1. Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease with type 2-skewed abnormal immunity, skin barrier impairment, and severe itch [
1,
2]. Upadacitinib, an oral Janus kinase (JAK) 1 inhibitor, is approved for the treatment of atopic dermatitis (AD) in Japan. We have previously reported that upadacitinib treatment for 12 weeks was well-tolerated and provided comparable or rather superior therapeutic effects for patients with AD in real-world clinical practice, compared with those in previous clinical trials [
3].
The neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR) have been identified as indicators of systemic inflammation [
4,
5,
6,
7]. In patients with psoriasis, the values of these parameters correlate with the area and severity index of psoriasis (PASI). In particular, NLR was reduced in parallel with PASI by treatment with tumor necrosis factor (TNF)-α inhibitors, indicating that NLR can act as an indicator of disease severity and treatment responses in patients with psoriasis [
8,
9]. Further, previous studies reported that the eosinophil-to-lymphocyte ratio (ELR), as well as NLR or PLR, in patients with AD, positively correlated with the scoring atopic dermatitis index, an AD severity score [
10,
11,
12]. Recently, Inokuchi-Sakata et al. have reported that ELR correlates with the degree of itch, while NLR correlates with the degree of inflammation and the area of the affected region in patients with AD [
13]. However, the transition of these parameters by treatment for AD has not been precisely examined.
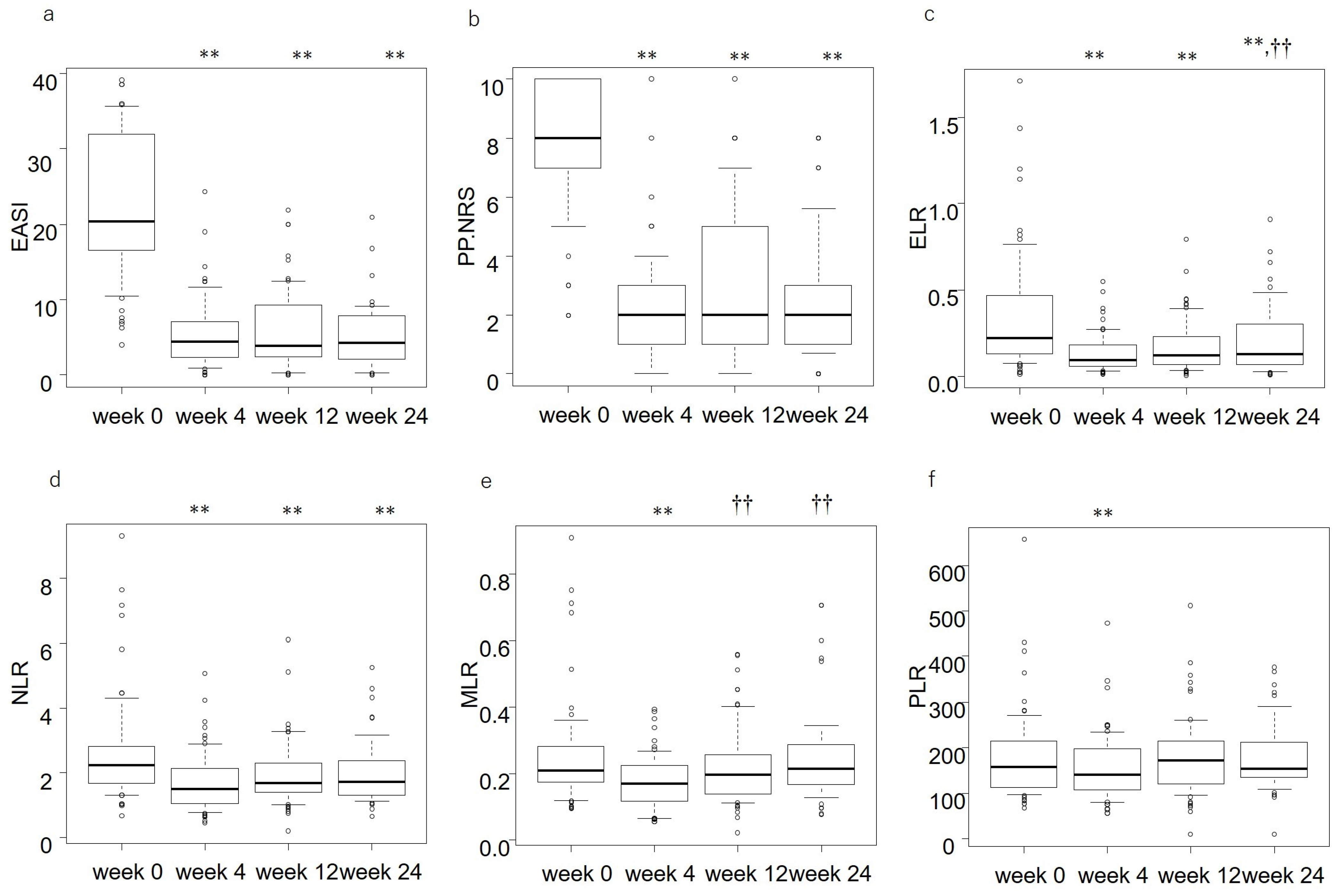
In this study, we examined how the values of ELR, NLR, MLR, and PLR might be altered by treatment with upadacitinib in patients with moderate-to-severe AD in real-world practice. We examined if changes in these parameters can reflect the improvement of clinical signs or itch by upadacitinib treatment, as assessed by the eczema area and severity index (EASI) or the peak pruritus-numerical rating scale (PP-NRS), respectively. We also attempted to detect background factors that predict the responsiveness to treatment with upadacitinib for AD.
