

The Effects of SGLT2 Inhibitors on Liver Cirrhosis Patients with Refractory Ascites: A Literature Review

Abstract
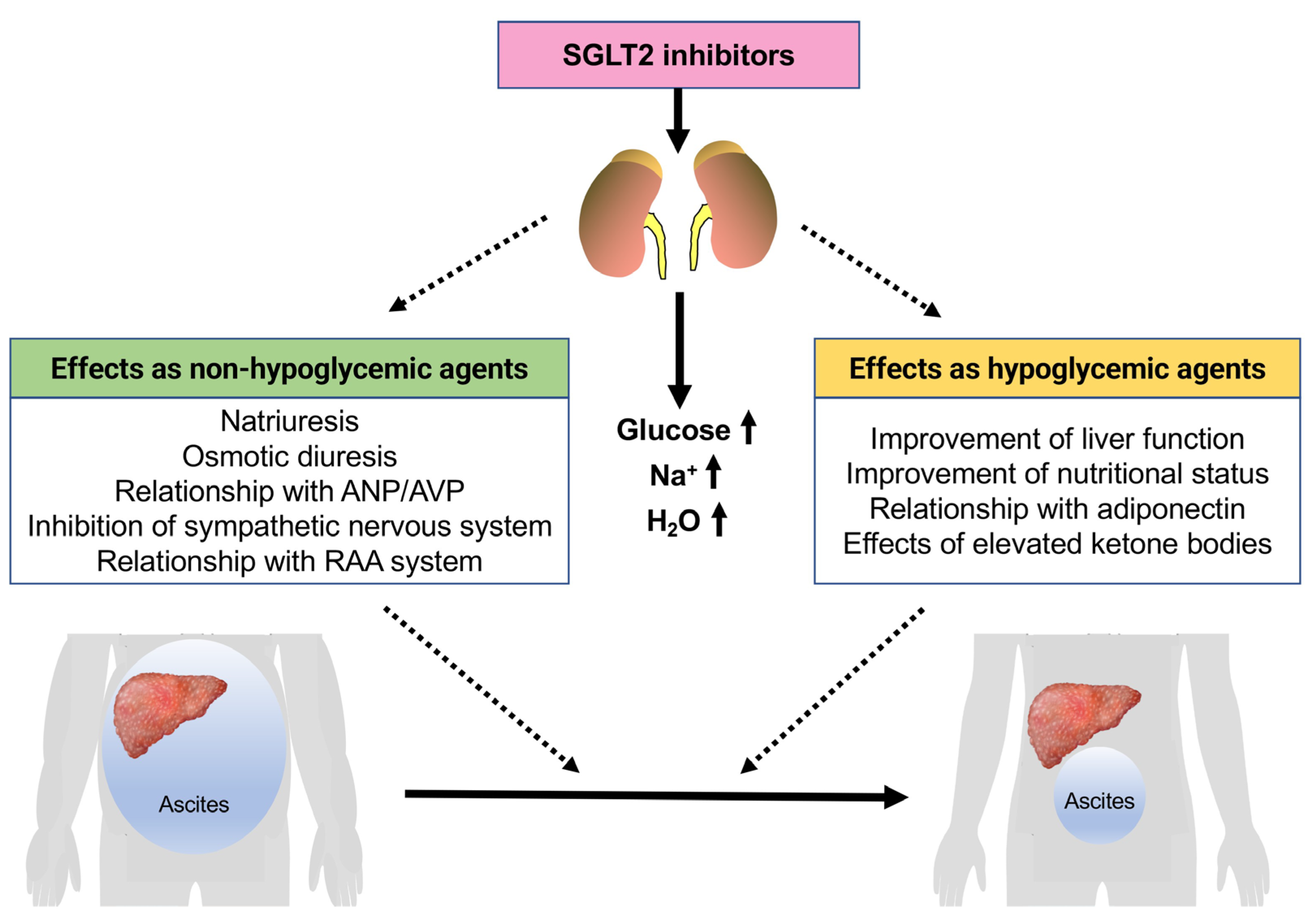
:1. Introduction
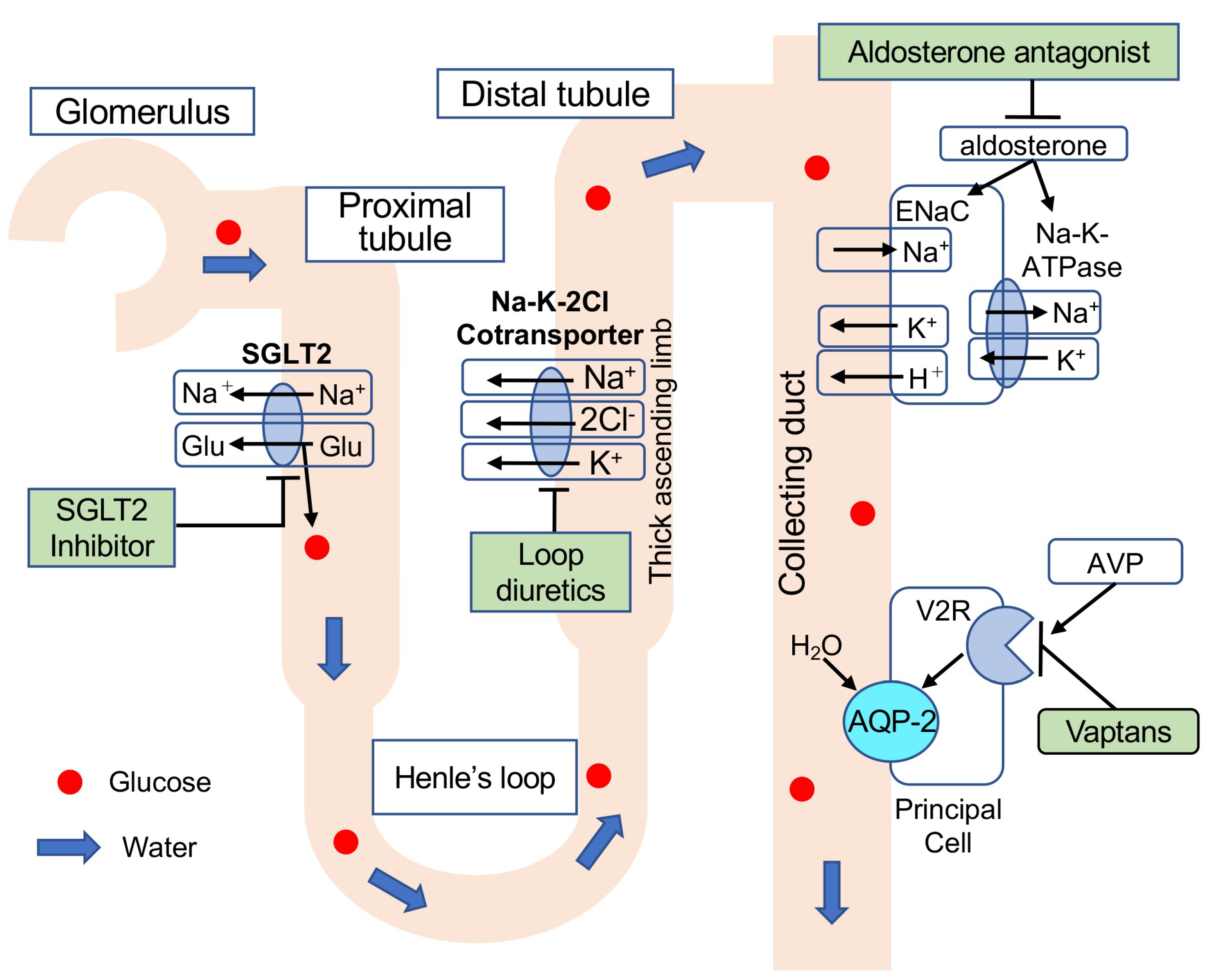
2. SGLT2 Inhibitors as Diuretics
3. Effects of SGLT2 Inhibitors on Serum Sodium Levels
4. Comparison of SGLT2 Inhibitors and Vaptans
5. Effects on the Sympathetic Nervous and RAA Systems
6. Effects on Liver Function and Nutritional Status
7. Effects on Adiponectin
8. Effects on Ketone Bodies
9. Impact of SGLT2 Inhibitors on the Renal Function
10. Conclusions and Future Perspectives
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ginés, P.; Quintero, E.; Arroyo, V.; Terés, J.; Bruguera, M.; Rimola, A.; Caballería, J.; Rodés, J.; Rozman, C. Compensated cirrhosis: Natural history and prognostic factors. Hepatology 1987, 7, 122–128. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef] [PubMed]
- Kozaki, K.; Iinuma, M.; Takagi, T.; Fukuda, T.; Sanpei, T.; Terunuma, Y.; Yatabe, Y.; Akano, K. Cell-Free and Concentrated Ascites Reinfusion Therapy for Decompensated Liver Cirrhosis. Ther. Apher. Dial. 2016, 20, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; Von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Herrington, W.G.; Staplin, N.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; Ng, S.Y.A.; et al.; Empa-Kidney Collaborative Group Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2022, 388, 117–127. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Vallon, V.; Verma, S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu. Rev. Physiol. 2021, 83, 503–528. [Google Scholar] [CrossRef]
- Masuda, T.; Muto, S.; Fukuda, K.; Watanabe, M.; Ohara, K.; Koepsell, H.; Vallon, V.; Nagata, D. Osmotic diuresis by SGLT2 inhibition stimulates vasopressin-induced water reabsorption to maintain body fluid volume. Physiol. Rep. 2020, 8, e14360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, X.; Verma, S.; Yun, J.; Brand-Arzamendi, K.; Singh, K.K.; Liu, X.; Garg, A.; Quan, A.; Wen, X.-Y. Effect of empagliflozin on cardiac biomarkers in a zebrafish model of heart failure: Clues to the EMPA-REG OUTCOME trial? Mol. Cell. Biochem. 2017, 433, 97–102. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, L.; Yuan, L.; Li, D.; Zhang, Y.; Zheng, R.; Liu, C.; Feng, X.; Li, Q.; Ma, J. Sodium-glucose co-transporter-2 inhibitors suppress atrial natriuretic peptide secretion in patients with newly diagnosed Type 2 diabetes. Diabet. Med. 2016, 33, 1732–1736. [Google Scholar] [CrossRef]
