

Elevated Blood Alcohol Concentration Is Associated with Improved Clinical Outcomes of Intravenous Thrombolysis Treatment in Acute Ischemic Stroke Patients—A Retrospective Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
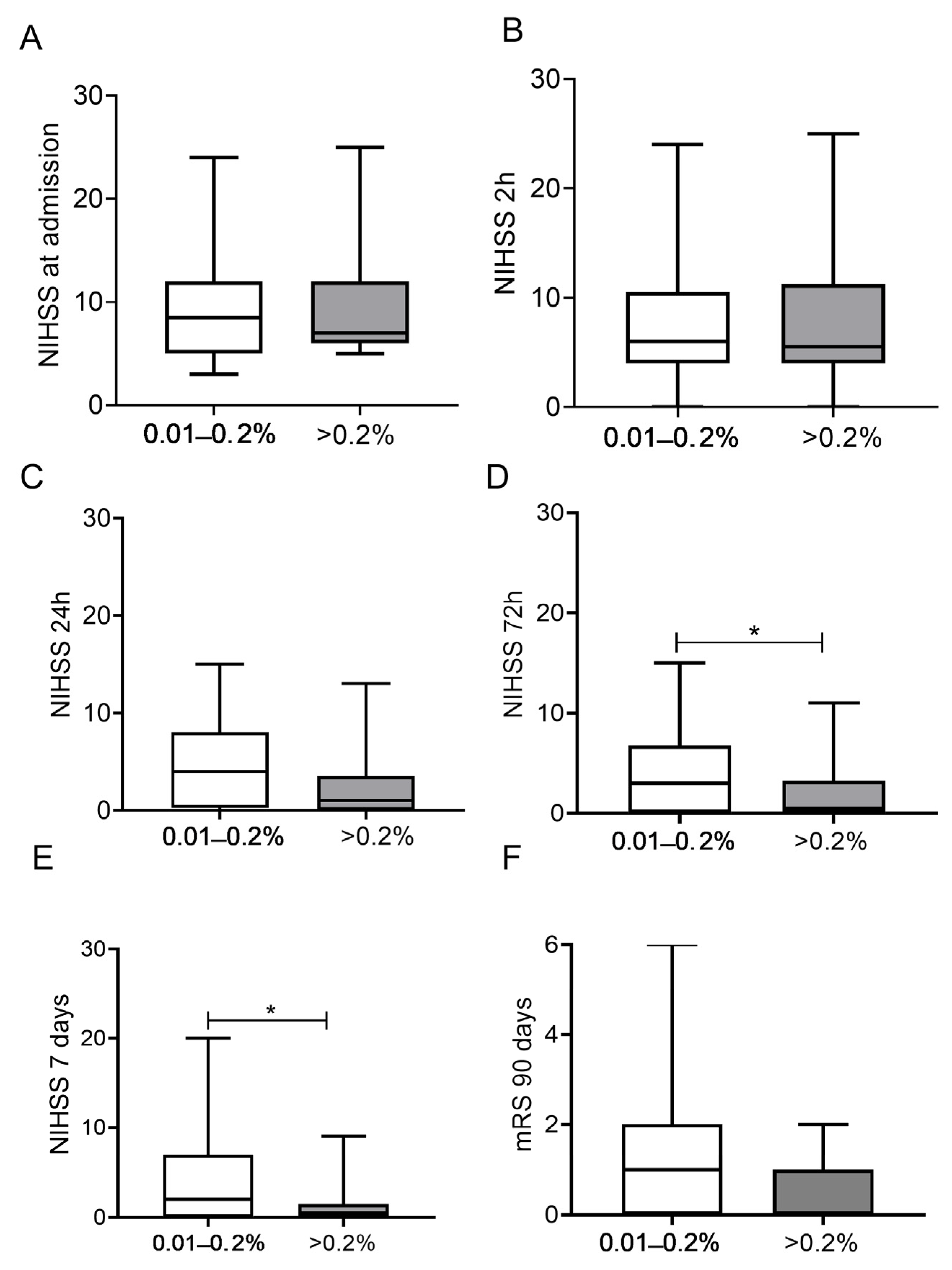
- The short-term outcome was assessed by the NIHSS score 7 days after IVT. Favorable outcome was defined as a decrease of at least 4 points in the NIHSS score as compared to the pretreatment value or a decrease to 0 points, while poor outcome was defined as an increase of at least 4 points [2].
