
Ultrasound Guided Parasternal Block for Perioperative Analgesia in Cardiac Surgery: A Prospective Study
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
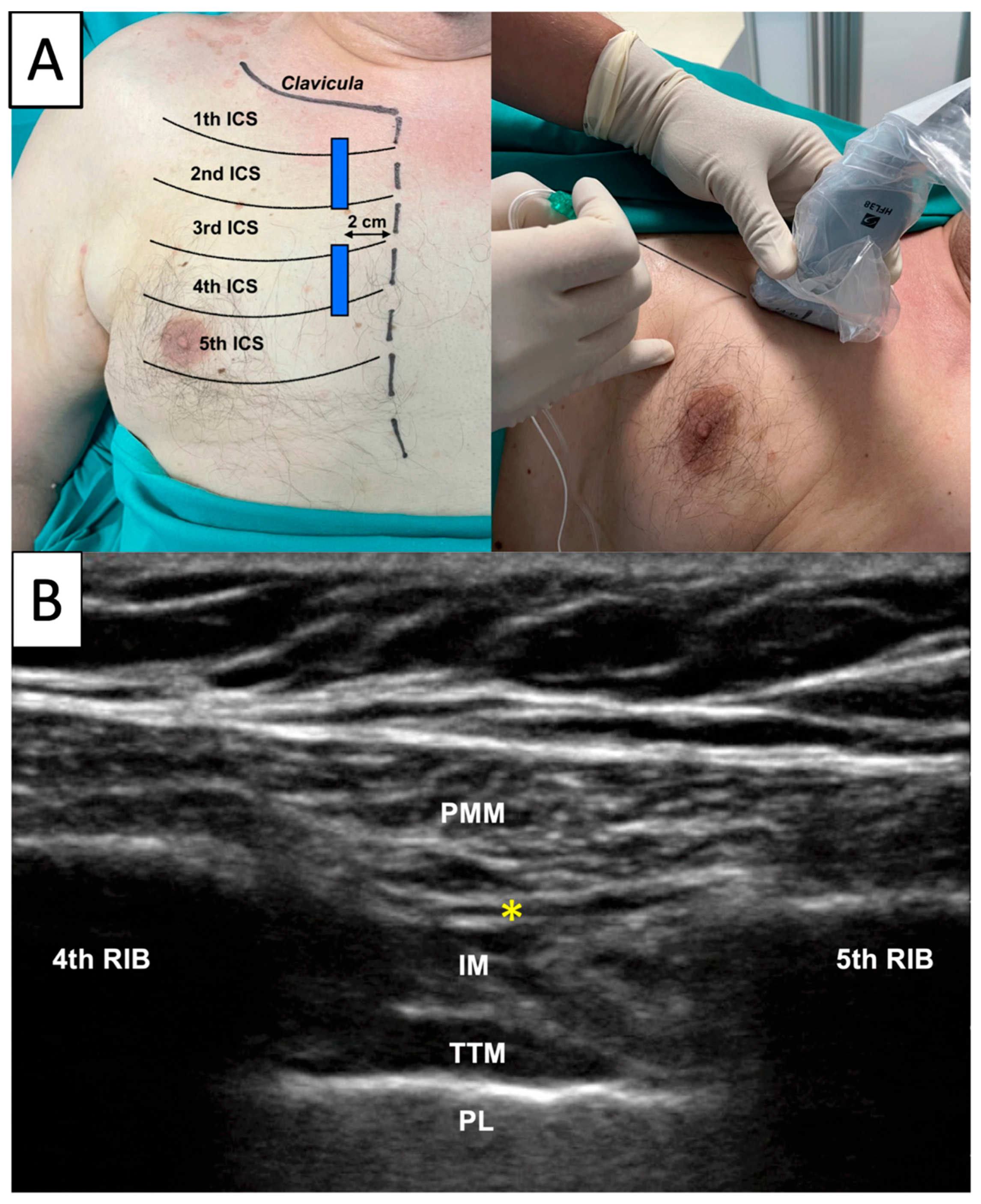
- The “Parasternal” group received ultrasound guided bilateral parasternal block after general anaesthesia induction and an infiltration with local anaesthetic of the surgical drainage sites at the end of surgery.
- The “Control” group received just the infiltration with local anaesthetic of the surgical drainage sites at the end of surgery.