- Kim, Y.; Babu, A.R. Clinical potential of sodium-glucose cotransporter 2 inhibitors in the management of type 2 diabetes. Diabetes Metab. Syndr. Obes. 2012, 5, 313–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallon, V.; Thomson, S.C. Targeting renal glucose reabsorption to treat hyperglycaemia: The pleiotropic effects of SGLT2 inhibition. Diabetologia 2017, 60, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, S.P.; Jowett, T.P.; Slater, J.D.; Arroyo, V.; Moodie, H.; Williams, R. Renal sodium retention in cirrhosis: Relation to aldosterone and nephron site. Clin. Sci. 1979, 56, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, Y.; Honda, A.; Yokose, S.; Nagata, M.; Miyamoto, J. Weaning from concentrated ascites reinfusion therapy for refractory ascites by SGLT2 inhibitor. Clin. Kidney J. 2022, 15, 831–833. [Google Scholar] [CrossRef]
- Kalambokis, G.N.; Tsiakas, I.; Filippas-Ntekuan, S.; Christaki, M.; Despotis, G.; Milionis, H. Empagliflozin Eliminates Refractory Ascites and Hepatic Hydrothorax in a Patient with Primary Biliary Cirrhosis. Am. J. Gastroenterol. 2021, 116, 618–619. [Google Scholar] [CrossRef] [PubMed]
- Montalvo-Gordon, I.; Chi-Cervera, L.A.; Garcia-Tsao, G. Sodium-Glucose Cotransporter 2 Inhibitors Ameliorate Ascites and Peripheral Edema in Patients with Cirrhosis and Diabetes. Hepatology 2020, 72, 1880–1882. [Google Scholar] [CrossRef] [PubMed]
- Refardt, J.; Imber, C.; Sailer, C.O.; Jeanloz, N.; Potasso, L.; Kutz, A.; Widmer, A.; Urwyler, S.A.; Ebrahimi, F.; Vogt, D.R.; et al. A Randomized Trial of Empagliflozin to Increase Plasma Sodium Levels in Patients with the Syndrome of Inappropriate Antidiuresis. J. Am. Soc. Nephrol. 2020, 31, 615–624. [Google Scholar] [CrossRef]
- Boorsma, E.M.; Beusekamp, J.C.; ter Maaten, J.M.; Figarska, S.M.; Danser, A.J.; van Veldhuisen, D.J.; van der Meer, P.; Heerspink, H.J.; Damman, K.; Voors, A.A. Effects of empagliflozin on renal sodium and glucose handling in patients with acute heart failure. Eur. J. Heart Fail. 2021, 23, 68–78. [Google Scholar] [CrossRef]
- Guevara, M.; Baccaro, M.E.; Torre, A.; Gómez-Ansón, B.; Ríos, J.; Torres, F.; Rami, L.; Monté-Rubio, G.C.; Martín-Llahí, M.; Arroyo, V.; et al. Hyponatremia is a risk factor of hepatic encephalopathy in patients with cirrhosis: A prospective study with time-dependent analysis. Am. J. Gastroenterol. 2009, 104, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Londoño, M.-C.; Cardenas, A.; Guevara, M.; Quintó, L.; Heras, D.D.L.; Navasa, M.; Rimola, A.; Garcia-Valdecasas, J.-C.; Arroyo, V.; Ginès, P. MELD score and serum sodium in the prediction of survival of patients with cirrhosis awaiting liver transplantation. Gut 2007, 56, 1283–1290. [Google Scholar] [CrossRef] [Green Version]
