
The Availability, Cost, Limitations, Learning Curve and Future of Robotic Systems in Urology and Prostate Cancer Surgery


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. History of Robotics in Urology
3. Robotic Systems
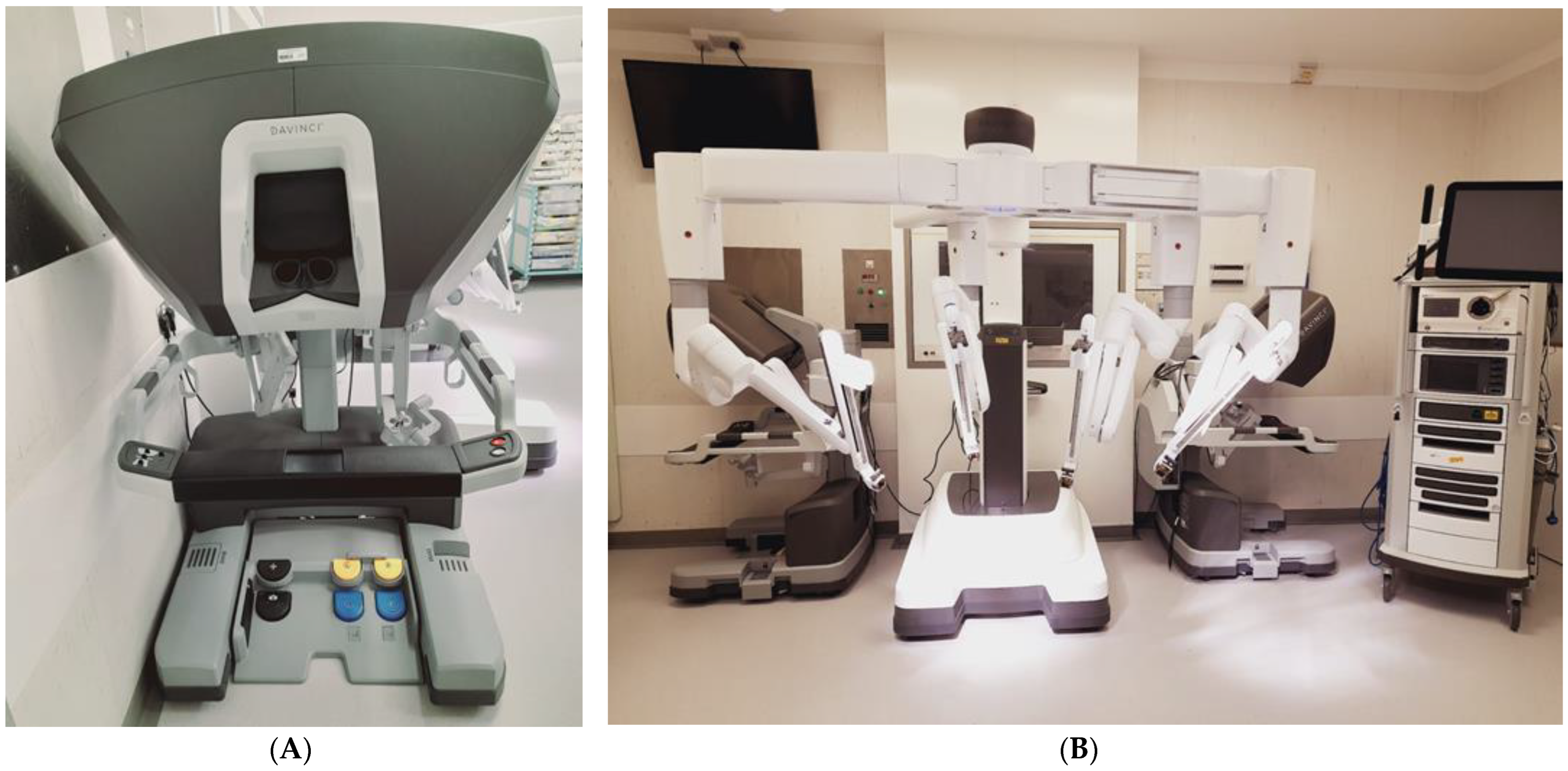
4. Da Vinci
5. Versius
6. Senhance
7. Hinotori
8. Revo-I
9. Hugo
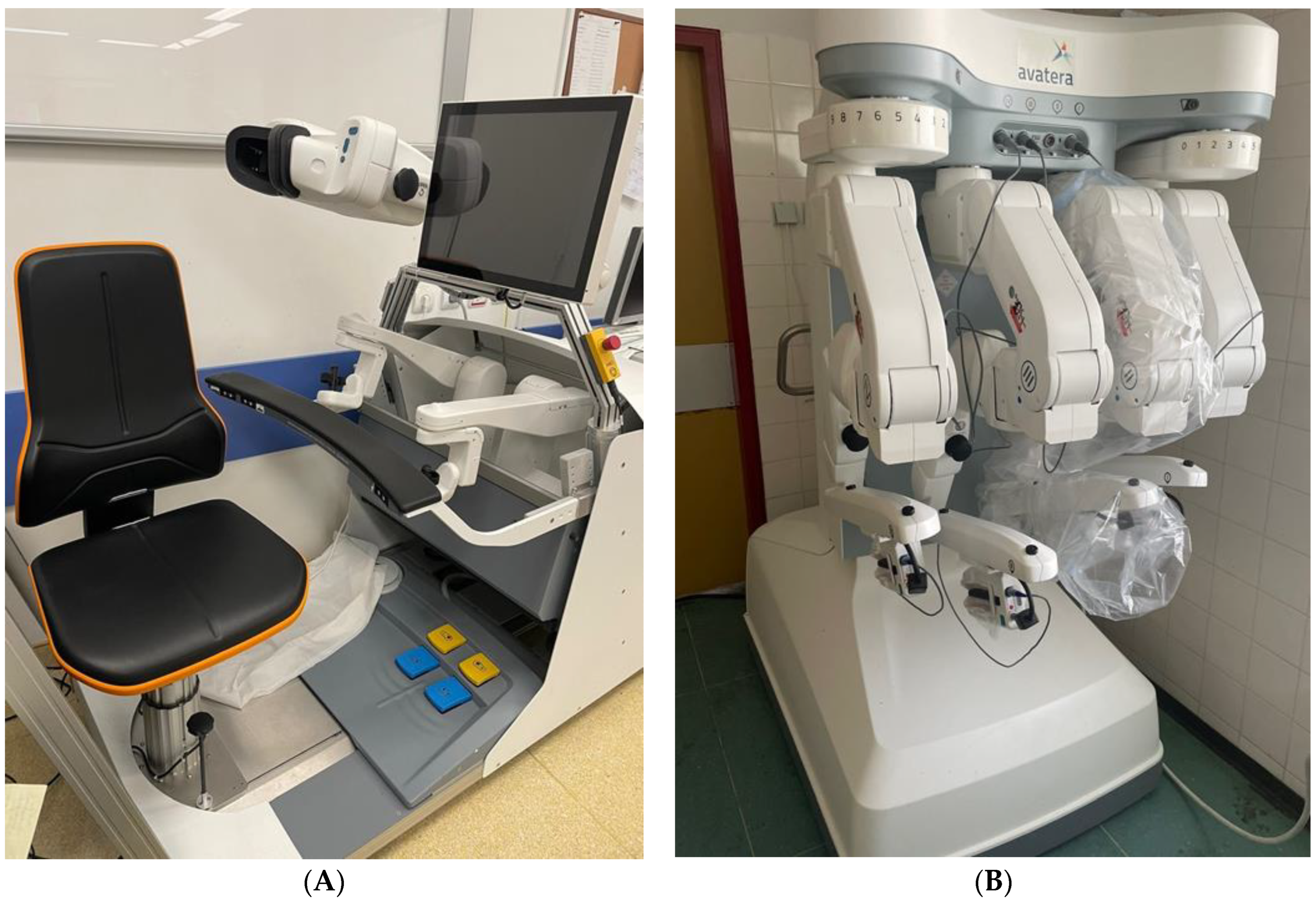
10. Avatera
11. Future Developments
12. Barriers to Robot-Assisted Surgery
13. Accessibility
14. Cost
15. Cost Comparison
16. Training and Learning Curves
17. Limitations of Robotic Surgery
18. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Marchi, D.; Mantica, G.; Tafuri, A.; Giusti, G.; Gaboardi, F. Robotic surgery in urology: A review from the beginning to the single-site. AME Med. J. 2022, 7, 16. [Google Scholar] [CrossRef]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Eberli, D.; De Meerleer, G.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; van der Kwast, T.H.; et al. European Association of Urologists Guidelines on Prostate Cancer. Available online: https://uroweb.org/guidelines/prostate-cancer (accessed on 14 November 2022).