- The long-term outcome was assessed by the mRS score at 3 months after stroke onset. Patients with an mRS score of 0–2 were defined as having a favorable long-term outcome [23].
- The safety of IVT in both groups was evaluated by the occurrence of intracranial hemorrhage according to the ECASS II criteria, based on the presence of asymptomatic (aSICH) or symptomatic intracranial hemorrhage (SICH).
- Mortality was assessed at 3 months post-event.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.; Blaha, M.; Chiuve, S.; Cushman, M.; Das, S.; Deo, R.; de Ferranti, S.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart disease and stroke statistics-2017 update: A report from the american heart association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Kwiatkowski, T.G.; Libman, R.B.; Frankel, M.; Tilley, B.C.; Morgenstern, L.B.; Lu, M.; Broderick, J.P.; Lewandowski, C.A.; Marler, J.R.; Levine, S.R.; et al. Effects of tissue plasminogen activator for acute ischemic stroke at one year. National institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Study Group. N. Engl. J. Med. 1999, 340, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 h after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [Green Version]
- Ji, Z.; Liu, K.; Cai, L.; Peng, C.; Xin, R.; Gao, Z.; Zhao, E.; Rastogi, R.; Han, W.; Rafols, J.A.; et al. Therapeutic effect of tPA in ischemic stroke is enhanced by its combination with normobaric oxygen and hypothermia or ethanol. Brain Res. 2015, 1627, 31–40. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Y.; Geng, X.; Asmaro, K.; Peng, C.; Sullivan, J.; Ding, J.; Ji, X.; Ding, Y. Neuroprotective effect of acute ethanol administration in a rat with transient cerebral ischemia. Stroke 2012, 43, 205–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemarchand, E.; Gauberti, M.; de Lizarrondo, S.M.; Villain, H.; Repessé, Y.; Montagne, A.; Vivien, D.; Ali, C.; Rubio, M. Impact of alcohol consumption on the outcome of ischemic stroke and thrombolysis: Role of the hepatic clearance of tissue-type plasminogen activator. Stroke 2015, 46, 1641–1650. [Google Scholar] [CrossRef] [Green Version]
- Kuikka, J.; Tiihonen, J.; Hakola, P.; Paanila, J.; Airaksinen, J.; Eronen, M.; Hallikainen, T. Acute ethanol-induced changes in cerebral blood flow. Am. J. Psychiatry 1994, 151, 1505–1508. [Google Scholar]
- Salem, R.O.; Laposata, M. Effects of alcohol on hemostasis. Am. J. Clin. Pathol. 2005, 123, S96–S105. [Google Scholar] [CrossRef] [PubMed]
- Aikens, M.L.; Grenett, H.E.; Benza, R.L.; Tabengwa, E.M.; Davis, G.C.; Booyse, F.M. Alcohol-induced upregulation of plasminogen activators and fibrinolytic activity in cultured human endothelial cells. Alcohol Clin. Exp. Res. 1998, 22, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Elmer, O.; Goransson, G.; Zoucas, E. Impairment of primary hemostasis and platelet function after alcohol ingestion in man. Haemostasis 1984, 14, 223–228. [Google Scholar] [CrossRef]
