
Uncemented Tibial Fixation Has Comparable Prognostic Outcomes and Safety Versus Cemented Fixation in Cruciate-Retaining Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
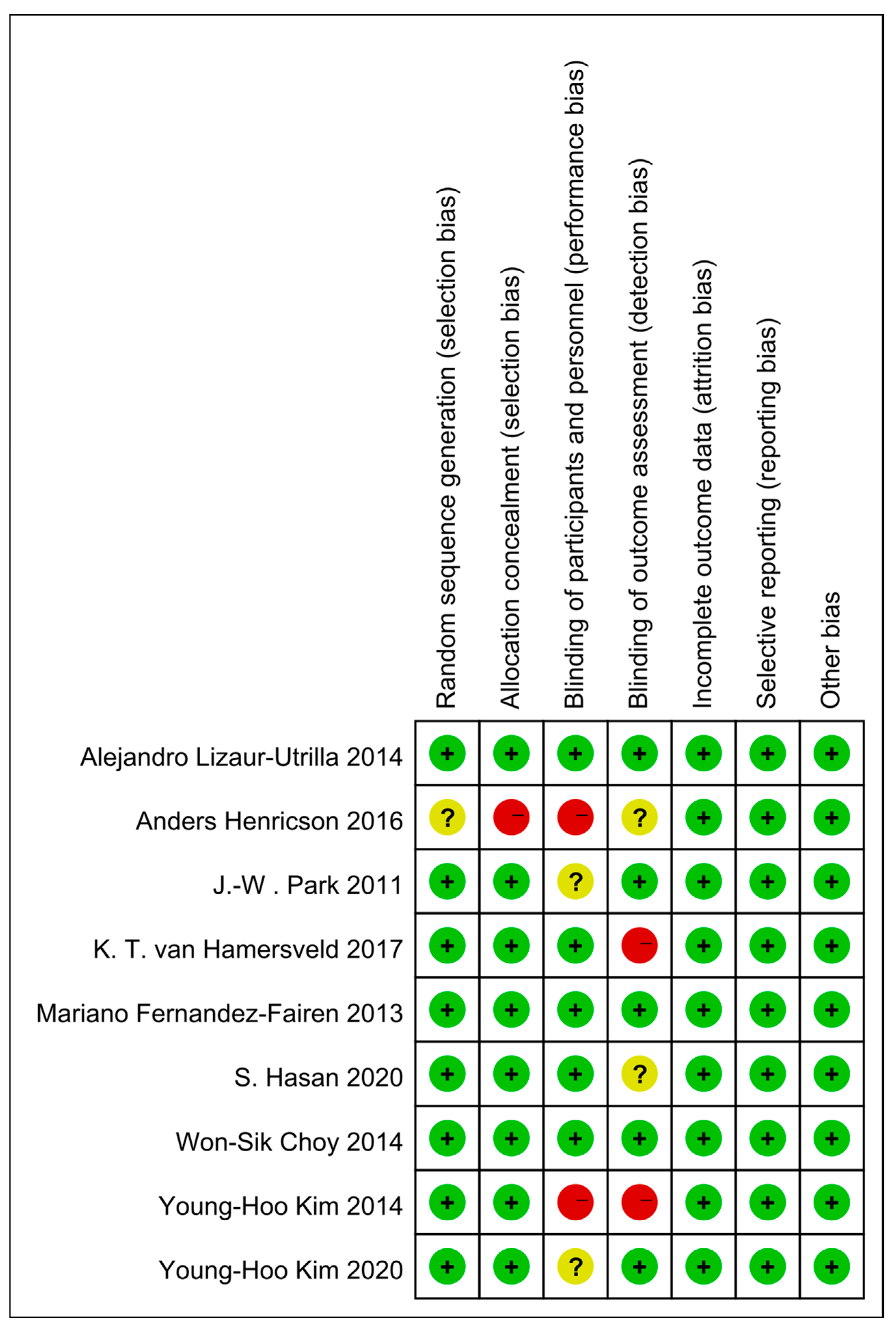
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
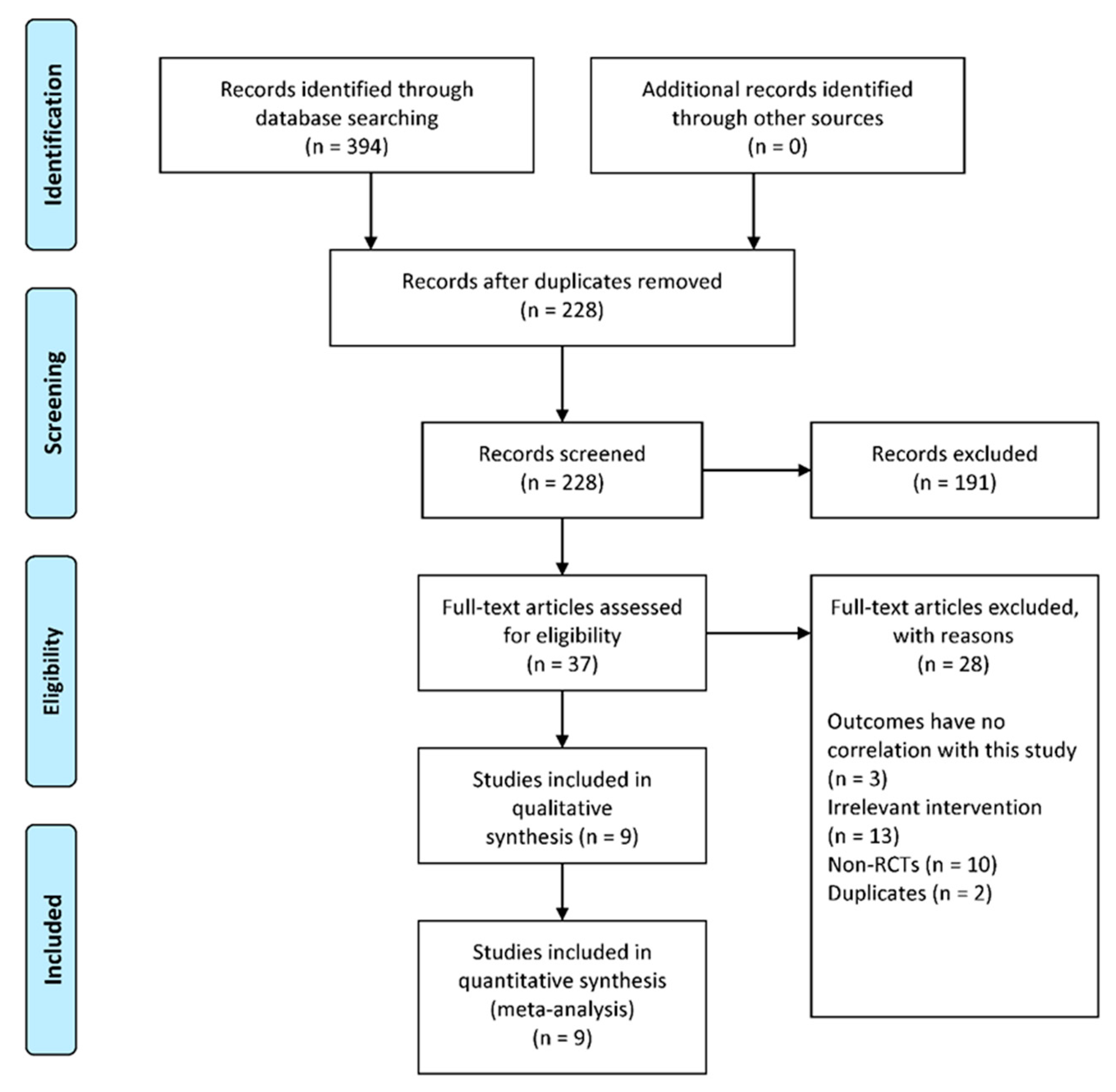
3.1. Study Identification and Characteristics
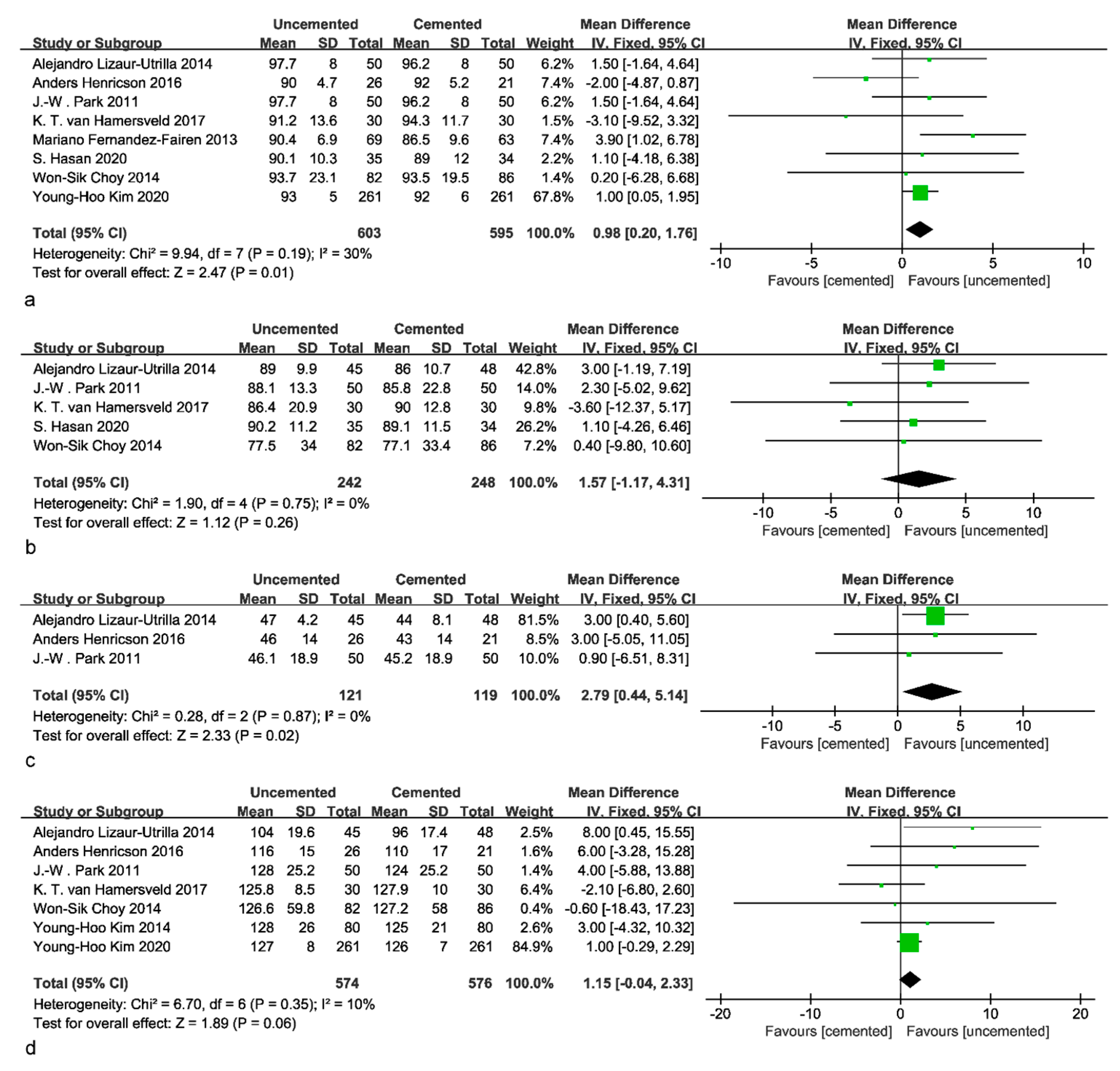
3.2. Clinical Outcomes
3.3. Radiological Outcomes
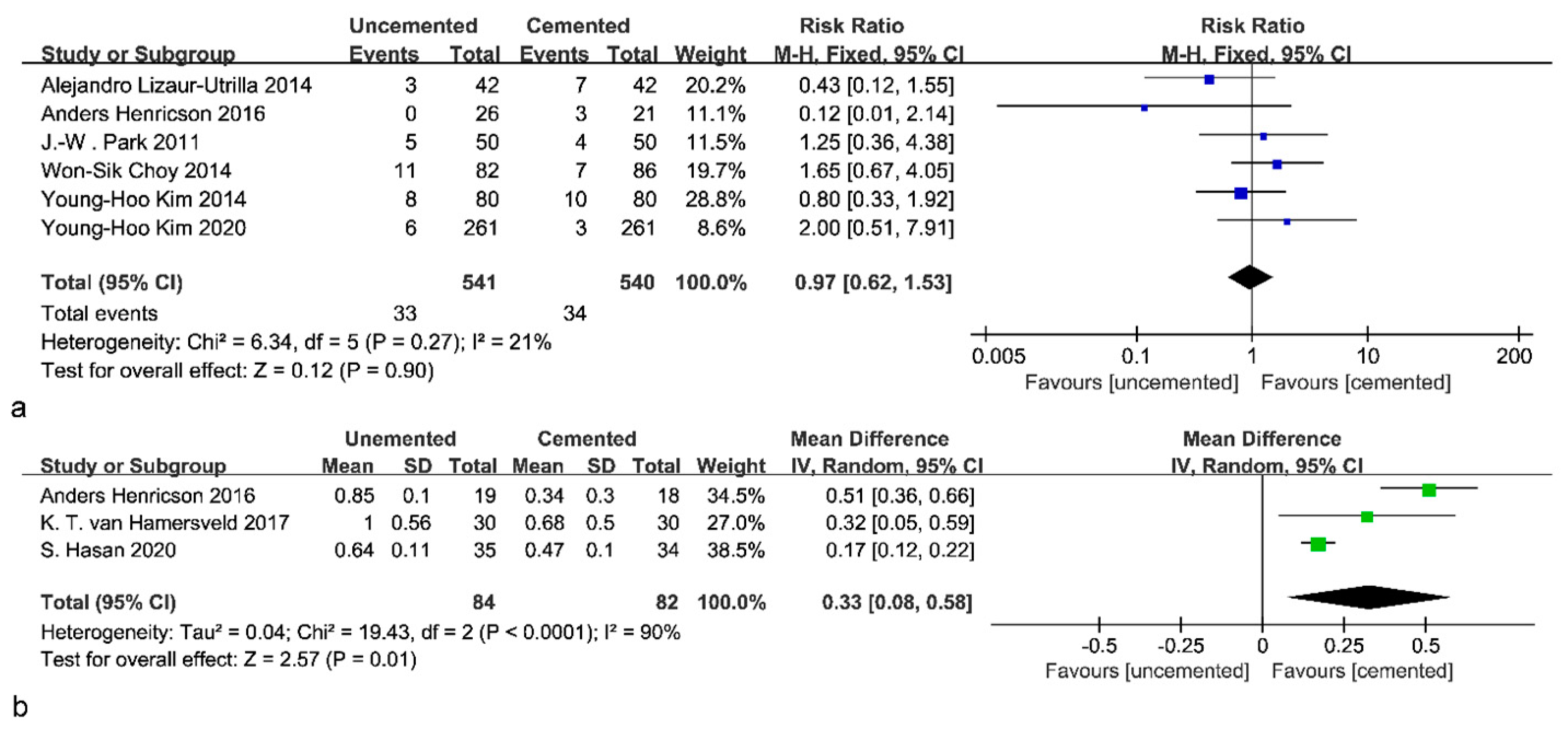
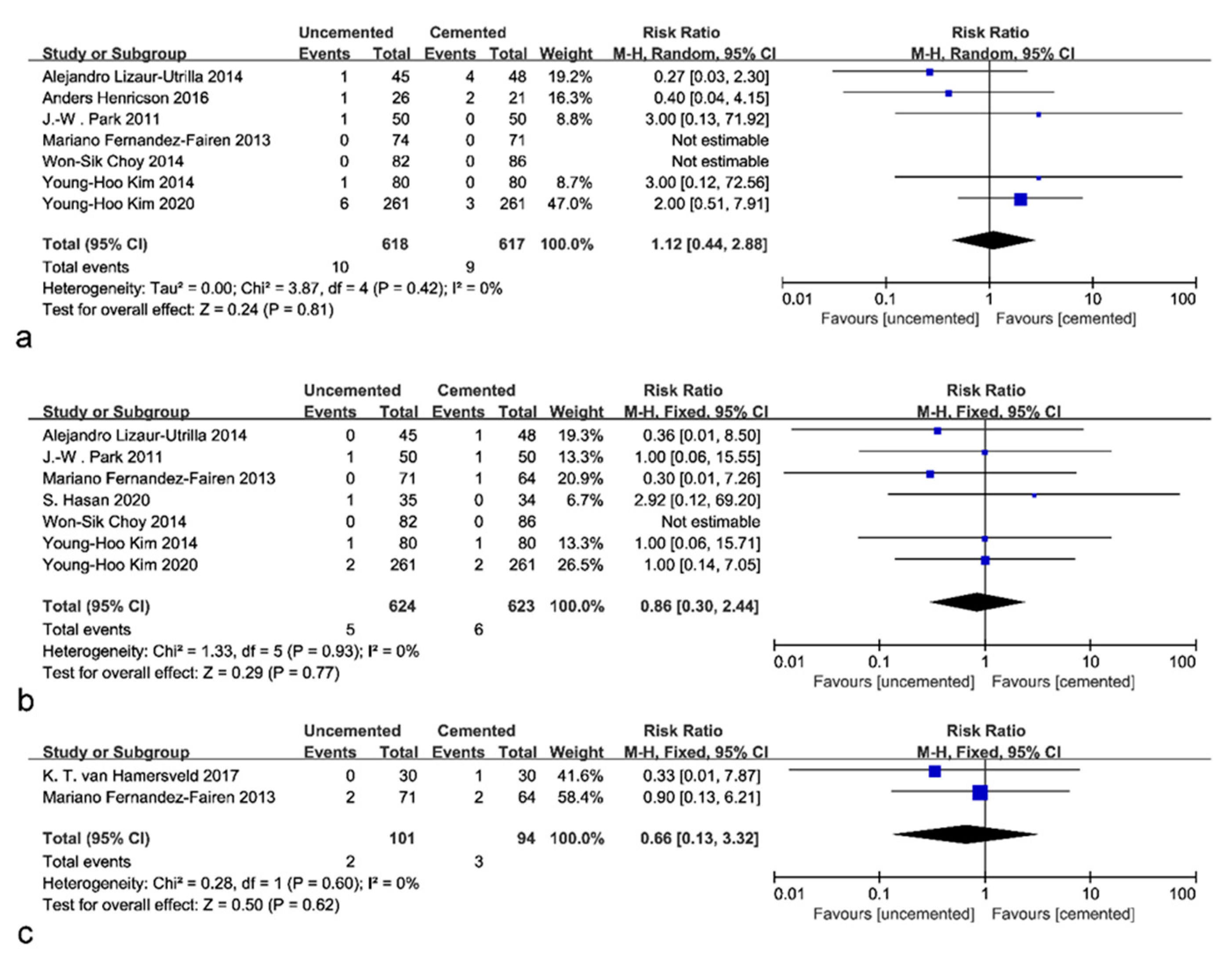
3.4. Complications
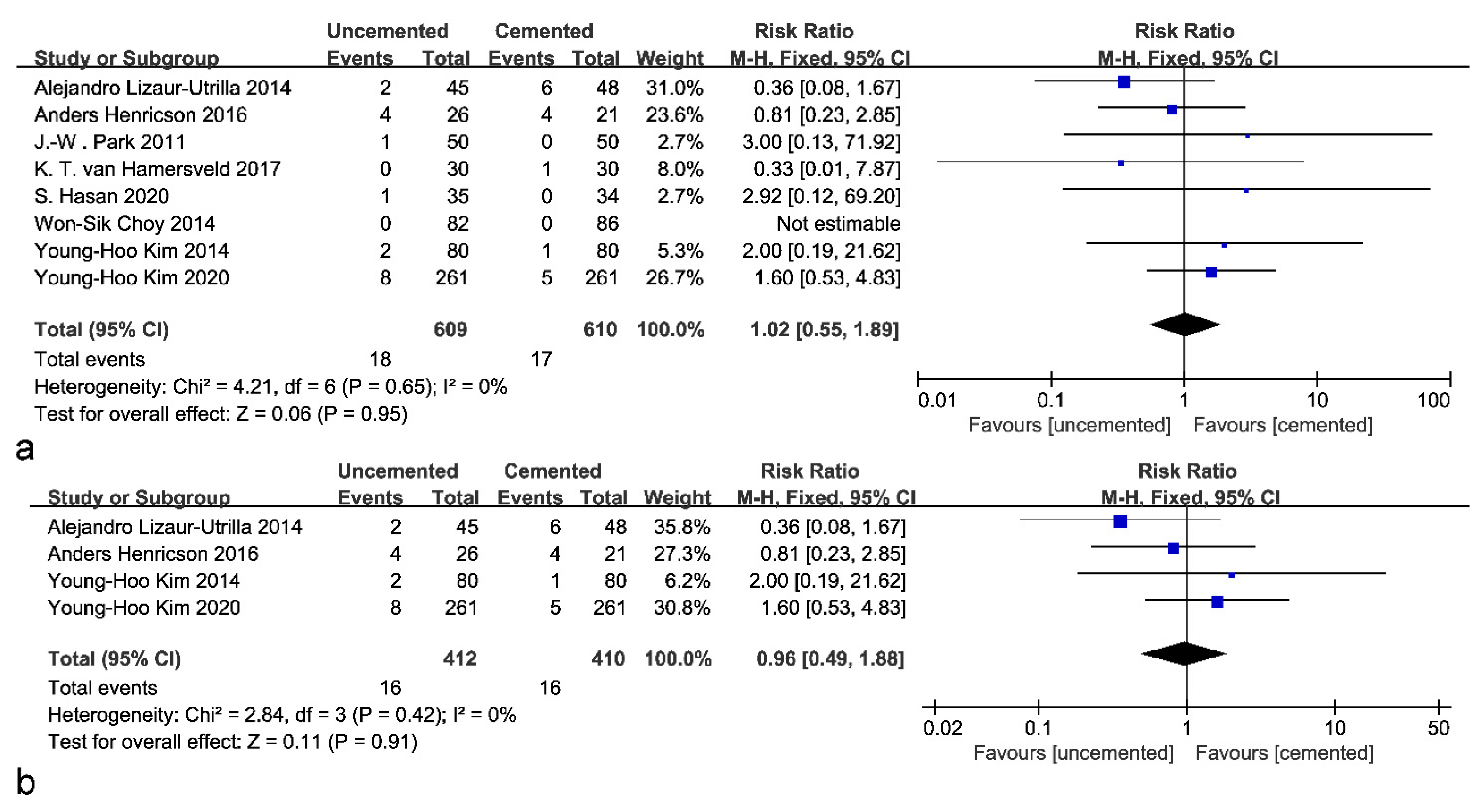
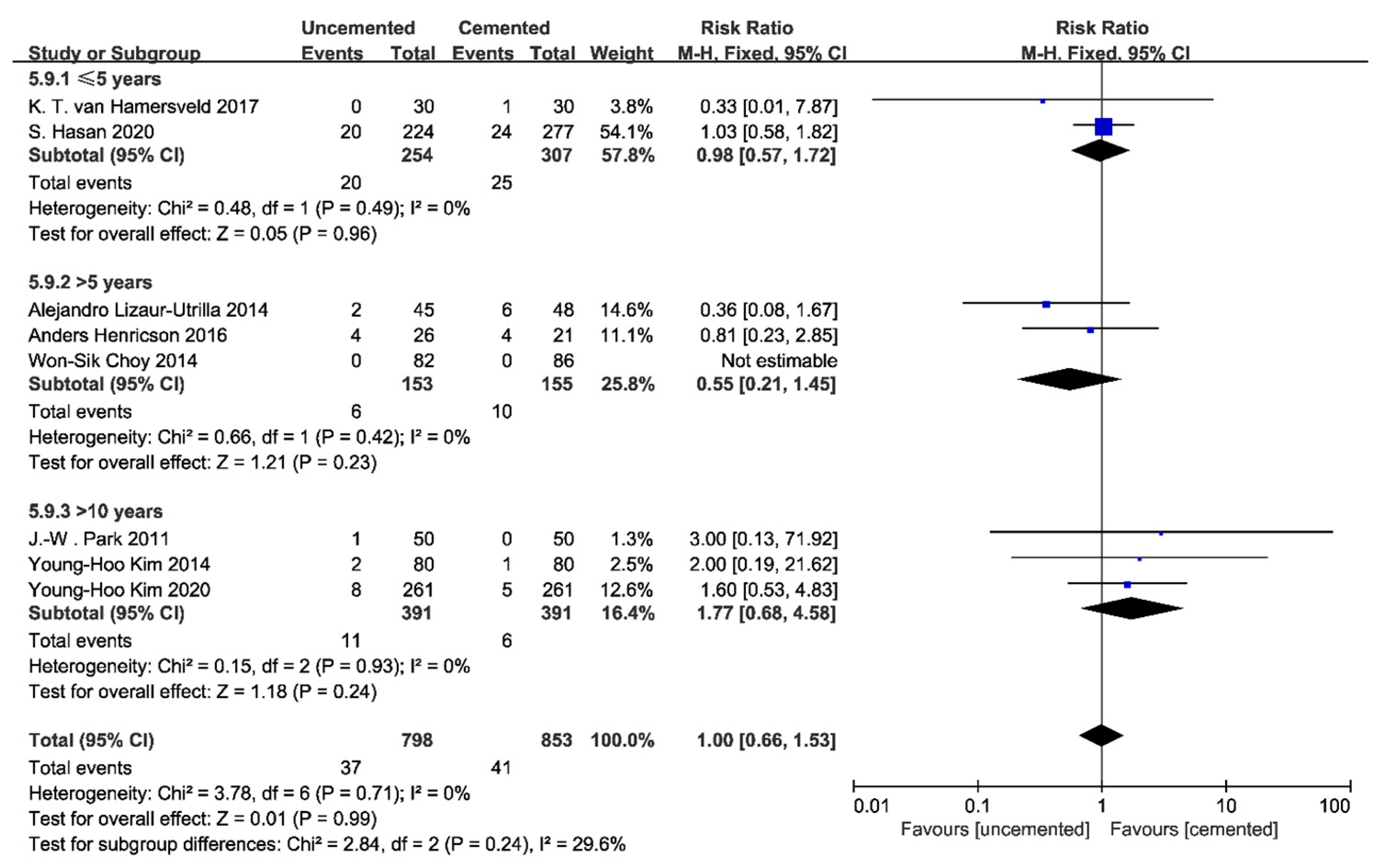
3.5. Revisions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Price, A.J.; Alvand, A.; Troelsen, A.; Katz, J.N.; Hooper, G.; Gray, A.; Carr, A.; Beard, D. Knee replacement. Lancet 2018, 392, 1672–1682. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, D.; Gori, D.; Desai, K.R.; Asch, S.; Carroll, I.R.; Curtin, C.; McDonald, K.M.; Fantini, M.P.; Hernandez-Boussard, T. Drug-Free Interventions to Reduce Pain or Opioid Consumption After Total Knee Arthroplasty: A Systematic Review and Meta-analysis. JAMA Surg. 2017, 152, e172872. [Google Scholar] [CrossRef] [PubMed]
- Losina, E.; Thornhill, T.S.; Rome, B.N.; Wright, J.; Katz, J.N. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J. Bone Jt. Surg. 2012, 94, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanchate, A.D.; Kapoor, A.; Katz, J.N.; McCormick, D.; Lasser, K.E.; Feng, C.; Manze, M.G.; Kressin, N.R. Massachusetts health reform and disparities in joint replacement use: Difference in differences study. BMJ 2015, 350, h440. [Google Scholar] [CrossRef] [Green Version]
- American Joint Replacement Registry (AJRR). 2020 Annual Report; American Academy of Orthopaedic Surgeons (AAOS): Rosemont, IL, USA, 2020. [Google Scholar]
