
Association of Hyperkalemia and Hypokalemia with Patient Characteristics and Clinical Outcomes in Japanese Hemodialysis (HD) Patients
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
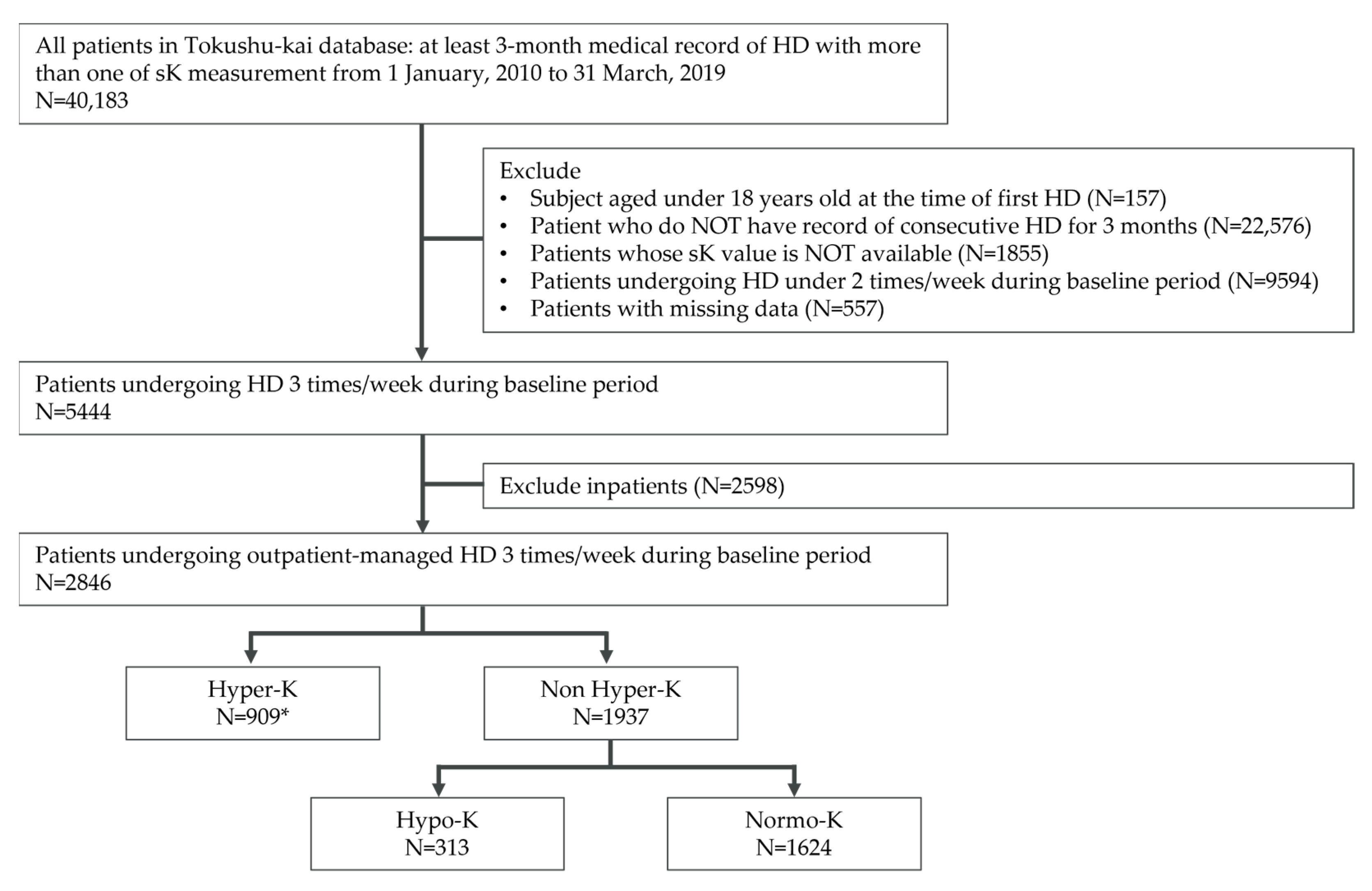
2.2. Study Population and Sample Size
2.3. Prevalence of Dyskalemia
2.4. Covariate and Outcome Measures
2.5. Statistical Analyses
3. Results
3.1. Prevalence of Dyskalemia
3.2. Baseline Outpatient Characteristics
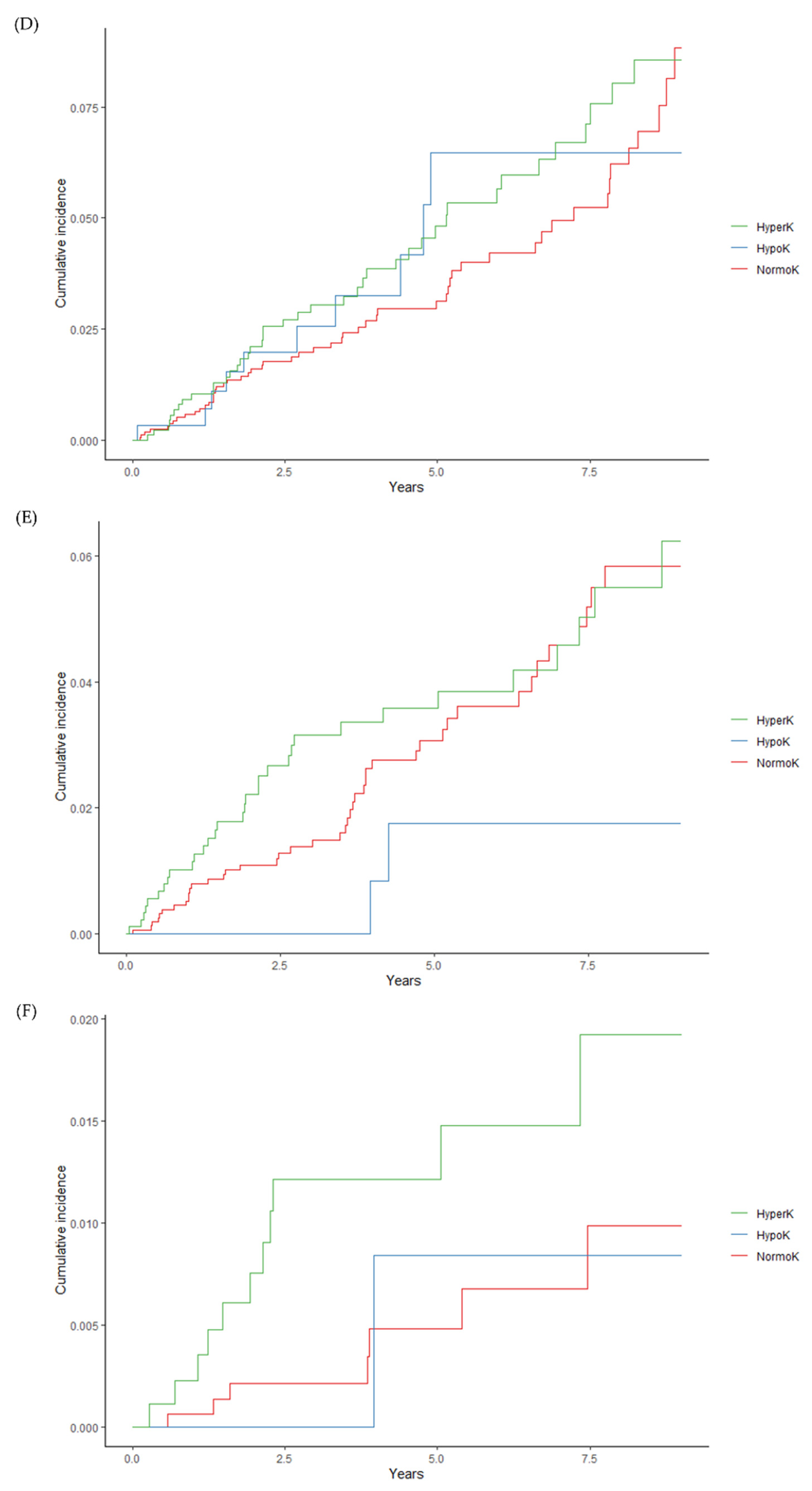
3.3. Clinical Outcomes
4. Discussion
4.1. Characteristics of Tokushu-kai Hospital Group Database
4.2. Association of Hypo-K with Baseline Characteristics and Outcomes
4.3. Association of Hyper-K with Baseline Characteristics and Outcomes
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devereaux, P.J.; Schünemann, H.J.; Ravindran, N.; Bhandari, M.; Garg, A.X.; Choi, P.T.; Grant, B.J.; Haines, T.; Lacchetti, C.; Weaver, B.; et al. Comparison of mortality between private for-profit and private not-for-profit hemodialysis centers: A systematic review and meta-analysis. JAMA 2002, 288, 2449–2457. [Google Scholar] [CrossRef] [PubMed]
- Eggers, P.W.; Frankenfield, D.L.; Greer, J.W.; McClellan, W.; Owen, W.F., Jr.; Rocco, M.V. Comparison of mortality and intermediate outcomes between medicare dialysis patients in HMO and fee for service. Am. J. Kidney Dis. 2002, 39, 796–804. [Google Scholar] [CrossRef] [PubMed]
- US Renal Data System 2022 Annul Data Report Figure 6.1a Mortality in Adult ESRD Patients, 2010–2020. Available online: https://usrds-adr.niddk.nih.gov/2022 (accessed on 31 December 2022).
- Arce, C.M.; Goldstein, B.A.; Mitani, A.A.; Winkelmayer, W.C. Trends in relative mortality between Hispanic and non-Hispanic whites initiating dialysis: A retrospective study of the US Renal Data System. Am. J. Kidney Dis. 2013, 62, 312–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucirka, L.M.; Grams, M.E.; Lessler, J.; Hall, E.C.; James, N.; Massie, A.B.; Montgomery, R.A.; Segev, D.L. Association of race and age with survival among patients undergoing dialysis. JAMA 2011, 306, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, G.; Norris, K.C.; Yu, A.J.; Ma, J.Z.; Greene, T.; Yu, W.; Cheung, A.K. The relationship of age, race, and ethnicity with survival in dialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 953–961. [Google Scholar] [CrossRef] [Green Version]