- Fu, P.; Peng, C.; Ding, J.; Asmaro, K.; Sullivan, J.; Guthikonda, M.; Ding, Y. Acute administration of ethanol reduces apoptosis following ischemic stroke in rats. Neurosci. Res. 2013, 76, 93–97. [Google Scholar] [CrossRef]
- Crews, F.T.; Steck, J.C.; Chandler, L.J.; Yu, C.J.; Day, A. Ethanol, stroke, brain damage, and excitotoxicity. Pharmacol. Biochem. Behav. 1998, 59, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Tien, H.C.; Tremblay, L.N.; Rizoli, S.B.; Gelberg, J.; Chughtai, T.; Tikuisis, P.; Shek, P.; Brenneman, F.D. Association between alcohol and mortality in patients with severe traumatic head injury. Arch. Surg. 2006, 141, 1185–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Schild, S.; Hallevi, H.; Shaltoni, H.; Barreto, A.D.; Gonzales, N.R.; Aronowski, J.; Savitz, S.I.; Grotta, J.C. Combined neuroprotective modalities coupled with thrombolysis in acute ischemic stroke: A pilot study of caffeinol and mild hypothermia. J. Stroke Cerebrovasc. Dis. 2009, 18, 86–96. [Google Scholar] [CrossRef] [Green Version]
- Piriyawat, P.; Labiche, L.A.; Burgin, W.S.; Aronowski, J.A.; Grotta, J.C. Pilot dose-escalation study of caffeine plus ethanol (caffeinol) in acute ischemic stroke. Stroke 2003, 34, 1242–1245. [Google Scholar] [CrossRef] [Green Version]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef] [PubMed]
- Aviv, R.I.; Mandelcorn, J.; Chakraborty, S.; Gladstone, D.; Malham, S.; Tomlinson, G.; Fox, A.J.; Symons, S. Alberta Stroke Program Early CT Scoring of CT perfusion in early stroke visualization and assessment. AJNR Am. J. Neuroradiol. 2007, 28, 1975–1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; von Kummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef]
- Kim, Y.G.; Han, K.-D.; Choi, J.-I.; Boo, K.Y.; Kim, D.Y.; Lee, K.-N.; Shim, J.; Kim, J.S.; Kim, Y.-H. Frequent drinking is a more important risk factor for new-onset atrial fibrillation than binge drinking: A nationwide population-based study. Europace 2020, 22, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Niemela, O. Biomarkers in alcoholism. Clin. Chim. Acta 2007, 377, 39–49. [Google Scholar] [CrossRef]
- Kolominsky-Rabas, P.L.; Weber, M.; Gefeller, O.; Neundoerfer, B.; Heuschmann, P.U. Epidemiology of ischemic stroke subtypes according to TOAST criteria: Incidence, recurrence, and long-term survival in ischemic stroke subtypes: A population-based study. Stroke 2001, 32, 2735–2740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [Green Version]
- Christensen, A.I.; Nordestgaard, B.G.; Tolstrup, J.S. Alcohol intake and risk of ischemic and haemorrhagic stroke: Results from a Mendelian randomisation study. J. Stroke 2018, 20, 218–227. [Google Scholar] [CrossRef]
- Ducroquet, A.; Leys, D.; Al Saabi, A.; Richard, F.; Cordonnier, C.; Girot, M.; Deplanque, D.; Casolla, B.; Allorge, D.; Bordet, R. Influence of chronic ethanol consumption on the neurological severity in patients with acute cerebral ischemia. Stroke 2013, 44, 2324–2326. [Google Scholar] [CrossRef] [Green Version]