- Portales-Castillo, I.; Sterns, R.H. Allostasis and the Clinical Manifestations of Mild to Moderate Chronic Hyponatremia: No Good Adaptation Goes Unpunished. Am. J. Kidney Dis. 2019, 73, 391–399. [Google Scholar] [CrossRef]
- Ohara, K.; Masuda, T.; Morinari, M.; Okada, M.; Miki, A.; Nakagawa, S.; Murakami, T.; Oka, K.; Asakura, M.; Miyazawa, Y.; et al. The extracellular volume status predicts body fluid response to SGLT2 inhibitor dapagliflozin in diabetic kidney disease. Diabetol. Metab. Syndr. 2020, 12, 37. [Google Scholar] [CrossRef]
- Weir, M.R.; Kline, I.; Xie, J.; Edwards, R.; Usiskin, K. Effect of canagliflozin on serum electrolytes in patients with type 2 diabetes in relation to estimated glomerular filtration rate (eGFR). Curr. Med. Res. Opin. 2014, 30, 1759–1768. [Google Scholar] [CrossRef]
- Bailey, C.J.; Iqbal, N.; T’Joen, C.; List, J.F. Dapagliflozin monotherapy in drug-naive patients with diabetes: A randomized-controlled trial of low-dose range. Diabetes Obes. Metab. 2012, 14, 951–959. [Google Scholar] [CrossRef]
- Scheen, A.J. Pharmacodynamics, efficacy and safety of sodium-glucose co-transporter type 2 (SGLT2) inhibitors for the treatment of type 2 diabetes mellitus. Drugs 2015, 75, 33–59. [Google Scholar] [CrossRef]
- Seman, L.; Macha, S.; Nehmiz, G.; Simons, G.; Ren, B.; Pinnetti, S.; Woerle, H.J.; Dugi, K. Empagliflozin (BI 10773), a Potent and Selective SGLT2 Inhibitor, Induces Dose-Dependent Glucosuria in Healthy Subjects. Clin. Pharmacol. Drug Dev. 2013, 2, 152–161. [Google Scholar] [CrossRef]
- Refardt, J.; Winzeler, B.; Meienberg, F.; Vogt, D.R.; Christ-Crain, M. Empagliflozin Increases Short-Term Urinary Volume Output in Artificially Induced Syndrome of Inappropriate Antidiuresis. Int. J. Endocrinol. 2017, 2017, 7815690. [Google Scholar] [CrossRef] [Green Version]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogiso, T.; Yamamoto, K.; Kobayashi, M.; Ikarashi, Y.; Kodama, K.; Taniai, M.; Torii, N.; Hashimoto, E.; Tokushige, K. Response to tolvaptan and its effect on prognosis in cirrhotic patients with ascites. Hepatol. Res. 2017, 47, 835–844. [Google Scholar] [CrossRef]
- Yi, J.H.; Shin, H.J.; Kim, H.J. V2 receptor antagonist; tolvaptan. Electrolytes Blood Press. 2011, 9, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiramine, Y.; Uto, H.; Mawatari, S.; Kanmura, S.; Imamura, Y.; Hiwaki, T.; Saishoji, A.; Yada, T.; Inada, Y.; Sakamoto, H.; et al. Effect of tolvaptan on the prognosis of patients with hepatic ascites. Hepatol. Res. 2019, 49, 765–777. [Google Scholar] [CrossRef]
