

Transcranial Doppler Echography Measurement in Hemodialysis Patients: The Potential Role of Angiotensin II Receptor Blockades on Cerebrovascular Circulation
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
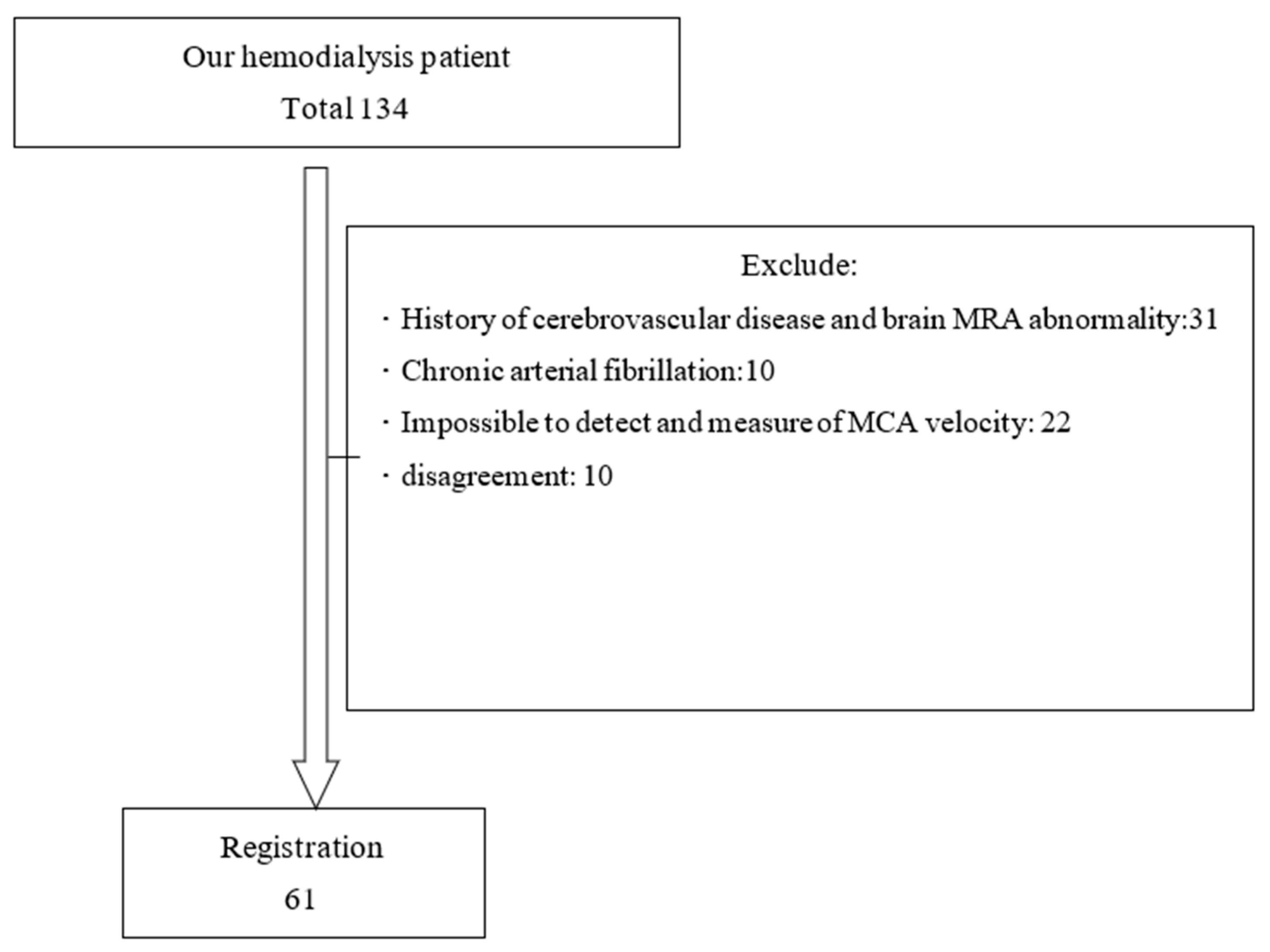
2.1. Patients
2.2. Method
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Doppler Echography Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Japanese Society for Dialysis Therapy. An Overview of Regular Dialysis Treatment in Japan; The Japanese Society for Dialysis Therapy: Tokyo, Japan, 2007. [Google Scholar]
- Heart Outcomes Prevention Evaluation (HOPE) Study Investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: Results of the HOPE study and MICRO-HOPE substudy. Lancet 2000, 355, 253–259. [Google Scholar] [CrossRef]
- Dahlöf, B.; Devereux, R.B.; Kjeldsen, S.E.; Julius, S.; Beevers, G.; Faire, U.; Fyhrquist, F.; Ibsen, H.; Kristiansson, K.; Lederballe-Pedersen, O.; et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): A randomized trial against atenolol. Lancet 2002, 359, 995–1003. [Google Scholar] [CrossRef]
- Ariff, B.; Zambanini, A.; Vamadeva, S.; Barratt, D.; Xu, Y.; Sever, P.; Stanton, A.; Hughes, A.; Thom, S. Candesartan- and Atenolol-based treatments induce different patterns of carotid artery and left ventricular remodeling in hypertension. Stroke 2006, 37, 2381–2384. [Google Scholar] [CrossRef] [Green Version]
- Thöne-Reineke, C.; Steckelings, U.M.; Unger, T. Angiotensin receptor blockers and cerebral protection in stroke. J. Hypertens. 2006, 24, S115–S129. [Google Scholar] [CrossRef]
- Vingerhoets, G.; Stroobant, N. Lateralizaion of cerebral blood flow velocity changes during cognitive tasks: A simultaneous bilateral Doppler study. Stroke 1999, 30, 2152–2158. [Google Scholar] [CrossRef]
- Kobayashi, S.; Moriya, H.; Aso, K.; Ohtake, T. Vitamin E–bonded hemodialyzer improves atherosclerosis associated with a rheological improvement of circulating red blood cells. Kidney Int. 2003, 63, 1881–1887. [Google Scholar] [CrossRef] [Green Version]
- Barnett, H.J.M.; Mohr, J.P.; Stein, B.M.; Yatsu, F. Transcranial Doppler echo. Stroke, 3rd ed.; Churchill Livingstone: New York, NY, USA, 1998; pp. 309–317. [Google Scholar]