- Binder, J.; Kramer, W. Robotically-assisted laparoscopic radical prostatectomy. BJU Int. 2001, 87, 408–410. [Google Scholar] [CrossRef] [PubMed]
- The British Association of Urological Surgeons (BAUS). Radical Prostatectomy Outcomes Data. Available online: www.baus.org.uk/patients/surgical_outcomes/radical_prostatectomy (accessed on 2 November 2022).
- Hubert, N.; Gilles, M.; Desbrosses, K.; Meyer, J.P.; Felblinger, J.; Hubert, J. Ergonomic assessment of the surgeon’s physical workload during standard and robotic assisted laparoscopic procedures. Int. J. Med. Robot. 2013, 9, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Prete, F.P.; Pezzolla, A.; Prete, F.; Testini, M.; Marzaioli, R.; Patriti, A.; Jimenez-Rodriguez, R.M.; Gurrado, A.; Strippoli, G.F. Robotic versus laparoscopic minimally invasive surgery for rectal cancer: A systematic review and meta-analysis of randomized controlled trials. Ann. Surg. 2018, 267, 1034–1046. [Google Scholar] [CrossRef]
- Supe, A.N.; Kulkarni, G.V.; Supe, P.A. Ergonomics in laparoscopic surgery. J. Minim. Access Surg. 2010, 6, 31–36. [Google Scholar] [CrossRef]
- Rao, P.P. Robotic surgery: New robots and finally some real competition! World J. Urol. 2018, 36, 537–541. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; Jung, J.H.; Edgerton, Z.; Lee, H.; Lee, S.; Bakker, C.J.; Dahm, P. Retzius-sparing versus standard robotic-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer. Cochrane Database Syst. Rev. 2020, 8, CD013641. [Google Scholar]
- Pal, R.P.; Koupparis, A.J. Expanding the indications of robotic surgery in urology: A systematic review of the literature. Arab. J. Urol. 2018, 16, 270–284. [Google Scholar] [CrossRef] [Green Version]
- Zahid, A.; Ayyan, M.; Farooq, M.; Cheema, H.A.; Shahid, A.; Naeem, F.; Ilyas, M.A.; Sohail, S. Robotic surgery in comparison to the open and laparoscopic approaches in the field of urology: A systematic review. J. Robotic Surg. 2023, 17, 11–29. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Kalapara, A.; Frydenberg, M.; Lawrentschuk, N.; Weight, C.J.; Parekh, D.; Konety, B.R. Robotic Assisted Radical Cystectomy vs Open Radical Cystectomy: Systematic Review and Meta-Analysis. J. Urol. 2019, 201, 715–720. [Google Scholar] [CrossRef]
- Choi, J.E.; You, J.H.; Kim, D.K.; Rha, K.H.; Lee, S.H. Comparison of perioperative outcomes between robotic and laparoscopic partial nephrectomy: A systematic review and meta-analysis. Eur. Urol. 2015, 67, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Garg, H.; Mansour, A.M.; Psutka, S.P.; Kim, S.P.; Porter, J.; Gaspard, C.S.; Dursun, F.; Pruthi, D.K.; Wang, H.; Kaushik, D. Robotic retroperitoneal lymph node dissection: A systematic review of perioperative outcomes. BJU Int. 2023. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Grand View Research. Surgical Robots Market Size, Share & Trends Analysis Report by Application (Orthopedics, Neurology, Urology, Gynecology), by Region (North America, Europe, Asia Pacific, LATAM, MEA), and Segment Forecasts, 2022–2030. Available online: https://www.grandviewresearch.com/industry-analysis/surgical-robot-market (accessed on 14 November 2022).