- Dahl, E.; Gluud, L.L.; Kimer, N.; Krag, A. Meta-analysis: The safety and efficacy of vaptans (tolvaptan, satavaptan and lixivaptan) in cirrhosis with ascites or hyponatraemia. Aliment. Pharmacol. Ther. 2012, 36, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Vasilakou, D.; Karagiannis, T.; Athanasiadou, E.; Mainou, M.; Liakos, A.; Bekiari, E.; Sarigianni, M.; Matthews, D.R.; Tsapas, A. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 262–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.H.; Bohm, N.; Nemecek, B.D.; Crawford, R.; Kelley, D.; Bhasin, B.; Nietert, P.J.; Velez, J.C.Q. Rapidity of Correction of Hyponatremia Due to Syndrome of Inappropriate Secretion of Antidiuretic Hormone Following Tolvaptan. Am. J. Kidney Dis. 2018, 71, 772–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasichayanula, S.; Liu, X.; Zhang, W.; Pfister, M.; LaCreta, F.P.; Boulton, D.W. Influence of hepatic impairment on the pharmacokinetics and safety profile of dapagliflozin: An open-label, parallel-group, single-dose study. Clin. Ther. 2011, 33, 1798–1808. [Google Scholar] [CrossRef]
- Bichet, D.G.; Van Putten, V.J.; Schrier, R.W. Potential role of increased sympathetic activity in impaired sodium and water excretion in cirrhosis. N. Engl. J. Med. 1982, 307, 1552–1557. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, K.M.; Shapiro, M.D.; Van Putten, V.J.; Kluge, R.; Chung, H.M.; Bichet, D.G.; Schrier, R.W. Elevated plasma norepinephrine concentrations in decompensated cirrhosis. Association with increased secretion rates, normal clearance rates, and suppressibility by central blood volume expansion. Circ. Res. 1985, 56, 457–461. [Google Scholar] [CrossRef] [Green Version]
- Schlager, G.; Sides, J. Characterization of hypertensive and hypotensive inbred strains of mice. Lab. Anim. Sci. 1997, 47, 288–292. [Google Scholar] [PubMed]
- Davern, P.J.; Nguyen-Huu, T.P.; La Greca, L.; Abdelkader, A.; Head, G.A. Role of the sympathetic nervous system in Schlager genetically hypertensive mice. Hypertension 2009, 54, 852–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herat, L.; Magno, A.; Rudnicka, C.; Hricova, J.; Carnagarin, R.; Ward, N.; Arcambal, A.; Kiuchi, M.G.; Head, G.; Schlaich, M.P.; et al. SGLT2 Inhibitor-Induced Sympathoinhibition: A Novel Mechanism for Cardiorenal Protection. JACC Basic Transl. Sci. 2020, 5, 169–179. [Google Scholar] [CrossRef]
- Schlaich, M.; Straznicky, N.; Lambert, E.; Lambert, G. Metabolic syndrome: A sympathetic disease? Lancet Diabetes Endocrinol. 2015, 3, 148–157. [Google Scholar] [CrossRef]