- Krejza, J.; Mariak, Z.; Walecki, J.; Szydlik, P.; Lewko, J.; Ustymowicz, A. Transcranial color Doppler sonography of basal cerebral arteries in 182 healthy subjects: Age and sex variability and normal reference values for blood flow parameters. AJR 1999, 172, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Yamakado, M. Protective vascular effect of angiotensin receptor blocker (ARB). Nihon Rinsho Jpn. J. Clin. Med. 2002, 60, 2020–2027. [Google Scholar]
- Wijnhoud, A.D.; Koudstaal, P.J.; Dippel, D.W.J. Relationships of transcranial blood flow Doppler parameters with major vascular risk factors: TCD study in patients with a recent TIA or nondisabling ischemic stroke. J. Clin. Ultrasound 2006, 34, 70–76. [Google Scholar] [CrossRef]
- Newell, D.W. Transcranial Doppler ultrasonography. Neurosurg. Clin. N. Am. 1994, 5, 619–631. [Google Scholar] [CrossRef]
- Norihiko, T.; Takuo, T.; Youichiro, A.; Daisuke, K.; Takashi, S.; Teruhiko, S.; Hiroshi, K. The effects of hemodialysis and A-V shunt formation on cerebral blood flow in patients with chronic renal failure. J. Jpn. Soc. Dial. Ther. 1993, 26, 1261–1265. [Google Scholar]
- Mitchell, J.A. Changes in vertebral artery blood flow following normal rotation of the cervical spine. J. Manip. Physiol. Ther. 2003, 26, 347–351. [Google Scholar] [CrossRef]
- Harper, C.; Cardullo, P.A.; Weyman, A.K.; Patterson, R.B. Transcranial Doppler ultrasonography of the basilar artery in patients with retrograde vertebral artery flow. J. Vasc. Surg. 2008, 48, 859–864. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Gao, S.; Wang, B.; Li, S. The evaluation of intra- and extra-cranial circulation in subclavian steel syndrome. Chin. Med. J. 1997, 110, 286–288. [Google Scholar]
- Ryoichi, Y.; Eiichi, O.; Osamu, I.; Yoshinori, I.; Noriyoshi, K. Right-left difference in cerebrovascular diseases—With reference to morphological changes in cerebral atrophy, ventricular enlargement, and cerebral arteriosclerosis. Jpn. J. Stroke 1993, 15, 434–438. [Google Scholar]
- Kobayashi, S.; Ikeda, T.; Moriya, H.; Ohtake, T.; Kumagai, H. Asymptomatic cerebral lacunae in patients with chronic kidney disease. Am. J. Kidney Dis. 2004, 44, 35–41. [Google Scholar] [CrossRef]


{kind=link}
| N = 61 | |
|---|---|
| Gender (male/female) | 44/17 |