- National Joint Registry. ISSN 2054-183X (Online). In 17th Annual Report 2020—National Joint Registry for England, Wales, Northern Ireland and the Isle of Man; National Joint Registry: London, UK, 2020. [Google Scholar]
- Chiu, F.Y.; Chen, C.M.; Lin, C.F.; Lo, W.H. Cefuroxime-impregnated cement in primary total knee arthroplasty: A prospective, randomized study of three hundred and forty knees. J. Bone Jt. Surg. 2002, 84, 759–762. [Google Scholar] [CrossRef]
- Naudie, D.D.; Ammeen, D.J.; Engh, G.A.; Rorabeck, C.H. Wear and osteolysis around total knee arthroplasty. J. Am. Acad. Orthop. Surg. 2007, 15, 53–64. [Google Scholar] [CrossRef]
- O'Rourke, M.R.; Callaghan, J.J.; Goetz, D.D.; Sullivan, P.M.; Johnston, R.C. Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design: Five to eight-year follow-up. J. Bone Jt. Surg. 2002, 84, 1362–1371. [Google Scholar] [CrossRef]
- Dalury, D.F. Cementless total knee arthroplasty: Current concepts review. Bone Jt. J. 2016, 98-B, 867–873. [Google Scholar] [CrossRef] [Green Version]
- Hungerford, D.S.; Krackow, K.A. Total joint arthroplasty of the knee. Clin. Orthop. Relat. Res. 1985, 192, 23–33. [Google Scholar] [CrossRef]
- Ranawat, C.S.; Johanson, N.A.; Rimnac, C.M.; Wright, T.M.; Schwartz, R.E. Retrieval analysis of porous-coated components for total knee arthroplasty. A report of two cases. Clin. Orthop. Relat. Res. 1986, 209, 244–248. [Google Scholar] [CrossRef]
- Moreland, J.R. Mechanisms of failure in total knee arthroplasty. Clin. Orthop. Relat. Res. 1988, 226, 49–64. [Google Scholar] [CrossRef]
- Collins, D.N.; Heim, S.A.; Nelson, C.L.; Smith, P., 3rd. Porous-coated anatomic total knee arthroplasty. A prospective analysis comparing cemented and cementless fixation. Clin. Orthop. Relat. Res. 1991, 267, 128–136. [Google Scholar] [CrossRef]