- Murthy, B.V.; Molony, D.A.; Stack, A.G. Survival advantage of Hispanic patients initiating dialysis in the United States is modified by race. J. Am. Soc. Nephrol. 2005, 16, 782–790. [Google Scholar] [CrossRef]
- Frankenfield, D.L.; Rocco, M.V.; Roman, S.H.; McClellan, W.M. Survival advantage for adult Hispanic hemodialysis patients? Findings from the end-stage renal disease clinical performance measures project. J. Am. Soc. Nephrol. 2003, 14, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Saran, R.; Li, Y.; Robinson, B.; Ayanian, J.; Balkrishnan, R.; Bragg-Gresham, J.; Chen, J.T.; Cope, E.; Gipson, D.; He, K.; et al. US Renal Data System 2014 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2015, 66, S1–S305. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P.; Regidor, D.L.; Mehrotra, R.; Jing, J.; McAllister, C.J.; Greenland, S.; Kopple, J.D.; Kalantar-Zadeh, K. Serum and dialysate potassium concentrations and survival in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2007, 2, 999–1007. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.Y.; Ha, S.K. Potassium balances in maintenance hemodialysis. Electrolytes Blood Press. 2013, 11, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, A.A.; Hu, Y.; Singh, B.; Menoyo, J.A.; Wetmore, J.B. Serum Potassium Levels and Mortality in Hemodialysis Patients: A Retrospective Cohort Study. Am. J. Nephrol. 2016, 44, 179–186. [Google Scholar] [CrossRef]
- Hayes, J.; Kalantar-Zadeh, K.; Lu, J.L.; Turban, S.; Anderson, J.E.; Kovesdy, C.P. Association of hypo- and hyperkalemia with disease progression and mortality in males with chronic kidney disease: The role of race. Nephron Clin. Pract. 2012, 120, c8–c16. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Rhee, C.M.; Streja, E.; Soohoo, M.; Obi, Y.; Chou, J.A.; Tortorici, A.R.; Ravel, V.A.; Kovesdy, C.P.; Kalantar-Zadeh, K. Racial and Ethnic Differences in Mortality Associated with Serum Potassium in a Large Hemodialysis Cohort. Am. J. Nephrol. 2017, 45, 509–521. [Google Scholar] [CrossRef] [Green Version]