- Intuitive Surgical. Intuitive Announces Preliminary Fourth Quarter and Full Year 2021 Results. Available online: https://isrg.intuitive.com/news-releases/news-release-details/intuitive-announces-preliminary-fourth-quarter-and-full-year-1 (accessed on 14 November 2022).
- Stephan, D.; Sälzer, H.; Willeke, F. First Experiences with the New Senhance® Telerobotic System in Visceral Surgery. Visc. Med. 2018, 34, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Haig, F.; Medeiros, A.C.B.; Chitty, K.; Slack, M. Usability assessment of Versius, a new robot-assisted surgical device for use in minimal access surgery. BMJ Surg. Interv. Health Technol. 2020, 22, e000028. [Google Scholar] [CrossRef] [PubMed]
- Hinata, N.; Yamaguchi, R.; Kusuhara, Y.; Kanayama, H.; Kohjimoto, Y.; Hara, I.; Fujisawa, M. Hinotori Surgical Robot System, a novel robot-assisted surgical platform: Preclinical and clinical evaluation. Int. J. Urol. 2022, 29, 1213–1220. [Google Scholar] [CrossRef]
- Chang, K.D.; Abdel Raheem, A.; Choi, Y.D.; Chung, B.H.; Rha, K.H. Retzius-sparing robot-assisted radical prostatectomy using the Revo-i robotic surgical system: Surgical technique and results of the first human trial. BJU Int. 2018, 122, 441–448. [Google Scholar] [CrossRef]
- Lam, K.; Clarke, J.; Purkayastha, S.; Kinross, J.M. Uptake and accessibility of surgical robotics in England. Int. J. Med. Robot. 2021, 17, e2174. [Google Scholar] [CrossRef]
- Soomro, N.A.; Hashimoto, D.A.; Porteous, A.J.; Ridley, C.J.A.; Marsh, W.J.; Ditto, R.; Roy, S. Systematic review of learning curves in robot-assisted surgery. BJS Open 2020, 4, 27–44. [Google Scholar] [CrossRef] [Green Version]
- Davies, B.L.; Hibberd, R.D.; Coptcoat, M.J.; Wickham, J.E.A. A surgeon robot prostatectomy—A laboratory evaluation. J. Med. Eng. Technol. 1989, 13, 273–277. [Google Scholar] [CrossRef]
- Sung, G.T.; Gill, I.S. Robotic laparoscopic surgery: A comparison of the da Vinci and Zeus systems. J. Urol. 2001, 58, 893–898. [Google Scholar] [CrossRef]
- Berguer, R.; Forkey, D.L.; Smith, W.D. The effect of laparoscopic instrument working angle on surgeons’ upper extremity workload. Surg. Endosc. 2001, 15, 1027–1029. [Google Scholar] [CrossRef] [PubMed]
- Barakat, B.; Othman, H.; Gauger, U.; Wolff, I.; Hadaschik, B.; Rehme, C. Retzius Sparing Radical Prostatectomy Versus Robot-assisted Radical Prostatectomy: Which Technique Is More Beneficial for Prostate Cancer Patients (MASTER Study)? A Systematic Review and Meta-analysis. Eur. Urol. Focus 2022, 8, 1060–1071. [Google Scholar] [CrossRef] [PubMed]