- Lieberman, E.G.; Barrack, R.L.; Schmalzried, T.P. Suspected Metal Allergy and Femoral Loosening After Total Knee Arthroplasty: A Diagnostic Dilemma. Arthroplast. Today 2021, 7, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Taljanovic, M.S.; Jones, M.D.; Hunter, T.B.; Benjamin, J.B.; Ruth, J.T.; Brown, A.W.; Sheppard, J.E. Joint arthroplasties and prostheses. Radiographics 2003, 23, 1295–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, D.; Lawrie, C.M.; Salih, R.; Nahhas, C.R.; Barrack, R.L.; Nunley, R.M. Cemented Versus Cementless Total Knee Arthroplasty of the Same Modern Design: A Prospective, Randomized Trial. J. Bone Jt. Surg. 2019, 101, 1185–1192. [Google Scholar] [CrossRef]
- Fricka, K.B.; McAsey, C.J.; Sritulanondha, S. To Cement or Not? Five-Year Results of a Prospective, Randomized Study Comparing Cemented vs Cementless Total Knee Arthroplasty. J. Arthroplast. 2019, 34, S183–S187. [Google Scholar] [CrossRef]
- Demey, G.; Servien, E.; Lustig, S.; Ait Si Selmi, T.; Neyret, P. Cemented versus uncemented femoral components in total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2011, 19, 1053–1059. [Google Scholar] [CrossRef]
- Brown, T.E.; Harper, B.L.; Bjorgul, K. Comparison of cemented and uncemented fixation in total knee arthroplasty. Orthopedics 2013, 36, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Schreurs, B.W.; Hannink, G. Total joint arthroplasty in younger patients: Heading for trouble? Lancet 2017, 389, 1374–1375. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Choy, W.S.; Yang, D.S.; Lee, K.W.; Lee, S.K.; Kim, K.J.; Chang, S.H. Cemented Versus Cementless Fixation of a Tibial Component in LCS Mobile-Bearing Total Knee Arthroplasty Performed by a Single Surgeon. J. Arthroplast. 2014, 29, 2397–2401. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Fairen, M.; Hernández-Vaquero, D.; Murcia, A.; Torres, A.; Llopis, R. Trabecular metal in total knee arthroplasty associated with higher knee scores: A randomized controlled trial. Clin. Orthop. Relat. Res. 2013, 471, 3543–3553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, S.; van Hamersveld, K.T.; Marang-van de Mheen, P.J.; Kaptein, B.L.; Nelissen, R.; Toksvig-Larsen, S. Migration of a novel 3D-printed cementless versus a cemented total knee arthroplasty: Two-year results of a randomized controlled trial using radiostereometric analysis. Bone Jt. J. 2020, 102B, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Henricson, A.; Nilsson, K.G. Trabecular metal tibial knee component still stable at 10 years: An RSA study of 33 patients less than 60 years of age. Acta Orthop. 2016, 87, 504–510. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.H.; Park, J.W.; Jang, Y.S. The 22 to 25-Year Survival of Cemented and Cementless Total Knee Arthroplasty in Young Patients. J. Arthroplast. 2020, 36, 566–572. [Google Scholar] [CrossRef]
- Lizaur-Utrilla, A.; Miralles-Muñoz, F.A.; Lopez-Prats, F.A. Similar survival between screw cementless and cemented tibial components in young patients with osteoarthritis. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1585–1590. [Google Scholar] [CrossRef]
- Park, J.W.; Kim, Y.H. Simultaneous cemented and cementless total knee replacement in the same patients: A prospective comparison of long-Term outcomes using an identical design of NexGen prosthesis. J. Bone Jt. Surg. Br. Vol. 2011, 93, 1479–1486. [Google Scholar] [CrossRef] [Green Version]
- Van Hamersveld, K.T.; Marang-van de Mheen, P.J.; Tsonaka, R.; Valstar, E.R.; Toksvig-Larsen, S. Fixation and clinical outcome of uncemented peri-apatite-coated versus cemented total knee arthroplasty: Five-year follow-up of a randomised controlled trial using radiostereometric analysis (RSA). Bone Jt. J. 2017, 99-B, 1467–1476. [Google Scholar] [CrossRef]
