
Evaluating Prescription Pattern and Effectiveness of Antihypertensive Drugs in Non-Operated Aortic Dissection Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
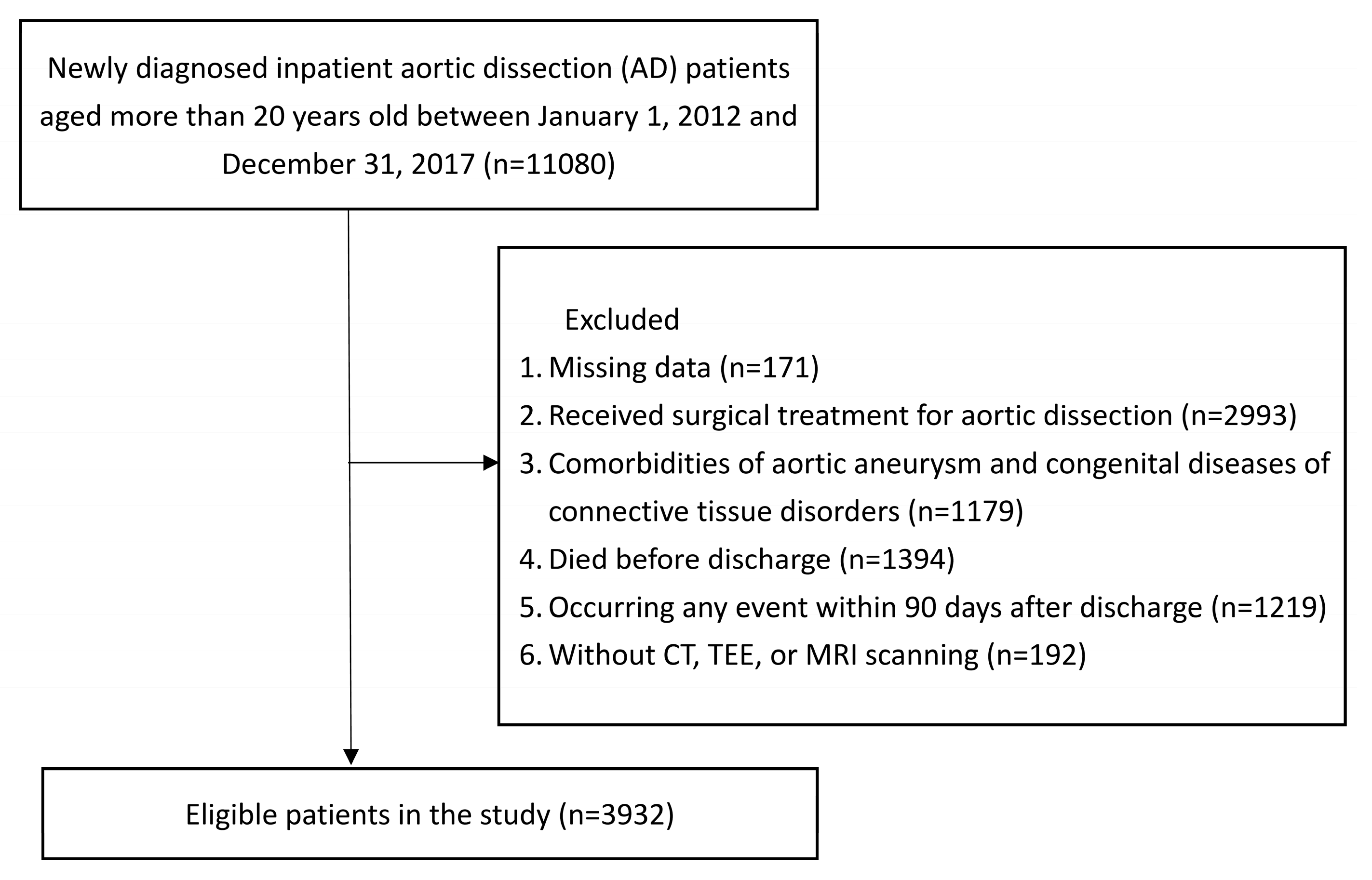
2.2. Study Population
2.3. Drug Use and Prescription Pattern
2.4. Outcomes
2.5. Characteristics
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nienaber, C.A.; Clough, R.E.; Sakalihasan, N.; Suzuki, T.; Gibbs, R.; Mussa, F.; Jenkins, M.P.; Thompson, M.M.; Evangelista, A.; Yeh, J.S.M.; et al. Aortic dissection. Nat. Rev. Dis. Prim. 2016, 2, 16053. [Google Scholar] [CrossRef] [PubMed]
- Riambau, V.; Böckler, D.; Brunkwall, J.; Cao, P.; Chiesa, R.; Coppi, G.; Czerny, M.; Fraedrich, G.; Haulon, S.; Jacobs, M.J.; et al. Editor’s Choice-Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 4–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evangelista, A.; Isselbacher, E.M.; Bossone, E.; Gleason, T.G.; DI Eusanio, M.; Sechtem, U.; Ehrlich, M.P.; Trimarchi, S.; Braverman, A.C.; Myrmel, T.; et al. Insights From the International Registry of Acute Aortic Dissection. Circulation 2018, 137, 1846–1860. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.-Y.; Chen, Y.-S.; Huang, S.-C.; Wang, S.-S.; Lin, F.-Y. Late outcome of patients with aortic dissection: Study of a national database. Eur. J. Cardiothorac. Surg. 2004, 25, 683–690. [Google Scholar] [CrossRef]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E., Jr.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar]
- Bossone, E.; LaBounty, T.M.; Eagle, K.A. Acute aortic syndromes: Diagnosis and management, an update. Eur. Heart J. 2018, 39, 739–749. [Google Scholar] [CrossRef] [Green Version]
- JCS Joint Working Group. Guidelines for diagnosis and treatment of aortic aneurysm and aortic dissection (JCS 2011): Digest version. Circ. J. 2013, 77, 789–828. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.-Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.-C. Data resource profile: The National Health Insurance Research Database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef]
- Yeh, T.Y.; Chen, C.Y.; Huang, J.W.; Chiu, C.C.; Lai, W.T.; Huang, Y.B. Epidemiology and Medication Utilization Pattern of Aortic Dissection in Taiwan: A Population-Based Study. Medicine 2015, 94, e1522. [Google Scholar] [CrossRef]
- Health Promotion Administration, Ministry of Health and Welfare. Statistics of Health Promoation 2013. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=268&pid=5199 (accessed on 3 January 2017).
- Health Promotion Administration, Ministry of Health and Welfare. Statistics of Health Promoation 2018. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=268&pid=12886&sid=5199 (accessed on 29 June 2020).