2.1. Block Execution
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, P.F.; Kehlet, H.; Neal, J.M.; Schricker, T.; Carr, D.B.; Carli, F. The role of the anesthesiologist in fast-track surgery: From multimodal analgesia to perioperative medical care. Anesth. Analg. 2007, 104, 1380–1396. [Google Scholar] [CrossRef]
- Zubrzycki, M.; Liebold, A.; Skrabal, C.; Reinelt, H.; Ziegler, M.; Perdas, E.; Zubrzycka, M. Assessment and pathophysiology of pain in cardiac surgery. J. Pain. Res. 2018, 11, 1599–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Emelife, P.I.; Prabhakar, A.; Moll, V.; Kendrick, J.B.; Parr, A.T.; Hyatali, F.; Pankaj, T.; Li, J.; Cornett, E.M.; et al. Regional anesthesia considerations for cardiac surgery. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 387–406. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Strumia, A.; Remore, L.M.; Pascarella, G.; Del Buono, R.; Tedesco, M.; Sepolvere, G.; Scimia, P.; Fusco, P. Breast surgery analgesia: Another perspective for PROSPECT guidelines. Anaesthesia 2020, 75, 1404–1405. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Strumia, A.; Pascarella, G.; Tomaselli, E.; Palminteri, M.; Antinolfi, V.; Montelione, N.; Stilo, F.; Spinelli, F.; Agrò, F.E. PECS II Block Combined with Supraclavicular Brachial Plexus Block Allows Anesthesia for Transaxillary Thoracic Outlet Syndrome Decompression Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 2234–2236. [Google Scholar] [CrossRef]
- Grasso, A.; Orsaria, P.; Costa, F.; D’Avino, V.; Caredda, E.; Hazboun, A.; Carino, R.; Pascarella, G.; Altomare, M.; Buonomo, O.C.; et al. Ultrasound-guided Interfascial Plane Blocks for Non-anesthesiologists in Breast Cancer Surgery: Functional Outcomes and Benefits. Anticancer Res. 2020, 40, 2231–2238. [Google Scholar] [CrossRef]
- Kar, P.; Ramachandran, G. Pain relief following sternotomy in conventional cardiac surgery: A review of non neuraxial regional nerve blocks. Ann. Card. Anaesth. 2020, 23, 200–208. [Google Scholar] [CrossRef]
- McDonald, S.B.; Jacobsohn, E.; Kopacz, D.J.; Desphande, S.; Helman, J.D.; Salinas, F.; Hall, R.A. Parasternal block and local anesthetic infiltration with levobupivacaine after cardiac surgery with desflurane: The effect on postoperative pain, pulmonary function, and tracheal extubation times. Anesth. Analg. 2005, 100, 25–32. [Google Scholar] [CrossRef]
- Barr, A.M.; Tutungi, E.; Almeida, A.A. Parasternal intercostal block with ropivacaine for pain management after cardiac surgery: A double-blind, randomized, controlled trial. J. Cardiothorac. Vasc. Anesth. 2007, 21, 547–553. [Google Scholar] [CrossRef]