- Lantz, A.; Bock, D.; Akre, O.; Angenete, E.; Bjartell, A.; Carlsson, S.; Modig, K.K.; Nyberg, M.; Kollberg, K.S.; Steineck, G.; et al. Functional and Oncological Outcomes After Open Versus Robot-assisted Laparoscopic Radical Prostatectomy for Localised Prostate Cancer: 8-Year Follow-up. Eur. Urol. 2021, 80, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Ngu, J.C.; Tsang, C.B.; Koh, D.C. The da Vinci Xi: A review of its capabilities, versatility, and potential role in robotic colorectal surgery. Robot Surg. 2017, 4, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, D.K.; Sharma, V.; Toussi, A.; Viers, B.R.; Tollefson, M.K.; Gettman, M.T.; Frank, I. Initial Experience with da Vinci Single-port Robot-assisted Radical Prostatectomies. Eur. Urol. 2020, 77, 373–379. [Google Scholar] [CrossRef]
- Kim, J.E.; Kaldany, A.; Lichtbroun, B.; Singer, E.A.; Jang, T.L.; Ghodoussipour, S.; Kim, M.M.; Kim, I.Y. Single-Port Robotic Radical Prostatectomy: Short-Term Outcomes and Learning Curve. J. Endourol. 2022, 36, 1285–1289. [Google Scholar] [CrossRef]
- Covas Moschovas, M.; Bhat, S.; Rogers, T.; Onol, F.; Roof, S.; Mazzone, E.; Mottrie, A.; Patel, P. Technical Modifications Necessary to Implement the da Vinci Single-port Robotic System. Eur. Urol. 2020, 78, 415–423. [Google Scholar] [CrossRef]
- Hinojosa-Gonzalez, D.E.; Roblesgil-Medrano, A.; Torres-Martinez, M.; Alanis-Garza, C.; Estrada-Mendizabal, R.J.; Gonzalez-Bonilla, E.A.; Flores-Villalba, E.; Olvera-Posada, D. Single-port versus multiport robotic-assisted radical prostatectomy: A systematic review and meta-analysis on the da Vinci SP platform. Prostate 2022, 82, 405–414. [Google Scholar] [CrossRef]
- CMR Surgical. CMR Presskit. Available online: https://cmrsurgical.com/press-kit (accessed on 23 February 2023).
- Thomas, B.C.; Slack, M.; Hussain, M.; Barber, N.; Pradhan, A.; Dinneen, E.; Stewart, G.D. Preclinical Evaluation of the Versius Surgical System, a New Robot-assisted Surgical Device for Use in Minimal Access Renal and Prostate Surgery. Eur. Urol. Focus 2021, 7, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Alkatout, I.; Salehiniya, H.; Allahqoli, L. Assessment of the Versius Robotic Surgical System in Minimal Access Surgery: A Systematic Review. J. Clin. Med. 2022, 11, 3754. [Google Scholar] [CrossRef]
- CMR Surgical. CMR Surgical Announces more than 100 Versius Systems Installed Globally. Available online: https://cmrsurgical.com/wp-content/uploads/2022/11/English-PDF.pdf (accessed on 22 November 2022).
