
Evaluation of Change in Radiographic Fractal Dimension around Dental Implants Placed with Low-Speed Drilling and Standard Drilling Protocols
 ,
,  , and
, and 
Abstract
:1. Introduction
- Osteoconduction: phase in which a bed of connective tissue and blood coagulation appears around the implant, which will mature over time into granulation tissue.
- Modeling: osteoclasts begin to appear, gradually reabsorbing the avascular bone. At the same time, the connective tissue rich in vessels will mature forming an osteoid that will form the reticular bone.
- Remodeling: the reticular bone is replaced by lamellar bone and bone marrow, with the intervention of osteoclasts. By the eighth week, all the original bone portions will have been replaced by new bone [2].
2. Materials and Methods
2.1. Design of the Study
2.2. Type of Sample, Inclusion and Exclusion Criteria
- Low-speed drilling without irrigation: 50 rpm.
- Conventional drilling with irrigation: 800 rpm.
- Patients of legal age and not pregnant.
- Patients who do not present pathologies that affect the bone.
- Insufficient quality images.
- Not having pre and post implants images.
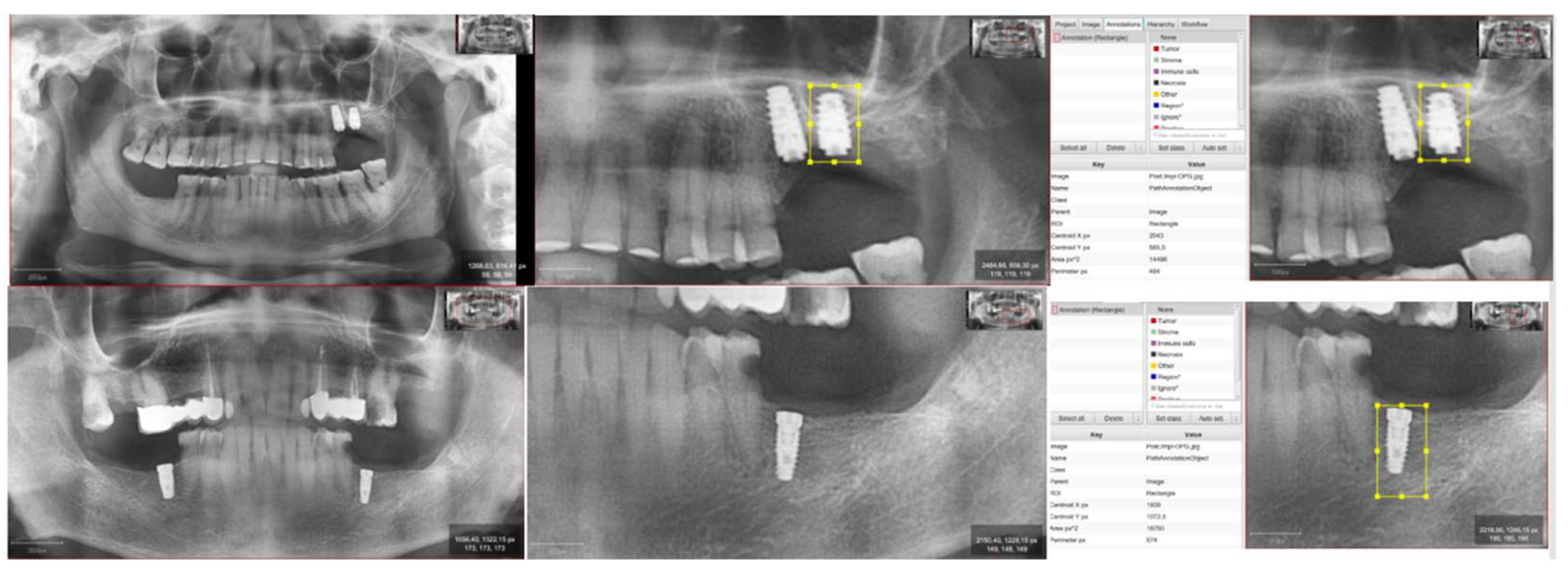
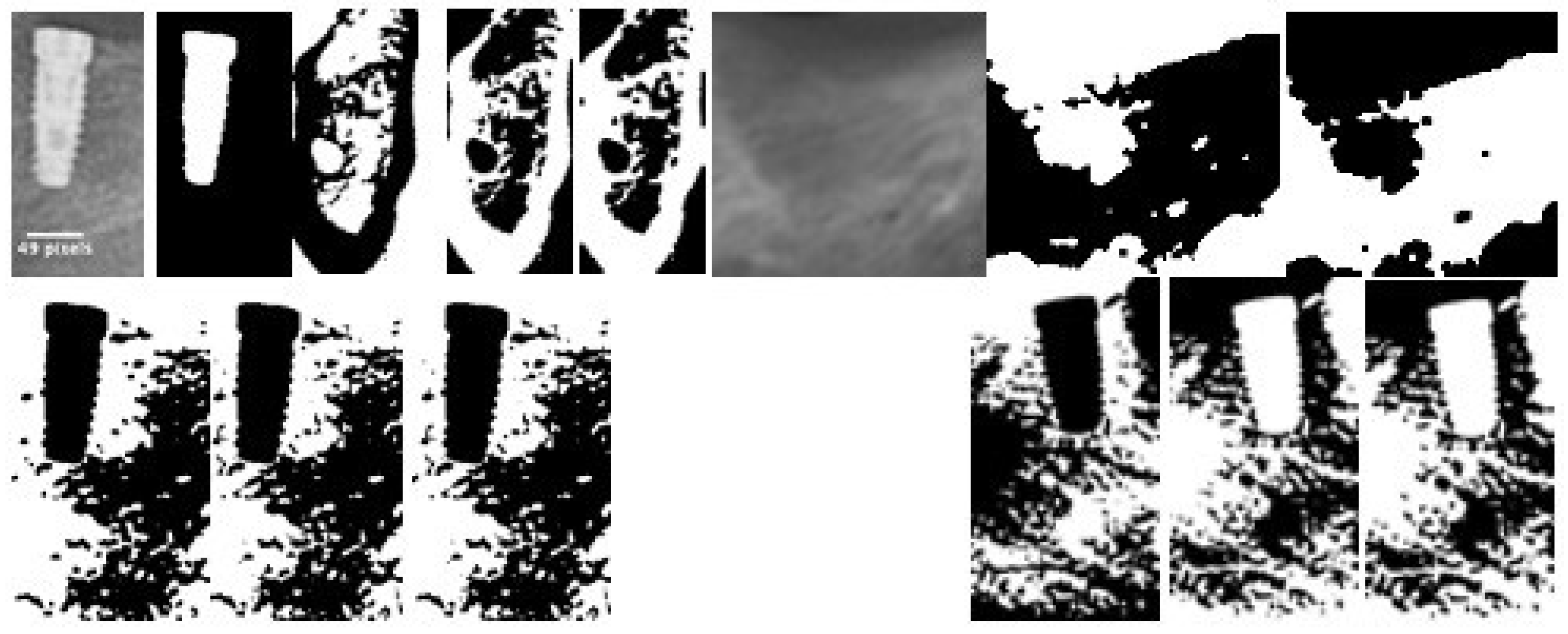
2.3. Obtaining Images and Processing
- Diagnostic or pre-implantation phase, CBCT obtained before the surgical procedure.
- Post-implantation phase, CBCT obtained after implant placement and with prosthetic load.