- Lee, C.Y.; Robinson, D.A.; Johnson, C.A., Jr.; Zhang, Y.; Wong, J.; Joshi, D.J.; Wu, T.T.; Knight, P.A. A Randomized Controlled Trial of Liposomal Bupivacaine Parasternal Intercostal Block for Sternotomy. Ann. Thorac. Surg. 2019, 107, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doğan Bakı, E.; Kavrut Ozturk, N.; Ayoğlu, R.U.; Emmiler, M.; Karslı, B.; Uzel, H. Effects of Parasternal Block on Acute and Chronic Pain in Patients Undergoing Coronary Artery Surgery. Semin. Cardiothorac. Vasc. Anesth. 2016, 20, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, N.K.; Baki, E.D.; Kavakli, A.S.; Sahin, A.S.; Ayoglu, R.U.; Karaveli, A.; Emmiler, M.; Inanoglu, K.; Karsli, B. Comparison of Transcutaneous Electrical Nerve Stimulation and Parasternal Block for Postoperative Pain Management after Cardiac Surgery. Pain. Res. Manag. 2016, 2016, 4261949. [Google Scholar] [CrossRef] [Green Version]
- Schiavoni, L.; Nenna, A.; Cardetta, F.; Pascarella, G.; Costa, F.; Chello, M.; Agrò, F.E.; Mattei, A. Parasternal Intercostal Nerve Blocks in Patients Undergoing Cardiac Surgery: Evidence Update and Technical Considerations. J. Cardiothorac. Vasc. Anesth. 2022, 36, 4173–4182. [Google Scholar] [CrossRef] [PubMed]
- Fusco, P.; Petrucci, E.; Marinangeli, F.; Scimia, P. Block failure or lack of efficacy? The "Double V" sign: A novel sonographic sign for a successful interfascial plane block. Minerva Anestesiol. 2019, 85, 917–918. [Google Scholar] [CrossRef]
- Padala, S.; Badhe, A.S.; Parida, S.; Jha, A.K. Comparison of preincisional and postincisional parasternal intercostal block on postoperative pain in cardiac surgery. J. Card. Surg. 2020, 35, 1525–1530. [Google Scholar] [CrossRef]
- Kehlet, H.; Dahl, J.B. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet 2003, 362, 1921–1928. [Google Scholar] [CrossRef]
- Blanco, R. The ‘pecs block’: A novel technique for providing analgesia after breast surgery. Anaesthesia 2011, 66, 847–848. [Google Scholar] [CrossRef]
- Yalamuri, S.; Klinger, R.Y.; Bullock, W.M.; Glower, D.D.; Bottiger, B.A.; Gadsden, J.C. Pectoral Fascial (PECS) I and II Blocks as Rescue Analgesia in a Patient Undergoing Minimally Invasive Cardiac Surgery. Reg. Anesth. Pain Med. 2017, 42, 764–766. [Google Scholar] [CrossRef]
- Khalil, A.E.; Abdallah, N.M.; Bashandy, G.M.; Kaddah, T.A. Ultrasound-Guided Serratus Anterior Plane Block Versus Thoracic Epidural Analgesia for Thoracotomy Pain. J. Cardiothorac. Vasc. Anesth. 2017, 31, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Fujii, S.; Roche, M.; Jones, P.M.; Vissa, D.; Bainbridge, D.; Zhou, J.R. Transversus thoracis muscle plane block in cardiac surgery: A pilot feasibility study. Reg. Anesth. Pain Med. 2019, 44, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.N.; Chauhan, S.; Bhoi, D.; Kaushal, B.; Hasija, S.; Sangdup, T.; Bisoi, A.K. Bilateral Erector Spinae Plane Block for Acute Post-Surgical Pain in Adult Cardiac Surgical Patients: A Randomized Controlled Trial. J. Cardiothorac. Vasc. Anesth. 