- Karaboyas, A.; Robinson, B.M.; James, G.; Hedman, K.; Moreno Quinn, C.P.; De Sequera, P.; Nitta, K.; Pecoits-Filho, R. Hyperkalemia excursions are associated with an increased risk of mortality and hospitalizations in hemodialysis patients. Clin. Kidney J. 2021, 14, 1760–1769. [Google Scholar] [CrossRef]
- Iwagami, M.; Yasunaga, H.; Noiri, E.; Horiguchi, H.; Fushimi, K.; Matsubara, T.; Yahagi, N.; Nangaku, M.; Doi, K. Current state of continuous renal replacement therapy for acute kidney injury in Japanese intensive care units in 2011: Analysis of a national administrative database. Nephrol. Dial. Transpl. 2015, 30, 988–995. [Google Scholar] [CrossRef] [Green Version]
- Miyake, K.; Iwagami, M.; Ohtake, T.; Moriya, H.; Kume, N.; Murata, T.; Nishida, T.; Mochida, Y.; Isogai, N.; Ishioka, K.; et al. Association of pre-operative chronic kidney disease and acute kidney injury with in-hospital outcomes of emergency colorectal surgery: A cohort study. World J. Emerg. Surg. 2020, 15, 22. [Google Scholar] [CrossRef]
- Kubota, K.; Yoshizawa, M.; Takahashi, S.; Fujimura, Y.; Nomura, H.; Kohsaka, H. The validity of the claims-based definition of rheumatoid arthritis evaluated in 64 hospitals in Japan. BMC Musculoskelet. Disord. 2021, 22, 373. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI clinical practice guidelines for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2019, 76, S1–S107. [Google Scholar] [CrossRef]
- An Overview of Regular Dialysis Treatment in Japan. Report. 2019. Available online: https://docs.jsdt.or.jp/overview/index2020.html (accessed on 28 October 2022).
- Ohnishi, T.; Kimachi, M.; Fukuma, S.; Akizawa, T.; Fukuhara, S. Postdialysis Hypokalemia and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 873. [Google Scholar] [CrossRef] [Green Version]
- Sumida, K.; Dashputre, A.A.; Potukuchi, P.K.; Thomas, F.; Obi, Y.; Molnar, M.Z.; Gatwood, J.D.; Streja, E.; Kalantar-Zadeh, K.; Kovesdy, C.P. Laxative Use and Risk of Dyskalemia in Patients with Advanced CKD Transitioning to Dialysis. J. Am. Soc. Nephrol. 2021, 32, 950–959. [Google Scholar] [CrossRef]
- Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am. J. Kidney Dis. 2000, 35, S17–S104. [CrossRef]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantar-Zadeh, K. Recent advances in understanding the malnutrition-inflammation-cachexia syndrome in chronic kidney disease patients: What is next? Semin. Dial. 2005, 18, 365–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carracedo, J.; Alique, M.; Vida, C.; Bodega, G.; Ceprián, N.; Morales, E.; Praga, M.; de Sequera, P.; Ramírez, R. Mechanisms of Cardiovascular Disorders in Patients with Chronic Kidney Disease: A Process Related to Accelerated Senescence. Front. Cell Dev. Biol. 2020, 8, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahathevan, S.; Khor, B.-H.; Ng, H.-M.; Gafor, A.H.A.; Mat Daud, Z.A.; Mafra, D.; Karupaiah, T. Understanding Development of Malnutrition in Hemodialysis Patients: A Narrative Review. Nutrients 2020, 12, 3147. [Google Scholar] [CrossRef]
- Cobo, G.; Lindholm, B.; Stenvinkel, P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol. Dial. Transpl. 2018, 33, iii35–iii40. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Streja, E.; Soohoo, M.; Rhee, C.M.; Eriguchi, R.; Kim, T.W.; Chang, T.I.; Obi, Y.; Kovesdy, C.P.; Kalantar-Zadeh, K. Serum Ferritin Variations and Mortality in Incident Hemodialysis Patients. Am. J. Nephrol. 2017, 46, 120–130. [Google Scholar] [CrossRef]
- Johansen, K.L.; Chertow, G.M.; Jin, C.; Kutner, N.G. Significance of frailty among dialysis patients. J. Am. Soc. Nephrol. 2007, 18, 2960–2967. [Google Scholar] [CrossRef] [Green Version]
- Jassal, S.V.; Karaboyas, A.; Comment, L.A.; Bieber, B.A.; Morgenstern, H.; Sen, A.; Gillespie, B.W.; De Sequera, P.; Marshall, M.R.; Fukuhara, S.; et al. Functional Dependence and Mortality in the International Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2016, 67, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Kanda, E.; Lopes, M.B.; Tsuruya, K.; Hirakata, H.; Iseki, K.; Karaboyas, A.; Bieber, B.; Jacobson, S.H.; Dasgupta, I.; Robinson, B.M. The combination of malnutrition-inflammation and functional status limitations is associated with mortality in hemodialysis patients. Sci. Rep. 2021, 11, 1582. [Google Scholar] [CrossRef]