- Thorp, A.A.; Schlaich, M.P. Relevance of Sympathetic Nervous System Activation in Obesity and Metabolic Syndrome. J. Diabetes Res. 2015, 2015, 341583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmerly, D.S.; Shoemaker, J.K. Hypovolemia and neurovascular control during orthostatic stress. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H645–H655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, J.; Tank, J.; Heusser, K.; Heise, T.; Wanner, C.; Heer, M.; Macha, S.; Mattheus, M.; Lund, S.S.; Woerle, H.J.; et al. The effect of empagliflozin on muscle sympathetic nerve activity in patients with type II diabetes mellitus. J. Am. Soc. Hypertens. 2017, 11, 604–612. [Google Scholar] [CrossRef]
- Wong, F.; Sniderman, K.; Blendis, L. The renal sympathetic and renin-angiotensin response to lower body negative pressure in well-compensated cirrhosis. Gastroenterology 1998, 115, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Trevisani, F.; Santini, C.; De Palma, R.; Gasbarrini, G. Aldosterone related blood volume expansion in cirrhosis before and during the early phase of ascites formation. Gut 1983, 24, 761–766. [Google Scholar] [CrossRef] [Green Version]
- Isshiki, M.; Sakuma, I.; Hayashino, Y.; Sumita, T.; Hara, K.; Takahashi, K.; Shiojima, I.; Satoh-Asahara, N.; Kitazato, H.; Ito, D.; et al. Effects of dapagliflozin on renin-angiotensin-aldosterone system under renin-angiotensin system inhibitor administration. Endocr. J. 2020, 67, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.; Perkins, B.A.; Soleymanlou, N.; Maione, M.; Lai, V.; Lee, A.; Fagan, N.M.; Woerle, H.J.; Johansen, O.E.; Broedl, U.C.; et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation 2014, 129, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Lambers Heerspink, H.J.; de Zeeuw, D.; Wie, L.; Leslie, B.; List, J. Dapagliflozin a glucose-regulating drug with diuretic properties in subjects with type 2 diabetes. Diabetes Obes. Metab. 2013, 15, 853–862. [Google Scholar] [CrossRef] [Green Version]
- Heise, T.; Jordan, J.; Wanner, C.; Heer, M.; Macha, S.; Mattheus, M.; Lund, S.S.; Woerle, H.J.; Broedl, U.C. Acute Pharmacodynamic Effects of Empagliflozin with and without Diuretic Agents in Patients with Type 2 Diabetes Mellitus. Clin. Ther. 2016, 38, 2248–2264.e5. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [Green Version]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Lopez-Larramona, G.; Lucendo, A.J.; Tenias, J.M. Association between nutritional screening via the Controlling Nutritional Status index and bone mineral density in chronic liver disease of various etiologies. Hepatol. Res. 2015, 45, 618–628. [Google Scholar] [CrossRef]
