
Autoimmune Hepatitis and Fibrosis

 , ,
, ,  and
and 
Abstract
:1. Introduction
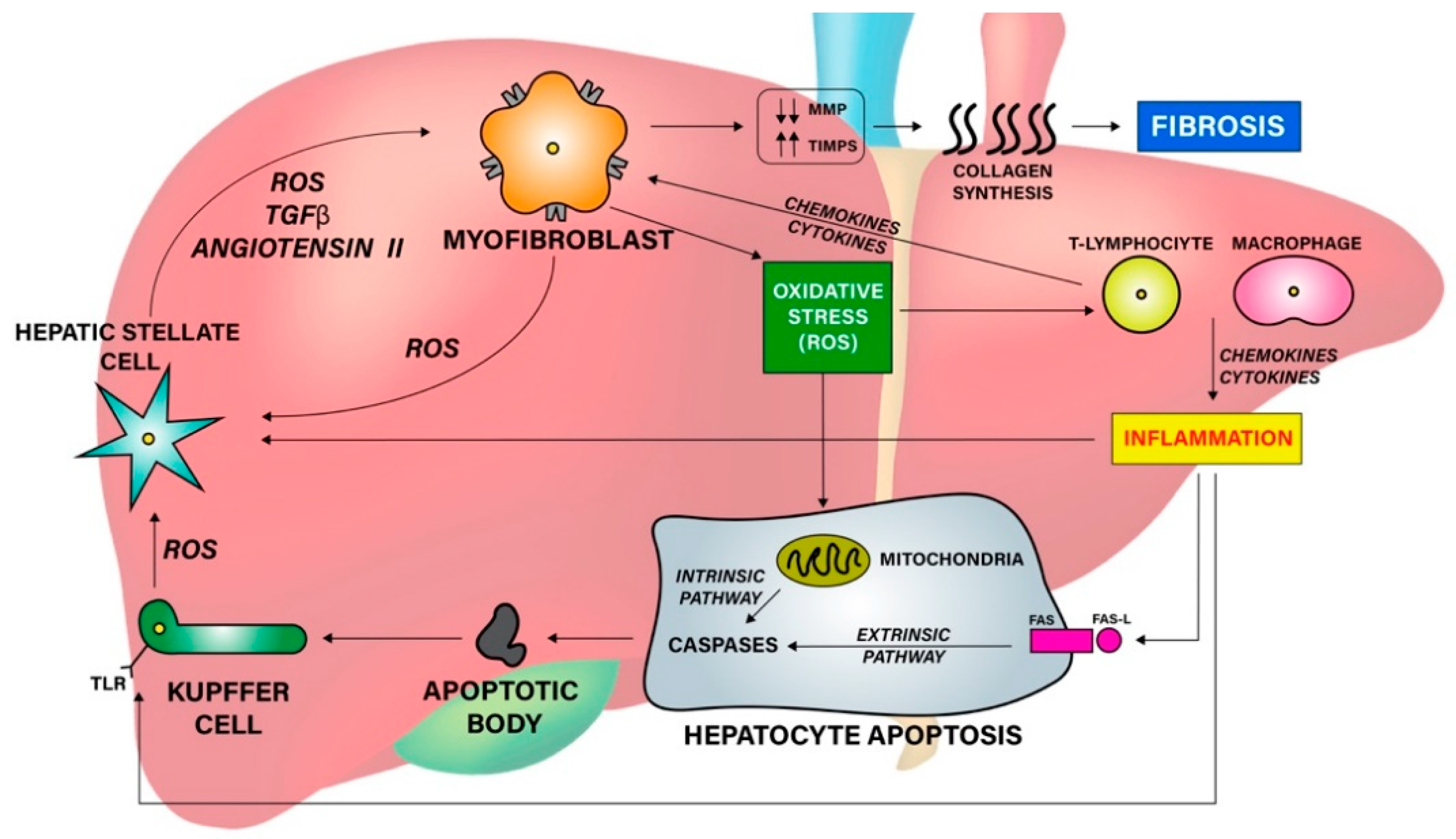
2. Fibrogenesis in AIH
3. Fibrosis Assessment
3.1. Liver Biopsy
3.2. Non-Invasive Laboratory Tests
3.2.1. Serum Biomarkers
3.2.2. Scoring Systems
3.3. Radiological Procedures
3.3.1. Conventional Ultrasound
3.3.2. Elastography
3.3.3. Magnetic Resonance Imaging
3.3.4. Computed Tomography
4. Fibrosis Treatment
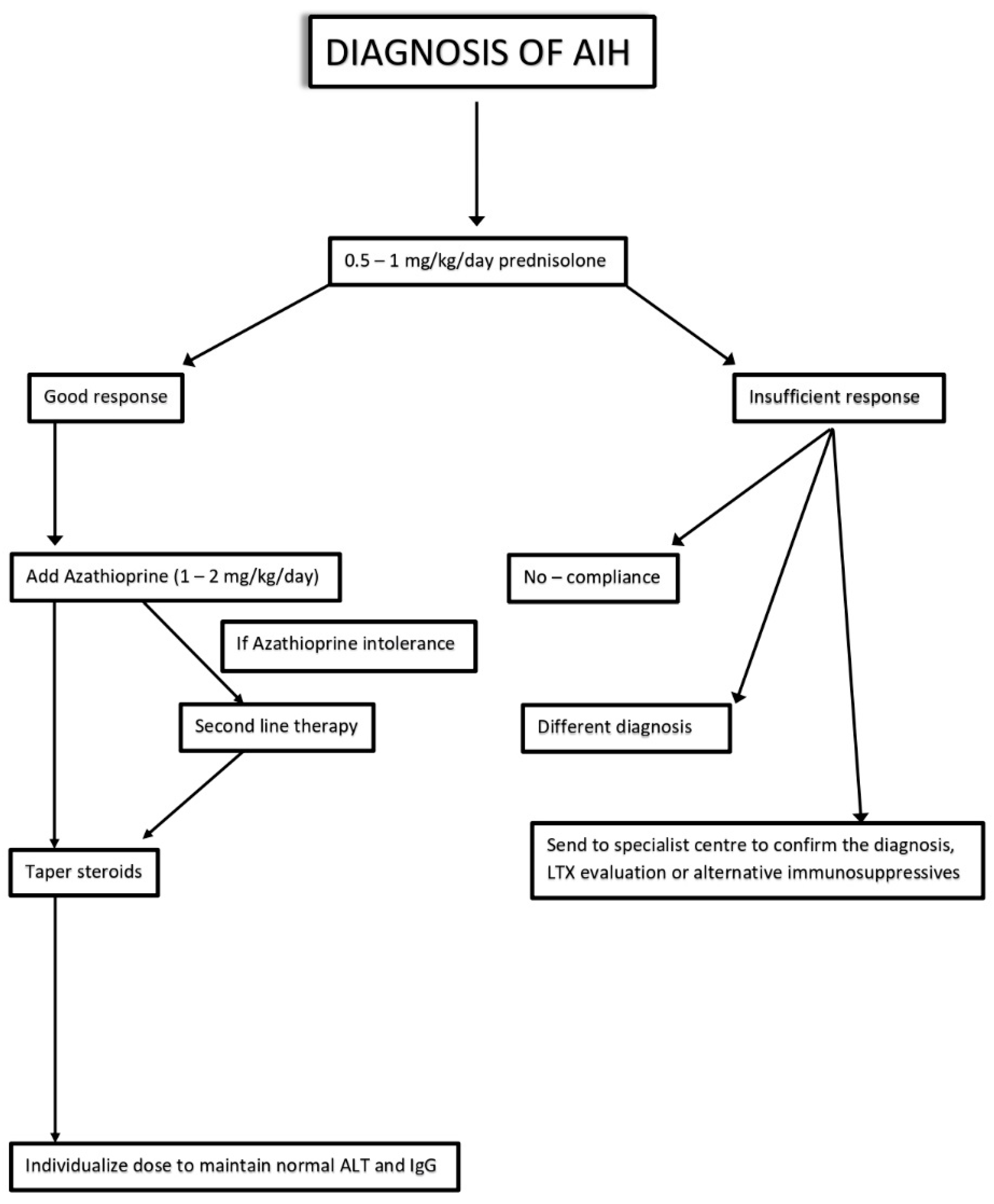
4.1. First-Line Therapies
4.2. Second-Line Therapies
4.3. Third-Line Therapies
4.4. New Therapeutic Perspectives
4.4.1. Pharmacological Agents in Development
4.4.2. Antioxidants
4.4.3. Gut Microbiota Modification
4.4.4. Epigenetic Regulation
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gatselis, N.K.; Zachou, K.; Koukoulis, G.K.; Dalekos, G.N. Autoimmune hepatitis, one disease with many faces: Etiopathogenetic, clinico-laboratory and histological characteristics. World J. Gastroenterol. 2015, 21, 60. [Google Scholar] [CrossRef] [PubMed]
- Komori, A. Recent updates on the management of autoimmune hepatitis. Clin. Mol. Hepatol. 2021, 27, 58. [Google Scholar] [CrossRef] [PubMed]
- Strassburg, C.P. Autoimmune hepatitis. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 667–682. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, P.W.; Aboutwerat, A.; Smith, A.; Burrows, P.C.; McMahon, R.F.; Warnes, T.W. Oxidant stress in type I autoimmune hepatitis: The link between necroinflammation and fibrogenesis? Biochim. Biophys. Acta 2004, 1689, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Hepatic inflammation and progressive liver fibrosis in chronic liver disease. World J. Gastroenterol. 2014, 20, 2515–2532. [Google Scholar] [CrossRef] [PubMed]
- Schuppan, D.; Ashfaq-Khan, M.; Yang, A.T.; Kim, Y.O. Liver fibrosis: Direct antifibrotic agents and targeted therapies. Matrix Biol. 2018, 68, 435–451. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Thandassery, R.B.; Czaja, A.J. Targeting hepatic fibrosis in autoimmune hepatitis. Dig. Dis. Sci. 2016, 61, 3118–3139. [Google Scholar] [CrossRef]
- Seki, E.; Schwabe, R.F. Hepatic inflammation and fibrosis: Functional links and key pathways. Hepatology 2015, 61, 1066–1079. [Google Scholar] [CrossRef] [Green Version]
- Saiman, Y.; Friedman, S.L. The role of chemokines in acute liver injury. Front. Physiol. 2012, 3, 213. [Google Scholar] [CrossRef] [Green Version]
- Altamirano-Barrera, A.; Barranco-Fragoso, B.; Méndez-Sánchez, N. Management strategies for liver fibrosis. Ann. Hepatol. 2017, 16, 48–56. [Google Scholar] [CrossRef]
- Lohse, A.W.; Chazouilleres, O.; Dalekos, G.; Drenth, J.; Heneghan, M.; Hofer, H. EASL clinical practice guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar]
- Sebode, M.; Hartl, J.; Vergani, D.; Lohse, A.W.; International Autoimmune Hepatitis Group. Autoimmune hepatitis: From current knowledge and clinical practice to future research agenda. Liver Int. 2018, 38, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez, F.; Berg, P.; Bianchi, F.; Bianchi, L.; Burroughs, A.; Cancado, E.; Chapman, R.; Cooksley, W.; Czaja, A.; Desmet, V.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Kessler, W.R.; Cummings, O.W.; Eckert, G.; Chalasani, N.; Lumeng, L.; Kwo, P.Y. Fulminant hepatic failure as the initial presentation of acute autoimmune hepatitis. Clin. Gastroenterol. Hepatol. 2004, 2, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Yasui, S.; Fujiwara, K.; Yonemitsu, Y.; Oda, S.; Nakano, M.; Yokosuka, O. Clinicopathological features of severe and fulminant forms of autoimmune hepatitis. J. Gastroenterol. 2011, 46, 378–390. [Google Scholar] [CrossRef]
- Stravitz, R.T.; Lefkowitch, J.H.; Fontana, R.J.; Gershwin, M.E.; Leung, P.S.C.; Sterling, R.K.; Manns, M.P.; Norman, G.L.; Lee, W.M.; the Acute Liver Failure Study Group. Autoimmune acute liver failure: Proposed clinical and histological criteria. Hepatology 2011, 53, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Panel, C.P.G.; Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis–2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar]