2.4. Fractal Dimension Analysis
2.5. Statistic Analysis
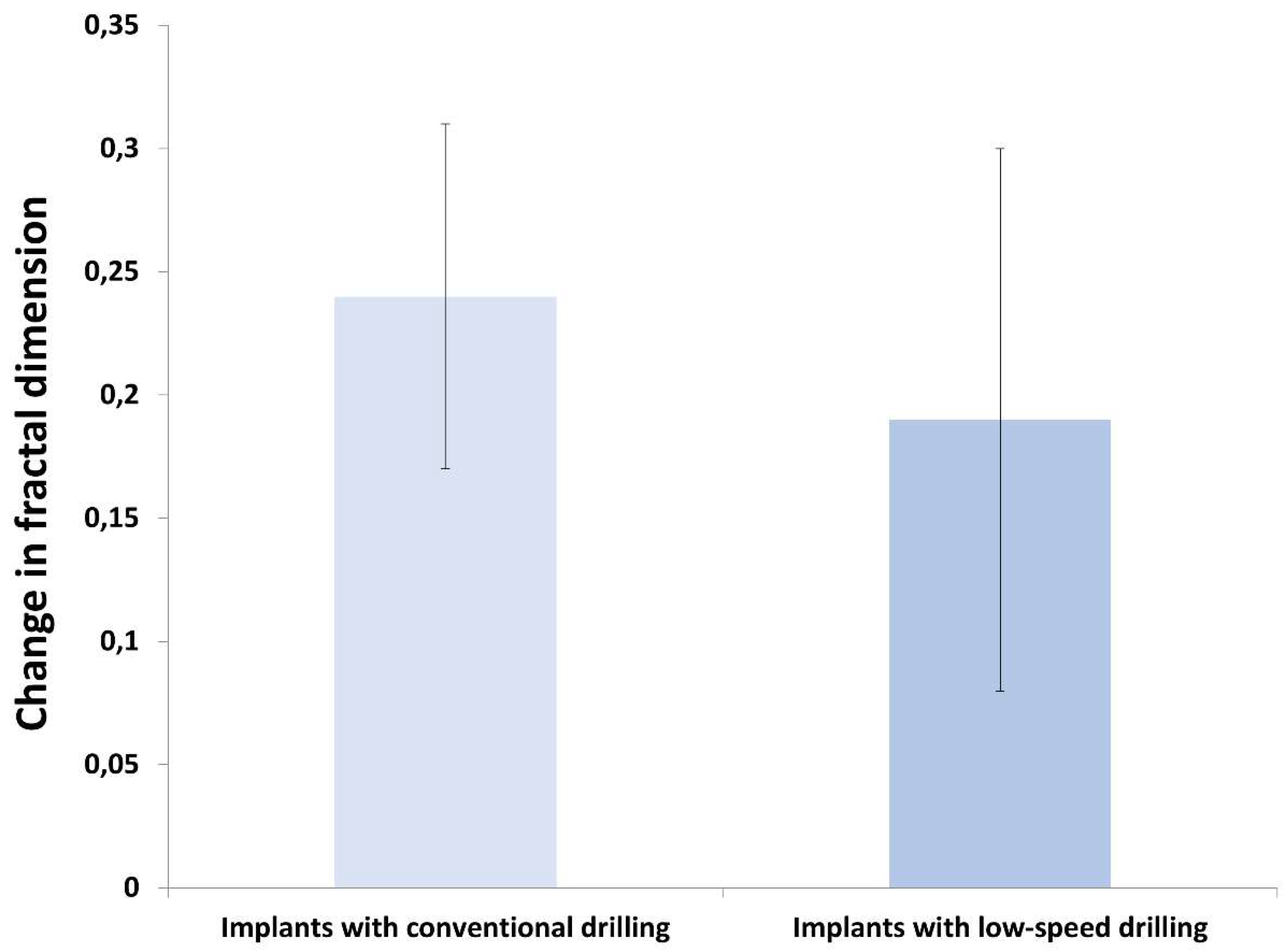
3. Results
4. Discussion
- -
- The assessment of the stability of the implants and the changes produced during the osseointegration process through the radiographic study have been analyzed by numerous authors. To the point of becoming a crucial requirement to assess the changes produced around the implant, both at the bone and soft tissue level [15,16].
- -
- -
- However, other authors have used the study of the fractal dimension to assess the state of the bone trabeculate due to its structural [19,20]. In the present paper we stated as a null hypothesis that there were no differences between the two groups subjected to conventional drilling and at low speed during the surgical phase. As a conclusion of our study, we cannot reject this null hypothesis.
- -
- The trabecular architecture complies with the mathematical definition of a fractal, as a complex structure that meets a series of criteria, including self-similarity. We could affirm that we analyze both the maxillary and mandibular bones from the orientation that we want to use (be it distal, mesial, vestibular, or lingual) and we always find partitions and spaces resembling a network.
