
Inward Displacement: A Novel Method of Regional Left Ventricular Functional Assessment for Left Ventriculoplasty Interventions in Heart Failure with Reduced Ejection Fraction (HFrEF)
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
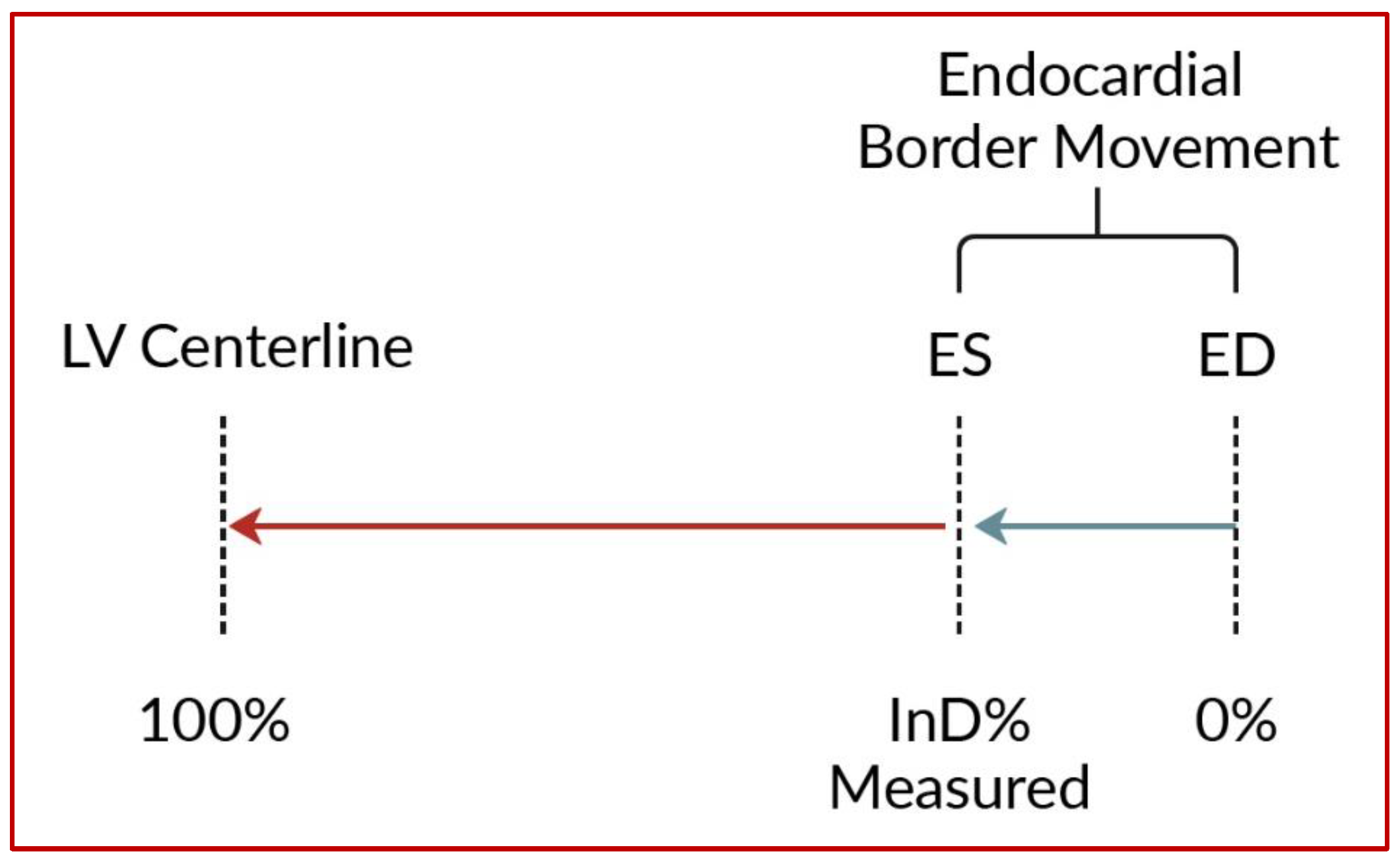
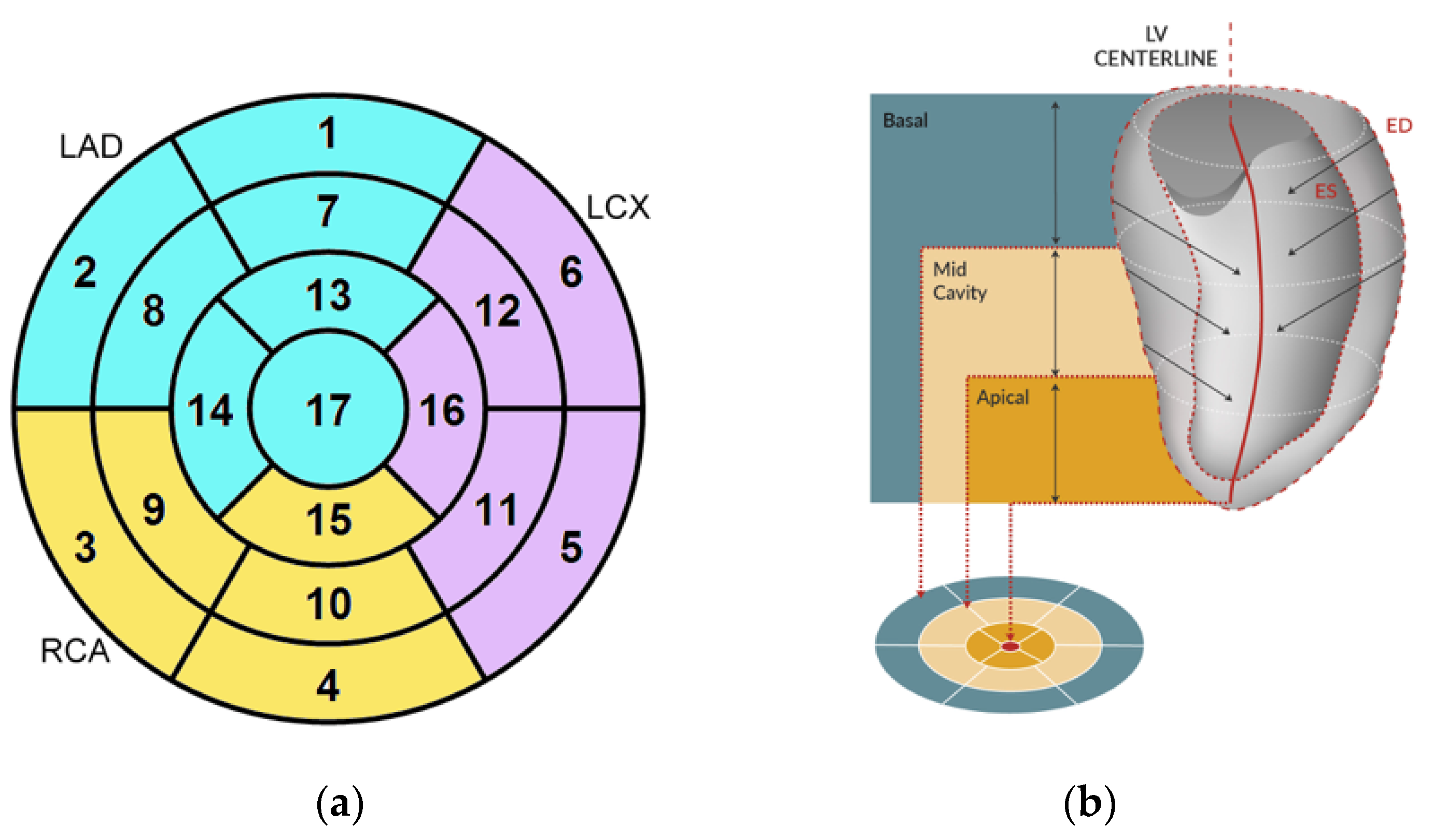
2.1. Inward Displacement
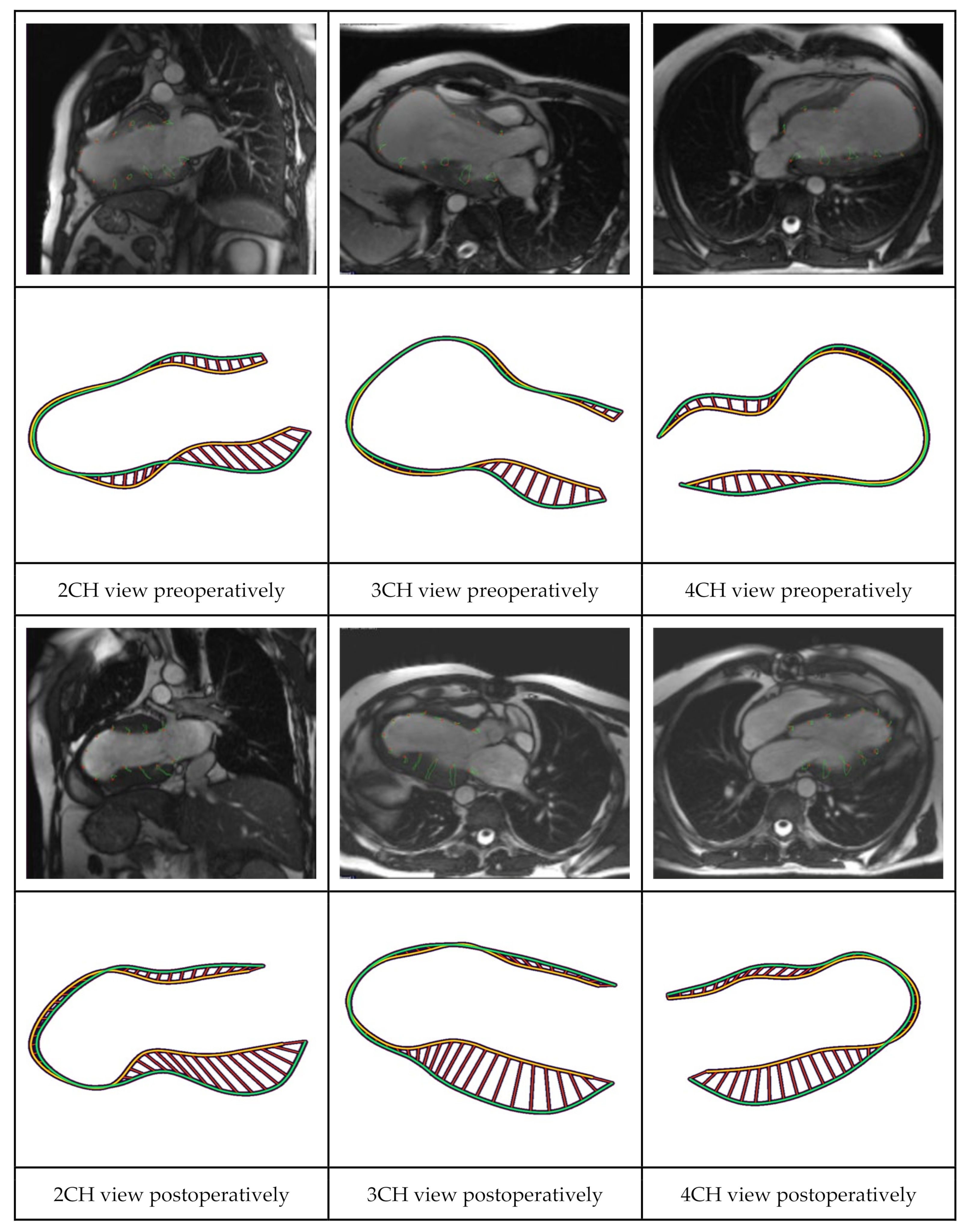
2.2. CMR and CT Analyses
2.3. Speckle Tracking Echocardiography
2.4. Study Population
2.5. Statistical Analysis
3. Results
3.1. Patient Selection
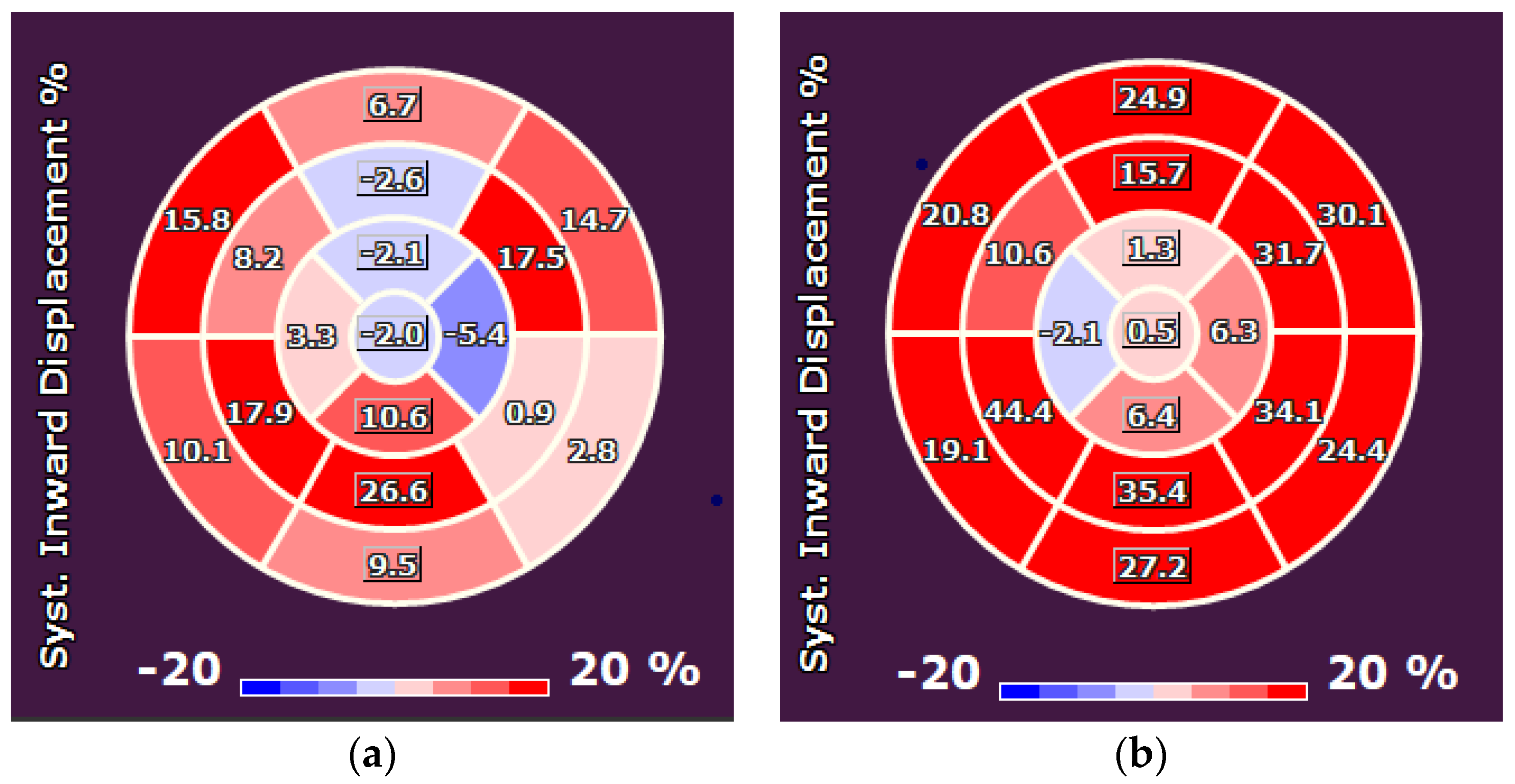
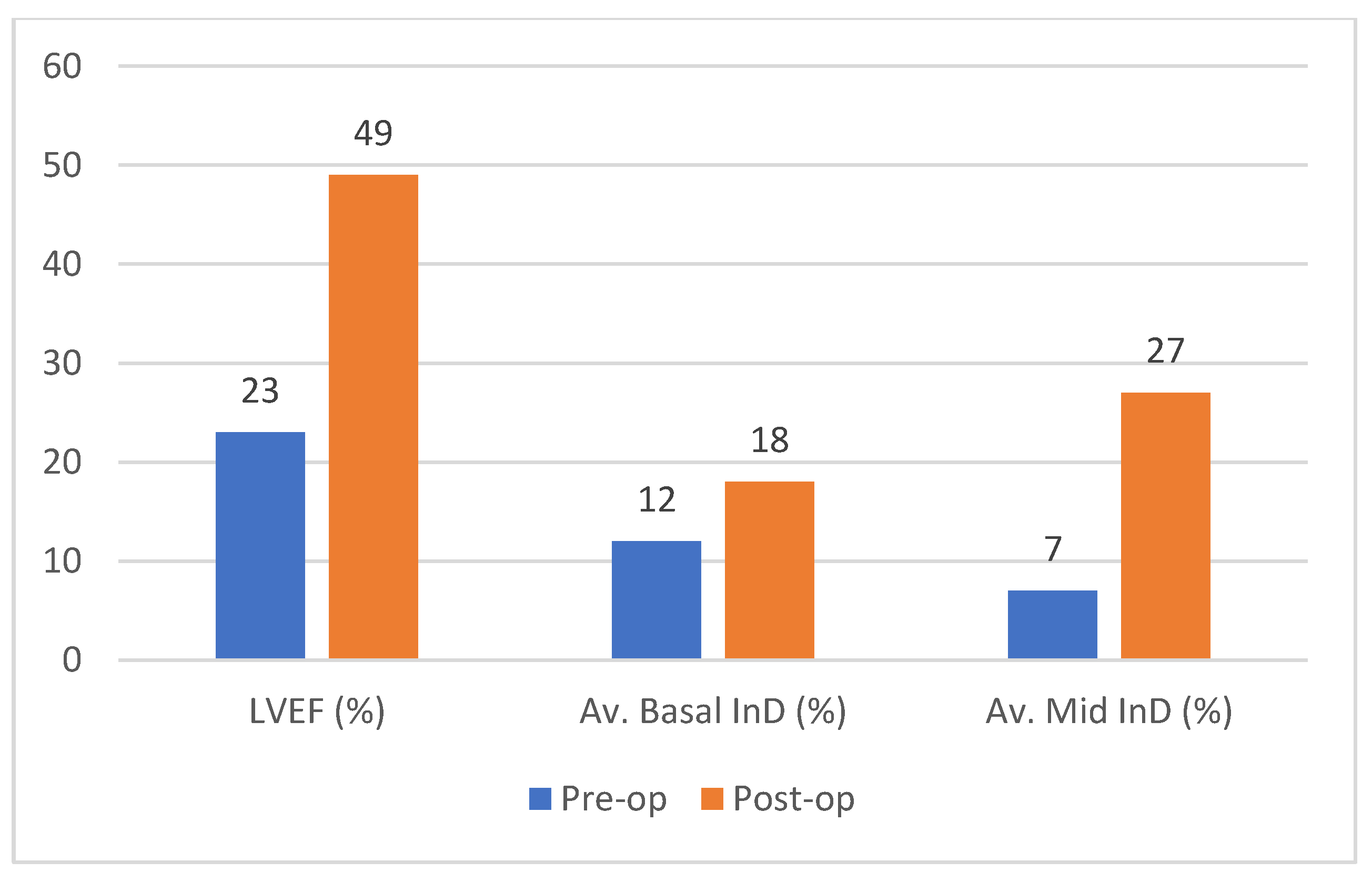
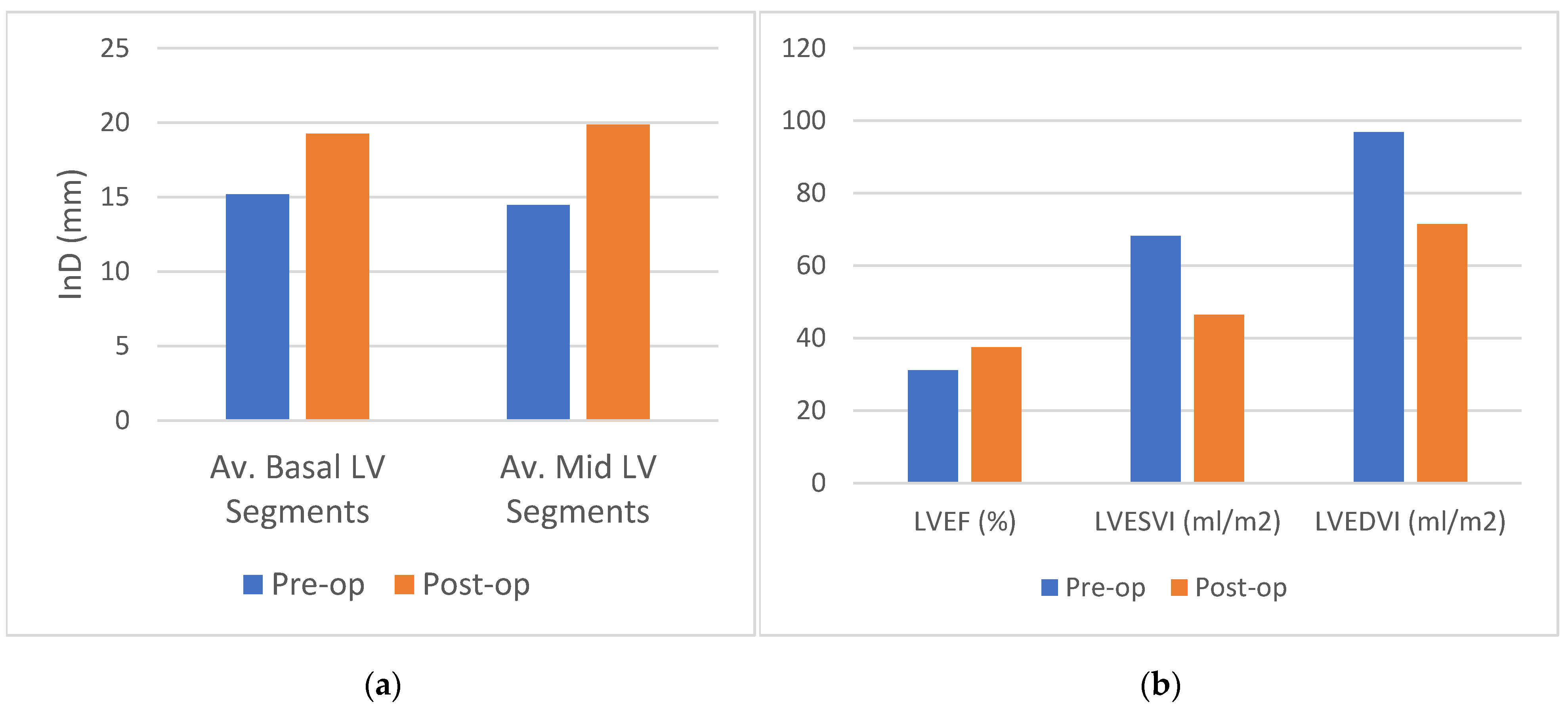
3.2. Analysis 1: InD Pre- and Post LVR
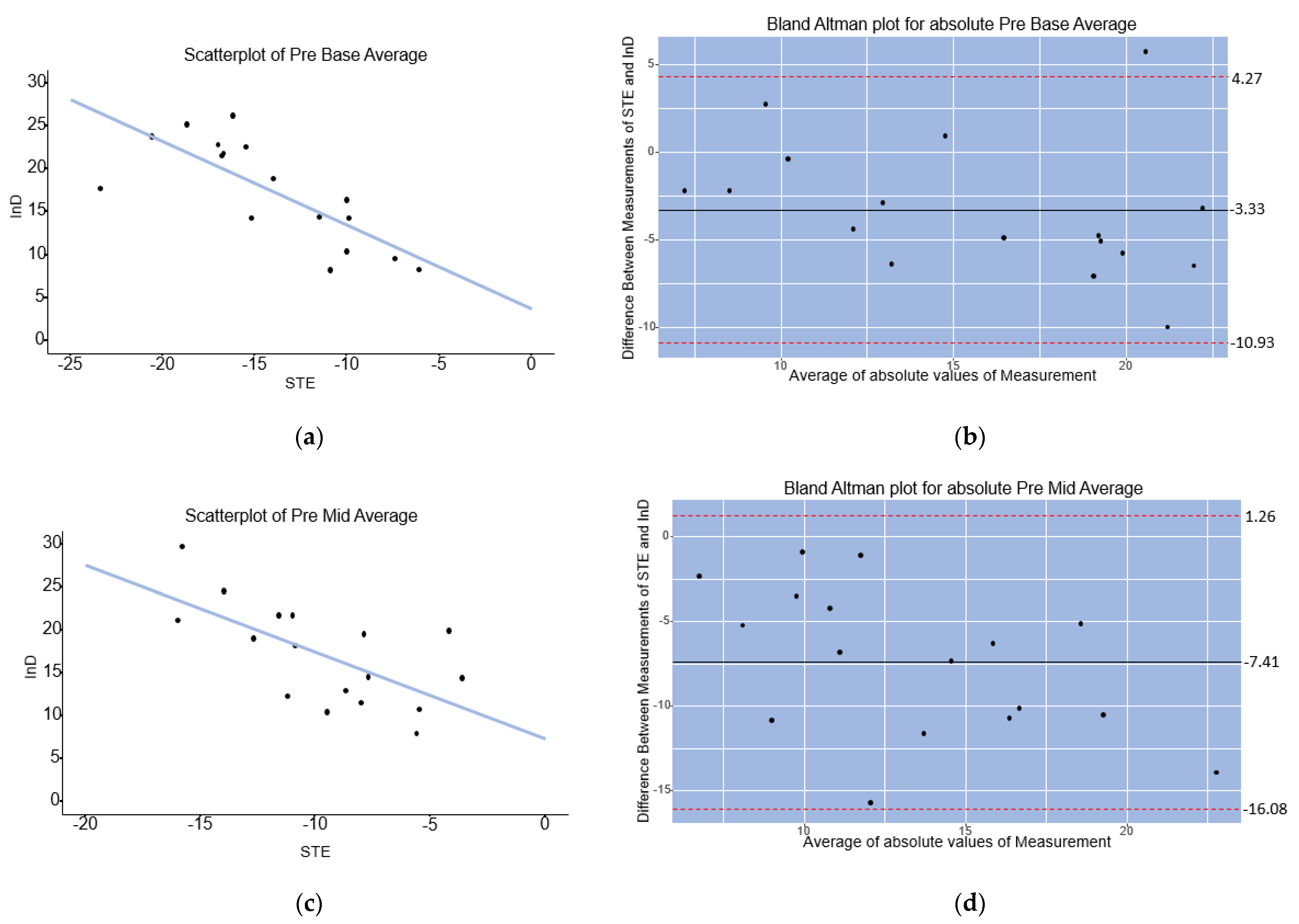
3.3. Analysis 2: Correlation of Baseline InD with STE