- Tsikrikoni, A.; Kyriakou, D.S.; Rigopoulou, E.I.; Alexandrakis, M.G.; Zachou, K.; Passam, F.; Dalekos, G.N. Markers of cell activation and apoptosis in bone marrow mononuclear cells of patients with autoimmune hepatitis type 1 and primary biliary cirrhosis. J. Hepatol. 2005, 42, 393–399. [Google Scholar] [CrossRef]
- Sakaguchi, K.; Kitano, M.; Nishimura, M.; Senoh, T.; Ohta, T.; Terao, M.; Shinji, N.; Koide, N.; Tsuji, T. Serum level of transforming growth factor-beta1 (TGF-beta1) and the expression of TGF-beta receptor type II in peripheral blood mononuclear cells in patients with autoimmune hepatitis. Hepato-Gastroenterol. 2004, 51, 1780–1783. [Google Scholar]
- Li, Y.S.; Ni, S.Y.; Meng, Y.; Shi, X.L.; Zhao, X.W.; Luo, H.H.; Li, X. Angiotensin II facilitates fibrogenic effect of TGF-β1 through enhancing the down-regulation of BAMBI caused by LPS: A new pro-fibrotic mechanism of angiotensin II. PLoS ONE 2013, 8, e76289. [Google Scholar] [CrossRef]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.F. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowlus, C.L.; Patel, K.; Guha, I.N.; Chapman, R.W.; Chazouilleres, O.; Chalasani, N.P.; Vierling, J.M.; Myers, R.P.; Ding, D.; Schall, R.E.A.; et al. Validation of serum fibrosis marker panels in patients with primary sclerosing cholangitis (PSC) in a randomized trial of simtuzumab. Hepatology 2015, 62, 519a. [Google Scholar]
- Tadokoro, T.; Morishita, A.; Masaki, T. Diagnosis and therapeutic management of liver fibrosis by MicroRNA. Int. J. Mol. Sci. 2021, 22, 8139. [Google Scholar] [CrossRef] [PubMed]
- Fagoonee, S.; Arigoni, M.; Manco, M.; Olivero, M.; Bizzaro, F.; Magagnotti, C.; Andolfo, A.; Miniscalco, B.; Forni, M.; Todeschi, S.; et al. Circulating extracellular vesicles contain liver-derived RNA species as indicators of severe cholestasis-induced early liver fibrosis in mice. Antioxid. Redox Signal. 2022, 36, 480–504. [Google Scholar] [CrossRef] [PubMed]
- Houot, M.; Ngo, Y.; Munteanu, M.; Marque, S.; Poynard, T. Systematic review with meta-analysis: Direct comparisons of biomarkers for the diagnosis of fibrosis in chronic hepatitis C and B. Aliment. Pharmacol. Ther. 2016, 43, 16–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poynard, T.; de Ledinghen, V.; Zarski, J.P.; Stanciu, C.; Munteanu, M.; Vergniol, J.; France, J.; Trifan, A.; Le Naour, G.; Vaillant, J.C.; et al. Relative performances of FibroTest, Fibroscan, and biopsy for the assessment of the stage of liver fibrosis in patients with chronic hepatitis C: A step toward the truth in the absence of a gold standard. J. Hepatol. 2012, 56, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Vali, Y.; Lee, J.; Boursier, J.; Spijker, R.; Verheij, J.; Brosnan, M.; Anstee, Q.; Bossuyt, P.; Zafarmand, M.; on behalf of the LITMUS Systematic Review Team. FibroTest for evaluating fibrosis in non-alcoholic fatty liver disease patients: A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 2415. [Google Scholar] [CrossRef]
- Dong, B.; Lyu, G.; Chen, Y.; Lin, G.; Wang, H.; Qin, R.; Gu, J. Comparison of two-dimensional shear wave elastography, magnetic resonance elastography, and three serum markers for diagnosing fibrosis in patients with chronic hepatitis B: A meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 1077–1089. [Google Scholar] [CrossRef]
- El Serafy, M.A.; Kassem, A.M.; Omar, H.; Mahfouz, M.S.; Maissa El Said, E.L. APRI test and hyaluronic acid as non-invasive diagnostic tools for post HCV liver fibrosis: Systematic review and meta-analysis. Arab. J. Gastroenterol. 2006, 18, 51–57. [Google Scholar] [CrossRef]
- Durazzo, M.; Marzari, L.; Bonetto, S.; Ferro, A.; Ghigo, M.C.; Belci, P.; Collo, A.; Fagoonee, S. Noninvasive diagnosis of fibrosis in non-alcoholic fatty liver disease: Diagnostic accuracy of different scores. Minerva Gastroenterol. Dietol. 2020, 66, 301–306. [Google Scholar] [CrossRef]