- -
- Based on this criterion, our study states the analysis of the patient’s bone individually, establishing an initial value before implant placement and then compare the different values obtained in the radiological examinations established by the protocol. It shall allow us to establish an optimal measure of assessment of small architectural changes at the trabecular level. Changes mediated by phases of bone resorption and apposition that take place around the implant and that end in its own osseointegration [21,22,23].
- Temperature during drilling.
- Revolutions in drilling.
- -
- Bernabeu-Mira et al. [27] carried out a systematic review on both types of reaming, concluding that most of the studies carried out obtained the same results as ours, no significant differences were found regarding osseointegration and success rate between both types of reaming. Regardless of the technique used to assess drilling, almost all of them are analyzed both pathologically and radiologically.
- -
- Sukanya Mishra et al. [39], in their review work, conclude that the fractal dimension may be a value that, together with conventional methods, helps to assess the stability of the implant. They analyze the results obtained in the different studies that use this method and correlate it with those obtained with conventional methods. We consider that with the limitations that the method presents, it can also at the radiographic level, being a minimally invasive technique, provide a lot of information in the times of the osseointegration process.
- -
- In recent times, this value is becoming very important in the field of dentistry, being applied in various processes, not only in implantology [40,41]. Even in other fields such as dermatology, ophthalmology… [42,43]. Which, in part, supports its application to the bone itself in surgical processes, since the results of most of the studies conclude that the fractal dimension is a value that presents advantages and seems to give conclusive results when it comes to quantifying bone density.
- -
- Kulczyk et al. [15] study the stability of the implant through the fractal dimension, concluding that it cannot be ensured that this measurement by itself is a sufficient value to determine the stability of the implant. Likewise, various authors establish that there is no consensus on the relationship between the fractal dimension and the complexity of the bone, but they do admit that certain changes in bone density occur [44,45].
- -
- Most of these articles where no correlation is found are quite old, so the radiographic technique could have some influence, since the quality of images obtained today is much higher, especially if we are talking about CBCT.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsunaga, S.; Shirakura, Y.; Ohashi, T.; Nakahara, K.; Tamatsu, Y.; Takano, N.; Ide, Y. Biomechanical role of peri-implant cancellous bone architecture. Int. J. Prosthodont. 2010, 23, 333–338. [Google Scholar] [PubMed]
- Álvarez, R.V. Factors Related to Peri-Implant Bone Loss. Ph.D. Thesis, University of Santiago de Compostela, Coruña, Spain, 2014; pp. 17–26. [Google Scholar]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 172–184. [Google Scholar] [CrossRef] [PubMed]
- Jolley, L.; Majumdar, S.; Kapila, S. Technical factors in fractal analysis of periapical radiographs. Dentomaxillofac. Radiol. 2006, 35, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Tosoni, G.M.; Lurie, A.G.; Cowan, A.E.; Burleson, J.A. Pixel intensity and fractal analyses: Detecting osteoporosis in perimenopausal and postmenopausal women by using digital panoramic images. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 235–241. [Google Scholar] [CrossRef]