- Zhang, X.; Harmsen, W.S.; Mettler, T.A.; Kim, W.R.; Roberts, R.O.; Therneau, T.M.; Roberts, L.R.; Chaiteerakij, R. Continuation of metformin use after a diagnosis of cirrhosis significantly improves survival of patients with diabetes. Hepatology 2014, 60, 2008–2016. [Google Scholar] [CrossRef] [Green Version]
- Elkrief, L.; Rautou, P.E.; Sarin, S.; Valla, D.; Paradis, V.; Moreau, R. Diabetes mellitus in patients with cirrhosis: Clinical implications and management. Liver Int. 2016, 36, 936–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamauchi, T.; Kamon, J.; Waki, H.; Terauchi, Y.; Kubota, N.; Hara, K.; Mori, Y.; Ide, T.; Murakami, K.; Tsuboyama-Kasaoka, N.; et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat. Med. 2001, 7, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, T.; Kamon, J.; Minokoshi, Y.; Ito, Y.; Waki, H.; Uchida, S.; Yamashita, S.; Noda, M.; Kita, S.; Ueki, K.; et al. Adiponectin stimulates glucose utilization and fatty-acid oxidation by activating AMP-activated protein kinase. Nat. Med. 2002, 8, 1288–1295. [Google Scholar] [CrossRef]
- Garvey, W.T.; Van Gaal, L.; Leiter, L.A.; Vijapurkar, U.; List, J.; Cuddihy, R.; Ren, J.; Davies, M.J. Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type 2 diabetes. Metabolism 2018, 85, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Shiba, K.; Tsuchiya, K.; Komiya, C.; Miyachi, Y.; Mori, K.; Shimazu, N.; Yamaguchi, S.; Ogasawara, N.; Katoh, M.; Itoh, M.; et al. Canagliflozin, an SGLT2 inhibitor, attenuates the development of hepatocellular carcinoma in a mouse model of human NASH. Sci. Rep. 2018, 8, 2362. [Google Scholar] [CrossRef] [Green Version]
- Kothari, S.; Dhami-Shah, H.; Shah, S.R. Antidiabetic Drugs and Statins in Nonalcoholic Fatty Liver Disease. J. Clin. Exp. Hepatol. 2019, 9, 723–730. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.M.; Berard, L.D.; Cheng, A.Y.; Gilbert, J.D.; Verma, S.; Woo, V.C.; Yale, J.-F. SGLT2 Inhibitor-associated Diabetic Ketoacidosis: Clinical Review and Recommendations for Prevention and Diagnosis. Clin Ther. 2016, 38, 2654–2664.e1. [Google Scholar] [CrossRef] [PubMed]
- Mudaliar, S.; Henry, R.R.; Boden, G.; Smith, S.; Chalamandaris, A.-G.; Duchesne, D.; Iqbal, N.; List, J. Changes in insulin sensitivity and insulin secretion with the sodium glucose cotransporter 2 inhibitor dapagliflozin. Diabetes Technol. Ther. 2014, 16, 137–144. [Google Scholar] [CrossRef]