- Drieu, A.; Lanquetin, A.; Levard, D.; Glavan, M.; Campos, F.; Quenault, A.; Lemarchand, E.; Naveau, M.; Pitel, A.L.; Castillo, J.; et al. Alcohol exposure-induced neurovascular inflammatory priming impacts ischemic stroke and is linked with brain perivascular macrophages. JCI Insight 2020, 5, e129226. [Google Scholar] [CrossRef] [Green Version]
- Hansagi, H.; Romelsjo, A.; Gerhardsson de Verdier, M.; Andreasson, S.; Leifman, A. Alcohol consumption and stroke mortality. 20-year follow-up of 15,077 men and women. Stroke 1995, 26, 1768–1773. [Google Scholar] [CrossRef] [PubMed]
- Rist, P.M.; Berger, K.; Buring, J.E.; Kase, C.S.; Gaziano, J.M.; Kurth, T. Alcohol consumption and functional outcome after stroke in men. Stroke 2010, 41, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altura, B.M.; Gebrewold, A.; Altura, B.T.; Gupta, R.K. Role of brain [Mg2+] i in alcohol-induced hemorrhagic stroke in a rat model: A 31p-NMR in vivo study. Alcohol 1995, 12, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.M.; Gebrewold, A. Alpha-tocopherol attenuates alcohol-induced cerebral vascular damage in rats: Possible role of oxidants in alcohol brain pathology and stroke. Neurosci. Lett. 1996, 220, 207–210. [Google Scholar] [CrossRef]
- Akyea, R.K.; Vinogradova, Y.; Qureshi, N.; Patel, R.S.; Kontopantelis, E.; Ntaios, G.; Asselbergs, F.W.; Kai, J.; Weng, S.F. Sex, Age, and Socioeconomic Differences in Nonfatal Stroke Incidence and Subsequent Major Adverse Outcomes. Stroke 2021, 52, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Kadlecová, P.; Andel, R.; Mikulík, R.; Handing, E.P.; Pedersen, N.L. Alcohol consumption at midlife and risk of stroke during 43 years of follow-up: Cohort and twin analyses. Stroke 2015, 46, 627–633. [Google Scholar] [CrossRef]
- Gattringer, T.; Enzinger, C.; Fischer, R.; Seyfang, L.; Niederkorn, K.; Khalil, M.; Ferrari, J.; Lang, W.; Brainin, M.; Willeit, J.; et al. IV thrombolysis in patients with ischemic stroke and alcohol abuse. Neurology 2015, 85, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Alcohol Group | Control Group | p | |
|---|---|---|---|
| Number of patients, n (%) | 60 | 180 | |
| Male, n (%) | 51 (85) | 155 (86) | 0.975 |
| Age (years), median (IQR) | 61 (54–69) | 62 (54–69) | 0.893 |
| Ethanol level (%), median (IQR) | 0.1515 (0.0523–0.2045) | - | |
| Affected brain area, n (%) | |||
| VBI | 16 (26) | 48 (27) | |
| Dominant MCA area | 14 (24) | 43 (24) | 0.996 |
| Non-dominant MCA area | 30 (50) | 89 (49) | |
| Cerebrovascular risk factors, n (%) | |||
| Hypertension | 34 (57) | 145 (81) | <0.001 |
| Diabetes mellitus | 7 (12) | 38 (21) | 0.356 |
| Hyperlipidemia | 27 (45) | 76 (39) | 0.756 |
| Atrial fibrillation | 5 (8) | 22 (12) | 0.408 |
| History of stroke | 10 (17) | 21 (11) | 0.317 |
| History of myocardial infarction | 7 (12) | 18 (10) | 0.366 |
| Peripheral arterial disease | 2 (3) | 3 (2) | 0.601 |
| Current smoker | 35 (58) | 85 (47) | 0.136 |