- Fernández-Martínez, M.; Gómez García, F.J.; Sánchez, Y.G.; Jornet, P.L. An intelligent system to study the fractal dimension of trabecular bones. J. Intell. Fuzzy Syst. 2018, 35, 4533–4540. [Google Scholar] [CrossRef]
- Stelt, F.; Geraets, W. The use of the fractal dimension to describe the trabecular pattern in osteoporosis. J. Dent. Res. 1990, 69, 287. [Google Scholar]
- Ruttiman, U.; Ship, J. The use of fractal dimension geometry to quantitate bone structure from radiographs. J. Dent. Res. 1990, 69, 287. [Google Scholar]
- Doyle, M.; Rabin, H.; Suri, J. Fractal analysis as a means fro the cuantification of intramandibular trabecular bone loss from dental radiographs. Proc. Biostereom. Technol. Appl. Opt. 1990, 1380, 227–235. [Google Scholar]
- Majumdar, S.; Weinstein, R.S.; Prasad, R.R. Application of fractal geometry techniques to the study of trabecular bone. Med. Phys. 1993, 20, 1611–1619. [Google Scholar] [CrossRef]
- Iyer, S.; Weiss, C.; Mehta, A. Effects of drill speed on heat production and the rate and quality of bone formation in dental implant osteotomies. Part I: Relationship between drill speed and heat production. Int. J. Prosthodont. 1997, 10, 411–414. [Google Scholar]
- Wiltfang, J.; Kloss, F.R.; Kessler, P.; Nkenke, E.; Schultze-Mosgau, S.; Zimmermann, R.; Schlegel, K.A. Effects of platelet-rich plasma on bone healing in combination with autogenous bone and bone substitutes in critical-size defects. An animal experiment. Clin. Oral Implant. Res. 2004, 15, 187–193. [Google Scholar] [CrossRef]
- White, S.C.; Rudolph, D.J. Alterations of the trabecular pattern of the jaws in patients with osteoporosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1999, 88, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Martínez, M.; Guerrero-Sánchez, Y.; López-Jornet, P. A novel approach to improve the accuracy of the box dimension calculations: Applications to trabecular bone quality. Discret. Contin. Dyn. Syst. Ser. S 2019, 12, 1527–1534. [Google Scholar] [CrossRef] [Green Version]
- Kulczyk, T.; Czajka-Jakubowska, A.; Przystańska, A. A Comparison between the Implant Stability Quotient and the Fractal Dimension of Alveolar Bone at the Implant Site. Biomed. Res. Int. 2018, 2018, 4357627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karthik, K.; Sivaraj, S.; Thangaswamy, V. Evaluation of Implant Success: A Review of Past and Present Concepts. J. Pharm. Bioallied Sci. 2013, 5, S117–S119. [Google Scholar] [CrossRef]
- Antonacci, D.; Del Fabbro, M.; Bollero, P.; Stocchero, M.; Jinno, Y.; Canullo, L. Clinical effects of conventional and underprepared drilling preparation of the implant site based on bone density: A systematic review and meta-regression. J. Prosthodont. Res. 2023, 67, 23–34. [Google Scholar] [CrossRef]
- Mashrah, M.A.; Ashour, S.H.; Al-Attab, R.; Yin, L. Immediate implant placement with simultaneous bone augmentation versus delayed implant placement following alveolar ridge preservation: A clinical and radiographic study. J. Stomatol. Oral Maxillofac. Surg. 2023, 124, 101291. [Google Scholar]
- Karadag, I.; Yilmaz, H.G. Evaluation of change in trabecular bone structure surrounding dental implants by fractal dimension analysis and comparison with radiomorphometric indicators: A retrospective study. PeerJ 2022, 10, e13145. [Google Scholar] [CrossRef]
- Griggs, J.A. Using fractal geometry to examine failed implants and prostheses. Dent. Mater. 2018, 34, 1748–1755. [Google Scholar] [CrossRef]
