
Does Anxiety Affect Survival in Patients with Coronary Heart Disease?
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
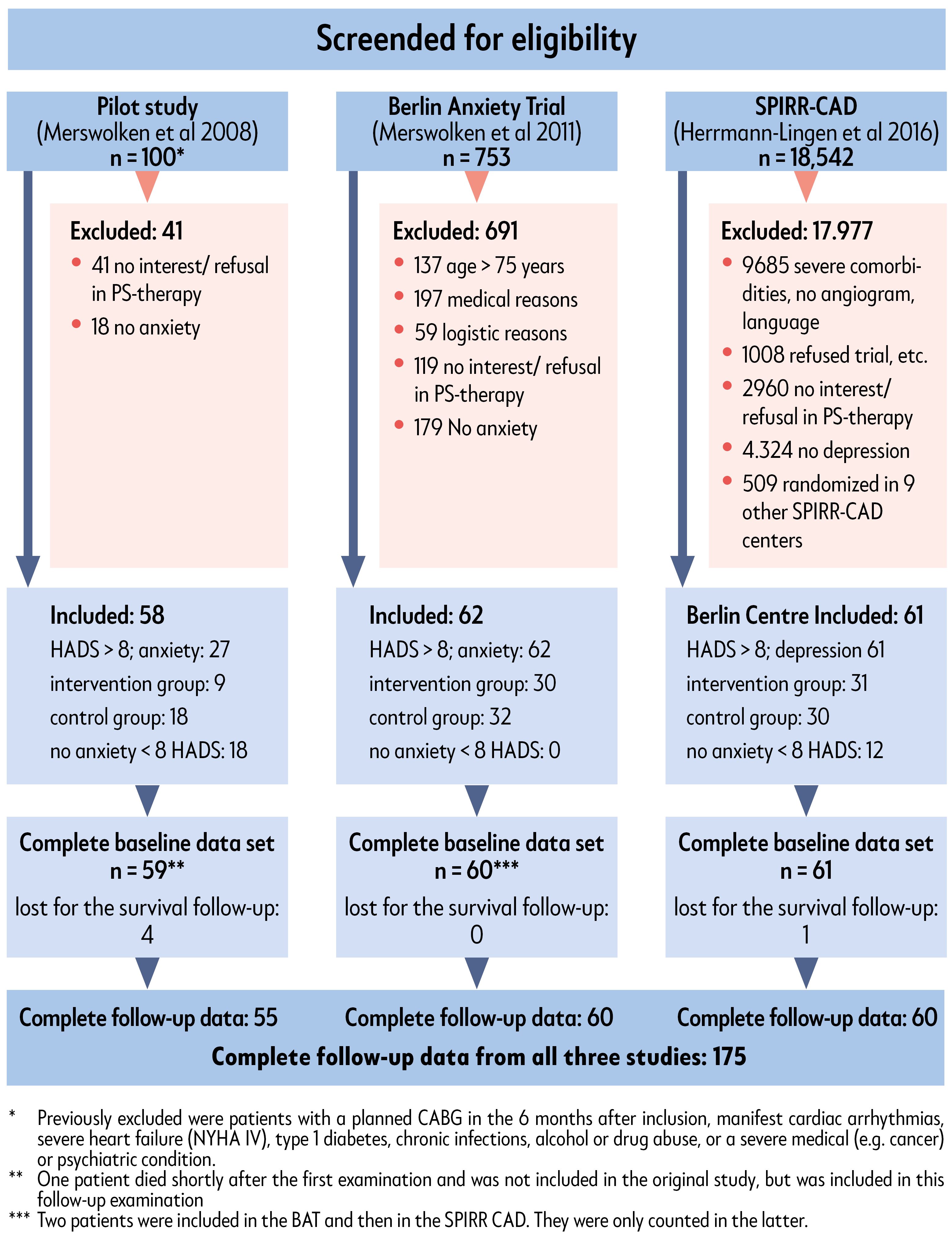
2.1. Study Sample
2.2. Data Collection
2.3. Study Design
2.4. Psychosocial Measures
- The 14-item type D scale (DS-14) [30], with the social inhibition and negative affectivity subscales.