- Liao, K.-M.; Chen, C.-Y.; Wang, S.-H.; Huang, J.-W.; Kuo, C.-C.; Huang, Y.-B. A Retrospective Observational Study to Assess Prescription Pattern in Patients with Type B Aortic Dissection and Treatment Outcome. Biomed. Res. Int. 2016, 2016, 5173898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.; Lin, H.; Wang, T.; Chen, C. Asian management of hypertension: Current status, home blood pressure, and specific concerns in Taiwan. J. Clin. Hypertens. 2020, 22, 511–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genoni, M.; Paul, M.; Jenni, R.; Graves, K.; Seifert, B.; Turina, M. Chronic beta-blocker therapy improves outcome and reduces treatment costs in chronic type B aortic dissection. Eur. J. Cardiothorac. Surg. 2001, 19, 606–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zierer, A.; Voeller, R.K.; Hill, K.E.; Kouchoukos, N.T.; Damiano, R.J.; Moon, M.R. Aortic enlargement and late reoperation after repair of acute type A aortic dissection. Ann. Thorac. Surg. 2007, 84, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Leach, S.D.; Toole, A.L.; Stern, H.; DeNatale, R.W.; Tilson, M.D. Effect of beta-adrenergic blockade on the growth rate of abdominal aortic aneurysms. Arch. Surg. 1988, 123, 606–609. [Google Scholar] [CrossRef]
- Shores, J.; Berger, K.R.; Murphy, E.A.; Pyeritz, R.E. Progression of aortic dilatation and the benefit of long-term beta-adrenergic blockade in Marfan’s syndrome. N. Engl. J. Med. 1994, 330, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Isselbacher, E.M.; Nienaber, C.A.; Pyeritz, R.E.; Eagle, K.A.; Tsai, T.T.; Cooper, J.V.; Januzzi, J.L.; Braverman, A.C.; Montgomery, D.G.; et al. Type-selective benefits of medications in treatment of acute aortic dissection (from the International Registry of Acute Aortic Dissection [IRAD]). Am. J. Cardiol. 2012, 109, 122–127. [Google Scholar] [CrossRef]
- Yetman, A.T.; Bornemeier, R.A.; McCrindle, B.W. Usefulness of enalapril versus propranolol or atenolol for prevention of aortic dilation in patients with the Marfan syndrome. Am. J. Cardiol. 2005, 95, 1125–1127. [Google Scholar] [CrossRef]
- Habashi, J.P.; Doyle, J.J.; Holm, T.M.; Aziz, H.; Schoenhoff, F.; Bedja, D.; Chen, Y.; Modiri, A.N.; Judge, D.P.; Dietz, H.C. Angiotensin II type 2 receptor signaling attenuates aortic aneurysm in mice through ERK antagonism. Science 2011, 332, 361–365. [Google Scholar] [CrossRef]
- Brooke, B.S.; Habashi, J.P.; Judge, D.P.; Patel, N.; Loeys, B.; Dietz, H.C., III. Angiotensin II blockade and aortic-root dilation in Marfan’s syndrome. N. Engl. J. Med. 2008, 358, 2787–2795. [Google Scholar] [CrossRef] [Green Version]