- Puchalska, P.; Crawford, P.A. Multi-dimensional Roles of Ketone Bodies in Fuel Metabolism, Signaling, and Therapeutics. Cell. Metab. 2017, 25, 262–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, H.; Novikov, A.; Vallon, V. Ketosis and diabetic ketoacidosis in response to SGLT2 inhibitors: Basic mechanisms and therapeutic perspectives. Diabetes Metab. Res. Rev. 2017, 33, e2886. [Google Scholar] [CrossRef]
- Juge, N.; Gray, J.A.; Omote, H.; Miyaji, T.; Inoue, T.; Hara, C.; Uneyama, H.; Edwards, R.H.; Nicoll, R.A.; Moriyama, Y. Metabolic control of vesicular glutamate transport and release. Neuron 2010, 68, 99–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, Y.; Hiasa, M.; Sakamoto, S.; Omote, H.; Nomura, M. Vesicular nucleotide transporter (VNUT): Appearance of an actress on the stage of purinergic signaling. Purinergic Signal. 2017, 13, 387–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasuzawa, N.; Moriyama, S.; Moriyama, Y.; Nomura, M. Physiopathological roles of vesicular nucleotide transporter (VNUT), an essential component for vesicular ATP release. Biochim. Biophys Acta Biomembr. 2020, 1862, 183408. [Google Scholar] [CrossRef]
- Sakamoto, S.; Miyaji, T.; Hiasa, M.; Ichikawa, R.; Uematsu, A.; Iwatsuki, K.; Shibata, A.; Uneyama, H.; Takayanagi, R.; Yamamoto, A.; et al. Impairment of vesicular ATP release affects glucose metabolism and increases insulin sensitivity. Sci. Rep. 2014, 4, 6689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsushima, K.; Hasuzawa, N.; Wang, L.; Hiasa, M.; Sakamoto, S.; Ashida, K.; Sudo, N.; Moriyama, Y.; Nomura, M. Vesicular ATP release from hepatocytes plays a role in the progression of nonalcoholic steatohepatitis. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166013. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre | 1 Week | 1 Month | 3 Months | 4 Months | 6 Months | 9 Months | ||
|---|---|---|---|---|---|---|---|---|
| Patient 1 [23] Age: 63 Sex: Female SGLT2-I: Empagliflozin Etiology: NASH | Body weight (kg) | 63 | 58.2 | 58.2 | 57.9 | 58.1 | ||
| Serum Na/K (mEq/L) | 139/4.2 | 140/4.2 | 137/4.3 | 136/4.6 | 135/4.3 | |||
| Serum albumin (g/dL) | 2.84 | 2.86 | 2.71 | 2.5 | 2.88 | |||
| Serum creatinine (mg/dL) | 0.7 | 0.72 | 0.78 | 0.78 | 0.87 | |||
| Platelets (×104/μL) | 10.2 | 10.3 | 10.4 | 9.9 | 9.9 | |||
| Fasting glucose (mg/dL) | 86 | 87 | 85 | 73 | 90 | |||
| Patient 2 [23] Age: 64 Sex: Female SGLT2-I: Canagliflozin Etiology: NASH | Body weight (kg) | 81.1 | 80.7 | 74.8 | 73.3 | 69.9 | ||
| Serum Na/K (mEq/L) | 120/4.1 | 140/5.2 | 138/4.5 | 145/4.3 | 141/4.7 | |||
| Serum albumin (g/dL) | 3.5 | N/A | 3.5 | 3.68 | 3.38 | |||
| Serum creatinine (mg/dL) | 0.7 | 1.00 | 0.80 | 0.81 | 0.86 | |||