- Structured rating interviews for the assessment of Axis I mental disorders, according to DSM-IV, applied by using the SCID [31] in the SPIRR-CAD subgroup and the DIPS [32] in the anxiety trial subgroup, respectively, to diagnose anxiety disorders in our sample. In this way, anxiety disorders (panic disorder, phobias, generalized anxiety disorder) were assessed in this study for the two subgroups. In the third subgroup (pilot study), a diagnostic interview could not be applied.
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics (Table 1)
3.2. Six-Month Follow-Up
3.3. Twelve-Year Follow-Up
4. Discussion
- (1)
- Between anxiety as risk of incident coronary heart disease, which has demonstrated convincing effects [33].
- (2)
- That after a cardiovascular event, anxiety as a trigger for new cardiovascular events in a short time perspective seems to be a risk [7,9]. An altered autonomic tone and increased susceptibility (e.g., to malignant arrhythmias), could be a possible pathway for increased mortality in patients with electrically unstable hearts after MACE.
- (3)
- In a long-term perspective, several samples have shown that anxiety is not a risk factor, 5 years after exercise testing [1,34] or 5 years after coronary stenting [15]. It is not clear to what extent self-selection for exercise testing or coronary stenting was influenced, besides by physicians’ decision, patients’ anxiety behavior or whether all patients were CHD patients or physically healthy anxiety patients [1]. In this study, we had a special selection of CHD patients who were interested in and participated in a psychosocial intervention study. The follow-up time was significantly longer at 12 years compared to former studies. It seems that anxiety in an early phase after MACE is associated with further MACE. At longer follow-up, anxiety seems to change its negative association with CHD. Additionally other factors could also play a role here. Besides low anxiety, we additionally found age and smoking in a regression analysis, and in a larger predictor model LVEF, as significant indicators of a severe disease and a well-known risk factor. Against our expectations, a previous MI, physical activity, and food intake could not predict all-cause mortality [34].
- Treatment Aspects
- Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrmann, C.; Brand-Driehorst, S.; Buss, U.; Rüger, U. Effects of anxiety and depression on 5-year mortality in 5057 patients referred for exercise testing. J. Psychosom. Res. 2000, 48, 455–462. [Google Scholar] [CrossRef]
- Fleet, R.; Lavoie, K.; Beitman, B.D. Is panic disorder associated with coronary artery disease? A critical review of the literature. J. Psychosom. Res. 2000, 48, 347–356. [Google Scholar] [CrossRef]
- Bankier, B.; Januzzi, J.L.; Littman, A.B. The High Prevalence of Multiple Psychiatric Disorders in Stable Outpatients With Coronary Heart Disease. Psychosom. Med. 2004, 66, 645–650. [Google Scholar] [CrossRef]
- Frasure-Smith, N.; Lespérance, F.; Gravel, G.M.; Masson, A.M.; Juneau, M.M.; Bourassa, M.G. Long-Term Survival Differences Among Low-Anxious, High-Anxious and Repressive Copers Enrolled in the Montreal Heart Attack Readjustment Trial. Psychosom. Med. 2002, 64, 571–579. [Google Scholar] [CrossRef]