- Feroze, U.; Noori, N.; Kovesdy, C.P.; Molnar, M.Z.; Martin, D.J.; Reina-Patton, A.; Benner, D.; Bross, R.; Norris, K.C.; Kopple, J.D.; et al. Quality-of-life and mortality in hemodialysis patients: Roles of race and nutritional status. Clin. J. Am. Soc. Nephrol. 2011, 6, 1100–1111. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Tortorici, A.R.; Chen, J.L.; Kamgar, M.; Lau, W.L.; Moradi, H.; Rhee, C.M.; Streja, E.; Kovesdy, C.P. Dietary restrictions in dialysis patients: Is there anything left to eat? Semin. Dial. 2015, 28, 159–168. [Google Scholar] [CrossRef] [Green Version]
- Moroi, M.; Tamaki, N.; Nishimura, M.; Haze, K.; Nishimura, T.; Kusano, E.; Akiba, T.; Sugimoto, T.; Hase, H.; Hara, K.; et al. Association between abnormal myocardial fatty acid metabolism and cardiac-derived death among patients undergoing hemodialysis: Results from a cohort study in Japan. Am. J. Kidney Dis. 2013, 61, 466–475. [Google Scholar] [CrossRef]
- Hiyamuta, H.; Tanaka, S.; Taniguchi, M.; Tokumoto, M.; Fujisaki, K.; Nakano, T.; Tsuruya, K.; Kitazono, T. The Incidence and Associated Factors of Sudden Death in Patients on Hemodialysis: 10-Year Outcome of the Q-Cohort Study. J. Atheroscler. Thromb. 2020, 27, 306–318. [Google Scholar] [CrossRef] [Green Version]
- Goodkin, D.; Bragg-Gresham, J.; Koenig, K.; Wolfe, R.; Akiba, T.; Andreucci, V.; Saito, A.; Rayner, H.; Kurokawa, K.; Port, F.; et al. Association of Comorbid Conditions and Mortality in Hemodialysis Patients in Europe, Japan, and the United States: The Dialysis Outcomes and Practice Patterns Study (DOPPS). J. Am. Soc. Nephrol. JASN 2003, 14, 3270–3277. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based Diets Are Associated with a Lower Risk of Incident Cardiovascular Disease, Cardiovascular Disease Mortality, and All-Cause Mortality in a General Population of Middle-Aged Adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar] [CrossRef]
- Chen, X.; Wei, G.; Jalili, T.; Metos, J.; Giri, A.; Cho, M.E.; Boucher, R.; Greene, T.; Beddhu, S. The Associations of Plant Protein Intake with All-Cause Mortality in CKD. Am. J. Kidney Dis. 2016, 67, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Noori, N.; Kalantar-Zadeh, K.; Kovesdy, C.P.; Murali, S.B.; Bross, R.; Nissenson, A.R.; Kopple, J.D. Dietary potassium intake and mortality in long-term hemodialysis patients. Am. J. Kidney Dis. 2010, 56, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Karaboyas, A.; Zee, J.; Brunelli, S.M.; Usvyat, L.A.; Weiner, D.E.; Maddux, F.W.; Nissenson, A.R.; Jadoul, M.; Locatelli, F.; Winkelmayer, W.C.; et al. Dialysate Potassium, Serum Potassium, Mortality, and Arrhythmia Events in Hemodialysis: Results From the Di-alysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2017, 69, 266–277. [Google Scholar] [CrossRef] [Green Version]