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Subramaniam, A.V.; Weston, S.A.; Killian, J.M.; Schulte, P.J.; Roger, V.L.; Redfield, M.M.; Blecker, S.B.; Dunlay, S.M. Development of Advanced Heart Failure: A Population-Based Study. Circ. Heart Fail. 2022, 15, e009218. [Google Scholar] [CrossRef] [PubMed]
- Hegeman, R.R.M.J.J.; Swaans, M.J.; van Kuijk, J.-P.; Klein, P. State-of-the-Art Review: Technical and Imaging Considerations in Hybrid Transcatheter and Minimally Invasive Left Ventricular Reconstruction for Ischemic Heart Failure. J. Clin. Med. 2022, 11, 4831. [Google Scholar] [CrossRef] [PubMed]
- Gooley, R.P.; Meredith, I.T. The Accucinch Transcatheter Direct Mitral Valve Annuloplasty System. EuroIntervention 2015, 11, w60–w61. [Google Scholar] [CrossRef] [PubMed]
- Brener, M.I.; Uriel, N.; Burkhoff, D. Left Ventricular Volume Reduction and Reshaping as a Treatment Option for Heart Failure. Struct. Heart 2020, 4, 264–283. [Google Scholar] [CrossRef]
- Cantinotti, M.; Koestenberger, M. Quantification of Left Ventricular Size and Function by 2-Dimensional Echocardiography: So Basic and So Difficult. Circ. Cardiovasc. Imaging 2017, 10, e007165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smistad, E.; Østvik, A.; Salte, I.M.; Melichova, D.; Nguyen, T.M.; Haugaa, K.; Brunvand, H.; Edvardsen, T.; Leclerc, S.; Bernard, O.; et al. Real-Time Automatic Ejection Fraction and Foreshortening Detection Using Deep Learning. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 2595–2604. [Google Scholar] [CrossRef] [PubMed]
- Castelvecchio, S.; Frigelli, M.; Sturla, F.; Milani, V.; Pappalardo, O.A.; Citarella, M.; Menicanti, L.; Votta, E. Elucidating the Mechanisms Underlying Left Ventricular Function Recovery in Patients with Ischemic Heart Failure Undergoing Surgical Remodeling: A 3-Dimensional Ultrasound Analysis. J. Thorac. Cardiovasc. Surg. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, F.H.; Bolson, E.L.; Dodge, H.T.; Mathey, D.G.; Schofer, J.; Woo, H.W. Advantages and Applications of the Centerline Method for Characterizing Regional Ventricular Function. Circulation 1986, 74, 293–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mady, C.; Salemi, V.M.C.; Ianni, B.M.; Arteaga, E.; Fernandes, F.; Ramires, F.J.A. Quantitative Assessment of Left Ventricular Regional Wall Motion in Endomyocardial Fibrosis. Arq. Bras. Cardiol. 2005, 84, 241–244. [Google Scholar] [PubMed]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef] [PubMed]
- De la Pena-Almaguer, E.; Hautemann, D.; Pedrizzetti, G. Computed Tomography Derived Left Ventricular Inward Displacement as a Novel Tool for Quantification of Segmental Wall Motion Abnormalities. Int. J. Cardiovasc. Imaging 2021, 37, 3589–3590. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; Machefsky, A.; Sanchez, A.A.; Patel, M.D.; Rogal, S.; Fowler, S.; Yaeger, L.; Hardi, A.; Holland, M.R.; Hamvas, A.; et al. Reference Ranges of Left Ventricular Strain Measures by Two-Dimensional Speckle-Tracking Echocardiography in Children: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2016, 29, 209–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, M.; Kasliwal, R.R. How Do i Do It? Speckle-Tracking Echocardiography. Indian Heart J. 2013, 65, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, P.; Anker, S.D.; Wechsler, A.; Skalsky, I.; Neuzil, P.; Annest, L.S.; Bifi, M.; McDonagh, T.; Frerker, C.; Schmidt, T.; et al. Less Invasive Ventricular