

Impact of Acrylic and Silicone-Based Soft-Liner Materials on Biting Force and Quality of Life of the Complete Denture Wearers: A Randomized Clinical Trial

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.5. Randomization
2.5.1. Sequence Generation
2.5.2. Allocation, Concealment Mechanism, and Implementation
2.6. Blinding
2.7. Statistical Methods
3. Results
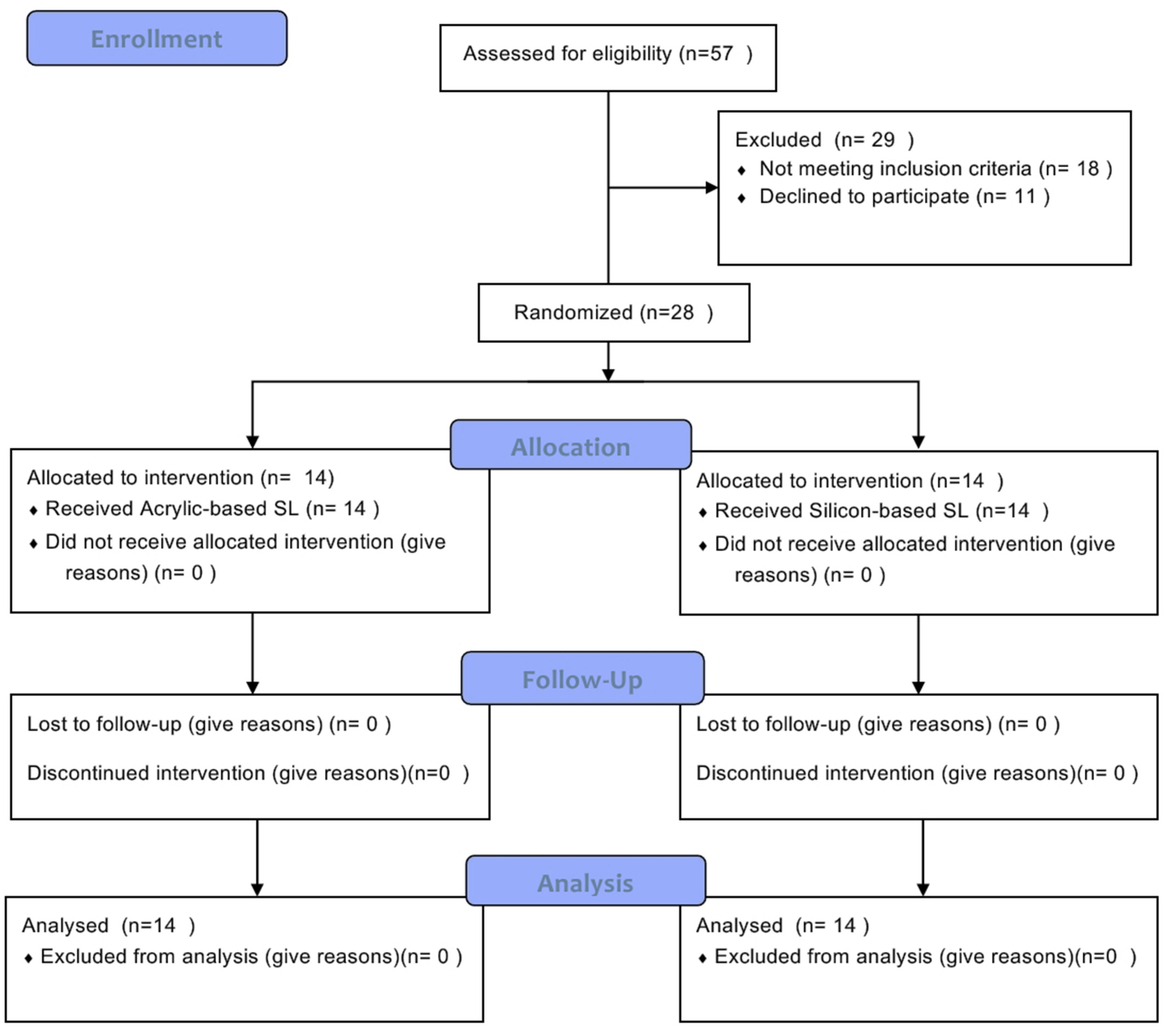
3.1. Participant Flow
3.2. Recruitment
3.3. Baseline Data
3.4. Numbers Analyzed
3.5. Outcomes and Estimation
3.5.1. The Oral Health-Related Quality of Life (OHRQoL)
3.5.2. The Pain Perception
3.5.3. Maximum Biting Force
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Douglass, C.W.; Watson, A.J. Future needs for fixed and removable partial dentures in the United States. J. Prosthet. Dent. 2002, 87, 9–14. [Google Scholar] [CrossRef]
- McCord, J.F.; Tyson, K.W. A conservative prosthodontic option for the treatment of edentulous patients with atrophic (flat) mandibular ridges. Br. Dent. J. 1997, 182, 469–472. [Google Scholar] [CrossRef]
- Zarb, G.A.; Schmitt, A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto Study. Part II: The prosthetic results. J. Prosthet. Dent. 1990, 64, 53–61. [Google Scholar] [CrossRef]
- Cardoso, R.G.; De Melo, L.A.; Barbosa, G.A.S.; Calderon, P.D.S.; Germano, A.R.; Junior, W.M.; Carreiro, A. Impact of mandibular conventional denture and overdenture on quality of life and masticatory efficiency. Braz. Oral Res. 2016, 30, e102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayakawa, I.; Hirano, S.; Takahashi, Y.; Keh, E.S. Changes in the masticatory function of complete denture wearers after relining the mandibular denture with a soft denture liner. Int. J. Prosthodont. 2001, 13, 227–231. [Google Scholar]
- Feine, J.S.; E Carlsson, G.; A Awad, M.; Chehade, A.; Duncan, W.J.; Gizani, S.; Head, T.; Heydecke, G.; Lund, J.P.; MacEntee, M.; et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology 2002, 19, 3–4. [Google Scholar]
- Helmy, M.-D.; Alqutaibi, A.; El-Ella, A.; Shawky, A. Effect of implant loading protocols on failure and marginal bone loss with unsplinted two-implant-supported mandibular overdentures: Systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Alqutaibi, A.Y.; Esposito, M.; Algabri, R.; Alfahad, A.; Kaddah, A.; Farouk, M.; Alsourori, A.A.A. Single vs. two implant-retained overdentures for edentulous mandibles: A systematic review. Eur. J. Oral Implant. 2017, 10, 243–261. [Google Scholar]
- Alqutaibi, A.; Kaddah, A.; Farouk, M. Randomized study on the effect of single-implant versus two-implant retained overdentures on implant loss and muscle activity: A 12-month follow-up report. Int. J. Oral Maxillofac. Surg. 2017, 46, 789–797. [Google Scholar] [CrossRef]
- Shim, J.S.; Watts, D.C. An examination of the stress distribution in a soft-lined acrylic resin mandibular complete denture by finite element analysis. Int. J. Prosthodont. 2000, 13, 19–24. [Google Scholar]