- Brunelli, S.M.; Spiegel, D.M.; Du Mond, C.; Oestreicher, N.; Winkelmayer, W.C.; Kovesdy, C.P. Serum-to-dialysate potassium gradient and its association with short-term outcomes in hemodialysis patients. Nephrol. Dial. Transpl. 2018, 33, 1207–1214. [Google Scholar] [CrossRef] [Green Version]
- Kashihara, N.; Kohsaka, S.; Kanda, E.; Okami, S.; Yajima, T. Hyperkalemia in Real-World Patients Under Continuous Medical Care in Japan. Kidney Int. Rep. 2019, 4, 1248–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall | Hyper-K Group | Hypo-K Group | Normo-K Group |
|---|---|---|---|---|
| n = 2846 | n = 909 (31.94%) | n = 313 (11.00%) | n = 1624 (57.06%) | |
| Age, year (mean ± SD) | 65.65 ± 12.63 | 65.03 ± 11.95 | 69.37 ± 12.68 | 65.28 ± 12.87 |
| Male, n (%) | 1909 (67.08) | 608 (66.89) | 194 (61.98) | 1107 (68.17) |
| BMI, kg/m2 (mean ± SD) | 22.4 ± 8.79 | 22.25 ± 6.68 | 21.37 ± 3.59 | 22.65 ± 10.26 |
| Dialysis vintage at baseline, median years (min, max) | 3.07 (0.10, 37.29) | 4.27 (0.23, 37.29) | 1.49 (0.24, 27.09) | 2.70 (0.10, 36.94) |
| 2.0 mEq/L potassium dialysate, n (%) | 2846 (100.00) | 909 (100.00) | 313 (100.00) | 1624 (100.00) |
| Kt/V (mean ± SD) | 1.37 ± 0.31 | 1.40 ± 0.30 | 1.33 ± 0.32 | 1.36 ± 0.31 |
| Potassium, mEq/L (mean ± SD) | 4.75 ± 0.77 | 5.44 ± 0.58 | 3.75 ± 0.65 | 4.55 ± 0.51 |
| Calcium, mg/dL (mean ± SD) | 8.73 ± 0.81 | 8.80 ± 0.81 | 8.51 ± 0.75 | 8.73 ± 0.82 |
| Phosphorus, mg/dL (mean ± SD) | 5.45 ± 1.48 | 5.85 ± 1.48 | 4.70 ± 1.55 | 5.36 ± 1.40 |
| Hemoglobin, g/dL (mean ± SD) | 10.79 ± 1.34 | 10.82 ± 1.30 | 10.64 ± 1.55 | 10.80 ± 1.32 |
| Total protein, g/dL (mean ± SD) | 6.48 ± 0.58 | 6.48 ± 0.57 | 6.36 ± 0.69 | 6.49 ± 0.56 |
| Albumin, g/dL (mean ± SD) | 3.63 ± 0.43 | 3.70 ± 0.39 | 3.41 ± 0.53 | 3.64 ± 0.42 |
| Creatinine, mg/dL (mean ± SD) | 9.77 ± 2.88 | 10.54 ± 2.73 | 7.69 ± 2.58 | 9.74 ± 2.82 |
| URR, % (mean ± SD) | 66.12 ± 8.34 | 66.57 ± 8.00 | 66.36 ± 8.83 | 65.81 ± 8.42 |