Reconstruction for Ischaemic Heart Failure. Eur. J. Heart Fail. 2019, 21, 1638–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegeman, R.R.M.J.J.; Swaans, M.J.; Van Kuijk, J.-P.; Klein, P. Midterm Outcome of Hybrid Transcatheter and Minimally Invasive Left Ventricular Reconstruction for the Treatment of Ischemic Heart Failure. Struct. Heart 2022, 6, 100081. [Google Scholar] [CrossRef]
- Fudim, M.; Abraham, W.T.; von Bardeleben, R.S.; Lindenfeld, J.A.; Ponikowski, P.P.; Salah, H.M.; Khan, M.S.; Sievert, H.; Stone, G.W.; Anker, S.D.; et al. Device Therapy in Chronic Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 931–956. [Google Scholar] [CrossRef] [PubMed]
- Verdonschot, J.A.J.; Henkens, M.T.H.M.; Wang, P.; Schummers, G.; Raafs, A.G.; Krapels, I.P.C.; van Empel, V.; Heymans, S.R.B.; Brunner-La Rocca, H.P.; Knackstedt, C. A Global Longitudinal Strain Cut-Off Value to Predict Adverse Outcomes in Individuals with a Normal Ejection Fraction. ESC Heart Fail. 2021, 8, 4343–4345. [Google Scholar] [CrossRef] [PubMed]
- Kramer, D.G.; Trikalinos, T.A.; Kent, D.M.; Antonopoulos, G.V.; Konstam, M.A.; Udelson, J.E. Quantitative Evaluation of Drug or Device Effects on Ventricular Remodeling as Predictors of Therapeutic Effects on Mortality in Patients with Heart Failure and Reduced Ejection Fraction: A Meta-Analytic Approach. J. Am. Coll. Cardiol. 2010, 56, 392–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegeman, R.R.M.J.J.; McManus, S.; van Kuijk, J.-P.; Harb, S.C.; Swaans, M.J.; Klein, P.; Puri, R. Inward Displacement: A Novel Method of Regional Left Ventricular Functional Assessment for Left Ventriculoplasty Interventions in Heart Failure with Reduced Ejection Fraction (HFrEF). J. Clin. Med. 2023, 12, 1997. https://doi.org/10.3390/jcm12051997
Hegeman RRMJJ, McManus S, van Kuijk J-P, Harb SC, Swaans MJ, Klein P, Puri R. Inward Displacement: A Novel Method of Regional Left Ventricular Functional Assessment for Left Ventriculoplasty Interventions in Heart Failure with Reduced Ejection Fraction (HFrEF). Journal of Clinical Medicine. 2023; 12(5):1997. https://doi.org/10.3390/jcm12051997
Chicago/Turabian StyleHegeman, Romy R. M. J. J., Sean McManus, Jan-Peter van Kuijk, Serge C. Harb, Martin J. Swaans, Patrick Klein, and Rishi Puri. 2023. "Inward Displacement: A Novel Method of Regional Left Ventricular Functional Assessment for Left Ventriculoplasty Interventions in Heart Failure with Reduced Ejection Fraction (HFrEF)" Journal of Clinical Medicine 12, no. 5: 1997. https://doi.org/10.3390/jcm12051997