- Murata, H.; Haberham, R.C.; Hamada, T.; Taguchi, N. Setting and stress relaxation behavior of resilient denture liners. J. Prosthet. Dent. 1998, 80, 714–722. [Google Scholar] [CrossRef]
- Murata, H.; Taguchi, N.; Hamada, T.; Kawamura, M.; McCabe, J.F. Dynamic viscoelasticity of soft liners and masticatory function. J. Dent. Res. 2002, 81, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Williamson, R.T. Clinical application of a soft denture liner: A case report. Quintessence Int. 1995, 26, 413–418. [Google Scholar] [PubMed]
- Chaves, C.D.A.L.; Machado, A.L.; Carlos, I.Z.; Giampaolo, E.T.; Pavarina, A.C.; Vergani, C.E. Cytotoxicity of monomers, plasticizer and degradation by-products released from dental hard chairside reline resins. Dent. Mater. 2010, 26, 1017–1023. [Google Scholar] [CrossRef]
- Urban, V.M.; Machado, A.L.; Vergani, C.E.; Giampaolo, E.T.; Pavarina, A.C.; de Almeida, F.G.; Cass, Q.B. Effect of water-bath post-polymerization on the mechanical properties, degree of conversion, and leaching of residual compounds of hard chairside reline resins. Dent. Mater. 2009, 25, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Kou, Z.; Yi, Q.; Zhi, X.; Society of Dental Materials; Chinese Stomatological Association. Summary of the seventh national conference on the science of dental materials. Zhonghua Kou Qiang Yi Xue Za Zhi 2012, 47, 567–568. [Google Scholar]
- Mese, A.; Guzel, K.G. Effect of storage duration on the hardness and tensile bond strength of silicone- and acrylic resin-based resilient denture liners to a processed denture base acrylic resin. J. Prosthet. Dent. 2008, 99, 153–159. [Google Scholar] [CrossRef]
- Atsu, S.; Keskin, Y. Effect of silica coating and silane surface treatment on the bond strength of soft denture liner to denture base material. J. Appl. Oral Sci. 2013, 21, 300–306. [Google Scholar] [CrossRef]
- Liao, W.-C.; Pearson, G.J.; Braden, M.; Wright, P.S. The interaction of various liquids with long-term denture soft lining materials. Dent. Mater. 2012, 28, e199–e206. [Google Scholar] [CrossRef]
- Bail, M.; Jorge, J.H.; Urban, V.M.; Campanha, N.H. Surface Roughness of Acrylic and Silicone-Based Soft Liners: In Vivo Study in a Rat Model. J. Prosthodont. 2013, 23, 146–151. [Google Scholar] [CrossRef]
- Nowakowska-Toporowska, A.; Raszewski, Z.; Wieckiewicz, W. Color change of soft silicone relining materials after storage in artificial saliva. J. Prosthet. Dent. 2015, 115, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Valentini, F.; Luz, M.S.; Boscato, N.; Pereira-Cenci, T. Biofilm formation on denture liners in a randomised controlled in situ trial. J. Dent. 2013, 41, 420–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santawisuk, W.; Kanchanavasita, W.; Sirisinha, C.; Harnirattisai, C. Mechanical properties of experimental silicone soft lining materials. Dent. Mater. J. 2013, 32, 970–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, J.F.; Smith, D.C. Evaluation of Indirect Resilient Liners for Dentures: Laboratory and Clinical Tests. J. Am. Dent. Assoc. 1965, 70, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Goll, G.; Smith, D.E.; Plein, J.B. The effect of denture cleansers on temporary soft liners. J. Prosthet. Dent. 1983, 50, 466–472. [Google Scholar] [CrossRef]
