
Spiradenocarcinoma: SEER Study of Epidemiology, Survival, and Treatment Options
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Variable Selection
2.3. Statistical Analysis
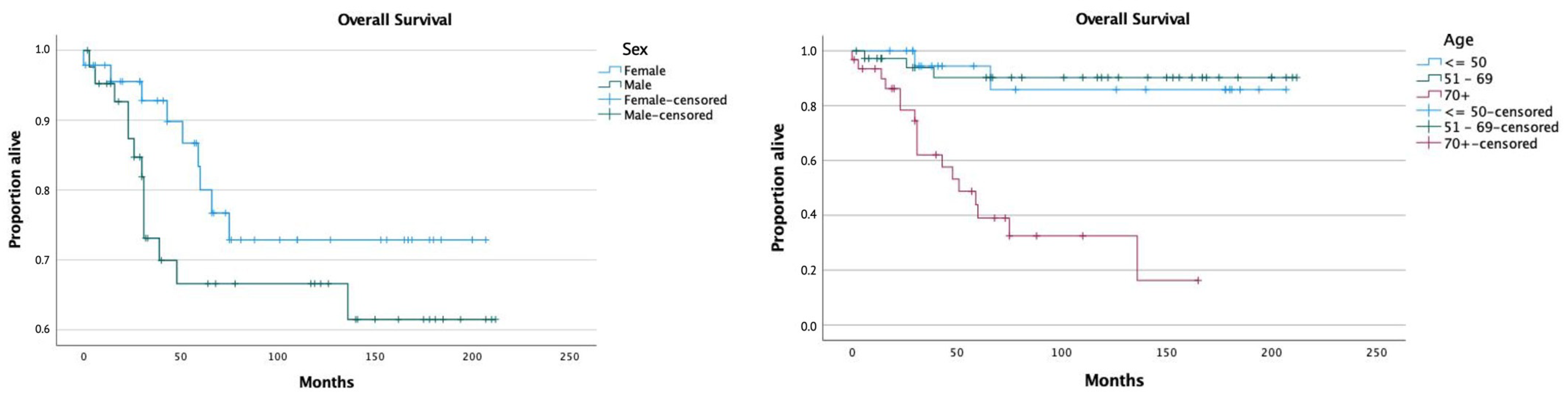
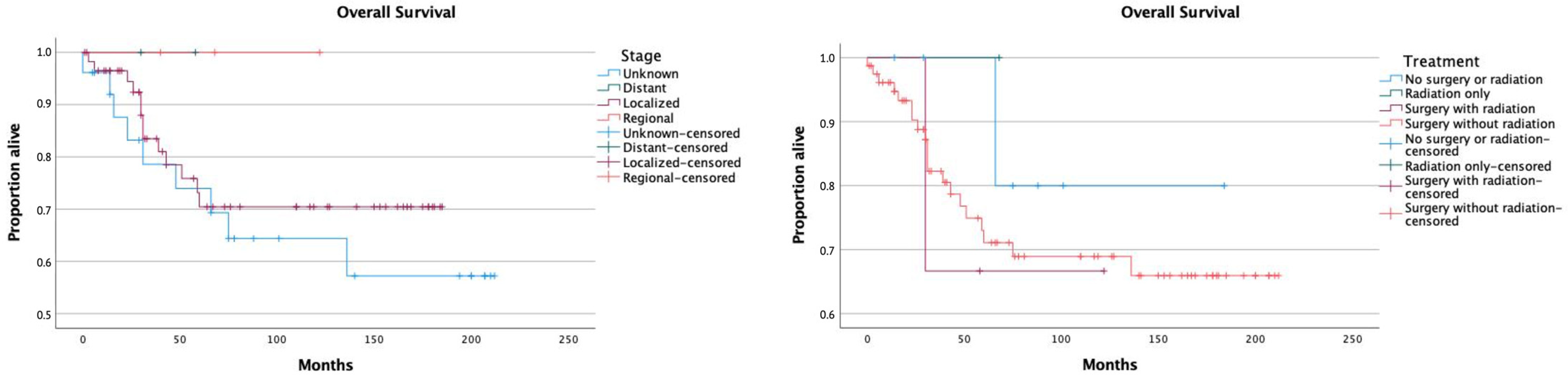
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ribeiro-Silva, A.; Shaletich, C.; Careta, R.S.; Kazava, D.K.; Siqueira, M.C.; Ponton, F. Spiradenocarcinoma of the Breast Arising in a Long-Standing Spiradenoma. Ann. Diagn. Pathol. 2004, 8, 162–166. [Google Scholar] [CrossRef]
- Tanese, K.; Sato, T.; Ishiko, A. Malignant Eccrine Spiradenoma: Case Report and Review of the Literature, Including 15 Japanese Cases. Clin. Exp. Dermatol. 2010, 35, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Staiger, R.D.; Helmchen, B.; Papet, C.; Mattiello, D.; Zingg, U. Spiradenocarcinoma: A Comprehensive Data Review. Am. J. Dermatopathol. 2017, 39, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Andreoli, M.T.; Itani, K.M.F. Malignant Eccrine Spiradenoma: A Meta-Analysis of Reported Cases. Am. J. Surg. 2011, 201, 695–699. [Google Scholar] [CrossRef]
- Dabska, M. On malignant transformation of eccrine spiradenoma. Nowotwory 1971, 21, 37–45. [Google Scholar] [PubMed]
- Wargo, J.J.; Carr, D.R.; Plaza, J.A.; Verschraegen, C.F. Metastatic Spiradenocarcinoma Managed With PD-1 Inhibition. J. Natl. Compr. Cancer Netw. 2022, 20, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Vyas, N.S.; Mercer, S.E.; Phelps, R.G. Histological Findings and Pathologic Diagnosis of Spiradenocarcinoma: A Case Series and Review of the Literature. J. Cutan. Pathol. 2019, 46, 243–250. [Google Scholar] [CrossRef]