| Age (years) | 67.8 ± 11.4 |
| DM (+%) | 27% |
| Smoking (+%) | 49% |
| BMI | 21.1 ± 2.9 |
| HD vintage (m) | 94.2 ± 58.6 |
| sBP (mmHg) | 149.7 ± 15.8 |
| dBP (mmHg) | 82.7 ± 11.1 |
| Pulse pressure (mmHg) | 66.8 ± 12.5 |
| α-Blocker (n) | 8 (18%) |
| β-Blocker (n) | 2 (3%) |
| αβ-Blocker (n) | 17 (28%) |
| CCB (n) | 34 (56%) |
| ACE-I (n) | 5 (8%) |
| ARB (n) | 22 (36%) |
| Vitamin D (n) | 25 (41%) |
| ARB (+) N = 22 | ARB (-) N = 39 | p-Value | |
|---|---|---|---|
| Gender (M/F) | 17/5 | 27/12 | 0.509 |
| Age (years) | 64.3 ± 10.2 | 69.8 ± 11.7 | 0.070 |
| DM (%) | 27 | 28 | 0.939 |
| Smoking (%) | 55 | 44 | 0.419 |
| BMI | 20.7 ± 2.9 | 21.3 ± 3.0 | 0.428 |
| HD vintage (months) | 100.9 ± 54.6 | 90.4 ± 61.1 | 0.506 |
| sBP (mmHg) | 154.7 ± 10.9 | 146.6 ± 17.5 | 0.061 |
| dBP (mmHg) | 84.3 ± 10.2 | 81.7 ± 11.7 | 0.406 |
| Pulse pressure (mmHg) | 70.2 ± 12.4 | 64.7 ± 12.2 | 0.112 |
| Ca (mg/dL) | 9.3 ± 1.1 | 8.9 ± 0.9 | 0.139 |
| IP (mg/dL) | 6.1 ± 1.2 | 5.9 ± 1.3 | 0.563 |
| Ca × IP | 56.3 ± 10.4 | 52.8 ± 13.1 | 0.277 |
| Intact PTH (ng/dL) | 350.5 ± 198.9 | 270.6 ± 211.4 | 0.151 |
| Hct (%) | 30.9 ± 4.0 | 32.6 ± 4.5 | 0.154 |
| Alb (g/dL) | 3.7 ± 0.3 | 3.6 ± 0.4 | 0.624 |
| β2MG (mg/L) | 30.2 ± 6.7 | 28.5 ± 6.0 | 0.319 |
| Log hsCRP | 2.35 ± 1.67 | 1.85 ± 1.33 | 0.205 |
| Fibrinogen (mg/dL) | 300 ± 77.3 | 336.2 ± 86.2 | 0.107 |
| CCB (%) | 63.6 | 51.3 | 0.419 |
| αβ-Blocker (%) | 27.3 | 28.2 | 0.936 |
| Our HD Patients N = 61 | Normal N = 335 (Age > 60) | ||
|---|---|---|---|
| Rt MCA | Vmax (cm/s) | 90.5 ± 27.4 | 92 |
| Vmin (cm/s) | 34.1 ± 11.1 | 37 | |
| Vmean (cm/s) | 51.6 ± 16.6 | 59 | |
| PI | 1.19 ± 0.5 | 0.96 ± 0.17 | |
| RI | 0.62 ± 0.1 | 0.60 ± 0.06 | |
| Lt MCA | Vmax (cm/s) | 86.0 ± 31.1 | 92 |
| Vmin (cm/s) | 31.2 ± 11.0 | 37 | |
| Vmean (cm/s) | 49.4 ± 16.2 | 59 | |
| PI | 1.10 ± 0.27 | 0.96 ± 0.17 | |
| RI | 0.60 ± 0.08 | 0.60 ± 0.06 | |
| Rt VA | Vmax (cm/s) | 51.2 ± 18.5 | 50.9 ± 18.7 |
| Vmin (cm/s) | 20.1 ± 6.5 | 21.2 ± 9.2 | |
| Vmean (cm/s) | 30.4 ± 9.9 | 30.5 ± 12.4 | |
| PI | 1.01 ± 0.24 | ||
| RI | 0.60 ± 0.09 | ||
| Lt VA | Vmax (cm/s) | 48.6 ± 19.6 | 50.9 ± 18.7 |
| Vmin (cm/s) | 20.0 ± 8.7 | 21.2 ± 9.2 | |
| Vmean (cm/s) | 29.5 ± 12.1 | 30.5 ± 12.4 | |
| PI | 0.98 ± 0.21 | ||
| RI | 0.59 ± 0.07 | ||