2019, 33, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Kelava, M.; Alfirevic, A.; Bustamante, S.; Hargrave, J.; Marciniak, D. Regional Anesthesia in Cardiac Surgery: An Overview of Fascial Plane Chest Wall Blocks. Anesth. Analg. 2020, 131, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Sepolvere, G.; Fusco, P.; Tedesco, M.; Scimia, P. Bilateral ultrasound-guided parasternal block for postoperative analgesia in cardiac surgery: Could it be the safest strategy? Reg. Anesth. Pain Med. 2020, 45, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Sepolvere, G.; Tedesco, M.; Cristiano, L. Ultrasound Parasternal Block as a Novel Approach for Cardiac Sternal Surgery: Could it Be the Safest Strategy? J. Cardiothorac. Vasc. Anesth. 2020, 34, 2284–2286. [Google Scholar] [CrossRef]
- Eldeen, H.M.S. Ultrasound guided pectoral nerve blockade versus thoracic spinal blockade for conservative breast surgery in cancer breast: A randomized controlled trial. Egypt. J. Anaesth. 2016, 32, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Kulhari, S.; Bharti, N.; Bala, I.; Arora, S.; Singh, G. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: A randomized controlled trial. Br. J. Anaesth. 2016, 117, 382–386. [Google Scholar] [CrossRef] [Green Version]
- Bloc, S.; Perot, B.P.; Gibert, H.; Law Koune, J.D.; Burg, Y.; Leclerc, D.; Vuitton, A.S.; De La Jonquière, C.; Luka, M.; Waldmann, T.; et al. Efficacy of parasternal block to decrease intraoperative opioid use in coronary artery bypass surgery via sternotomy: A randomized controlled trial. Reg. Anesth. Pain Med. 2021, 46, 671–678. [Google Scholar] [CrossRef]
- Wick, E.C.; Grant, M.C.; Wu, C.L. Postoperative Multimodal Analgesia Pain Management With Nonopioid Analgesics and Techniques: A Review. JAMA Surg. 2017, 152, 691–697. [Google Scholar] [CrossRef]
- Plowman, E.K.; Anderson, A.; York, J.D.; DiBiase, L.; Vasilopoulos, T.; Arnaoutakis, G.; Beaver, T.; Martin, T.; Jeng, E.I. Dysphagia after cardiac surgery: Prevalence, risk factors, and associated outcomes. J. Thorac. Cardiovasc. Surg. 2021, 165, 737.e3–746.e3. [Google Scholar] [CrossRef]
- Fabio, C.; Giuseppe, P.; Chiara, P.; Antongiulio, V.; Enrico, D.; Filippo, R.; Federica, B.; Eugenio, F.A. Sufentanil sublingual tablet system (Zalviso®) as an effective analgesic option after thoracic surgery: An observational study. Saudi J. Anaesth. 2019, 13, 222–226. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parasternal (63) | Control (63) | p-Value | |
|---|---|---|---|