| nPCR, g/kg/day (mean ± SD) | 0.83 ± 0.24 | 0.84 ± 0.36 | 0.79 ± 0.07 | 0.83 ± 0.15 |
| GNRI (mean ± SD) | 93.08 ± 7.41 | 94.15 ± 7.26 | 90.51 ± 9.16 | 92.92 ± 7.07 |
| Ferritin, ng/mL (median; min, max) | 77.80 (0.07, 1970.0) | 75.20 (0.19, 1900.9) | 82.95 (0.07, 1970.0) | 77.15 (0.17, 1961.3) |
| CRP, mg/dL (median; min, max) | 0.11 (0.00, 39.47) | 0.10 (0.01, 39.47) | 0.20 (0.01, 11.03) | 0.11 (0.00, 17.94) |
| Comorbidities, n (%) | ||||
| Diabetes | 1558 (54.74) | 484 (53.25) | 191 (61.02) | 883 (54.37) |
| Hypertension | 2587 (90.90) | 832 (91.53) | 281 (89.78) | 1474 (90.76) |
| Heart failure | 1163 (40.86) | 371 (40.81) | 126 (40.26) | 666 (41.01) |
| Cardiac arrest | 6 (0.21) | 5 (0.55) | 1 (0.32) | 0 (0.00) |
| Myocardial infarction | 61 (2.41) | 23 (2.53) | 5 (1.60) | 33 (2.03) |
| Stroke | 383 (13.46) | 123 (13.53) | 34 (10.86) | 226 (13.92) |
| Peripheral vascular diseases | 974 (34.22) | 331 (36.41) | 94 (30.03) | 549 (33.81) |
| Cerebrovascular diseases | 797 (28.00) | 249 (27.39) | 93 (29.71) | 455 (28.02) |
| Dementia | 115 (4.04) | 18 (1.98) | 38 (12.14) | 59 (3.63) |
| Sarcopenia | 213 (7.48) | 56 (6.16) | 40 (12.78) | 117 (7.20) |
| Medications, n (%) | ||||
| β-blockers | 671 (23.58) | 227 (24.97) | 67 (21.41) | 377 (23.21) |
| RAASi (ACEi/ARB/MRA) | 1474 (51.79) | 544 (59.85) | 139 (44.41) | 791 (48.71) |
| ACEi | 168 (5.90) | 69 (7.59) | 22 (7.03) | 77 (4.74) |
| ARB | 1406 (49.40) | 522 (57.43) | 128 (40.89) | 756 (46.55) |
| MRA | 22 (0.77) | 2 (0.22) | 3 (0.96) | 17 (1.05) |
| Laxative agent | 1082 (38.02) | 289 (31.79) | 169 (53.99) | 624 (38.42) |
| Potassium adsorbents (SPS/CPS) | 384 (13.49) | 193 (21.23) | 20 (6.39) | 171 (10.53) |
| CPS | 311 (10.93) | 149 (16.39) | 14 (4.47) | 148 (9.11) |
| SPS | 91 (3.20) | 52 (5.72) | 7 (2.24) | 32 (1.97) |
| Potassium supplements | 16 (0.56) | 1 (0.11) | 7 (2.24) | 8 (0.49) |
| Nutritional guidance | 1555 (54.64) | 489 (53.80) | 202 (64.54) | 864 (53.20) |
| N | 100 Person-Year | Hazard Ratio (95% C.I.) | ||
|---|---|---|---|---|
| Crude | Adjusted a | |||
| All-cause mortality | ||||
| Hyper-K (n = 909) | 314 | 7.50 | 1.01 (0.87, 1.16) | 0.92 (0.78, 1.09) |
| Hypo-K (n = 313) | 120 | 11.29 | 1.58 (1.30, 1.94) | 1.47 (1.13, 1.92) |