- Huffman, J.C.; Smith, F.A.; Blais, M.A.; Januzzi, J.L.; Fricchione, G.L. Anxiety, independent of depressive symptoms, is associated with in-hospital cardiac complications after acute myocardial infarction. J. Psychosom. Res. 2008, 65, 557–563. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Stern, T.A.; Pasternak, R.C.; DeSanctis, R.W. The influence of anxiety and depression on outcomes of patients with coronary artery disease. Arch. Intern. Med. 2000, 160, 1913–1921. [Google Scholar] [CrossRef] [Green Version]
- Frasure-Smith, N.; Lespérance, F. Depression and Anxiety as Predictors of 2-Year Cardiac Events in Patients With Stable Coronary Artery Disease. Arch. Gen. Psychiatry 2008, 65, 62–71. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.D.; LaCroix, A.Z.; Spertus, J.A.; Hecht, J. Five-year prospective study of the effects of anxiety and depression in patients with coronary artery disease. Am. J. Cardiol. 2000, 86, 1135–1138. [Google Scholar] [CrossRef]
- Roest, A.; Martens, E.J.; Denollet, J.; de Jonge, P. Prognostic Association of Anxiety Post Myocardial Infarction With Mortality and New Cardiac Events: A Meta-Analysis. Psychosom. Med. 2010, 72, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Fan, A.Z.; Strine, T.W.; Jiles, R.; Mokdad, A.H. Depression and anxiety associated with cardiovascular disease among persons aged 45 years and older in 38 states of the United States, 2006. Prev. Med. 2008, 46, 445–450. [Google Scholar] [CrossRef]
- Scherrer, J.F.; Chrusciel, T.; Zeringue, A.; Garfield, L.D.; Hauptman, P.J.; Lustman, P.J.; Freedland, K.E.; Carney, R.M.; Bucholz, K.K.; Owen, R.; et al. Anxiety disorders increase risk for incident myocardial infarction in depressed and nondepressed Veterans Administration patients. Am. Heart J. 2010, 159, 772–779. [Google Scholar] [CrossRef]
- Phillips, A.C.; Batty, G.D.; Gale, C.R.; Deary, I.J.; Osborn, D.; MacIntyre, K.; Carroll, D. Generalized Anxiety Disorder, Major Depressive Disorder, and Their Comorbidity as Predictors of All-Cause and Cardiovascular Mortality: The Vietnam Experience Study. Psychosom. Med. 2009, 71, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Grace, S.L.; Abbey, S.E.; Irvine, J.; Shnek, Z.M.; Stewart, D.E. Prospective Examination of Anxiety Persistence and Its Relationship to Cardiac Symptoms and Recurrent Cardiac Events. Psychother. Psychosom. 2004, 73, 344–352. [Google Scholar] [CrossRef]
- Tully, P.J.; Turnbull, D.A.; Beltrame, J.; Horowitz, J.; Cosh, S.; Baumeister, H.; Wittert, G.A. Panic disorder and incident coronary heart disease: A systematic review and meta-regression in 1 131 612 persons and 58 111 cardiac events. Psychol. Med. 2015, 45, 2909–2920. [Google Scholar] [CrossRef]
- Meyer, T.; Hussein, S.; Lange, H.W.; Herrmann-Lingen, C. Anxiety is associated with a reduction in both mortality and major adverse cardiovascular events five years after coronary stenting. Eur. J. Prev. Cardiol. 2013, 22, 75–82. [Google Scholar] [CrossRef]
- Bishop, S.J.; Duncan, J.; Lawrence, A.D. State Anxiety Modulation of the Amygdala Response to Unattended Threat-Related Stimuli. J. Neurosci. 2004, 24, 10364–10368. [Google Scholar] [CrossRef] [Green Version]
- Merswolken, M.; Deter, H.-C.; Siebenhuener, S.; Orth-Gomér, K.; Weber, C.S. Anxiety as Predictor of the Cortisol Awakening Response in Patients with Coronary Heart Disease. Int. J. Behav. Med. 2012, 20, 461–467. [Google Scholar] [CrossRef]
- Weber, C.; Fangauf, S.V.; Michal, M.; Ronel, J.; Herrmann-Lingen, C.; Ladwig, K.-H.; Beutel, M.; Albus, C.; Söllner, W.; Perschel, F.H.; et al. Cortisol Awakening Reaction and Anxiety in Depressed Coronary Artery Disease Patients. J. Clin. Med. 2022, 11, 374. [Google Scholar] [CrossRef]