- Nikawa, H.; Iwanaga, H.; Hamada, T.; Yuhta, S. Effects of denture cleansers on direct soft denture lining materials. J. Prosthet. Dent. 1994, 72, 657–662. [Google Scholar] [CrossRef]
- Sinobad, D.; Murphy, W.; Huggett, R.; Brooks, S. Bond strength and rupture properties of some soft denture liners. J. Oral Rehabil. 1992, 19, 151–160. [Google Scholar] [CrossRef]
- Aydın, A.; Terzioğlu, H.; Akınay, A.; Ulubayram, K.; Hasırcı, N. Bond strength and failure analysis of lining materials to denture resin. Dent. Mater. 1999, 15, 211–218. [Google Scholar] [CrossRef]
- Eick, J.D.; Craig, R.G.; Peyton, F.A. Properties of resilient denture liners in simulated mouth conditions. J. Prosthet. Dent. 1962, 12, 1043–1052. [Google Scholar] [CrossRef]
- Hayakawa, I.; Hirano, S.; Kobayashi, S.; Nagao, M.; Masuhara, E. The creep behavior of denture-supporting tissues and soft lining materials. Int. J. Prosthodont. 1994, 7, 339–347. [Google Scholar]
- Mangtani, N.; Pillai, R.S.; Babu, D.; Jain, V. Effect of resilient liner on masticatory efficiency and general patient satisfaction in completely edentulous patients. J. Dent. Spec. 2015, 3, 150–155. [Google Scholar] [CrossRef]
- Kimoto, S.; Yamamoto, S.; Shinomiya, M.; Kawai, Y. Randomized controlled trial to investigate how acrylic-based resilient liner affects on masticatory ability of complete denture wearers. J. Oral Rehabil. 2010, 37, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Kalachandra, S.; Minton, R.; Taylor, D.; Takamata, T. Characterization of some proprietary soft lining materials. J. Mater. Sci. Mater. Med. 1995, 6, 647–652. [Google Scholar] [CrossRef]
- Kazanji, M.N.; Watkinson, A.C. Soft lining materials: Their absorption of, and solubility in, artificial saliva. Br. Dent. J. 1988, 165, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Murata, H.; Hamada, T.; Sadamori, S. Relationship between viscoelastic properties of soft denture liners and clinical efficacy. Jpn. Dent. Sci. Rev. 2008, 44, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Elawady, A.F.; Eissa, S.M.; Esmat, A.M. Effect of soft liner on clinical implication of tooth supported overdenture. J. Arab. Soc. Med. Res. 2021, 16, 1. [Google Scholar]
- Fayad, M.I. Oral health impact profile in edentulous patients rehabilitated with conventional and flexible complete denture. Egypt Dent. J. 2016, 62, 1–8. [Google Scholar]
- Sakr, H.; Fayad, M. Bite force and oral health impact profile in completely edentulous patients rehabilitated with two different types of denture bases. Tanta Dent. J. 2017, 14, 173–180. [Google Scholar]
- Pisani, M.X.; Malheiros-Segundo, A.d.L.; Balbino, K.L.; Souza, R.d.F.; Paranhos, H.d.F.O.; Lovato da Silva, C.H. Oral health related quality of life of edentulous patients after denture relining with a silicone-based soft liner. Gerodontology 2012, 29, 474–480. [Google Scholar] [CrossRef]