| Normo-K (n = 1624) | 513 | 7.41 | 1.00 (Reference) | 1.00 (Reference) |
| MACE | ||||
| Hyper-K (n = 909) | 415 | 10.88 | 1.02 (0.91, 1.16) | 0.97 (0.84, 1.12) |
| Hypo-K (n = 313) | 152 | 16.29 | 1.57 (1.31, 1.87) | 1.48 (1.17, 1.86) |
| Normo-K (n = 1624) | 671 | 10.63 | 1.00 (Reference) | 1.00 (Reference) |
| Hospitalization | ||||
| Hyper-K (n = 909) | 751 | 41.97 | 1.14 (1.04, 1.24) | 1.09 (0.98, 1.22) |
| Hypo-K (n = 313) | 227 | 43.54 | 1.13 (0.98, 1.31) | 1.13 (0.94, 1.37) |
| Normo-K (n = 1624) | 1216 | 37.00 | 1.00 (Reference) | 1.00 (Reference) |
| Cardiac arrest | ||||
| Hyper-K (n = 909) | 41 | 0.98 | 1.24 (0.83, 1.86) | 1.30 (0.80, 2.12) |
| Hypo-K (n = 313) | 10 | 0.94 | 1.31 (0.66, 2.60) | 1.41 (0.58, 3.38) |
| Normo-K (n = 1624) | 54 | 0.78 | 1.00 (Reference) | 1.00 (Reference) |
| Fatal arrythmia | ||||
| Hyper-K (n = 909) | 32 | 0.78 | 1.25 (0.79, 1.97) | 1.44 (0.86, 2.39) |
| Hypo-K (n = 313) | 2 | 0.19 | 0.31 (0.08, 1.30) | 0.28 (0.04, 2.16) |
| Normo-K (n = 1624) | 43 | 0.63 | 1.00 (Reference) | 1.00 (Reference) |
| Death related to arrythmia | ||||
| Hyper-K (n = 909) | 11 | 0.26 | 2.65 (1.03, 6.84) | 3.11 (1.03, 9.33) |
| Hypo-K (n = 313) | 1 | 0.09 | 0.98 (0.12, 8.07) | 2.65 (0.31, 22.89) |
| Normo-K (n = 1624) | 7 | 0.10 | 1.00 (Reference) | 1.00 (Reference) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwagami, M.; Kanemura, Y.; Morita, N.; Yajima, T.; Fukagawa, M.; Kobayashi, S. Association of Hyperkalemia and Hypokalemia with Patient Characteristics and Clinical Outcomes in Japanese Hemodialysis (HD) Patients. J. Clin. Med. 2023, 12, 2115. https://doi.org/10.3390/jcm12062115
Iwagami M, Kanemura Y, Morita N, Yajima T, Fukagawa M, Kobayashi S. Association of Hyperkalemia and Hypokalemia with Patient Characteristics and Clinical Outcomes in Japanese Hemodialysis (HD) Patients. Journal of Clinical Medicine. 2023; 12(6):2115. https://doi.org/10.3390/jcm12062115
Chicago/Turabian StyleIwagami, Masao, Yuka Kanemura, Naru Morita, Toshitaka Yajima, Masafumi Fukagawa, and Shuzo Kobayashi. 2023. "Association of Hyperkalemia and Hypokalemia with Patient Characteristics and Clinical Outcomes in Japanese Hemodialysis (HD) Patients" Journal of Clinical Medicine 12, no. 6: 2115. https://doi.org/10.3390/jcm12062115