- Watkins, L.L.; Blumenthal, J.A.; Davidson, J.R.T.; Babyak, M.A.; McCants, C.B.; Sketch, M.H. Phobic Anxiety, Depression, and Risk of Ventricular Arrhythmias in Patients With Coronary Heart Disease. Psychosom. Med. 2006, 68, 651–656. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Binder, L.; Klinge, M.; Sander, J.; Schenker, W.; Beyermann, B.; Von Lewinski, D.; Pieske, B. High Plasma Levels of N-Terminal Pro-Atrial Natriuretic Peptide Associated With Low Anxiety in Severe Heart Failure. Psychosom. Med. 2003, 65, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Fangauf, S.V.; Meyer, T.; Albus, C.; Binder, L.; Deter, H.-C.; Ladwig, K.-H.; Michal, M.; Ronel, J.; Rothenberger, A.; Söllner, W.; et al. Longitudinal relationship between B-type natriuretic peptide and anxiety in coronary heart disease patients with depression. J. Psychosom. Res. 2019, 123, 109728. [Google Scholar] [CrossRef] [PubMed]
- Van Elderen, T.; Maes, S.; Dusseldorp, E. Coping with coronary heart disease: A longitudinal study. J. Psychosom. Res. 1999, 47, 175–183. [Google Scholar] [CrossRef]
- Celano, C.M.; Rachel AMillstein, R.M.; Bedoya, C.A.; Healy, B.C.; Roest, A.; Huffman, J.C. Association between anxiety and mortality in patients with coronary artery disease: A meta-analysis. Am. Heart J. 2015, 170, 1105–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merswolken, M.; Albert, W.; Orth-Gomér, K.; Pauschinger, M.; Deter, H.-C. Symptoms of depression and anxiety in patients with coronary heart disease: Natural course and results of a psychotherapeutic pilot study. Z. Psychosom. Med. Psychother. 2008, 54, 381–392. [Google Scholar] [PubMed]
- Merswolken, M.; Siebenhuener, S.; Orth-Gomér, K.; Zimmermann-Viehoff, F.; Deter, H.-C. Treating Anxiety in Patients with Coronary Heart Disease: A Randomized Controlled Trial. Psychother. Psychosom. 2011, 80, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Herrmann-Lingen, C.; Beutel, M.; Bosbach, A.; Deter, H.C.; Fritzsche, K.; Hellmich, M.; Jordan, J.; Jünger, J.; Ladwig, K.H.; Michal, M.; et al. A Stepwise Psychotherapy Intervention for Reducing Risk in Coronary Artery Disease (SPIRR-CAD): Results of an Observer-Blinded, Multicenter, Randomized Trial in Depressed Patients With Coronary Artery Disease. Psychosom. Med. 2016, 78, 704–715. [Google Scholar] [CrossRef]
- Grün, A.S.; Weber, C. Social support, gender, and other psychosocial predictors of survival of CHD patients. J. Psychosom. Res. 2023. submitted. [Google Scholar]
- Herrmann, C.; Buss, U.; Snaith, R.P. HADS-D-Hospital Anxiety and Depression Scale-Deutsche Version; Huber: Bern, Switzerland, 1995. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Denollet, J. DS14: Standard Assessment of Negative Affectivity, Social Inhibition, and Type D Personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef]
- Wittchen, H.; Zaudig, M.; Fydrich, T. Strukturiertes Klinisches Interview für DSMIV (SKID I und SKID-II); Hogrefe: Göttingen, Germany, 1997. [Google Scholar]
- Schneider, S.; Margraf, J. DIPS: Diagnostisches Interview bei Psychischen Störungen; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Roest, A.M.; Martens, E.J.; de Jonge, P.; Denollet, J. Anxiety and Risk of Incident Coronary Heart Disease: A Meta-Analysis. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Meyer, T.; Buss, U.; Herrmann-Lingen, C. Role of Cardiac Disease Severity in the Predictive Value of Anxiety for All-Cause Mortality. Psychosom. Med. 2010, 72, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Smith, P.J.; Jiang, W.; Hinderliter, A.; Watkins, L.L.; Hoffman, B.M.; Kraus, W.E.; Mabe, S.; Liao, L.; Davidson, J.; et al. Exercise and Escitalopram in the Treatment of Anxiety in Patients with Coronary Heart Disease: One Year Follow-Up of the UNWIND Randomized Clinical Trial. J. Cardiovasc. Dev. Dis. 2022, 9, 320. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Smith, P.J.; Jiang, W.; Hinderliter, A.; Watkins, L.L.; Hoffman, B.M.; Kraus, W.E.; Liao, L.; Davidson, J.; Sherwood, A. Effect of Exercise, Escitalopram, or Placebo on Anxiety in Patients with Coronary Heart Disease: The Understanding the Benefits of Exercise and Escitalopram in Anxious Patients with Coronary Heart Disease (UNWIND) Randomized Clinical Trial. JAMA Psychiatry 2021, 78, 1270. [Google Scholar] [CrossRef] [PubMed]
- Buigues, C.; Queralt, A.; De Velasco, J.; Salvador-Sanz, A.; Jennings, C.; Wood, D.; Trapero, I. Psycho-Social Factors in Patients with Cardiovascular Disease Attending a Family-Centred Prevention and Rehabilitation Programme: EUROACTION Model in Spain. Life 2021, 11, 89. [Google Scholar] [CrossRef] [PubMed]
- Orth-Gomér, K.; Schneidermann, N.; Wang, H.X.; Walldin, C.; Blom, M.; Jernberg, T. Stress reduction prolongs life in women with coronary disease. The Stockholm Women’s Intervention Trial for Coronary Heart Disease (SWITCHD). Circ. Cardiovasc. Qual. Outcomes 2009, 2, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, K.; Bennett, P.; West, R.; Davey Smith, G.; Ebrahim, S. Psychological interventions for coronary heart disease. Cochrane Libr. 2004, 4, 1–47. [Google Scholar]
- Albus, C.; Theissen, P.; Hellmich, M.; Griebenow, R.; Wilhelm, B.; Aslim, D.; Schicha, H.; Köhle, K. Long-Term Effects of a Multimodal Behavioral Intervention on Myocardial Perfusion—A Randomized Controlled Trial. Int. J. Behav. Med. 2009, 16, 219–226. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Buss, U. Angst und Depressivität im Verlauf der Koronaren Herzkrankheit. Reihe Statuskonferenz Psychokardiologie; VAS-Verlag: Frankfurt, Germany, 2002. [Google Scholar]
- Strik, J.J.; Denollet, J.; Lousberg, R.; Honig, A. Comparing symptoms of depression and anxiety as predictors of cardiac events and increased health care consumption after myocardial infarction. J. Am. Coll. Cardiol. 2003, 42, 1801–1807. [Google Scholar] [CrossRef] [Green Version]
- Shen, B.-J.; Avivi, Y.E.; Todaro, J.F.; Spiro, A.; Laurenceau, J.-P.; Ward, K.D.; Niaura, R. Anxiety Characteristics Independently and Prospectively Predict Myocardial Infarction in Men: The Unique Contribution of Anxiety Among Psychologic Factors. J. Am. Coll. Cardiol. 2008, 51, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Ströhle, A.; Holsboer, F. Stress Responsive Neurohormones in Depression and Anxiety. Pharmacopsychiatry 2003, 36 (Suppl. 3), 207–214. [Google Scholar] [CrossRef]
- Dimsdale, J.E. What Does Heart Disease Have to Do With Anxiety? J. Am. Coll. Cardiol. 2010, 56, 47–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| No Anxiety HADS-A 0–7 N = 48 | Moderate Anxiety HADS-A 8–12 N = 88 | High Anxiety HADS-A 13–18 N = 44 | Chi-Square p | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Male sex | 35 | 72.9 | 66 | 75 | 32 | 72.7 | 0.95 |
| Married | 16 | 55.1 | 56 | 71.8 | 28 | 70 | 0.47. |
| Socioeconomic status | 0.47 | ||||||
| Low | 4 | 33.3 | 13 | 43.3 | 5 | 26.3 | |
| Medium | 4 | 33.3 | 13 | 43.3 | 8 | 42.1 | |
| High | 4 | 33.3 | 4 | 13.3 | 6 | 31.6 | |
| Previous MI (n = 176) | 20 | 43.5 | 51 | 58.6 | 23 | 52.3 | 0.21 |
| NYHA class (n = 127) | <0.001 | ||||||