- Venckus, R.; Jasenas, M.; Telksnys, T.; Venckus, M.; Janusonis, V.; Dulskas, A.; Samalavicius, N.E. Robotic-assisted radical prostatectomy with the Senhance® robotic platform: Single center experience. World J. Urol. 2021, 39, 4305–4310. [Google Scholar] [CrossRef] [PubMed]
- Kastelan, Z.; Hudolin, T.; Kulis, T.; Knezevic, N.; Penezic, L.; Maric, M.; Zekulic, T. Upper urinary tract surgery and radical prostatectomy with Senhance® robotic system: Single center experience-First 100 cases. Int. J. Med. Robot. 2021, 17, e2269. [Google Scholar] [CrossRef] [PubMed]
- Alip, S.; Koukourikis, P.; Han, W.K.; Rha, K.H.; Na, J.C. Comparing Revo-i and da Vinci in Retzius-Sparing Robot-Assisted Radical Prostatectomy: A Preliminary Propensity Score Analysis of Outcomes. J. Endourol. 2022, 36, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Sarchi, L.; Mottaran, A.; Bravi, C.A.; Paciotti, M.; Farinha, R.; Piazza, P.; Puliatti, S.; De Groote, R.; De Naeyer, G.; Gallagher, A.; et al. Robot-assisted radical prostatectomy feasibility and setting with the Hugo™ robot-assisted surgery system. BJU Int. 2022, 130, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Bravi, C.A.; Paciotti, M.; Sarchi, L.; Mottaran, A.; Nocera, L.; Farinha, R.; De Backer, P.; Vinckier, M.H.; De Naeyer, G.; D’Hondt, F.; et al. Robot-assisted Radical Prostatectomy with the Novel Hugo Robotic System: Initial Experience and Optimal Surgical Set-up at a Tertiary Referral Robotic Center. Eur. Urol. 2022, 82, 233–237. [Google Scholar] [CrossRef]
- Totaro, A.; Campetella, M.; Bientinesi, R.; Gandi, C.; Palermo, G.; Russo, A.; Aceto, P.; Bassi, P.; Sacco, E. The new surgical robotic platform HUGOTMRAS: System description and docking settings for robot-assisted radical prostatectomy. Urologia 2022, 89, 603–609. [Google Scholar] [CrossRef]
- Avateramedical. Avatera system. Available online: https://www.avatera.eu/en/avatera-system (accessed on 23 February 2023).
- Peteniaris, A.; Kallidonis, P.; Tsaturyan, A.; Pagonis, K.; Faitatziadis, S.; Gkeka, K.; Vagionis, A.; Natsos, A.; Obaidat, M.; Anaplioti, E.; et al. The feasibility of robot-assisted radical cystectomy: An experimental study. World J. Urol. 2023, 41, 477–482. [Google Scholar] [CrossRef]
- Gkeka, K.; Tsaturyan, A.; Faitatziadis, S.; Peteinaris, A.; Anaplioti, E.; Pagonis, K.; Vagionis, A.; Tatanis, V.; Vrettos, T.; Kallidonis, P.; et al. Robot-Assisted Radical Nephrectomy Using the Novel Avatera Robotic Surgical System: A Feasibility Study in a Porcine Model. J. Endourol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Distalmotion. Distalmotion Dexter. Available online: https://www.distalmotion.com/product/ (accessed on 24 November 2022).
- Distalmotion. First Dexter Surgeries in Urology Carried Out in Bern. Available online: https://www.distalmotion.com/first-dexter-surgeries-in-urology/ (accessed on 24 November 2022).
- Whooley, S. Ottava Surgical Assistant Robot Finally Unveiled by Johnson and Johnson. Available online: www.therobotreport.com/ottava-surgical-assistant-robot-finally-unveiled-by-johnson-johnson (accessed on 24 November 2022).