| BMI, median (IQR) | 25.2 (22.1–29.3) | 28.3 (24.2–31.7) | 0.001 |
| Medication at admission, n (%) | |||
| Antiplatelet therapy | 7 (12) | 51 (28) | 0.008 |
| Oral anticoagulant | 2 (3) | 10 (6) | 0.735 |
| Oral antidiabetics | 5 (8) | 29 (16) | 0.150 |
| Lipid lowering therapy | 8 (13) | 28 (15) | 0.751 |
| OTN, min, median (IQR) | 139.5 (113.0–177.0) | 137.0 (109.0–180.0) | 0.700 |
| DTN, min, median (IQR) | 41.0 (32.0–57.0) | 42.5 (32.0–57.0) | 0.893 |
| r-tPA dose, mg, median (IQR) | 66.0 (56.0–78.0) | 76.0 (62.1–86.0) | 0.002 |
| Laboratory parameters at admission, median (IQR) | |||
| Serum sodium (mmol/L) | 140.0 (137.0–142.0) | 139.0 (137.0–141.0) | 0.223 |
| Serum glucose (mmol/L) | 5.8 (5.0–6.3) | 6.4 (5.6–7.8) | <0.001 |
| Creatinine (μ mol/L) | 72.0 (63.8–83.0) | 76.0 (65.0–91.0) | 0.117 |
| hsCRP (mg/L) | 2.6 (1.1–5.8) | 2.5 (1.4–4.9) | 0.775 |
| AST (U/L) | 23.5 (17.0–35.0) | 20.0 (15.0–24.0) | 0.003 |
| ALT (U/L) | 18.5 (13.0–30.0) | 19.0 (14.0–26.0) | 0.809 |
| GGT (U/L) | 51.0 (28.0–101.5) | 37.0 (22.5–63.0) | 0.014 |
| WBC (G/L) | 7.6 (6.4–9.0) | 8.4 (6.7–10.5) | 0.057 |
| MCV (fL) | 92.69 ± 6.62 | 88.93 ± 5.69 | <0.001 |
| Platelet count (G/L) | 237 (191–278) | 216 (183–252) | 0.055 |
| APTT | 28.9 ± 3.3 | 28.2 ± 3.2 | 0.157 |
| INR | 0.96 (0.92–1.01) | 0.97 (0.93–1.01) | 0.633 |
| Stroke etiology (TOAST), n (%) | |||
| Large artery atherosclerosis | 20 (35) | 58 (33) | |
| Cardioembolic | 9 (15) | 34 (20) | 0.867 |
| Small-vessel occlusion | 14 (25) | 44 (25) | |
| Other/undetermined | 15 (25) | 38 (22) | |
| Admission BP systolic (mmHg), mean±SD | 160 ± 27.0 | 170.0 ± 26.5 | 0.011 |
| Admission BP diastolic (mmHg), mean ± SD | 94.3 ± 16.6 | 94.0 ± 17.0 | 0.874 |
| ASPECTS at admission | 10 (9–10) | 10 (9–10) | 0.649 |
| ASPECTS at 24 h | 9 (7–10) | 8 (6–9) | 0.017 |
| Alcohol consumption habits, n (%) | |||
| Non-drinker, mild drinker | 16 (27) | 108 (60) | <0.001 |
| Moderate, heavy drinker | 44 (73) | 72 (40) | |
| NIHSS at admission, median (IQR) | 7 (5–12) | 8 (5–11) | 0.699 |
| NIHSS at 2 h, median (IQR) | 6 (4–11) | 7 (4–11) | 0.740 |
| NIHSS at 24 h, median (IQR) | 4 (0–7) | 6 (3–12) | <0.001 |
| NIHSS at 72 h, median (IQR) | 3 (0–6) | 5 (3–10) | 0.001 |
| NIHSS at 7 day, median (IQR) | 2 (0–7) | 5 (2–10) | <0.001 |
| ΔNIHSS 2 h–0 h | −1 (−3–0) | 0 (−2–0) | 0.026 |
| ΔNIHSS 24 h–0 h | −4 (−7 to −2) | −1 (−3 to 1) | <0.001 |
| ΔNIHSS 72 h–0 h | −5 (−7 to −3) | −2 (−5 to 0) | <0.001 |
| ΔNIHSS day 7–0 h | −6 (−7 to −4) | −2 (−5 to 0) | <0.001 |
| Outcomes, n (%) | |||
| Short-term outcome (7 days) | |||
| good outcome (NIHSS ≥ 4 points decrease or 0) | 49 (82) | 65 (36) | |
| unchanged status (ΔNIHSS ± 3 points) | 8 (13) | 97 (54) | <0.001 |
| poor outcome (NIHSS ≥ 4 points increase) | 3 (5) | 18 (10) | |
| Long-term outcome (90 days) | |||
| mRS 0–2 | 54 (90) | 114 (63) | <0.001 |
| mRS 3–6 | 6 (10) | 66 (37) | |
| Intracranial hemorrhage (ECASS II) | |||
| no hemorrhage | 59 (98) | 171 (95) | |