- Ismaiel, A.; Leucuta, D.C.; Popa, S.L.; Fagoonee, S.; Pellicano, R.; Abenavoli, L.; Dumitrascu, D.L. Non-invasive biomarkers in predicting non-alcoholic steatohepatitis and assessing liver fibrosis: Systematic review and meta-analysis. Panminerva Med. 2021, 63, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Yang, Z.; Zhou, J.; Zeng, N.; He, Z.; Zhan, S.; Jia, J.; You, H. Systematic review: Diagnostic accuracy of non-invasive tests for staging liver fibrosis in autoimmune hepatitis. Hepatol. Int. 2019, 13, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.; Chen, Y.; Lyu, G.; Yang, X. Aspartate Aminotransferase to Platelet Ratio Index and Fibrosis-4 Index for Detecting Liver Fibrosis in Patients With Autoimmune Hepatitis: A Meta-Analysis. Front. Immunol. 2022, 13, 892454. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Duan, S.Z.; Cao, J.; Gao, N.; Xu, J.; Zhang, L. Noninvasive inflammatory markers for assessing liver fibrosis stage in autoimmune hepatitis patients. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1467. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. Comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Ai, L.; Mu, S.; Hu, Y. Prognostic role of RDW in hematological malignancies: A systematic review and meta-analysis. Cancer Cell Int. 2018, 18, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iida, H.; Kaibori, M.; Matsui, K.; Ishizaki, M.; Kon, M. Ratio of mean platelet volume to platelet count is a potential surrogate marker predicting liver cirrhosis. World J. Hepatol. 2018, 10, 82–87. [Google Scholar] [CrossRef]
- Chen, M.; Wu, Z.; Du, Z.; Sun, S.; Wu, J.; Luo, J. Diagnostic accuracy of red blood cell distribution width to platelet ratio for predicting liver fibrosis in patients with chronic hepatitis B: A meta-analysis. Gastroenterol. Hepatol. 2022, 45, 361–372. [Google Scholar] [CrossRef]
- Gozdas, H.T.; Ince, N. Elevated mean platelet volume to platelet ratio predicts advanced fibrosis in chronic hepatitis C. Eur. J. Gastroenterol. Hepatol. 2020, 32, 524–527. [Google Scholar] [CrossRef]
- Li, X.; Xu, H.; Gao, P. Red blood cell distribution width-to-platelet ratio and other laboratory indices associated with severity of histological hepatic fibrosis in patients with autoimmune hepatitis: A retrospective study at a single center. Med. Sci. Monit. 2020, 26, e927946-1. [Google Scholar] [CrossRef]
- Malik, N.; Venkatesh, S.K. Imaging of autoimmune hepatitis and overlap syndromes. Abdom. Radiol. 2017, 42, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Di Lelio, A.; Cestari, C.; Lomazzi, A.; Beretta, L. Cirrhosis: Diagnosis with sonographic study of the liver surface. Radiology 1989, 172, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Hepatocellular carcinoma and other malignancies in autoimmune hepatitis. Dig. Dis. Sci. 2013, 58, 1459–1476. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, E.A.; Mózes, F.E.; Jayaswal, A.N.A.; Zafarmand, M.H.; Vali, Y.; Lee, J.A.; Levick, C.K.; Young, L.A.J.; Palaniyappan, N.; Liu, C.-H.; et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: A systematic review and meta-analysis. J. Hepatol. 2021, 75, 770–785. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, E.; de Lédinghen, V.; Cassinotto, C.; Chu, W.C.W.; Leung, V.Y.F.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: An individual patient data-based meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017. Ultraschall Med. 2017, 38, e16–e47. [Google Scholar]
- Zhou, X.; Rao, J.; Wu, X.; Deng, R.; Ma, Y. Comparison of 2-D shear wave elastography and point shear wave elastography for assessing liver fibrosis. Ultrasound Med. Biol. 2021, 47, 408–427. [Google Scholar] [CrossRef]
- Park, D.W.; Lee, Y.J.; Chang, W.; Park, J.H.; Lee, K.H.; Kim, Y.H.; Kang, N.K.; Chung, J.W.; Jang, H.Y.; Ahn, S.; et al. Diagnostic performance of a point shear wave elastography (pSWE) for hepatic fibrosis in patients with autoimmune liver disease. PLoS ONE 2019, 14, e0212771. [Google Scholar] [CrossRef] [Green Version]
- Xing, X.; Yan, Y.; Shen, Y.; Xue, M.; Wang, X.; Luo, X.; Yang, L. Liver fibrosis with two-dimensional shear-wave elastography in patients with autoimmune hepatitis. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 631–638. [Google Scholar] [CrossRef]