- Groenink, M.; den Hartog, A.W.; Franken, R.; Radonic, T.; de Waard, V.; Timmermans, J.; Scholte, A.J.; Berg, M.P.V.D.; Spijkerboer, A.M.; Marquering, H.A.; et al. Losartan reduces aortic dilatation rate in adults with Marfan syndrome: A randomized controlled trial. Eur. Heart J. 2013, 34, 3491–3500. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-W.; Chan, Y.-H.; Lin, C.-P.; Wu, V.C.-C.; Cheng, Y.-T.; Chen, D.-Y.; Chang, S.-H.; Hung, K.-C.; Chu, P.-H.; Chou, A.-H. Association of Long-term Use of Antihypertensive Medications. JAMA Netw. Open 2021, 4, e210469. [Google Scholar] [CrossRef]
- Tomita, N.; Yamasaki, K.; Izawa, K.; Kunugiza, Y.; Osako, M.K.; Ogihara, T.; Morishita, R. Inhibition of experimental abdominal aortic aneurysm progression by nifedipine. Int. J. Mol. Med. 2008, 21, 239–244. [Google Scholar] [CrossRef]
- Yokokura, H.; Hiromatsu, S.; Akashi, H.; Kato, S.; Aoyagi, S. Effects of calcium channel blocker azelnidipine on experimental abdominal aortic aneurysms. Surg. Today 2007, 37, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Wilmink, A.B.; Katerina, A.; Day, N.E.; Ashton, H.A.; Scott, A.P.; Quick, C.R. Are antihypertensive drugs associated with abdominal aortic aneurysms? J. Vasc. Surg. 2002, 36, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, K.; Kubo, N.; Ako, J.; Fujiwara, N.; Funayama, H.; Ikeda, N.; Nakamura, T.; Sugawara, Y.; Yasu, T.; Kawakami, M.; et al. Determinants of long-term mortality in patients with type B acute aortic dissection. Am. J. Hypertens. 2009, 22, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Overall (n = 3932) | Group 0 (n = 424) | Group 1 (n = 676) | Group 2 (n = 1035) | Group 3 (n = 1100) | Group 4 (n = 697) |
|---|---|---|---|---|---|---|
| Age, mean, year (SD) | 66.81 (14.82) | 68.28 (16.55) | 72.81 (13.87) | 69.74 (13.48) | 64.55 (14.12) | 59.33 (13.79) |
| Sex, N (%) | ||||||
| Male | 2803 (71.29) | 302 (71.23) | 453 (67.01) | 694 (67.05) | 811 (73.73) | 543 (77.91) |
| Female | 1129 (28.71) | 122 (28.77) | 223 (32.99) | 341 (32.95) | 289 (26.27) | 154 (22.09) |
| Geographic area, N (%) | ||||||
| North | 1737 (44.18) | 176 (41.51) | 297 (43.93) | 462 (44.64) | 480 (43.64) | 322 (46.2) |
| Middle | 695 (17.68) | 85 (20.05) | 133 (19.67) | 171 (16.52) | 180 (16.36) | 126 (18.08) |
| South | 1391 (35.38) | 150 (35.38) | 232 (34.32) | 367 (35.46) | 410 (37.27) | 232 (33.29) |
| East | 109 (2.77) | 13 (3.07) | 14 (2.07) | 35 (3.38) | 30 (2.73) | 17 (2.44) |
| Urbanization, N (%) | ||||||
| Urban | 1866 (47.46) | 203 (47.88) | 304 (44.97) | 495 (47.83) | 514 (46.73) | 350 (50.22) |
| Suburban | 1636 (41.61) | 177 (41.75) | 289 (42.75) | 428 (41.35) | 466 (42.36) | 276 (39.6) |
| Rural | 430 (10.94) | 44 (10.38) | 83 (12.28) | 112 (10.82) | 120 (10.91) | 71 (10.19) |