- Kim, Y.H.; Park, J.W.; Lim, H.M.; Park, E.S. Cementless and cemented total knee arthroplasty in patients younger than fifty five years. Which is better? Int. Orthop. 2014, 38, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Mavrogenis, A.F.; Dimitriou, R.; Parvizi, J.; Babis, G.C. Biology of implant osseointegration. J. Musculoskelet. Neuronal Interact 2009, 9, 61–71. [Google Scholar]
- Cherian, J.J.; Banerjee, S.; Kapadia, B.H.; Jauregui, J.J.; Harwin, S.F.; Mont, M.A. Cementless total knee arthroplasty: A review. J. Knee Surg. 2014, 27, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Akizuki, S.; Takizawa, T.; Horiuchi, H. Fixation of a hydroxyapatite-tricalcium phosphate-Coated cementless knee prosthesis. Clinical and radiographic evaluation seven years after surgery. J. Bone Jt. Surg. Br. 2003, 85, 1123–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, R.A.; Lyon, J.H.; Jacobs, J.J.; Barden, R.M.; Berkson, E.M.; Sheinkop, M.B.; Rosenberg, A.G.; Galante, J.O. Problems with cementless total knee arthroplasty at 11 years followup. Clin. Orthop. Relat. Res. 2001, 392, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Nafei, A.; Nielsen, S.; Kristensen, O.; Hvid, I. The press-fit Kinemax knee arthroplasty. High failure rate of non-Cemented implants. J. Bone Jt. Surg. Br. 1992, 74, 243–246. [Google Scholar] [CrossRef] [Green Version]
- Ranawat, C.S.; Meftah, M.; Windsor, E.N.; Ranawat, A.S. Cementless fixation in total knee arthroplasty: Down the boulevard of broken dreams—Affirms. J. Bone Jt. Surg. Br. 2012, 94, 82–84. [Google Scholar] [CrossRef] [Green Version]