- Botticelli, D.; Lang, N.P. Dynamics of osseointegration in various human and animal models - a comparative analysis. Clin. Oral Implant. Res. 2017, 28, 742–748. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Lang, N.P. The role of bone debris in early healing adjacent to hydrophilic and hydrophobic implant surfaces in man. Clin. Oral Implant. Res. 2011, 22, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T.; Linder, E.; Lang, N.P.; Lindhe, J. Early bone formation adjacent to rough and turned endosseous implant surfaces. An experimental study in the dog. Clin. Oral Implant. Res. 2004, 15, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Kotsakis, G.A.; Romanos, G.E. Biological mechanisms underlying complications related to implant site preparation. Periodontol. 2000 2022, 88, 52–63. [Google Scholar] [CrossRef]
- Nagy, Á.L.; Tóth, Z.; Tarjányi, T.; Práger, N.T.; Baráth, Z.L. Biomechanical properties of the bone during implant placement. BMC Oral Health 2021, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Frizzera, F.; Spin-Neto, R.; Padilha, V.; Nicchio, N.; Ghiraldini, B.; Bezerra, F.; Marcantonio, E., Jr. Effect of osseodensification on the increase in ridge thickness and the prevention of buccal peri-implant defects: An in vitro randomized split mouth pilot study. BMC Oral Health 2022, 22, 233. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu-Mira, J.C.; Pellicer-Chover, H.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. In Vitro Study on Bone Heating during Drilling of the Implant Site: Material, Design and Wear of the Surgical Drill. Materials 2020, 13, 1921. [Google Scholar] [CrossRef]
- Salomó-Coll, O.; Auriol-Muerza, B.; Lozano-Carrascal, N.; Hernández-Alfaro, F.; Wang, H.L.; Gargallo-Albiol, J. Influence of bone density, drill diameter, drilling speed, and irrigation on temperature changes during implant osteotomies: An in vitro study. Clin. Oral Investig. 2020, 25, 1047–1053. [Google Scholar] [CrossRef]
- Anitua, E.; Carda, C.; Andia, I. A novel drilling procedure and subsequent bone autograft preparation: A technical note. Int. J. Oral Maxillofac. Implant. 2007, 22, 138–145. [Google Scholar]
- Calvo-Guirado, J.L.; Delgado-Peña, J.; Maté-Sánchez, J.E.; Mareque Bueno, J.; Delgado-Ruiz, R.A.; Romanos, G.E. Novel hybrid drilling protocol: Evaluation for the implant healing--thermal changes, crestal bone loss, and bone-to-implant contact. Clin. Oral Implant. Res. 2015, 26, 753–760. [Google Scholar] [CrossRef]
- Oh, J.H.; Fang, Y.; Jeong, S.M.; Choi, B.H. The effect of low-speed drilling without irrigation on heat generation: An experimental study. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Fraguas de San Jose, L.; Ruggeri, F.M.; Rucco, R.; Zubizarreta-Macho, Á.; Alonso Pérez-Barquero, J.; Riad Deglow, E.; Hernández Montero, S. Influence of drilling technique on the radiographic, thermographic, and geomorphometric effects of dental implant drills and osteotomy site preparations. J. Clin. Med. 2020, 9, 3631. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Aloy-Prosper, A.; Sanchis-Gonzalez, J.C.; Peñarrocha-Diago, M.A.; Peñarrocha-Diago, M. Comparison of peri-implant bone loss between conventional drilling with irrigation versus low-speed drilling without irrigation. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e730–e736. [Google Scholar] [CrossRef]
- Abdelsattar, M.; El Khader, A.; Abdel Rassoul, M. Assessment of low-speed drilling without irrigation versus convencitonal drilling with irrigation regarding heat generation and peri-implant marginal bone loss (randomized clinical trial). Alex. Dent. J. 2021, 46, 33–38. [Google Scholar]