| BA | Vmax (cm/s) | 59.5 ± 21.6 | 62 |
| Vmin (cm/s) | 23.0 ± 8.4 | 26 | |
| Vmean (cm/s) | 35.2 ± 12.3 | 40 | |
| PI | 1.04 ± 0.23 | 0.94 ± 0.16 | |
| RI | 0.61 ± 0.08 | 0.60 ± 0.09 |
| ARB (+) N = 22 | ARB (-) N = 39 | p-Value | |
|---|---|---|---|
| Rt MCA (cm/s) | 103.0 ± 30.3 | 84.5 ± 24.4 | 0.065 |
| Lt MCA (cm/s) | 105.7 ± 38.2 | 75.9 ± 23.3 | 0.011 |
| Rt VA (cm/s) | 56.1 ± 21.8 | 46.9 ± 15.8 | 0.068 |
| Lt VA (cm/s) | 53.5 ± 25.0 | 44.8 ± 14.0 | 0.101 |
| BA (cm/s) | 65.6 ± 28.3 | 55.7 ± 16.4 | 0.142 |
| Rt CCA max IMT (mm) | 0.8 ± 0.2 | 0.9 ± 0.3 | 0.102 |
| Lt CCA max IMT (mm) | 0.8 ± 0.2 | 0.9 ± 0.3 | 0.084 |
| r | p-Value | |
|---|---|---|
| Age | 0.110 | 0.563 |
| HD vintage | 0.273 | 0.145 |
| DM+/− | 0.094 | 0.622 |
| Smoking+/− | 0.260 | 0.165 |
| Hct | −0.357 | 0.045 |
| Albumin | 0.233 | 0.216 |
| β₂MG | 0.043 | 0.824 |
| Log hsCRP | 0.043 | 0.824 |
| Fibrinogen | 0.050 | 0.183 |
| sBP | 0.265 | 0.181 |
| dBP | 0.190 | 0.343 |
| Pulse pressure | 0.332 | 0.078 |
| ARB | 0.443 | 0.011 |
| CCB | 0.227 | 0.227 |
| 95% CI | β | p-Value | |
|---|---|---|---|
| ARB usage | 3.961–48.464 | 0.389 | 0.022 |
| Hct | −4.210–0.37 | −0.282 | 0.091 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maesato, K.; Kobayashi, S.; Ohtake, T.; Mochida, Y.; Ishioka, K.; Oka, M.; Moriya, H.; Hidaka, S. Transcranial Doppler Echography Measurement in Hemodialysis Patients: The Potential Role of Angiotensin II Receptor Blockades on Cerebrovascular Circulation. J. Clin. Med. 2023, 12, 2295. https://doi.org/10.3390/jcm12062295
Maesato K, Kobayashi S, Ohtake T, Mochida Y, Ishioka K, Oka M, Moriya H, Hidaka S. Transcranial Doppler Echography Measurement in Hemodialysis Patients: The Potential Role of Angiotensin II Receptor Blockades on Cerebrovascular Circulation. Journal of Clinical Medicine. 2023; 12(6):2295. https://doi.org/10.3390/jcm12062295
Chicago/Turabian StyleMaesato, Kyoko, Shuzo Kobayashi, Takayasu Ohtake, Yasuhiro Mochida, Kunihiro Ishioka, Machiko Oka, Hidekazu Moriya, and Sumi Hidaka. 2023. "Transcranial Doppler Echography Measurement in Hemodialysis Patients: The Potential Role of Angiotensin II Receptor Blockades on Cerebrovascular Circulation" Journal of Clinical Medicine 12, no. 6: 2295. https://doi.org/10.3390/jcm12062295