- Aprato, A.; Risitano, S.; Sabatini, L.; Giachino, M.; Agati, G.; Massè, A. Cementless total knee arthroplasty. Ann. Transl. Med. 2016, 4, 129. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Sun, H.; Zhang, K.; Li, S.; Wu, G.; Zhou, J.; Sun, X. Better outcomes are associated with cementless fixation in primary total knee arthroplasty in young patients: A systematic review and meta-analysis of randomized controlled trials. Medicine 2020, 99, e18750. [Google Scholar] [CrossRef]
- Chen, C.; Li, R. Cementless versus cemented total knee arthroplasty in young patients: A meta-analysis of randomized controlled trials. J. Orthop Surg. Res. 2019, 14, 262. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pfitzner, T.; von Roth, P.; Mayr, H.O.; Sostheim, M.; Hube, R. Fixation of stem in revision of total knee arthroplasty: Cemented versus cementless—A meta-Analysis. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 3200–3211. [Google Scholar] [CrossRef]
- Hampton, M.; Mansoor, J.; Getty, J.; Sutton, P.M. Uncemented tantalum metal components versus cemented tibial components in total knee arthroplasty: 11- to 15-year outcomes of a single-blinded randomized controlled trial. Bone Jt. J. 2020, 102-B, 1025–1032. [Google Scholar] [CrossRef]
- Rand, J.A. Cement or cementless fixation in total knee arthroplasty? Clin. Orthop. Relat. Res. 1991, 52–62. [Google Scholar] [CrossRef]
- Pap, K.; Vasarhelyi, G.; Gal, T.; Nemeth, G.; Abonyi, B.; Hangody, L.R.; Hangody, G.M.; Hangody, L. Evaluation of clinical outcomes of cemented vs uncemented knee prostheses covered with titanium plasma spray and hydroxyapatite: A minimum two years follow-up. Eklem Hastalik. Cerrahisi 2018, 29, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Savov, P.; Mielke, E.; Windhagen, H.; Calliess, T.; Richter, A.; Ettinger, M. Higher revision rate for posterior cruciate-retaining than posterior-stabilized total knee arthroplasty for the treatment of valgus