- Galina, P.; Alexopoulou, E.; Mentessidou, A.; Mirilas, P.; Zellos, A.; Lykopoulou, L.; Patereli, A.; Salpasaranis, K.; Kelekis, N.L.; Zarifi, M. Diagnostic accuracy of two-dimensional shear wave elastography in detecting hepatic fibrosis in children with autoimmune hepatitis, biliary atresia and other chronic liver diseases. Pediatr. Radiol. 2021, 51, 1358–1368. [Google Scholar] [CrossRef]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.-M.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient elastography: A new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Su, Y.; Song, R.; Sheng, Y.; Ai, W.; Wu, X.; Liu, H. Performance of transient elastography assessing fibrosis of single hepatitis B virus infection: A systematic review and meta-analysis of a diagnostic test. Hepatol. Int. 2015, 9, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.; Gurusamy, K.S.; Ntaoula, S.; Cholongitas, E.; Davidson, B.R.; Burroughs, A.K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, Y.-S.; Wang, Z.-Z.; Yang, Z.-R.; Sun, F.; Zhan, S.-Y.; Liu, X.-E.; Zhuang, H. Systematic review with meta-analysis: The diagnostic accuracy of transient elastography for the staging of liver fibrosis in patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 2016, 43, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic accuracy of non-invasive tests for advanced fibrosis in patients with NAFLD: An individual patient data meta-analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef]
- Gu, Q.; Cen, L.; Lai, J.; Zhang, Z.; Pan, J.; Zhao, F.; Yu, C.; Li, Y.; Chen, C.; Chen, W.; et al. A meta-analysis on the diagnostic performance of magnetic resonance imaging and transient elastography in nonalcoholic fatty liver disease. Eur. J. Clin. Investig. 2021, 51, e13446. [Google Scholar] [CrossRef]
- Shi, K.Q.; Fan, Y.C.; Pan, Z.Z.; Lin, X.F.; Liu, W.Y.; Chen, Y.P.; Zheng, M.H. Transient elastography: A meta-analysis of diagnostic accuracy in evaluation of portal hypertension in chronic liver disease. Liver Int. 2013, 33, 62–71. [Google Scholar] [CrossRef]
- Guo, L.; Zheng, L.; Hu, L.; Zhou, H.; Yu, L.; Liang, W. Transient elastography (FibroScan) performs better than non-invasive markers in assessing liver fibrosis and cirrhosis in autoimmune hepatitis patients. Med. Sci. Monit. 2017, 23, 5106. [Google Scholar] [CrossRef] [Green Version]
- Hartl, J.; Denzer, U.; Ehlken, H.; Zenouzi, R.; Peiseler, M.; Sebode, M.; Hübener, S.; Pannicke, N.; Weiler-Normann, C.; Quaas, A.; et al. Transient elastography in autoimmune hepatitis: Timing determines the impact of inflammation and fibrosis. J. Hepatol. 2016, 65, 769–775. [Google Scholar] [CrossRef]
- Sagir, A.; Erhardt, A.; Schmitt, M.; Häussinger, D. Transient elastography is unreliable for detection of cirrhosis in patients with acute liver damage. Hepatology 2008, 47, 592–595. [Google Scholar] [CrossRef]
- Janik, M.K.; Kruk, B.; Szczepankiewicz, B.; Kostrzewa, K.; Raszeja-Wyszomirska, J.; Górnicka, B.; Lammert, F.; Milkiewicz, P.; Krawczyk, M. Measurement of liver and spleen stiffness as complementary methods for assessment of liver fibrosis in autoimmune hepatitis. Liver Int. 2021, 41, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.-S.; Vergniol, J.; Wong, G.L.-H.; Foucher, J.; Chan, A.; Chermak, F.; Choi, P.C.-L.; Merrouche, W.; Chu, S.H.-T.; Pesque, S.; et al. Liver stiffness measurement using XL probe in patients with nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2012, 107, 1862–1871. [Google Scholar] [CrossRef] [PubMed]
- Arena, U.; Lupsor Platon, M.; Stasi, C.; Moscarella, S.; Assarat, A.; Bedogni, G.; Piazzolla, V.; Badea, R.; Laffi, G.; Marra, F.; et al. Liver stiffness is influenced by a standardized meal in patients with chronic hepatitis C virus at different stages of fibrotic evolution. Hepatology 2013, 58, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Van Katwyk, S.; Coyle, D.; Cooper, C.; Pussegoda, K.; Cameron, C.; Skidmore, B.; Brener, S.; Moher, D.; Thavorn, K. Transient elastography for the diagnosis of liver fibrosis: A systematic review of economic evaluations. Liver Int. 2017, 37, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, C.J. Magnetic resonance spectroscopy. Sci. Prog. 2017, 100, 241–292. [Google Scholar] [CrossRef]