- Sutton, A.F.; Glenny, A.M.; McCord, J.F. Interventions for Replacing Missing Teeth: Denture Chewing Surface Designs in Edentulous People; The Cochrane Library: London, UK, 2005. [Google Scholar]
- Bural, C.; Geckili, O.; Erdogan, O.; Bektas-Kayhan, K.; Dayan, S.C. Reliability and validity of the Turkish version of oral health impact profile for edentulous subjects. Eur. Oral Res. 2021, 55, 67–73. [Google Scholar] [CrossRef]
- Larsson, P.; List, T.; Lundström, I.; Marcusson, A.; Ohrbach, R. Reliability and validity of a Swedish version of the Oral Health Impact Profile (OHIP-S). Acta Odontol. Scand. 2004, 62, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; He, F.-M. Reliability and validity of the Chinese version of the 5-item oral health impact profile]. Hua Xi Kou Qiang Yi Xue Za Zhi 2020, 38, 145–148. [Google Scholar] [PubMed]
- Motallebnejad, M.; Hadian, H.; Mehdizadeh, S.; Hajiahmadi, M. Validity and reliability of the Persian version of the oral health impact profile (OHIP)-14. Caspian J. Intern. Med. 2011, 2, 314–320. [Google Scholar]
- Sato, Y.; Kaiba, Y.; Yamaga, E.; Minakuchi, S. Reliability and validity of a Japanese version of the Oral Health Impact Profile for edentulous subjects. Gerodontology 2011, 29, e1033–e1037. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, B.; Niraula, S.R.; Parajuli, P.K.; Suwal, P.; Singh, R.K. Reliability and Validity of a Nepalese Version of the Oral Health Impact Profile for Edentulous Subjects. J Prosthodont. 2018, 27, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Kimoto, S.; Kimoto, K.; Gunji, A.; Kawai, Y.; Murakami, H.; Tanaka, K.; Syu, K.; Aoki, H.; Toyoda, M.; Kobayashi, K. Clinical effects of acrylic resilient denture liners applied to mandibular complete dentures on the alveolar ridge. J. Oral Rehabil. 2007, 34, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.; Bates, J.; Basker, R.; Gutteridge, D.; Harrison, A. A survey of the dissatisfied denture patient. Eur. J. Prosthodont. Restor. Dent. 1993, 2, 73–78. [Google Scholar]
- Kimoto, S.; Furuse, N.; Ogawa, T.; Nakashima, Y.; Furokawa, S.; Okubo, M.; Yamaguchi, H.; Kawai, Y. Receptivity of the mandible versus the maxilla to external stimuli in patients with complete dentures. J. Prosthodont. Res. 2019, 63, 299–302. [Google Scholar] [CrossRef]
- Shinogaya, T.; Sodeyama, A.; Matsumoto, M. Bite force and occlusal load distribution in normal complete dentitions of young adults. Eur. J. Prosthodont. Restor. Dent. 1999, 7, 65–70. [Google Scholar]