- Suntharasivam, T.; Mukherjee, A.; Luk, A.; Aboumarzouk, O.; Somani, B.; Rai, B.P. The role of robotic surgery in the management of renal tract calculi. Transl. Androl. Urol. 2019, 8 (Suppl. S4), S457–S460. [Google Scholar] [CrossRef]
- Murgu, S.D. Robotic assisted-bronchoscopy: Technical tips and lessons learned from the initial experience with sampling peripheral lung lesions. BMC Pulm. Med. 2019, 19, 89. [Google Scholar] [CrossRef] [Green Version]
- Chi, T.; Hathaway, L.; Chok, R.; Stoller, M. MP15-09 Robotic-Assisted Percutaneous Nephrolithotomy and Ureteroscopy with the Monarch® Platform, Urology Compares Favorably Against Conventional Techniques. Abstracts of the 39th World Congress of Endourology: WCE 2022. J. Endourol. 2022, 36 (Suppl. S1), A1–A315. [Google Scholar]
- Mohan, A.; Wara, U.; Arshad Shaikh, M.; Rahman, R.M.; Zaidi, Z.A. Telesurgery and Robotics: An Improved and Efficient Era. Cureus 2021, 13, e14124. [Google Scholar] [CrossRef] [PubMed]
- Marescaux, J.; Leroy, J.; Gagner, M.; Rubino, F.; Mutter, D.; Vix, M.; Butner, S.E.; Smith, M.K. Transatlantic robot-assisted telesurgery. Nature 2001, 413, 379–380. [Google Scholar] [CrossRef] [PubMed]
- McBride, K.; Steffens, D.; Stanislaus, C.; Solomon, M.; Anderson, T.; Thanigasalam, R.; Leslie, S.; Bannon, P.G. Detailed cost of robotic-assisted surgery in the Australian public health sector: From implementation to a multi-specialty caseload. BMC Health Serv. Res. 2021, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Care Excellence (NICE). Prostate Cancer: Diagnosis and Management. NICE Guidance 131. Available online: https://www.nice.org.uk/guidance/ng131 (accessed on 14 November 2022).
- Forsmark, A.; Gehrman, J.; Angenete, E.; Bjartell, A.; Björholt, I.; Carlsson, S.; Hugosson, J.; Marlow, T.; Stinesen-Kollberg, K.; Stranne, J.; et al. Health Economic Analysis of Open and Robot-assisted Laparoscopic Surgery for Prostate Cancer Within the Prospective Multicentre LAPPRO Trial. Eur. Urol. 2018, 74, 816–824. [Google Scholar] [CrossRef] [Green Version]
- Bijlani, A.; Hebert, A.E.; Davitian, M.; May, H.; Speers, M.; Leung, R.; Mohamed, N.E.; Sacks, H.S.; Tewari, A. A Multidimensional Analysis of Prostate Surgery Costs in the United States: Robotic-Assisted versus Retropubic Radical Prostatectomy. Value Health 2016, 19, 391–403. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Cheng, L.; Li, Y.; Kreaden, U.; Snyder, S.R. Systematic literature review of cost-effectiveness analyses of robotic-assisted radical prostatectomy for localised prostate cancer. BMJ Open 2022, 12, e058394. [Google Scholar] [CrossRef]
- Mjaess, G.; Diamand, R.; Aoun, F.; Assenmacher, G.; Assenmacher, C.; Verhoest, G.; Holz, S.; Naudin, M.; Ploussard, G.; Mari, A.; et al. Cost-analysis of robot-assisted radical cystectomy in Europe: A cross-country comparison. Eur. J. Surg. Oncol. 2022, S0748–S07983, 00584-4. [Google Scholar] [CrossRef]
- Hague, C.M.; Merrill, S.B. Integration of Robotics in Urology Residency Programs: An Unchecked Technological Revolution. Curr. Urol. Rep. 2021, 22, 47. [Google Scholar] [CrossRef]
- Butterworth, J.; Sadry, M.; Julian, D.; Haig, F. Assessment of the training program for Versius, a new innovative robotic system for use in minimal access surgery. BMJ Surg. Interv. Health Technol. 2021, 18, e000057. [Google Scholar] [CrossRef]