- Hsu, C.; Caussy, C.; Imajo, K.; Chen, J.; Singh, S.; Kaulback, K.; Le, M.-D.; Hooker, J.; Tu, X.; Bettencourt, R.; et al. Magnetic resonance vs transient elastography analysis of patients with nonalcoholic fatty liver disease: A systematic review and pooled analysis of individual participants. Clin. Gastroenterol. Hepatol. 2019, 17, 630–637. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Malik, N.; Yin, M.; Smyrk, T.C.; Czaja, A.J.; Ehman, R.L.; Venkatesh, S.K. Magnetic resonance elastography is accurate in detecting advanced fibrosis in autoimmune hepatitis. World J. Gastroenterol. 2017, 23, 859. [Google Scholar] [CrossRef]
- Sevastianova, K.; Hakkarainen, A.; Kotronen, A.; Cornér, A.; Arkkila, P.; Arola, J.; Westerbacka, J.; Bergholm, R.; Lundbom, J.; Lundbom, N.; et al. Nonalcoholic fatty liver disease: Detection of elevated nicotinamide adenine dinucleotide phosphate with in vivo 3.0-T 31P MR spectroscopy with proton decoupling. Radiology 2010, 256, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Orlacchio, A.; Bolacchi, F.; Cadioli, M.; Bergamini, A.; Cozzolino, V.; Angelico, M.; Simonetti, G. Evaluation of the severity of chronic hepatitis C with 3-T1H-MR spectroscopy. Am. J. Roentgenol. 2008, 190, 1331–1339. [Google Scholar] [CrossRef] [Green Version]
- Puustinen, L.; Hakkarainen, A.; Kivisaari, R.; Boyd, S.; Nieminen, U.; Färkkilä, M.; Lundbom, N.; Arkkila, P. 31Phosphorus magnetic resonance spectroscopy of the liver for evaluating inflammation and fibrosis in autoimmune hepatitis. Scand. J. Gastroenterol. 2017, 52, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Romero-Gómez, M.; Gómez-González, E.; Madrazo, A.; Vera-Valencia, M.; Rodrigo, L.; Pérez-Alvarez, R.; Pérez-López, R.; Castellano-Megias, V.M.; Nevado-Santos, M.; Alcón, J.C.; et al. Optical analysis of computed tomography images of the liver predicts fibrosis stage and distribution in chronic hepatitis C. Hepatology 2008, 47, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Son, J.H.; Lee, S.S.; Lee, Y.; Kang, B.K.; Sung, Y.S.; Jo, S.; Yu, E. Assessment of liver fibrosis severity using computed tomography–based liver and spleen volumetric indices in patients with chronic liver disease. Eur. Radiol. 2020, 30, 3486–3496. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, L.; Weng, H.L.; Liebe, R.; Ding, H.G. Computed tomography vs liver stiffness measurement and magnetic resonance imaging in evaluating esophageal varices in cirrhotic patients: A systematic review and meta-analysis. World J. Gastroenterol. 2020, 26, 2247. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.L.; Salomon, J.A.; Goldie, S.J.; Chung, R.T. Cost effectiveness of alternative surveillance strategies for hepatocellular carcinoma in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2008, 6, 1418–1424. [Google Scholar] [CrossRef] [Green Version]
- Liberal, R.; Krawitt, E.L.; Vierling, J.M.; Manns, M.P.; Mieli-Vergani, G.; Vergani, D. Cutting edge issues in autoimmune hepatitis. J. Autoimmun. 2016, 75, 6–19. [Google Scholar] [CrossRef]
- Czaja, A.J. Current and prospective pharmacotherapy for autoimmune hepatitis. Expert Opin. Pharmacother. 2014, 15, 1715–1736. [Google Scholar] [CrossRef]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and management of autoimmune hepatitis in adults and children: 2019 practice guidance and guidelines from the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [Green Version]
- Soloway, R.D.; Summerskill, W.H.J.; Baggenstoss, A.H.; Geall, M.G.; Gitnick, G.L.; Elveback, L.R.; Schoenfield, L.J. Clinical, biochemical, and histological remission of severe chronic active liver disease: A controlled study of treatments and early prognosis. Gastroenterology 1972, 63, 820–833. [Google Scholar] [CrossRef]
- Czaja, A.J.; Menon, K.N.; Carpenter, H.A. Sustained remission after corticosteroid therapy for type 1 autoimmune hepatitis: A retrospective analysis. Hepatology 2002, 35, 890–897. [Google Scholar] [CrossRef]