- Tortopidis, D.; Lyons, M.F.; Baxendale, R.H.; Gilmour, W.H. The variability of bite force measurement between sessions, in different positions within the dental arch. J. Oral Rehabil. 1998, 25, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Fontijn-Tekamp, F.A.; Slagter, A.P.; Van Der Bilt, A.; Van’T Hof, M.A.; Witter, D.J.; Kalk, W.J.J.A.; Jansen, J.A. Biting and chewing in overdentures, full dentures, and natural dentitions. J. Dent. Res. 2000, 79, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- Furokawa, S.; Kimoto, S.; Furuse, N.; Furuya, Y.; Ogawa, T.; Nakashima, Y.; Okubo, M.; Yamaguchi, H.; Kawai, Y. The effects of silicone-based resilient denture liners on pain: A randomized controlled trial. J. Prosthodont. Res. 2020, 64, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Kimoto, S.; So, K.; Yamamoto, S.; Ohno, Y.; Shinomiya, M.; Ogura, K.; Kobayashi, K. Randomized controlled clinical trial for verifying the effect of silicone-based resilient denture liner on the masticatory function of complete denture wearers. Int. J. Prosthodont. 2006, 19, 593–600. [Google Scholar] [PubMed]


{kind=link}
| Variable | Acrylic-Based SL Group (n = 14) | Silicone-Based SL Group (n = 14) |
|---|---|---|
| Age (years), mean ± SD | 60.1 ± 12.4 | 58.7 ± 13.1 |
| Edentulous period (mandible) (years), mean ± SD | 5.9 ± 2.3 | 6.4 ± 1.8 |
| Height of alveolar ridge (mm), mean ± SD | 16.9 ± 4.2 | 17.6 ± 3.3 |
| Mucosal thickness (mm), mean ± SD | 1.9 ± 0.7 | 2.2 ± 0.2 |
| Mucosal resiliency (firm, resilient, flappy) | (10, 4, 0) | (9, 5, 0) |
| Denture difficulty classification (I, II, III, IV) | (6, 7, 1, 0) | (7, 6, 1, 0) |
| Interventions | Baseline | One Month | Three Months |
|---|---|---|---|
| Acrylic-Based SL | 56.3 ± 8.2 Aa | 34.6 ± 7.8 Bb | 29.4 ± 5.9 Bb |
| Silicone-Based SL | 53.1 ± 12.8 Aa | 31.9 ± 7.4 Bb | 25.8 ± 6.2 Bb |
| MD (CI) | −3.2 (−11.5 to 5.1) | −2.7 (−8.6 to 3.2) | −3.6 (−8.3 to 1.1) |
| Interventions | Baseline (Before Relining) | At the Time of the Initial Adjustment |
|---|---|---|
| Acrylic-Based SL | 63.5 ± 29.8 Aa | 47.1 ± 34.9 Bb |
| Silicone-Based SL | 61.1 ± 31.1 Aa | 45.9 ± 36.1 Bb |
| MD (CI) | −2.4 (−26.1 to 21.2) | −1.2 (−28.8 to 26.3) |
| Interventions | Baseline | One Month | Three Months |
| Acrylic-Based SL | 75 ± 31 Aa | 145 ± 53 Bb | 116 ± 47 Bc |
| Silicone-Based SL | 83 ± 32 Aa | 156 ± 49 Bb | 166 ± 57 Cb |
| MD (CI) | 8 (−16.4 to 32.4) | 11 (−28.6 to 50.6) | 50 (9.4 to 60.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqutaibi, A.Y.; Alnazzawi, A.A.; Farghal, A.E.; Bakr, R.M.; Mahmoud, I.I. Impact of Acrylic and Silicone-Based Soft-Liner Materials on Biting Force and Quality of Life of the Complete Denture Wearers: A Randomized Clinical Trial. J. Clin. Med. 2023, 12, 2073. https://doi.org/10.3390/jcm12052073
Alqutaibi AY, Alnazzawi AA, Farghal AE, Bakr RM, Mahmoud II. Impact of Acrylic and Silicone-Based Soft-Liner Materials on Biting Force and Quality of Life of the Complete Denture Wearers: A Randomized Clinical Trial. Journal of Clinical Medicine. 2023; 12(5):2073. https://doi.org/10.3390/jcm12052073
Chicago/Turabian StyleAlqutaibi, Ahmed Yaseen, Ahmad A. Alnazzawi, Ahmed E. Farghal, Ramy M. Bakr, and Ihab Ismail Mahmoud. 2023. "Impact of Acrylic and Silicone-Based Soft-Liner Materials on Biting Force and Quality of Life of the Complete Denture Wearers: A Randomized Clinical Trial" Journal of Clinical Medicine 12, no. 5: 2073. https://doi.org/10.3390/jcm12052073