- Spampinato, G.; Binet, A.; Fourcade, L.; Mendoza Sagaon, M.; Villemagne, T.; Braik, K.; Grosos, C.; Lardy, H.; Ballouhey, Q. Comparison of the Learning Curve for Robot-Assisted Laparoscopic Pyeloplasty Between Senior and Junior Surgeons. J. Laparoendosc. Adv. Surg. Technol. 2021, 31, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Morozov, A.; Babaevskaya, D.; Taratkin, M.; Inoyatov, J.; Laukhtina, E.; Moschini, M.; Singla, N.; Gomez Rivas, J.; Teoh, J.Y.; Glybochko, P.; et al. Systematic Review: The Learning Curve for Robot-Assisted Radical Cystectomy—What Do We Know? J. Endourol. 2022, 36, 770–784. [Google Scholar] [CrossRef] [PubMed]
- Dixon, F.; Keeler, B.D. Robotic surgery: Training, competence assessment and credentialising. Bull. R Coll. Surg. Eng. 2020, 102, 302–306. [Google Scholar] [CrossRef]
- Nayyar, R.; Yadav, S.; Singh, P.; Dogra, P.N. Impact of assistant surgeon on outcomes in robotic surgery. Indian J. Urol. 2016, 32, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Ferrarese, A.; Pozzi, G.; Borghi, F.; Marano, A.; Delbon, P.; Amato, B.; Santangelo, M.; Buccelli, C.; Niola, M.; Martino, V.; et al. Malfunctions of robotic system in surgery: Role and responsibility of surgeon in legal point of view. Open Med. 2016, 11, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.H.; Jang, W.S.; Park, J.W.; Ham, S.K.; Han, W.K.; Rha, K.H.; Choi, Y.F. Efficacy and Safety of Robotic Procedures Performed Using the da Vinci Robotic Surgical System at a Single Institute in Korea: Experience with 10000 Cases. Yonsei Med. J. 2018, 59, 975–981. [Google Scholar] [CrossRef]
- Maerz, D.A.; Beck, L.N.; Sim, A.J.; Gainsburg, D.M. Complications of robotic-assisted laparoscopic surgery distant from the surgical site. BJA Br. J. Anaesth. 2017, 118, 492–503. [Google Scholar] [CrossRef] [Green Version]
- Wen, T.; Deibert, C.M.; Siringo, F.S.; Spencer, B.A. Positioning-related complications of minimally invasive radical prostatectomies. J. Endourol. 2014, 28, 660–667. [Google Scholar] [CrossRef]
- Aceto, P.; Beretta, L.; Cariello, C.; Claroni, C.; Esposito, C.; Forastiere, E.M.; Guarracino, F.; Perucca, R.; Romagnoli, S.; Sollazzi, L.; et al. Joint consensus on anesthesia in urologic and gynecologic robotic surgery: Specific issues in management from a task force of the SIAARTI, SIGO, and SIU. Minerva Anestesiol. 2019, 85, 871–885. [Google Scholar] [CrossRef]
- Shoham, M.A.; Baker, N.M.; Peterson, M.E.; Fox, P. The environmental impact of surgery: A systematic review. Surgery 2022, 172, 897–905. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Kumar, N.S.; Vanhoestenberghe, A.; Francis, N.K. Environmental sustainability in robotic and laparoscopic surgery: Systematic review. Br. J. Surg. 2022, 109, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Fleming, C.A.; Fullard, A.; Croghan, S.; Pellino, G.; Pata, F. Robotic abdominal surgery and COVID-19: A systematic review of published literature and peer-reviewed guidelines during the SARS-CoV-2 Pandemic. J. Clin. Med. 2022, 11, 2957. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, T.; Rai, B.; Madaan, S.; Chedgy, E.; Somani, B. The Availability, Cost, Limitations, Learning Curve and Future of Robotic Systems in Urology and Prostate Cancer Surgery. J. Clin. Med. 2023, 12, 2268. https://doi.org/10.3390/jcm12062268
Hughes T, Rai B, Madaan S, Chedgy E, Somani B. The Availability, Cost, Limitations, Learning Curve and Future of Robotic Systems in Urology and Prostate Cancer Surgery. Journal of Clinical Medicine. 2023; 12(6):2268. https://doi.org/10.3390/jcm12062268
Chicago/Turabian StyleHughes, Thomas, Bhavan Rai, Sanjeev Madaan, Edmund Chedgy, and Bhaskar Somani. 2023. "The Availability, Cost, Limitations, Learning Curve and Future of Robotic Systems in Urology and Prostate Cancer Surgery" Journal of Clinical Medicine 12, no. 6: 2268. https://doi.org/10.3390/jcm12062268