| Insurance premium, N (%) | ||||||
| ≤22,800 TWDs | 2730 (69.43) | 316 (74.53) | 510 (75.44) | 719 (69.47) | 735 (66.82) | 450 (64.56) |
| >22,800 TWDs | 1202 (30.57) | 108 (25.47) | 166 (24.56) | 316 (30.53) | 365 (33.18) | 247 (35.44) |
| Comedication, N (%) | ||||||
| Antiplatelet | 867 (22.05) | 96 (22.64) | 186 (27.51) | 258 (24.93) | 225 (20.45) | 102 (14.63) |
| Anticoagulant | 158 (4.02) | 19 (4.48) | 36 (5.33) | 43 (4.15) | 46 (4.18) | 14 (2.01) |
| Antidiabetic agent | 592 (15.06) | 63 (14.86) | 117 (17.31) | 158 (15.27) | 156 (14.18) | 98 (14.06) |
| Statin | 569 (14.47) | 37 (8.73) | 97 (14.35) | 162 (15.65) | 171 (15.55) | 102 (14.63) |
| Comorbidity, N (%) | ||||||
| Hypertension | 3344 (85.05) | 222 (52.36) | 538 (79.59) | 930 (89.86) | 996 (90.55) | 658 (94.4) |
| Hyperlipidemia | 861 (21.90) | 64 (15.09) | 167 (24.7) | 263 (25.41) | 229 (20.82) | 138 (19.8) |
| Diabetes mellitus | 702 (17.85) | 75 (17.69) | 150 (22.19) | 185 (17.87) | 181 (16.45) | 111 (15.93) |
| Heart failure | 407 (10.35) | 39 (9.2) | 96 (14.2) | 107 (10.34) | 113 (10.27) | 52 (7.46) |
| Atrial fibrillation | 253 (6.43) | 17 (4.01) | 55 (8.14) | 65 (6.28) | 85 (7.73) | 31 (4.45) |
| Coronary artery disease | 993 (25.25) | 87 (20.52) | 222 (32.84) | 293 (28.31) | 265 (24.09) | 126 (18.08) |
| Cerebrovascular disease | 670 (17.04) | 94 (22.17) | 163 (24.11) | 191 (18.45) | 155 (14.09) | 67 (9.61) |
| Chronic kidney disease | 530 (13.48) | 48 (11.32) | 122 (18.05) | 154 (14.88) | 126 (11.45) | 80 (11.48) |
| Chronic obstructive pulmonary disease | 456 (11.60) | 71 (16.75) | 111 (16.42) | 128 (12.37) | 107 (9.73) | 39 (5.6) |
| Charlson comorbidity index score, mean (SD) | 2.38 (1.68) | 2.68 (1.76) | 2.91 (1.83) | 2.46 (1.68) | 2.16 (1.58) | 1.93 (1.42) |
| Location of AD, N (%) | ||||||
| UAD | 666 (16.94) | - | - | - | - | - |
| TAD | 1242 (31.59) | - | - | - | - | - |
| AAD | 537 (13.66) | - | - | - | - | - |
| TAAD | 1487 (37.82) | - | - | - | - | - |
| Variables | Overall (n = 3932) |
|---|---|
| Categories of antihypertensive drugs, N (%) | |
| β-blocker | 2456 (62.46) |
| CCB | 2587 (65.79) |
| ACEI | 174 (4.43) |
| ARB | 2061 (52.42) |
| Renin-inhibitor | 9 (0.23) |
| Diuretic | 1062 (27.01) |
| Vasodilator | 193 (4.91) |
| Centrally α2-agonist | 41 (1.04) |
| α-blocker | 664 (16.89) |
| Reserpine, Rauwolfia serpentine, guanethidine | 8 (0.20) |
| Prescription patterns, N (%), stratified by classes | |
| Group 0 | 424 (10.78) |
| Group 1 | 676 (17.19) |
| β-blocker | 244 (6.21) |
| CCB | 219 (5.57) |
| RAS | 107 (2.72) |
| Others | 106 (2.70) |
| Group 2 | 1035 (26.32) |
| β-blocker + CCB | 357 (9.08) |
| β-blocker + RAS | 180 (4.58) |
| β-blocker + Others | 88 (2.24) |
| CCB + RAS | 246 (6.26) |