| aSICH | 1 (2) | 7 (4) | 0.500 |
| SICH | 0 (0) | 2 (1) | |
| Mortality at 90 days after thrombolysis | 1 (2) | 10 (6) | 0.300 |
| Alcohol Group (n = 60) | Control Group (n = 180) | p | |
|---|---|---|---|
| Patients with presence of symptoms, n (%) | |||
| At admission | |||
| dysarthria | 42 (70) | 96 (53) | 0.024 |
| ataxia | 10 (17) | 23 (13) | 0.449 |
| eye movement disorder | 15 (25) | 39 (22) | 0.592 |
| At 24 h post-event | |||
| dysarthria | 22 (37) | 80 (44) | 0.291 |
| ataxia | 6 (10) | 20 (11) | 0.811 |
| eye movement disorder | 6 (10) | 31 (17) | 0.179 |
| Ratio of patients with improvement of symptoms, n/total, (%) | |||
| At 24 h post-event | |||
| dysarthria | 25/42 (60) | 20/96 (21) | <0.001 |
| ataxia | 7/10 (70) | 12/23 (52) | 0.341 |
| eye movement disorder | 11/15 (73) | 18/39 (46) | 0.073 |
| OR | 95% CI | p | |
|---|---|---|---|
| Unfavorable short-term outcome £ | |||
| Acute alcohol consumption | 0.091 | 0.036–0.227 | <0.001 |
| NIHSS on admission (per 1 point) | 0.908 | 0.844–0.976 | 0.009 |
| Age (per 1 year) | 1.035 | 1.004–1.067 | 0.025 |
| Systolic blood pressure on admission (per 1 Hgmm) | 1.015 | 1.002–1.028 | 0.025 |
| AST (per 1 U/L) | 0.978 | 0.955–1.003 | 0.082 |
| Unfavorable long-term outcome § | |||
| NIHSS on admission (per 1 point) | 1.215 | 1.121–1.318 | <0.001 |
| Acute alcohol consumption | 0.187 | 0.066–0.535 | 0.002 |
| Age (per 1 year) | 1.056 | 1.015–1.097 | 0.006 |
| Systolic blood pressure on admission (per 1 Hgmm) | 1.017 | 1.004–1.031 | 0.013 |
| Serum glucose on admission (per 1 mmol/L) | 1.125 | 0.999–1.267 | 0.051 |
| White blood cell count on admission (per 1 G/L) | 1.139 | 0.986–1.315 | 0.077 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Árokszállási, T.; Balogh, E.; Orbán-Kálmándi, R.; Pásztor, M.; Árokszállási, A.; Nagy, E.B.; Belán, I.; May, Z.; Csépány, T.; Csiba, L.; et al. Elevated Blood Alcohol Concentration Is Associated with Improved Clinical Outcomes of Intravenous Thrombolysis Treatment in Acute Ischemic Stroke Patients—A Retrospective Study. J. Clin. Med. 2023, 12, 2238. https://doi.org/10.3390/jcm12062238
Árokszállási T, Balogh E, Orbán-Kálmándi R, Pásztor M, Árokszállási A, Nagy EB, Belán I, May Z, Csépány T, Csiba L, et al. Elevated Blood Alcohol Concentration Is Associated with Improved Clinical Outcomes of Intravenous Thrombolysis Treatment in Acute Ischemic Stroke Patients—A Retrospective Study. Journal of Clinical Medicine. 2023; 12(6):2238. https://doi.org/10.3390/jcm12062238
Chicago/Turabian StyleÁrokszállási, Tamás, Eszter Balogh, Rita Orbán-Kálmándi, Máté Pásztor, Anita Árokszállási, Edit Boglárka Nagy, Ivett Belán, Zsolt May, Tünde Csépány, László Csiba, and et al. 2023. "Elevated Blood Alcohol Concentration Is Associated with Improved Clinical Outcomes of Intravenous Thrombolysis Treatment in Acute Ischemic Stroke Patients—A Retrospective Study" Journal of Clinical Medicine 12, no. 6: 2238. https://doi.org/10.3390/jcm12062238