- Lamers, M.M.; van Oijen, M.G.; Pronk, M.; Drenth, J.P. Treatment options for autoimmune hepatitis: A systematic review of randomized controlled trials. J. Hepatol. 2010, 53, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Manns, M.P.; Woynarowski, M.; Kreisel, W.; Lurie, Y.; Rust, C.; Zuckerman, E.; Bahr, M.J.; Günther, R.; Hultcrantz, R.W.; Spengler, U.; et al. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology 2010, 134, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Hempfling, W.; Grunhage, F.; Dilger, K.; Reichel, C.; Beuers, U.; Sauerbruch, T. Pharmacokinetics and pharmacodynamic action of budesonide in early-and late-stage primary biliary cirrhosis. Hepatology 2003, 38, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Sharzehi, K.; Huang, M.A.; Schreibman, I.R.; Brown, K.A. Mycophenolate mofetil for the treatment of autoimmune hepatitis in patients refractory or intolerant to conventional therapy. Can. J. Gastroenterol. 2010, 24, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Lohse, A.W.; Sebode, M.; Jørgensen, M.H.; Ytting, H.; Karlsen, T.H.; Kelly, D.; Manns, M.P.; Vesterhus, M.; European Reference Network on Hepatological Diseases (ERN RARE-LIVER); International Autoimmune Hepatitis Group (IAIHG). Second-line and third-line therapy for autoimmune hepatitis: A position statement from the European Reference Network on Hepatological Diseases and the International Autoimmune Hepatitis Group. J. Hepatol. 2020, 73, 1496–1506. [Google Scholar] [CrossRef] [PubMed]
- Zachou, K.; Gatselis, N.; Papadamou, G.; Rigopoulou, E.I.; Dalekos, G.N. Mycophenolate for the treatment of autoimmune hepatitis: Prospective assessment of its efficacy and safety for induction and maintenance of remission in a large cohort of treatment-naive patients. J. Hepatol. 2011, 55, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Hlivko, J.T.; Shiffman, M.L.; Stravitz, R.T.; Luketic, V.A.; Sanyal, A.J.; Fuchs, M.; Sterling, R.K. A single center review of the use of mycophenolate mofetil in the treatment of autoimmune hepatitis. Clin. Gastroenterol. Hepatol. 2008, 6, 1036–1040. [Google Scholar] [CrossRef]
- Hennes, E.M.; Oo, Y.H.; Schramm, C.; Denzer, U.; Buggisch, P.; Wiegard, C.; Kanzler, S.; Schuchmann, M.; Boecher, W.; Galle, P.R.; et al. Mycophenolate mofetil as second line therapy in autoimmune hepatitis? Am. J. Gastroenterol. 2008, 103, 3063–3070. [Google Scholar] [CrossRef]
- Czaja, A.J. Mycophenolate mofetil to the rescue in autoimmune hepatitis: A fresh sprout on the decision tree. J. Hepatol. 2009, 51, 8–10. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.J.; Zhang, L.L.; Huang, T.T.; Zhu, J.S.; He, Z.B. Comparison of mycophenolate mofetil with standard treatment for autoimmune hepatitis: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 873–877. [Google Scholar] [CrossRef]
- Furukawa, A.; Wisel, S.A.; Tang, Q. Impact of immune- modulatory drugs on regulatory T cell. Transplantation 2016, 100, 2288–2300. [Google Scholar] [CrossRef] [Green Version]
- Sherman, K.E.; Narkewicz, M.; Pinto, P.C. Cyclosporine in the management of corticosteroid-resistant type I autoimmune chronic active hepatitis. J. Hepatol. 1994, 21, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.F.; Redeker, A.G.; Vierling, J.M.; Villamil, F.G.; Fong, T.L. Cyclosporine therapy in patients with steroid resistant autoimmune hepatitis. Am. J. Gastroenterol. 1999, 94, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Bucy, R.P.; Xu, X.Y.; Li, J.; Huang, G. Cyclosporin A-induced autoimmune disease in mice. J. Immunol. 1993, 151, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.Y.; Goldschneider, I. Cyclosporin A-induced autologous graft-versus-host disease: A prototypical model of autoimmunity and active (dominant) tolerance coordinately induced by recent thymic emigrants. J. Immunol. 1999, 162, 6926–6933. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, R.; Nasseri-Moghaddam, S.; Kaviani, M.J.; Taheri, H.; Kamalian, N.; Sotoudeh, M. Cyclosporin A is a promising alternative to corticosteroids in autoimmune hepatitis. Dig. Dis. Sci. 2001, 46, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Larsen, F.S.; Vainer, B.; Eefsen, M.; Bjerring, P.N.; Hansen, B.A. Low-dose tacrolimus ameliorates liver inflammation and fibrosis in steroid refractory autoimmune hepatitis. World J. Gastroenterol. 2007, 13, 3232. [Google Scholar] [CrossRef]