| Platelets (×104/μL) | 6.8 | N/A | 7.0 | 6.6 | 7.8 | |||
| Fasting glucose (mg/dL) | 140 | 91 | 140 | 141 | 121 | |||
| Patient 3 [23] Age: 53 Sex: Male SGLT2-I: Canagliflozin Etiology: NASH | Body weight (kg) | 57.6 | 55.7 | 53.5 | 51.9 | 51.0 | ||
| Serum Na/K (mEq/L) | 135/4.9 | 139/4.7 | 139/4.5 | 139/4.5 | 145/4.4 | |||
| Serum albumin (g/dL) | 3.4 | 3.1 | 3.2 | 3.4 | 3.6 | |||
| Serum creatinine (mg/dL) | 1.80 | 1.24 | 1.00 | 1.04 | 0.90 | |||
| Platelets (×104/μL) | 11.1 | 16.6 | 10.5 | 6.6 | 9.9 | |||
| Fasting glucose (mg/dL) | 187 | 123 | 130 | 119 | 150 | |||
| Patient 4 [22] Age: 54 Sex: Female SGLT2-I: Empagliflozin Etiology: PBC | Body weight (kg) | |||||||
| Serum Na/K (mEq/L) | 133/4.39 | 136/4.42 | 139/4.1 | 140/3.71 | ||||
| Serum albumin (g/dL) | 3.1 | 2.9 | 3.5 | 3.7 | ||||
| Serum creatinine (mg/dL) | 0.84 | 0.77 | 0.60 | 0.55 | ||||
| Platelets (×104/μL) | ||||||||
| Fasting glucose (mg/dL) | 286 | 165 | 137 | 116 | ||||
| HbA1c (%) | 6.6 | 5.8 | ||||||
| Child–Pugh score | 8 | 8 | 6 | 5 | ||||
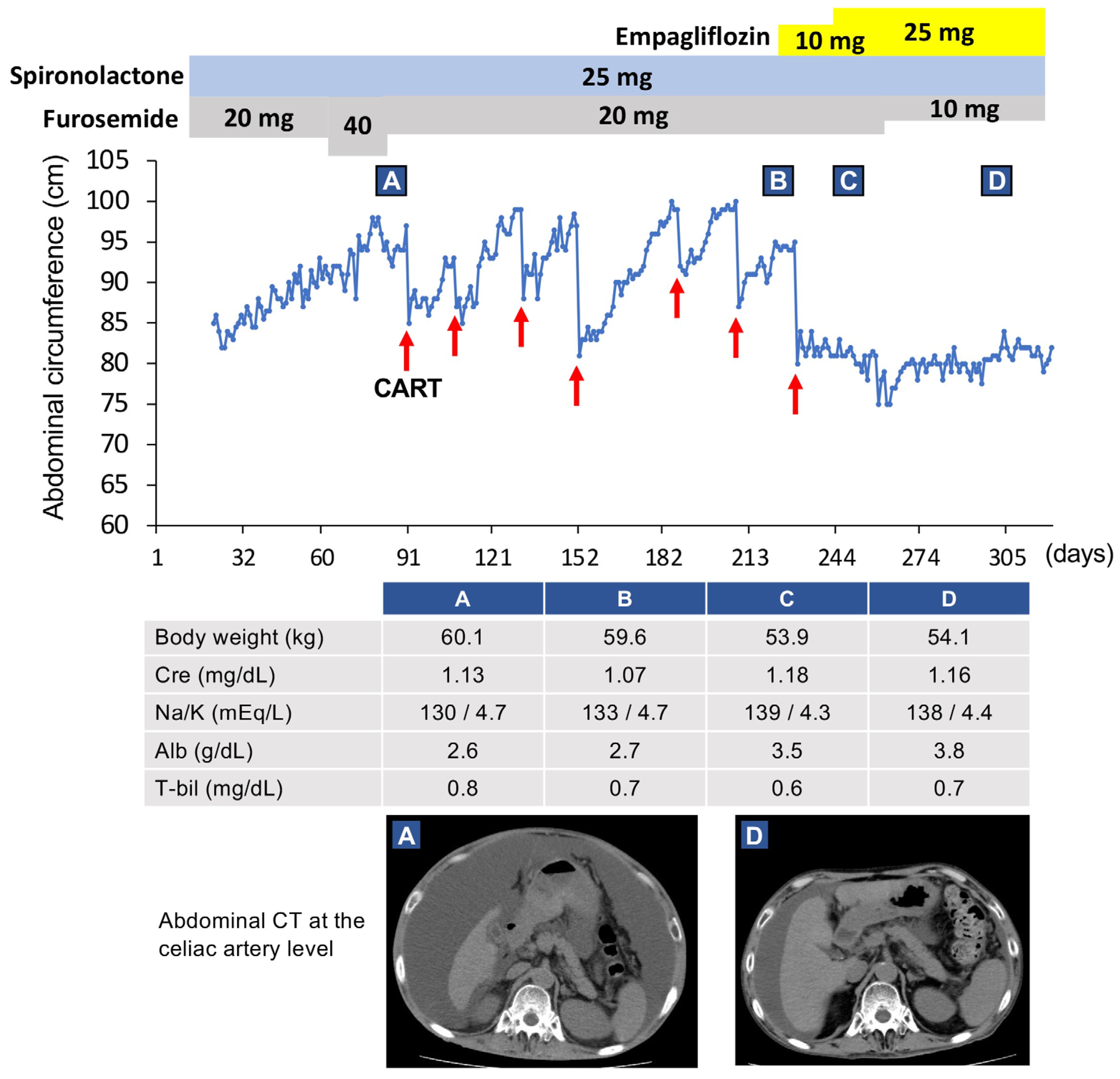
| Patient 5 [21] Age: 59 Sex: Male SGLT2-I: Empagliflozin Etiology: Alcohol | Body weight (kg) | 59.6 | 53.8 | 54.9 | 54.1 | 55.2 | 55.4 | 54.7 |
| Serum Na/K (mEq/L) | 133/4.7 | 136/4.1 | 139/4.3 | 138/4.4 | 137/4.5 | 141/4.4 | 141/4.6 | |
| Serum albumin (g/dL) | 2.7 | 3.3 | 3.5 | 3.8 | 3.8 | 4.0 | 4.4 | |
| Serum creatinine (mg/dL) | 1.07 | 1.10 | 1.18 | 1.16 | 1.24 | 1.18 | 1.16 | |
| Platelets (×104/μL) | 8.8 | 8.2 | 9.3 | 10.1 | 9.8 | 10.7 | 12.8 | |
| Fasting glucose (mg/dL) | 125 | 183 | 144 | 129 | 107 | 137 | 104 | |
| HbA1c (%) | 7.5 | 7.2 | 6.4 | 6.5 | 6.5 | 6.1 | ||
| ChE (IU/L) | 45 | 72 | 82 | 89 | 93 | 112 | ||
| Child–Pugh score | 10 | 7 | 7 | 6 | 6 | 6 | 6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyamoto, Y.; Honda, A.; Yokose, S.; Nagata, M.; Miyamoto, J. The Effects of SGLT2 Inhibitors on Liver Cirrhosis Patients with Refractory Ascites: A Literature Review. J. Clin. Med. 2023, 12, 2253. https://doi.org/10.3390/jcm12062253
Miyamoto Y, Honda A, Yokose S, Nagata M, Miyamoto J. The Effects of SGLT2 Inhibitors on Liver Cirrhosis Patients with Refractory Ascites: A Literature Review. Journal of Clinical Medicine. 2023; 12(6):2253. https://doi.org/10.3390/jcm12062253
Chicago/Turabian StyleMiyamoto, Yasunori, Akira Honda, Seiji Yokose, Mariko Nagata, and Jiro Miyamoto. 2023. "The Effects of SGLT2 Inhibitors on Liver Cirrhosis Patients with Refractory Ascites: A Literature Review" Journal of Clinical Medicine 12, no. 6: 2253. https://doi.org/10.3390/jcm12062253