osteoarthritis. Arch. Orthop. Trauma Surg. 2021, 141, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Spekenbrink-Spooren, A.; Van Steenbergen, L.N.; Denissen, G.A.W.; Swierstra, B.A.; Poolman, R.W.; Nelissen, R.G.H.H. Higher mid-Term revision rates of posterior stabilized compared with cruciate retaining total knee arthroplasties: 133,841 cemented arthroplasties for osteoarthritis in the Netherlands in 2007–2016. Acta Orthop. 2018, 89, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rassir, R.; Nolte, P.A.; van der Lugt, J.C.T.; Nelissen, R.; Sierevelt, I.N.; Verra, W.C. No differences in cost-effectiveness and short-term functional outcomes between cemented and uncemented total knee arthroplasty. BMC Musculoskelet. Disord. 2020, 21, 448. [Google Scholar] [CrossRef] [PubMed]
- Yayac, M.; Harrer, S.; Hozack, W.J.; Parvizi, J.; Courtney, P.M. The Use of Cementless Components Does Not Significantly Increase Procedural Costs in Total Knee Arthroplasty. J. Arthroplast. 2020, 35, 407–412. [Google Scholar] [CrossRef] [Green Version]
- Lawrie, C.M.; Schwabe, M.; Pierce, A.; Nunley, R.M.; Barrack, R.L. The cost of implanting a cemented versus cementless total knee arthroplasty. Bone Jt. J. 2019, 101-B, 61–63. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Level of Evidence | No of Patients | No of Knees (C/UC) | Male (%) | Mean Age (C/UC) | CR or PS | Femoral Prosthesis | Tibial Prosthesis | Patellar Resurfacing | Mean Follow-Up (Years) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hasan [25] | 2020 | I | 69 | 34/35 | 52.17% | 66/65 | CR | Random | Random | No | 2.0 | Complications, Revision |
| Kim [27] | 2020 | I | 261 | 261/261 | 31.03% | 62.5 | CR | Random | Random | Yes | 23.8 | KSS, ROM, RLL, Complications, Revision, Survivorship |