- Rubin, J.N.; Te, H.S. Refractory autoimmune hepatitis: Beyond standard therapy. Dig. Dis. Sci. 2016, 61, 1757–1762. [Google Scholar] [CrossRef]
- Than, N.; Schmidt, D.; Hodson, J.; Wawman, R.; Burak, K.; Botter, M.; Jones, R.; Montano-Loza, A.; Gautam, N.; Appanna, G.; et al. Rituximab treatment experience in patients with complicated type 1 autoimmune hepatitis in Europe and North America. J. Hepatol. 2018, 68, S217–S218. [Google Scholar] [CrossRef]
- Béland, K.; Marceau, G.; Labardy, A.; Bourbonnais, S.; Alvarez, F. Depletion of B cells induces remission of autoimmune hepatitis in mice through reduced antigen presentation and help to T cells. Hepatology 2015, 62, 1511–1523. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; Muñoz, S.; Soria, N.; Galiana, D.; Bertolaccini, L.; Cuadrado, M.-J.; Khamashta, M.A. Autoimmune diseases induced by TNF-targeted therapies: Analysis of 233 cases. Medicine 2007, 86, 242–251. [Google Scholar] [CrossRef]
- Hsu, M.C.; Liu, S.H.; Wang, C.W.; Hu, N.Y.; Wu, E.S.; Shih, Y.C.; Chiu, P.J. JKB-122 is effective, alone or in combination with prednisolone in Con A-induced hepatitis. Eur. J. Pharmacol. 2017, 812, 113–120. [Google Scholar] [CrossRef]
- Doycheva, I.; Watt, K.D.; Gulamhusein, A.F. Autoimmune hepatitis: Current and future therapeutic options. Liver Int. 2019, 39, 1002–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, L.G.; Sutherland, A.P.; Newton, R.; Qian, F.; Cachero, T.G.; Scott, M.L.; Thompson, J.S.; Wheway, J.; Chtanova, T.; Groom, J.; et al. B cell-activating factor be-longing to the TNF family (BAFF)-R is the principal BAFF receptor facilitating BAFF costimulation of circulating T and B cells. J. Immunol. 2004, 173, 807–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migita, K.; Abiru, S.; Maeda, Y.; Nakamura, M.; Komori, A.; Ito, M.; Fujiwara, S.; Yano, K.; Yatsuhashi, H.; Eguchi, K.; et al. Elevated serum BAFF levels in patients with autoimmune hepatitis. Hum. Immunol. 2007, 68, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Jeffery, H.C.; Hunter, S.; Bhogal, R.; Birtwistle, J.; Braitch, M.K.; Roberts, S.; Ming, M.; Hannah, J.; Thomas, C.; et al. Human intrahepatic regulatory T cells are functional, require IL-2 from effector cells for survival, and are susceptible to Fas ligand-mediated apoptosis. Hepatology 2016, 64, 138–150. [Google Scholar] [CrossRef] [Green Version]
- Vignali, D.A.; Collison, L.W.; Workman, C.J. How regulatory T cells work. Nat. Rev. Immunol. 2008, 8, 523–532. [Google Scholar] [CrossRef] [Green Version]
- Abramovitch, S.; Dahan-Bachar, L.; Sharvit, E.; Weisman, Y.; Tov, A.B.; Brazowski, E.; Reif, S. Vitamin D inhibits proliferation and profibrotic marker expression in hepatic stellate cells and decreases thioacetamide-induced liver fibrosis in rats. Gut 2011, 60, 1728–1737. [Google Scholar] [CrossRef]
- Potter, J.J.; Liu, X.; Koteish, A.; Mezey, E. 1,25-dihydroxyvitamin D3 and its nuclear receptor repress human alpha1 (I) collagen expres- sion and type I collagen formation. Liver Int. 2013, 33, 677–686. [Google Scholar] [CrossRef] [Green Version]
- Efe, C.; Kav, T.; Aydin, C.; Cengiz, M.; Imga, N.N.; Purnak, T.; Smyk, D.S.; Torgutalp, M.; Turhan, T.; Ozenirler, S.; et al. Low serum vitamin D levels are associated with severe histological features and poor response to therapy in patients with autoimmune hepatitis. Dig. Dis. Sci. 2014, 59, 3035–3042. [Google Scholar] [CrossRef]
- Bjelakovic, M.; Nikolova, D.; Bjelakovic, G.; Gluud, C. Vitamin D supplementation for chronic liver diseases in adults. Cochrane Database Syst. Rev. 2021, 8, CD011564. [Google Scholar]
- Moriya, K.; Nishimura, N.; Namisaki, T.; Takaya, H.; Sawada, Y.; Kawaratani, H.; Kaji, K.; Shimozato, N.; Sato, S.; Furukawa, M.; et al. Zinc Administration and Improved Serum Markers of Hepatic Fibrosis in Patients with Autoimmune Hepatitis. J. Clin. Med. 2021, 10, 2465. [Google Scholar] [CrossRef] [PubMed]