| I | 3 | 18.8 | 30 | 41.7 | 18 | 46.2 | |
| II | 10 | 62.5 | 42 | 58.3 | 21 | 53.8 | |
| III + IV | 3 | 18.8 | 0 | 0 | |||
| Hyperlipidemia (n = 177) | 39 | 81.3 | 75 | 86.2 | 40 | 90.9 | 0.62 |
| Hypertension (n = 178) | 38 | 80.9 | 73 | 83.9 | 38 | 86.4 | 0.63 |
| Diabetes mellitus (n = 176) | 13 | 27.1 | 19 | 21.8 | 13 | 29.5 | 0.56 |
| Smoking (n = 134) | 14 | 70 | 27 | 36.0 | 12. | 30.8 | 0.009 |
| Beta-blocker (n = 122) | 11 | 91.7 | 68 | 95.8 | 38 | 97.4 | 0.68 |
| Statins | 12 | 100 | 68 | 95.8 | 39 | 100 | 0.33 |
| M | SD | M | SD | M | SD | Kruskal–Wallis p | |
| Age years (n = 180) | 65.0 | 9.0 | 60.3 | 8.7 | 60.8 | 9.5 | <0.001 1:2; 1:3 |
| BMI (n = 156) | 24.2 | 11.9 | 27.4 | 4.1 | 28.5 | 6.5 | 0.23 |
| LVEF | 56.2 | 14.9 | 58.9 | 12.9 | 59.8 | 10.7 | 0.53 |
| CCI | 2.5 | 1.4 | 1.9 | 1.2 | 1.8 | 1.1 | 0.21 |
| Aerobic exercise (min/week) (n = 100) | 290.0 | 117.6 | 235.1 | 181.0 | 369.4 | 297.3 | 0.08 |
| No Anxiety HADS A <8 N = 48 | Moderate Anxiety HADS A 8–12 N = 88 | High Anxiety HADS-A >12 N = 44 | Kruskal Wallis Test p | ||||
|---|---|---|---|---|---|---|---|
| Pilot *: N = 36 | Pilot: N = 17 | Pilot: N = 4 | |||||
| AS *: N = 0 | AS: N = 41 | AS: N = 21 | |||||
| SPIRR *: N = 12 | SPIRR: N = 30 | SPIRR: N = 19 | |||||
| M | SD | M | SD | M | SD | ||
| HADS anxiety t0 (n = 180) | 4.5 | 2.2 | 9.8 | 1.3 | 15.0 | 1.6 | <0.001 |
| HADS anxiety t2 (n = 133) ** | 3.9 | 3.5 | 8.5 | 3.4 | 11.0 | 2.9 | <0.001 |
| HADS depression t0 | 5.5 | 3.0 | 8.1 | 3.3 | 11.7 | 3.5 | <0.001 |
| N | % | N | % | N | % | Chi square p | |
| Neg. affectivity posi-tive; DS 14 (n = 178) | 25 | 53.2 | 75 | 86.2 | 39 | 88.6 | <0.001 |
| Social inhibition posi-tive; DS 14 (n = 178) | 17 | 36.2 | 60 | 69.0 | 35 | 79.5 | <0.001 |
| Anxiety disorder (DSM IV) interview ***; n = 123) | 0.018 | ||||||
| yes | 0 | 20 | 29.6 | 21 | 52.2 | ||
| no | 12 | 100 | 50 | 70.4 | 19 | 47.8 | |
| Panic disturbance Agora phobia-(n = 123) | |||||||
| yes | 0 | 11 | 15.5 | 16 | 40.0 | ||
| no | 12 | 100 | 60 | 84.5 | 24 | 60.0 | |
| Phobia (n = 123) | |||||||
| yes | 0 | 2 | 1.6 | 1 | 2.5 | ||
| no | 12 | 100 | 69 | 98.4 | 39 | 97.5 | |
| Generalized Anxiety disorder (n = 123) | |||||||
| yes | 0 | 8 | 6.5 | 2 | 7.5 | ||
| no | 12 | 100 | 63 | 93.5 | 38 | 92.5 | |
| HADS Anxiety | ||||
|---|---|---|---|---|
| No Anxiety HADS-A: 0–7 | Moderate Anxiety HADS-A: 8–12 | High Anxiety HADS-A: 13–22 | ||
| alive | N | 19 | 60 | 37 |
| % within anxiety group | 41.3% | 69.8% | 86.0% | |
| dead | N | 27 | 26 | 6 |
| % within anxiety group | 58.7% | 30.2% | 14.0% | |
| Total | N | 46 | 86 | 43 |
| % within anxiety group | 100.0% | 100.0% | 100.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deter, H.-C.; Albert, W.; Weber, C.; Merswolken, M.; Orth-Gomér, K.; Herrmann-Lingen, C.; Grün, A.-S. Does Anxiety Affect Survival in Patients with Coronary Heart Disease? J. Clin. Med. 2023, 12, 2098. https://doi.org/10.3390/jcm12062098
Deter H-C, Albert W, Weber C, Merswolken M, Orth-Gomér K, Herrmann-Lingen C, Grün A-S. Does Anxiety Affect Survival in Patients with Coronary Heart Disease? Journal of Clinical Medicine. 2023; 12(6):2098. https://doi.org/10.3390/jcm12062098
Chicago/Turabian StyleDeter, Hans-Christian, Wolfgang Albert, Cora Weber, Melanie Merswolken, Kristina Orth-Gomér, Christoph Herrmann-Lingen, and Anna-Sophia Grün. 2023. "Does Anxiety Affect Survival in Patients with Coronary Heart Disease?" Journal of Clinical Medicine 12, no. 6: 2098. https://doi.org/10.3390/jcm12062098