- Satturwar, S.; Wakely, P.E.; Lott Limbach, A. Fine Needle Aspiration Cytopathology of Eccrine Spiradenoma. J. Am. Soc. Cytopathol. 2022, 11, 274–280. [Google Scholar] [CrossRef]
- Wagner, K.; Jassal, K.; Lee, J.C.; Ban, E.-J.; Cameron, R.; Serpell, J. Challenges in Diagnosis and Management of a Spiradenocarcinoma: A Comprehensive Literature Review. ANZ J. Surg. 2021, 91, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Petitto, G.; Sarwari, N.M.; Jain, P.; Swaby, M.; Bhattacharjee, M. FDG PET/CT in Malignant Eccrine Spiradenoma. Clin. Nucl. Med. 2017, 42, 125–126. [Google Scholar] [CrossRef]
- Nyame, T.T.; Mattos, D.; Lian, C.G.; Granter, S.R.; Laga, A.C.; Caterson, E.J. Malignant Eccrine Spiradenoma of the Face. J. Craniofac. Surg. 2015, 26, 1711–1712. [Google Scholar] [CrossRef]
- Chow, W.; Griffiths, M. A Malignant Eccrine Spiradenoma of the Scalp. BMJ Case Rep. 2014, 2014, bcr2013202524. [Google Scholar] [CrossRef] [PubMed]
- Chase, D.M.; Basu, T.; Saffari, B.; Ries, S.; Berman, M.L. Malignant Eccrine Spiradenoma of the Vulva: A Case Report and Review of the Literature. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2006, 16, 1465–1469. [Google Scholar] [CrossRef]
- You, D.; Ma, Z.; Liu, J.; Song, X.; Dong, W. Malignant Eccrine Spiradenoma of the External Auditory Canal: A Case Report and Literature Review. Front. Oncol. 2020, 10, 574112. [Google Scholar] [CrossRef]
- SEER*Stat Databases: November 2021 Submission. Available online: https://seer.cancer.gov/data-software/documentation/seerstat/nov2021/index.html (accessed on 23 October 2022).