- Diglio, D.C.; Fernandes, S.A.; Stein, J.; Azeredo-da-Silva, A.; de Mattos, A.A.; Tovo, C.V. Role of zinc supplementation in the management of chronic liver diseases: A systematic review and meta-analysis. Ann. Hepatol. 2021, 19, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Gelow, K.; Chalasani, S.; Green, K.; Lammert, C. Utilization and Impact of Complementary and Alternative Medicines in Symptomatic Autoimmune Hepatitis Patients. Dig. Dis. Sci. 2022, 67, 2891–2898. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Li, Y.; Yan, L.; Sun, C.; Miao, Q.; Wang, Q.; Xiao, X.; Lian, M.; Li, B.; Chen, Y.; et al. Alterations of gut microbiome in autoimmune hepatitis. Gut 2020, 69, 569–577. [Google Scholar] [CrossRef]
- Liwinski, T.; Casar, C.; Ruehlemann, M.C.; Bang, C.; Sebode, M.; Hohenester, S.; Denk, G.; Lieb, W.; Lohse, A.W.; Franke, A.; et al. A disease-specific decline of the relative abundance of Bifidobacterium in patients with autoimmune hepatitis. Aliment. Pharm. Ther. 2020, 51, 1417–1428. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, M.; Liu, X.; Zhong, W.; Li, Y.; Ran, Y.; Guo, L.; Chen, X.; Zhao, J.; Wang, B.; et al. Bifidobacterium animalis ssp. Lactis 420 mitigates autoimmune hepatitis through regulating intestinal barrier and liver immune cells. Front. Immunol. 2020, 11, 569104. [Google Scholar] [CrossRef]
- Liu, Q.; Tian, H.; Kang, Y.; Tian, Y.; Li, L.; Kang, X.; Yang, H.; Wang, Y.; Tian, J.; Zhang, F.; et al. Probiotics alleviate autoimmune hepatitis in mice through modulation of gut microbiota and intestinal permeability. J. Nutr. Biochem. 2021, 98, 108863. [Google Scholar] [CrossRef]
- Wu, J.L.; Zou, J.Y.; Hu, E.D.; Chen, D.Z.; Chen, L.; Lu, F.B.; Xu, L.-M.; Zheng, M.-H.; Li, H.; Huang, Y.; et al. Sodium butyrate ameliorates S100/FCA-induced autoimmune hepatitis through regulation of intestinal tight junction and toll-like receptor 4 signaling pathway. Immunol. Lett. 2017, 190, 169–176. [Google Scholar] [CrossRef]
- Ke, Q.H.; Chen, H.Y.; He, Z.L.; Lv, Z.; Xu, X.F.; Qian, Y.G.; Zheng, S.S. Silencing of microRNA-375 affects immune function in mice with liver failure by upregulating astrocyte elevated gene-1 through reducing apoptosis of Kupffer cells. J. Cell. Biochem. 2019, 120, 253–263. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Q.; Lan, Y.Y.; Guo, Y.C.; Yuan, Q.W.; Liu, P. Down-regulation of microRNA-138 improves immunologic function via negatively targeting p53 by regulating liver macrophage in mice with acute liver failure. Biosci. Rep. 2019, 39, BSR20190763. [Google Scholar] [CrossRef]
- Tu, H.; Chen, D.; Cai, C.; Du, Q.; Lin, H.; Pan, T.; Sheng, L.; Xu, Y.; Teng, T.; Tu, J.; et al. MicroRNA-143-3p attenuated development of hepatic fibrosis in autoimmune hepatitis through regulation of TAK1 phosphorylation. J. Cell Mol. Med. 2020, 24, 1256–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, T.; Qiu, X.; Liu, H.; Gan, C.; Tan, Z.; Xie, Y.; Wang, Y.; Ye, T. Epigenetic regulation in fibrosis progress. Pharmacol. Res. 2021, 173, 105910. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| General Method | Specific Procedures |
|---|---|
| Liver biopsy | - |
| Serum biomarkers | TGF-β Angiotensin-converting enzyme (ACE) |
| Scoring systems | FibroTest Aspartate Amino-Transferase/platelet Ratio Index (APRI) Fibrosis-4 Index (FIB-4) Red cell distribution width to Plateled Ratio (RPR) |
| Radiological procedures | Conventional ultrasound Elastography Magnetic resonance elastography (MRE) Magnetic resonance spectroscopy (MRS) Computed tomography (CT) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellicano, R.; Ferro, A.; Cicerchia, F.; Mattivi, S.; Fagoonee, S.; Durazzo, M. Autoimmune Hepatitis and Fibrosis. J. Clin. Med. 2023, 12, 1979. https://doi.org/10.3390/jcm12051979
Pellicano R, Ferro A, Cicerchia F, Mattivi S, Fagoonee S, Durazzo M. Autoimmune Hepatitis and Fibrosis. Journal of Clinical Medicine. 2023; 12(5):1979. https://doi.org/10.3390/jcm12051979
Chicago/Turabian StylePellicano, Rinaldo, Arianna Ferro, Francesca Cicerchia, Simone Mattivi, Sharmila Fagoonee, and Marilena Durazzo. 2023. "Autoimmune Hepatitis and Fibrosis" Journal of Clinical Medicine 12, no. 5: 1979. https://doi.org/10.3390/jcm12051979