| Hamersveld [30] | 2017 | I | 60 | 30/30 | 46.67% | 65.7/66.8 | CR | Random | Random | No | 5.0 | KSS, Complications, Revision |
| Henricson [26] | 2016 | I | 33 | 26/21 | 56.10% | 54 | CR | NA | Random | No | 10.0 | KSS, ROM, RLL, Complications, Revision, Survivorship |
| Choy [23] | 2014 | I | 126 | 86/82 | 7.94% | 69/65 | CR | UC | Random | No | 9.5 | KSS, ROM, RLL, Complications, Revision |
| Lizaur-Utrilla [28] | 2014 | I | 93 | 48/45 | 27.96% | 52/51.4 | CR | UC | Random | NA | 7.1 | KSS, RLL, Complications, Revision, Survivorship |
| Kim [31] | 2014 | I | 80 | 80/80 | 21.25% | 54.3/54.3 | CR | Random | Random | Yes | 16.6 | ROM, RLL, Complications, Revision |
| Fernandez-Fairen [24] | 2013 | I | 145 | 71/74 | 24.83% | 60/61 | CR | UC | Random | No | 5.0 | KSS, RLL, Complications |
| Park [29] | 2011 | I | 50 | 50/50 | 22.00% | 58.4 | CR | Random | Random | Yes | 13.6 | KSS, ROM, RLL, Complications, Revision, Survivorship |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.; Xu, J.; Dai, H.; Yu, Y.; Wang, Y.; Zhu, Y.; Tao, T.; Jiang, Y. Uncemented Tibial Fixation Has Comparable Prognostic Outcomes and Safety Versus Cemented Fixation in Cruciate-Retaining Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 1961. https://doi.org/10.3390/jcm12051961
Chen K, Xu J, Dai H, Yu Y, Wang Y, Zhu Y, Tao T, Jiang Y. Uncemented Tibial Fixation Has Comparable Prognostic Outcomes and Safety Versus Cemented Fixation in Cruciate-Retaining Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(5):1961. https://doi.org/10.3390/jcm12051961
Chicago/Turabian StyleChen, Kai, Jintao Xu, Hanhao Dai, Yaohui Yu, Yishu Wang, Yi Zhu, Tianqi Tao, and Yiqiu Jiang. 2023. "Uncemented Tibial Fixation Has Comparable Prognostic Outcomes and Safety Versus Cemented Fixation in Cruciate-Retaining Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 5: 1961. https://doi.org/10.3390/jcm12051961