- Martinez, S.R.; Barr, K.L.; Canter, R.J. Rare Tumors Through the Looking Glass: An Examination of Malignant Cutaneous Adnexal Tumors. Arch. Dermatol. 2011, 147, 1058–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avraham, J.B.; Villines, D.; Maker, V.K.; August, C.; Maker, A.V. Survival after Resection of Cutaneous Adnexal Carcinomas with Eccrine Differentiation: Risk Factors and Trends in Outcomes: Survival Factors in Eccrine Carcinoma. J. Surg. Oncol. 2013, 108, 57–62. [Google Scholar] [CrossRef]
- Tripathi, R.; Ezaldein, H.H.; Scott, J.F.; Bordeaux, J.S. Trends in the Incidence and Survival of Eccrine Malignancies in the United States: A SEER Population-Based Study. J. Am. Acad. Dermatol. 2019, 80, 1769–1771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbs, D.C.; Yeung, H.; Blalock, T.W. Incidence and Trends of Cutaneous Adnexal Tumors in the United States in 2000-2018: A Population-Based Study. J. Am. Acad. Dermatol. 2022, 88, 226–228. [Google Scholar] [CrossRef]
- Garcovich, S.; Colloca, G.; Sollena, P.; Andrea, B.; Balducci, L.; Cho, W.C.; Bernabei, R.; Peris, K. Skin Cancer Epidemics in the Elderly as An Emerging Issue in Geriatric Oncology. Aging Dis. 2017, 8, 643. [Google Scholar] [CrossRef] [Green Version]
- Kazakov, D.V.; Benkova, K.; Michal, M.; Vanecek, T.; Kacerovska, D.; Skalova, A. Skin Type Spiradenoma of the Parotid Gland with Malignant Transformation: Report of a Case with Analysis of the CYLD Gene. Hum. Pathol. 2009, 40, 1499–1503. [Google Scholar] [CrossRef]
- van der Horst, M.P.J.; Marusic, Z.; Hornick, J.L.; Luzar, B.; Brenn, T. Morphologically Low-Grade Spiradenocarcinoma: A Clinicopathologic Study of 19 Cases with Emphasis on Outcome and MYB Expression. Mod. Pathol. 2015, 28, 944–953. [Google Scholar] [CrossRef] [Green Version]
- Beaulieu, D.; Fathi, R.; Mir, A.; Nijhawan, R.I. Spiradenocarcinoma Treated With Mohs Micrographic Surgery. Dermatol. Surg. 2019, 45, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Catteau, X.; D’haene, N.; Noël, J.-C. Low Grade Malignant Eccrine Spiradenoma of the Vulva: Case Report, Review of the Literature and Discussion about the Role of P53 and HPV. Diagn. Pathol. 2020, 15, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hantash, B.M.; Chan, J.L.; Egbert, B.M.; Gladstone, H.B. De Novo Malignant Eccrine Spiradenoma: A Case Report and Review of the Literature. Dermatol. Surg. 2006, 32, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Granter, S.R.; Seeger, K.; Calonje, E.; Busam, K.; McKee, P.H. Malignant Eccrine Spiradenoma (Spiradenocarcinoma): A Clinicopathologic Study of 12 Cases. Am. J. Dermatopathol. 2000, 22, 97–103. [Google Scholar] [CrossRef]
- Mirza, I.; Kloss, R.; Sieber, S.C. Malignant Eccrine Spiradenoma. Arch. Pathol. Lab. Med. 2002, 126, 591–594. [Google Scholar] [CrossRef]
- Morris, D.M.; Sanusi, I.D.; Lanehart, W.H. Carcinoma of Eccrine Sweat Gland: Experience with Chemotherapy, Autopsy Findings in a Patient with Metastatic Eccrine Carcinoma, and a Review of the Literature. J. Surg. Oncol. 1986, 31, 26–30. [Google Scholar] [CrossRef]
- Wu, C.; Chow, M.; Temby, M.; McCalmont, T.H.; Daud, A. Response to PD-1 Immunotherapy in Metastatic Spiradenocarcinoma. JCO Precis. Oncol. 2021, 5, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Scampa, M.; Merat, R.; Kalbermatten, D.F.; Oranges, C.M. Head and Neck Porocarcinoma: SEER Analysis of Epidemiology and Survival. J. Clin. Med. 2022, 11, 2185. [Google Scholar] [CrossRef]