| CCB + Others | 91 (2.31) |
| RAS + Others | 73 (1.86) |
| Group 3 | 1100 (27.98) |
| β-blocker + CCB + RAS | 588 (14.95) |
| β-blocker + CCB + Others | 179 (4.55) |
| β-blocker + RAS + Others | 123 (3.13) |
| CCB + RAS + Others | 210 (5.34) |
| Group 4 | 697 (17.73) |
| β-blocker + CCB + RAS + Others | 697 (17.73) |
| N | Events | PY | Rate (%) a | Crude HR (95% CI) | p Value | Adjusted HR b (95% CI) | p Value | |
|---|---|---|---|---|---|---|---|---|
| Group 1 | ||||||||
| β-blocker | 244 | 100 | 888 | 11.26 | 0.48 (0.35–0.66) | <0.001 * | 0.74 (0.53–1.03) | 0.074 |
| CCB | 219 | 110 | 741 | 14.84 | 0.64 (0.47–0.86) | 0.004 * | 0.72 (0.53–0.99) | 0.043 |
| RAS | 107 | 47 | 402 | 11.70 | 0.51 (0.35–0.73) | <0.001 * | 0.58 (0.39–0.84) | 0.005 * |
| Others | 106 | 68 | 290 | 23.46 | 1 (reference) | 1 (reference) | ||
| Group 2 | ||||||||
| β-blocker + CCB | 357 | 125 | 1452 | 8.61 | 0.42 (0.30–0.58) | <0.001 * | 0.60 (0.42–0.85) | 0.004 * |
| β-blocker + Others | 88 | 43 | 310 | 13.87 | 0.67 (0.44–1.01) | 0.057 | 0.69 (0.46–1.05) | 0.086 |
| β-blocker + RAS | 180 | 69 | 672 | 10.27 | 0.49 (0.34–0.72) | <0.001 * | 0.70 (0.48–1.02) | 0.066 |
| CCB + Others | 91 | 59 | 296 | 19.92 | 0.96 (0.65–1.40) | 0.814 | 1.11 (0.75–1.64) | 0.617 |
| CCB + RAS | 246 | 92 | 949 | 9.69 | 0.47 (0.33–0.66) | <0.001 * | 0.60 (0.41–0.86) | 0.006* |
| RAS + Others | 73 | 46 | 219 | 21.02 | 1 (reference) | 1 (reference) | ||
| Group 3 | ||||||||
| β-blocker + CCB + Others | 179 | 74 | 728 | 10.16 | 0.93 (0.68–1.26) | 0.634 | 1.07 (0.77–1.47) | 0.701 |
| β-blocker + CCB + RAS | 588 | 182 | 2343 | 7.77 | 0.71 (0.55–0.91) | 0.008 * | 1.01 (0.77–1.32) | 0.942 |
| β-blocker + RAS + Others | 123 | 52 | 446 | 11.66 | 1.06 (0.76–1.5) | 0.729 | 1.23 (0.86–1.74) | 0.258 |
| CCB + RAS + Others | 210 | 89 | 811 | 10.97 | 1 (reference) | 1 (reference) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-H.; Chiu, K.-L.; Shen, C.-W.; Bair, M.-J.; Chen, C.-Y. Evaluating Prescription Pattern and Effectiveness of Antihypertensive Drugs in Non-Operated Aortic Dissection Patients. J. Clin. Med. 2023, 12, 1962. https://doi.org/10.3390/jcm12051962
Huang Y-H, Chiu K-L, Shen C-W, Bair M-J, Chen C-Y. Evaluating Prescription Pattern and Effectiveness of Antihypertensive Drugs in Non-Operated Aortic Dissection Patients. Journal of Clinical Medicine. 2023; 12(5):1962. https://doi.org/10.3390/jcm12051962
Chicago/Turabian StyleHuang, Yun-Hui, Kai-Lin Chiu, Chuan-Wei Shen, Ming-Jong Bair, and Chung-Yu Chen. 2023. "Evaluating Prescription Pattern and Effectiveness of Antihypertensive Drugs in Non-Operated Aortic Dissection Patients" Journal of Clinical Medicine 12, no. 5: 1962. https://doi.org/10.3390/jcm12051962