- Tabassum, A.; Kazmi, F.; Wismeijer, D.; Siddiqui, I.A.; Tahmaseb, A. A prospective randomized clinical trial on radiographic crestal bone loss around dental implants placed using two different drilling protocols: 12-month follow-up. Int. J. Oral Maxillofac. Implant. 2021, 36, e175–e182. [Google Scholar] [CrossRef] [PubMed]
- Giro, G.; Marin, C.; Granato, R.; Bonfante, E.A.; Suzuki, M.; Janal, M.N.; Coelho, P.G. Effect of drilling technique on the early integration of plateau root form endosteal implants: An experimental study in dogs. J. Oral Maxillofac. Surg. 2011, 69, 2158–2163. [Google Scholar] [CrossRef]
- Favero, V.; Sakuma, S.; Apaza Alccayhuaman, K.A.; Benedetto, G.A.; Bengazi, F.; Botticelli, D. Healing at sites prepared using different drilling protocols. An experimental study in the tibiae of sheep. PLoS ONE 2018, 13, e0202957. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Kumar, M.; Mishra, L.; Mohanty, R.; Nayak, R.; Das, A.C.; Mishra, S.; Panda, S.; Lapinska, B. Fractal Dimension as a Tool for Assessment of Dental Implant Stability—A Scoping Review. J. Clin. Med. 2022, 11, 4051. [Google Scholar] [CrossRef] [PubMed]
- Aragonez, G.C.; Pilecco, R.O.; Dapieve, K.S.; Burgo, T.A.L.; Guilardi, L.F.; Prochnow, C.; Valandro, L.F.; Rippe, M.P. Simulation of CAD/CAM milling on lithium disilicate: Mechanical and topographic analyses of surface grinding different protocols. J. Mech. Behav. Biomed. Mater. 2022, 132, 105278. [Google Scholar] [CrossRef]
- Machry, R.V.; Cadore-Rodrigues, A.C.; Packaeser, M.G.; Lorenzett, E.; Burgo, T.A.L.; Pereira, G.K.R.; Valandro, L.F. Influence of surface treatment of resin composite substrate on the load-bearing capacity under fatigue of lithium disilicate monolithic simplified restorations. J. Mech. Behav. Biomed. Mater. 2021, 124, 104792. [Google Scholar] [CrossRef]
- Guarini, G.; Onofri, E. Nuovi orizzonti in medicina. I frattali [New horizons in medicine. Fractals]. Recenti Prog. Med. 1993, 84, 438–442. (In Italian) [Google Scholar] [PubMed]
- Lin, M.J.; Dubin, D.P.; Torbeck, R.L.; Bernstein, D.M.; Nabatian, A.; Dolan, C.K.; Bacigalupi, R.; Zade, J.; Zheng, Z.; Desman, G.; et al. Early Fractional Ablative Laser for Skin Cancer Excision Scars: A Randomized Split-Scar Study. Dermatol. Surg. 2023, 10, 1097. [Google Scholar] [CrossRef] [PubMed]
- Ruttimann, U.E.; Webber, R.L.; Hazelrig, J.B. Fractal dimension fromradiographs of peridental alveolar bone. Apossible Medicine. Oral Pathol. Oral Radiol. Endodontol. 1992, 74, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Zeytinoglu, M.; Ilhan, B.; Dundar, N.; Boyacioglu, H. Fractal analysis for the assessment of trabecular peri-implant alveolar bone using panoramic radiographs. Clin. Oral Investig. 2015, 19, 519–524. [Google Scholar] [CrossRef]
- Heo, M.S.; Park, K.S.; Lee, S.S.; Choi, S.C.; Koak, J.Y.; Heo, S.J.; Han, C.-H.; Kim, J.-D. Fractal analysis of mandibular bony healing after orthognathic surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 763–767. [Google Scholar] [CrossRef]
- Ying, Z.; Abdeldayem, M.M. Research on Resonance Properties of Semantic Wave Fractal Fractals Based on Quantitative Analysis of English Corpus. Appl. Math. Nonlinear Sci. 2022. ahead of print. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients with Conventional Drilling (n = 25) | Patients with Low-Speed Drilling (n = 25) | p-Value |
|---|---|---|---|
| Age: mean ± SD * | 56.52 ± 11.95 | 52.76 ± 13.03 | 0.293 |
| Sex: n (%) | 1.000 | ||
| Male | 13 (52) | 13 (52) | |
| Female | 12 (48) | 12 (48) | |