- Aizer, A.A.; Chen, M.-H.; McCarthy, E.P.; Mendu, M.L.; Koo, S.; Wilhite, T.J.; Graham, P.L.; Choueiri, T.K.; Hoffman, K.E.; Martin, N.E.; et al. Marital Status and Survival in Patients With Cancer. J. Clin. Oncol. 2013, 31, 3869–3876. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Age at diagnosis | |
| <50 | 20 (22.2) |
| 50–69 | 39 (43.4) |
| ≥70 | 31 (34.4) |
| Sex | |
| Male | 43 (47.8) |
| Female | 47 (52.2) |
| Ethnicity | |
| White | 74 (82.2) |
| Black | 4 (4.4) |
| Asian or Pacific Islander | 7 (7.8) |
| Unknown | 5 (5.6) |
| Marital status | |
| Married | 35 (38.9) |
| Divorced | 8 (8.9) |
| Separated | 1 (1.1) |
| Single | 17 (18.9) |
| Widowed | 12 (13.3) |
| Unknown | 17 (18.9) |
| Year of diagnosis | |
| 2000–2004 | 18 (20) |
| 2005–2009 | 21 (23.3) |
| 2010–2014 | 23 (25.6) |
| 2015–2019 | 28 (31.1) |
| Primary site | |
| C07.9—Parotid gland | 1 (1.1) |
| C21.0—Anus, NOS | 1 (1.1) |
| C44.1—Eyelid | 1 (1.1) |
| C44.2—External ear | 4 (4.4) |
| C44.3—Skin other/unspec. parts of face | 10 (11.1) |
| C44.4—Skin of scalp and neck | 12 (13.3) |
| C44.5—Skin of trunk | 27 (30) |
| C44.6—Skin of upper limb and shoulder | 15 (16.7) |
| C44.7—Skin of lower limb and hip | 15 (16.7) |
| C44.9—Skin, NOS | 1 (1.1) |
| C51.0—Labium majus | 1 (1.1) |
| C51.9—Vulva, NOS | 1 (1.1) |
| C60.9—Penis, NOS | 1 (1.1) |
| Grade | |
| Well differentiated; Grade I | 2 (2.2) |
| Moderately differentiated; Grade II | 8 (8.9) |
| Poorly differentiated; Grade III | 7 (7.8) |
| Unknown | 73 (81.1) |
| Stage | |
| Localized | 59 (65.6) |
| Regional | 3 (3.3) |
| Distant | 2 (2.2) |
| Unstaged | 26 (28.9) |
| Tumor size | n = 49 |
| Mean | 37.6 mm |
| Std deviation | 33.1 mm |
| Range | 4–200 mm |
| Treatment | |
| No surgery or radiation | 7 (7.8) |
| Radiation only | 1 (1.1) |
| Surgery with radiation | 3 (3.3) |
| Surgery without radiation | 79 (87.8) |
| Type of surgery | |
| None | 8 (8.9) |
| Local tumor excision | 36 (40) |
| Biopsy of primary tumor followed by a gross excision | 15 (16.7) |
| Mohs surgery | 4 (4.4) |
| Wide excision or re-excision of lesion with margins > 1 cm | 25 (27.8) |
| Major amputation | 1 (1.1) |
| Unknown | 1 (1.1) |
| Reason for no surgery | |
| Not recommended | 6 (6.7) |
| Recommended but not performed, unknown reason | 2 (2.2) |
| Surgery performed | 82 (91.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martineau, J.; Walz, S.N.; Scampa, M.; Giordano, S.; Kalbermatten, D.F.; Oranges, C.M. Spiradenocarcinoma: SEER Study of Epidemiology, Survival, and Treatment Options. J. Clin. Med. 2023, 12, 2045. https://doi.org/10.3390/jcm12052045
Martineau J, Walz SN, Scampa M, Giordano S, Kalbermatten DF, Oranges CM. Spiradenocarcinoma: SEER Study of Epidemiology, Survival, and Treatment Options. Journal of Clinical Medicine. 2023; 12(5):2045. https://doi.org/10.3390/jcm12052045
Chicago/Turabian StyleMartineau, Jérôme, Solange N. Walz, Matteo Scampa, Salvatore Giordano, Daniel F. Kalbermatten, and Carlo M. Oranges. 2023. "Spiradenocarcinoma: SEER Study of Epidemiology, Survival, and Treatment Options" Journal of Clinical Medicine 12, no. 5: 2045. https://doi.org/10.3390/jcm12052045