’Elia, L.; Galletti, F.; La Fata, E.; Sabino, P.; Strazzullo, P. Effect of dietary sodium restriction on arterial stiffness: Systematic review and meta-analysis of the randomized controlled trials. J. Hypertens. 2018, 36, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.N.; Buchanich, J.M.; Youk, A.; Brooks, M.M.; Barinas-Mitchell, E.; Conroy, M.B.; Sutton-Tyrrell, K. Reductions in arterial stiffness with weight loss in overweight and obese young adults: Potential mechanisms. Atherosclerosis 2012, 223, 485–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaitkevicius, P.V.; Fleg, J.L.; Engel, J.H.; O’Connor, F.C.; Wright, J.G.; Lakatta, L.E.; Yin, F.C.; Lakatta, E.G. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation 1993, 88, 1456–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Palta, P.; Folsom, A.R.; Meyer, M.L.; Matsushita, K.; Evenson, K.R.; Aguilar, D.; Heiss, G. Habitual physical activity and central artery stiffening in older adults: The Atherosclerosis Risk in Communities study. J. Hypertens. 2018, 36, 1889–1894. [Google Scholar] [CrossRef]
- Ahmadi-Abhari, S.; Sabia, S.; Shipley, M.J.; Kivimaki, M.; Singh-Manoux, A.; Tabak, A.; McEniery, C.; Wilkinson, I.B.; Brunner, E.J. Physical Activity, Sedentary Behavior, and Long-Term Changes in Aortic Stiffness: The Whitehall II Study. J. Am. Heart Assoc. 2017, 6, 5974. [Google Scholar] [CrossRef]
- Tanaka, H. Antiaging Effects of Aerobic Exercise on Systemic Arteries. Hypertension 2019, 74, 237–243. [Google Scholar] [CrossRef]
- Evans, W.; Willey, Q.; Hanson, E.D.; Stoner, L. Effects of Resistance Training on Arterial Stiffness in Persons at Risk for Cardiovascular Disease: A Meta-analysis. Sports Med. 2018, 48, 2785–2795. [Google Scholar] [CrossRef]
- Ceciliato, J.; Costa, E.C.; Azevedo, L.; Sousa, J.C.; Fecchio, R.Y.; Brito, L.C. Effect of Resistance Training on Arterial Stiffness in Healthy Subjects: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22, 51. [Google Scholar] [CrossRef]
- Ong, K.T.; Delerme, S.; Pannier, B.; Safar, M.E.; Benetos, A.; Laurent, S.; Boutouyrie, P.; Investigators. Aortic stiffness is reduced beyond blood pressure lowering by short-term and long-term antihypertensive treatment: A meta-analysis of individual data in 294 patients. J. Hypertens. 2011, 29, 1034–1042. [Google Scholar] [CrossRef]
- Mallareddy, M.; Parikh, C.R.; Peixoto, A.J. Effect of angiotensin-converting enzyme inhibitors on arterial stiffness in hypertension: Systematic review and meta-analysis. J. Clin. Hypertens. (Greenwich) 2006, 8, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Ling, Q.; Song, Q.; Bai, J.; Wu, S.; Zhang, W.; Chen, M.; Cai, J. Temporal Relationship Between Arterial Stiffness and Systolic Blood Pressure Under Intensive or Standard Control: A Post Hoc Analysis of the STEP Trial. Hypertension 2022, 79, 2755–2763. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.F.; Wang, Y.; Wang, G.; Zhou, Z.; Chen, S.; Geng, T.; Zhang, Y.B.; Wang, Y.; Chen, J.X.; Pan, A.; et al. Association Between Statin Use and Progression of Arterial Stiffness Among Adults With High Atherosclerotic Risk. JAMA Netw. Open 2022, 5, e2218323. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triposkiadis, F.; Xanthopoulos, A.; Lampropoulos, K.; Briasoulis, A.; Sarafidis, P.; Skoularigis, J.; Boudoulas, H. Aortic Stiffness: A Major Risk Factor for Multimorbidity in the Elderly. J. Clin. Med. 2023, 12, 2321. https://doi.org/10.3390/jcm12062321
Triposkiadis F, Xanthopoulos A, Lampropoulos K, Briasoulis A, Sarafidis P, Skoularigis J, Boudoulas H. Aortic Stiffness: A Major Risk Factor for Multimorbidity in the Elderly. Journal of Clinical Medicine. 2023; 12(6):2321. https://doi.org/10.3390/jcm12062321
Chicago/Turabian StyleTriposkiadis, Filippos, Andrew Xanthopoulos, Konstantinos Lampropoulos, Alexandros Briasoulis, Pantelis Sarafidis, John Skoularigis, and Harisios Boudoulas. 2023. "Aortic Stiffness: A Major Risk Factor for Multimorbidity in the Elderly" Journal of Clinical Medicine 12, no. 6: 2321. https://doi.org/10.3390/jcm12062321