| Smoking behaviour: n (%) | 0.269 | ||
| Non-smoker | 19 (76) | 22 (88) | |
| smoker | 6 (24) | 3 (12) |
| Characteristics | Total (n = 129) n (%) | Implants with Conventional Drilling (n = 65) n (%) | Implants with Low-Speed Drilling (n = 64) n (%) |
|---|---|---|---|
| Dental implant type | |||
| BTI® | 60 (46.52) | 37 (56.92) | 23 (35.93) |
| Galimplant® | 33 (25.57) | 0 (0) | 33 (51.56) |
| Biomet3i® | 36 (27.91) | 28 (43.08) | 8 (12.51) |
| Maxilla/Mandible | |||
| Maxilla | 60 (46.52) | 27 (41.54) | 33 (51.56) |
| Mandible | 69 (53.48) | 38 (58.46) | 31 (48.44) |
| Length | |||
| 8 mm | 3 (2.32) | 0 (0) | 3 (4.68) |
| 8.5 mm | 10 (7.75) | 7 (10.76) | 3 (4.68) |
| 10 mm | 73 (56.58) | 37 (56.92) | 36 (56.25) |
| 11.5 mm | 27 (20.93) | 15 (23.07) | 12 (18.75) |
| 12 mm | 12 (9.31) | 2 (3.10) | 10 (15.64) |
| 13 mm | 4 (3.11) | 4 (6.15) | 0 (0) |
| Diameter | |||
| 3.25 mm | 3 (2.32) | 3 (4.54) | 0 (0) |
| 3.50 mm | 11 (8.52) | 0 (0) | 11 (17.18) |
| 3.75 mm | 23 (17.84) | 10 (15.38) | 13 (20.31) |
| 4.00 mm | 80 (62.01) | 45 (69.23) | 35 (54.68) |
| 4.50 mm | 12 (9.31) | 7 (10.76) | 5 (7.83) |
| Site | |||
| 1.14 | (3.11) | 1 (1.53) | 3 (4.68) |
| 1.22 | (1.55) | 1 (1.53) | 1 (1.56) |
| 1.35 | (3.87) | 3 (4.54) | 2 (3.12) |
| 1.46 | (4.65) | 2 (3.10) | 4 (6.25) |
| 1.55 | (3.87) | 1 (1.53) | 4 (6.25) |
| 1.68 | (6.21) | 5 (8.07) | 3 (4.68) |
| 2.13 | (2.32) | 0 (0) | 3 (4.68) |
| 2.24 | (3.11) | 2 (3.10) | 2 (3.12) |
| 2.36 | (4.65) | 3 (4.54) | 3 (4.68) |
| 2.46 | (4.65) | 4 (6.15) | 2 (3.12) |
| 2.57 | (5.46) | 3 (4.54) | 4 (6.25) |
| 2.65 | (3.87) | 2 (3.10) | 3 (4.68) |
| 2.72 | (1.55) | 1 (1.53) | 1 (1.56) |
| 3.11 | (0.77) | 0 (0) | 1 (1.56) |
| 3.23 | (2.32) | 2 (3.10) | 1 (1.56) |
| 3.32 | (1.55) | 1 (1.53) | 1 (1.56) |
| 3.42 | (1.55) | 1 (1.53) | 1 (1.56) |
| 3.55 | (3.87) | 1 (1.53) | 4 (6.25) |
| 3.616 | (12.41) | 9 (13.84) | 7 (10.93) |
| 3.74 | (3.11) | 4 (6.15) | 0 (0) |
| 4.12 | (1.55) | 1 (1.53) | 1 (1.56) |
| 4.21 | (0.77) | 0 (0) | 1 (1.56) |
| 4.32 | (1.55) | 1 (1.53) | 1 (1.56) |
| 4.41 | (0.77) | 0 (0) | 1 (1.56) |
| 4.55 | (3.87) | 3 (4.54) | 2 (3.12) |
| 4.617 | (13.17) | 11 (16.92) | 6 (9.47) |
| 4.75 | (3.87) | 3 (4.54) | 2 (3.12) |
| Fractal Dimension | |||
|---|---|---|---|
| Groups | Presurgical Mean ± SD * | Postsurgical Mean ± SD | p-Value |
| Implants with conventional drilling (n = 65) | 1.68 ± 0.06 | 1.71 ± 0.05 | <0.001 |
| Implants with low-speed drilling (n = 64) | 1.67 ± 0.08 | 1.69 ± 0.07 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soler-Alcaraz, S.; Guerrero-Sánchez, Y.; Pérez-Sayáns, M.; Bernabeu-Mira, J.C.; Peñarrocha-Oltra, D.; Camacho-Alonso, F. Evaluation of Change in Radiographic Fractal Dimension around Dental Implants Placed with Low-Speed Drilling and Standard Drilling Protocols. J. Clin. Med. 2023, 12, 2244. https://doi.org/10.3390/jcm12062244
Soler-Alcaraz S, Guerrero-Sánchez Y, Pérez-Sayáns M, Bernabeu-Mira JC, Peñarrocha-Oltra D, Camacho-Alonso F. Evaluation of Change in Radiographic Fractal Dimension around Dental Implants Placed with Low-Speed Drilling and Standard Drilling Protocols. Journal of Clinical Medicine. 2023; 12(6):2244. https://doi.org/10.3390/jcm12062244
Chicago/Turabian StyleSoler-Alcaraz, Sofía, Yolanda Guerrero-Sánchez, Mario Pérez-Sayáns, Juan Carlos Bernabeu-Mira, David Peñarrocha-Oltra, and Fabio Camacho-Alonso. 2023. "Evaluation of Change in Radiographic Fractal Dimension around Dental Implants Placed with Low-Speed Drilling and Standard Drilling Protocols" Journal of Clinical Medicine 12, no. 6: 2244. https://doi.org/10.3390/jcm12062244