| Age (years) | 67 ± 10 | 69.6 ± 10 | 0.17 |
| Sex (M/F) | 33/30 | 35/28 | 0.8 |
| BMI (kg/m2) | 26.7 ± 4 | 26.5 ± 3.3 | 0.9 |
| Chronic opiates medication | 2 (3%) | 3 (5%) | >0.9 |
| Diabetes Mellitus | 13 (21%) | 12(19%) | >0.9 |
| Pre-existing pulmonary disorders | 11 (17%) | 10 (16%) | 0.88 |
| Type of surgery | |||
| CABG | 36 (57%) | 41 (65%) | 0.6 |
| CABG off pump | 3 (5%) | 4 (6%) | |
| Valvular surgery | 19 (30%) | 16 (25%) | |
| CABG + valvular surgery | 4 (6%) | 1 (2%) | |
| Thoracic aorta aneurysm | 1 (2%) | 1 (2%) | |
| Surgery duration (min) | 230.7 ± 53.5 | 213 ± 40.8 | 0.08 |
| Parasternal | Control | p-Value | |
|---|---|---|---|
| Intraoperative fentanyl (γ) | 406.3 ± 81.6 | 864.3 ± 154.4 | <0.001 |
| Intraoperative remifentanil (γ) | 336.1 ± 13.1 | 338.3 ± 13.5 | 0.3367 |
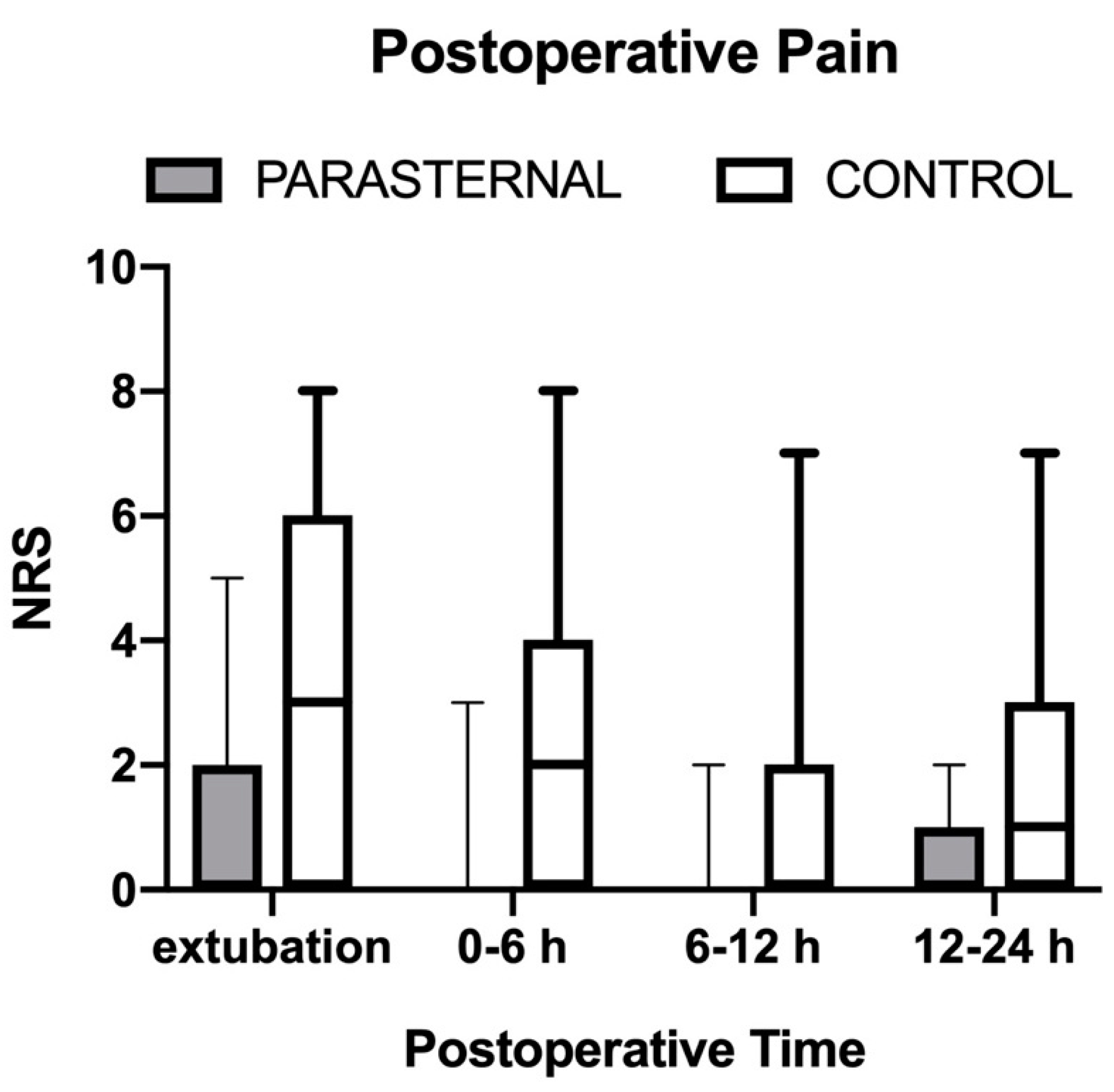
| Postoperative pain (NRS max 0–10) | |||
| Extubation | 2 (0–4.5) | 3 (0–6) | 0.07 |
| 0–6 h | 0 (0–3) | 2 (0–4) | 0.46 |
| 6–12 h | 0 (0–2) | 0 (0–2) | 0.57 |
| 12–24 h | 1 (0–2) | 2 (0–3) | 0.69 |
| Postoperative opiates consumption | |||
| Yes | 19 (30%) | 18 (29%) | 0.8 |
| No | 44 (70%) | 45 (71%) | |
| Time to first opioid (min) | 30 (10–45) | 30 (11–60) | 0.6 |
| Morphine consumption 0–24 h (mg) | 0 (0–2) | 0 (0–2) | >0.9 |
| Parasternal | Control | p-Value | |
|---|---|---|---|
| Time to extubation (min) | 191 ± 48 | 305 ± 62 | <0.001 |
| Pulmonary performance (balls moved up) | |||
| Basal | 3 (2–3) | 3 (2–3) | 0.9 |
| After extubation | 2 (1–2) | 1 (1–2) | 0.045 |
| Side effects | |||
| Nausea | 2 (3%) | 1 (2%) | – |
| Vomit | 1 (2%) | 2 (3%) | – |
| Delirium | 1 (2%) | 2 (3%) | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascarella, G.; Costa, F.; Nonnis, G.; Strumia, A.; Sarubbi, D.; Schiavoni, L.; Di Pumpo, A.; Mortini, L.; Grande, S.; Attanasio, A.; et al. Ultrasound Guided Parasternal Block for Perioperative Analgesia in Cardiac Surgery: A Prospective Study. J. Clin. Med. 2023, 12, 2060. https://doi.org/10.3390/jcm12052060
Pascarella G, Costa F, Nonnis G, Strumia A, Sarubbi D, Schiavoni L, Di Pumpo A, Mortini L, Grande S, Attanasio A, et al. Ultrasound Guided Parasternal Block for Perioperative Analgesia in Cardiac Surgery: A Prospective Study. Journal of Clinical Medicine. 2023; 12(5):2060. https://doi.org/10.3390/jcm12052060
Chicago/Turabian StylePascarella, Giuseppe, Fabio Costa, Giulia Nonnis, Alessandro Strumia, Domenico Sarubbi, Lorenzo Schiavoni, Annalaura Di Pumpo, Lara Mortini, Stefania Grande, Andrea Attanasio, and et al. 2023. "Ultrasound Guided Parasternal Block for Perioperative Analgesia in Cardiac Surgery: A Prospective Study" Journal of Clinical Medicine 12, no. 5: 2060. https://doi.org/10.3390/jcm12052060