4. Discussion
Before upadacitinib treatment, baseline ELR, NLR, MLR, and PLR significantly correlated with baseline EASI (
Table 2). The results were consistent with those of the previous reports [
10,
11,
13], indicating that ELR, NLR, MLR, and PLR may reflect the long-term control status of AD.
Baseline PP-NRS was significantly correlated with baseline NLR and PLR, but not with baseline ELR. This may be related to the contribution of other cells, such as basophils or mast cells, to the baseline pruritus in AD patients, in addition to eosinophils; these cells are a close proximity of sensory nerves in AD lesions and produce substance P and interleukin (IL)-4/13/31, generating itch [
16].
The percent reduction of ELR correlated with those of EASI and PP-NRS at weeks 4, 12, and 24. This suggests that the reduction of ELR may reflect the improvement of clinical signs and itch by upadacitinib. The results also indicate that eosinophils may play key roles in the rash and itch of AD and may be the target of upadacitinib treatment. Eosinophils in AD skin lesions secrete granules, such as major basic protein (MBP), eosinophil peroxidase (EPO), and eosinophil cationic protein (ECP) [
17]. These granules can induce the damage of keratinocytes, promoting the release of alarmins, such as IL-33 which stimulate basophils, mast cells, and eosinophils. Eosinophil-derived EPO, MBP, ECP, and substance P act on mast cells and induce their degranulation and release of histamine and cytokines, such as TNF-α or type 2 cytokines [
18,
19]. Eosinophils release a larger amount of IL-31 compared to CD4+ or CD8+T cells, and the released IL-31 further induces chemotaxis and production of IL-31 in eosinophils [
20]. The oral JAK1 inhibitor upadacitinib can suppress the effects of IL-31 transducing JAK1/signal transduction and activator of transcription (STAT) signals. This medicine may block the autoactivation of eosinophils, possibly via IL-31 in AD skin lesions.
In the upper dermis of AD lesions, eosinophils are in close proximity to substance P+ nerve fibers and are abundantly producing brain-derived neurotrophic factor (BDNF). The eosinophil-derived BDNF promotes the growth of sensory nerves and induces chemotaxis, and prolongs the survival of eosinophils in an autocrine manner [
21]. Conversely, neurons secrete substance P, which induces degranulation and chemotaxis of eosinophils, and suppresses their apoptosis [
22]. The activated eosinophils secrete IL-4/IL-13 or IL-31, which bind IL-4Rα or IL-31RA, respectively, on sensory nerve endings and stimulate the JAK1/STAT pathway, generating an itch sensation [
23,
24]. The eosinophil-derived IL-31 also promotes the growth of sensory nerves [
25]. The oral JAK1 inhibitor upadacitinib might suppress the effects of IL-31 or IL-4/IL-13 and block the communication between nerves and eosinophils, leading to the suppression of pruritus.
The change of NLR, MLR, and PLR did not correlate with that of EASI or PP-NRS in upadacitinib treatment, except for the transient correlation (
Table 3). Granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), or thrombopoietin promotes the granulopoiesis, granulopoiesis/monocytopoiesis [
26], or thrombopoiesis, respectively, in bone marrow [
27]. Though these cytokines, G-CSF, GM-CSF, and thrombopoietin transduce signals through JAK2, and the JAK1 inhibitor upadacitinib can suppress JAK2 at tissue concentrations generated by the standard intake [
28]. Therefore, upadacitinib may suppress the effects of these cytokines and, resultantly, reduce the numbers of peripheral neutrophils, monocytes, and platelets within the range, allowing the continuation of treatment. However, the decrease of NLR, MLR, and PLR appears independent of the improvement of clinical signs or itch, indicating that neutrophils, monocytes, or platelets may not directly mediate the upadacitinib-induced improvement of rash or itch. We should further examine if this trend can be seen in other treatments for AD.
Older age was associated with a high percent reduction of PP-NRS at weeks 4 and 12, indicating that older age may predict better improvement of itch by upadacitinib. This may possibly be because older patients might show reduced type 2 activities compared to younger patients [
29]; in adult patients with AD, the levels of IL-31 or IL-13 (cytokines generating itch) in the skin lesions are reduced with ageing [
29,
30]. Thus, older patients with AD might be more susceptible to the inhibitory effects of upadacitinib on the cytokines related to itch.
High baseline PP-NRS was associated with a high percent reduction of PP-NRS at weeks 4 and 24, indicating that high baseline PP-NRS may predict better improvement of itch by upadacitinib. This is possibly because patients with higher PP-NRS values before treatment may have more room to be improved by upadacitinib compared to the patients with lower PP-NRS. A similar trend can be seen in patients with psoriasis; patients with higher pretreatment PASI result in a higher percent reduction of PASI by treatment with biologics [
31].
Female sex was associated with a high percent reduction of EASI at week 4, indicating that female patients may predict better improvement of rash by upadacitinib than male patients. However, the bias caused by the male-preponderance (71% of the patients) and small sample size cannot be denied in this study. The sex difference in the response to upadacitinib treatment should be further examined strictly in larger cohorts with a uniform assignment of sexes.
This study has several limitations. First, this study evaluated the efficacy of only 15 mg/day of upadacitinib. The results for 30 mg/day upadacitinib should be further examined. Second, this study is a retrospective one with a small sample size. Third, this study included patients treated with oral upadacitinib plus topical corticosteroids, but not those with oral upadacitinib alone or with topical corticosteroids alone. Therefore, it is unclear whether upadacitinib plus topical corticosteroids additively or synergistically improved clinical signs and itch. Further prospective study with a larger cohort should compare the therapeutic effects of upadacitinib alone, topical corticosteroids alone, and both treatments.




{kind=link}