
An Artificial Intelligence-Enabled ECG Algorithm for Predicting the Risk of Recurrence in Patients with Paroxysmal Atrial Fibrillation after Catheter Ablation
Abstract
:1. Introduction
2. Materials and Methods
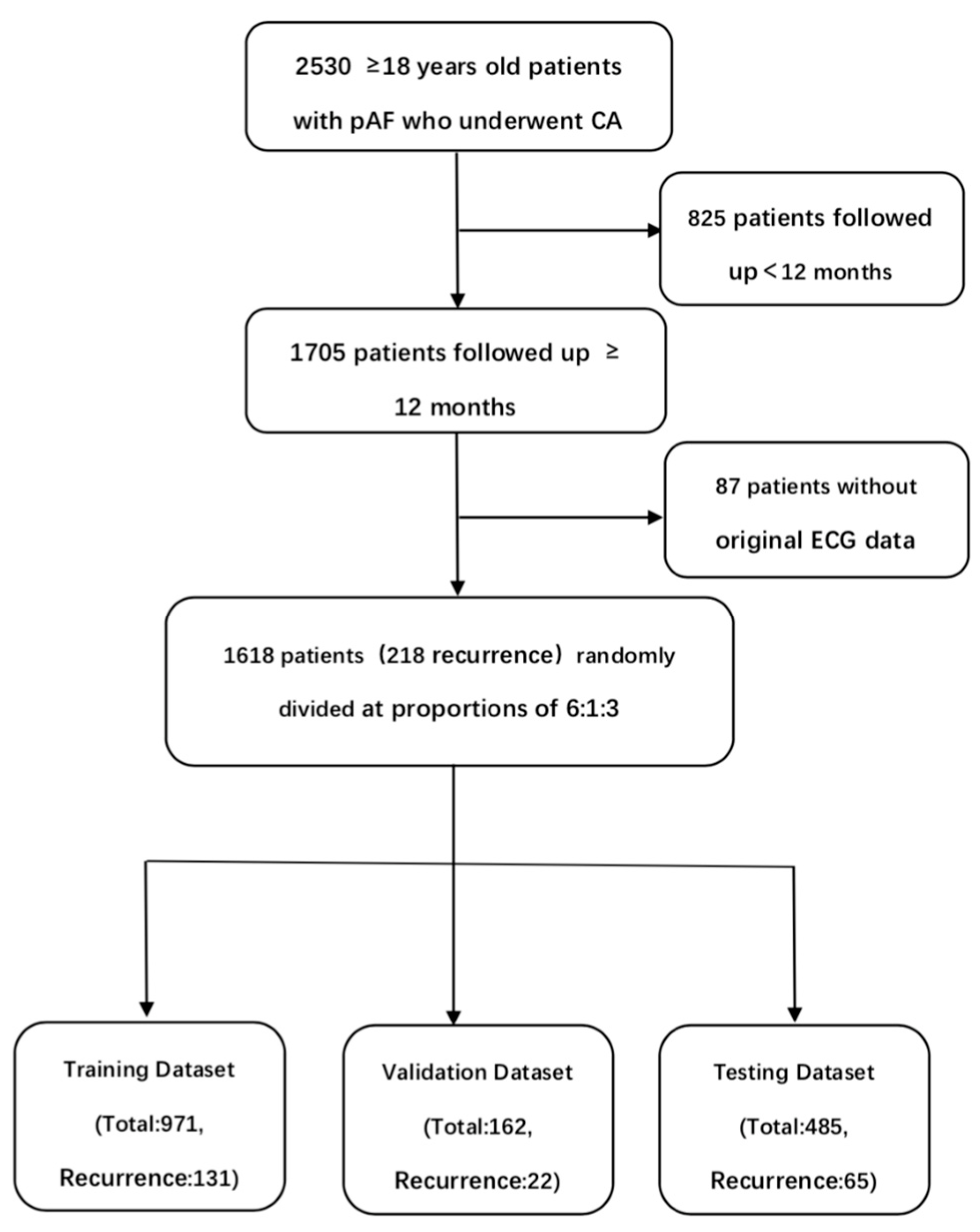
2.1. Data Sources and Study Population
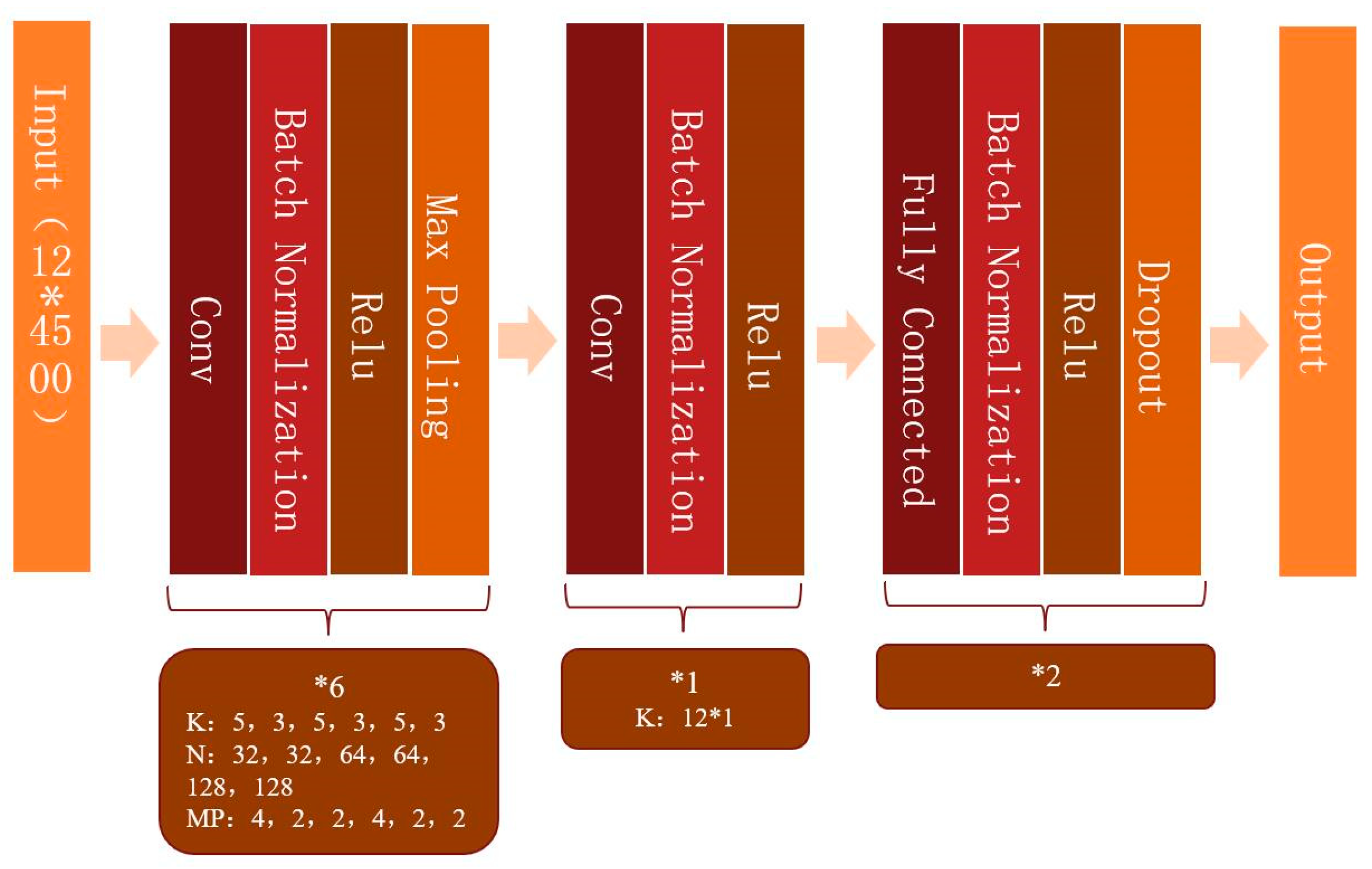
2.2. Model Development
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
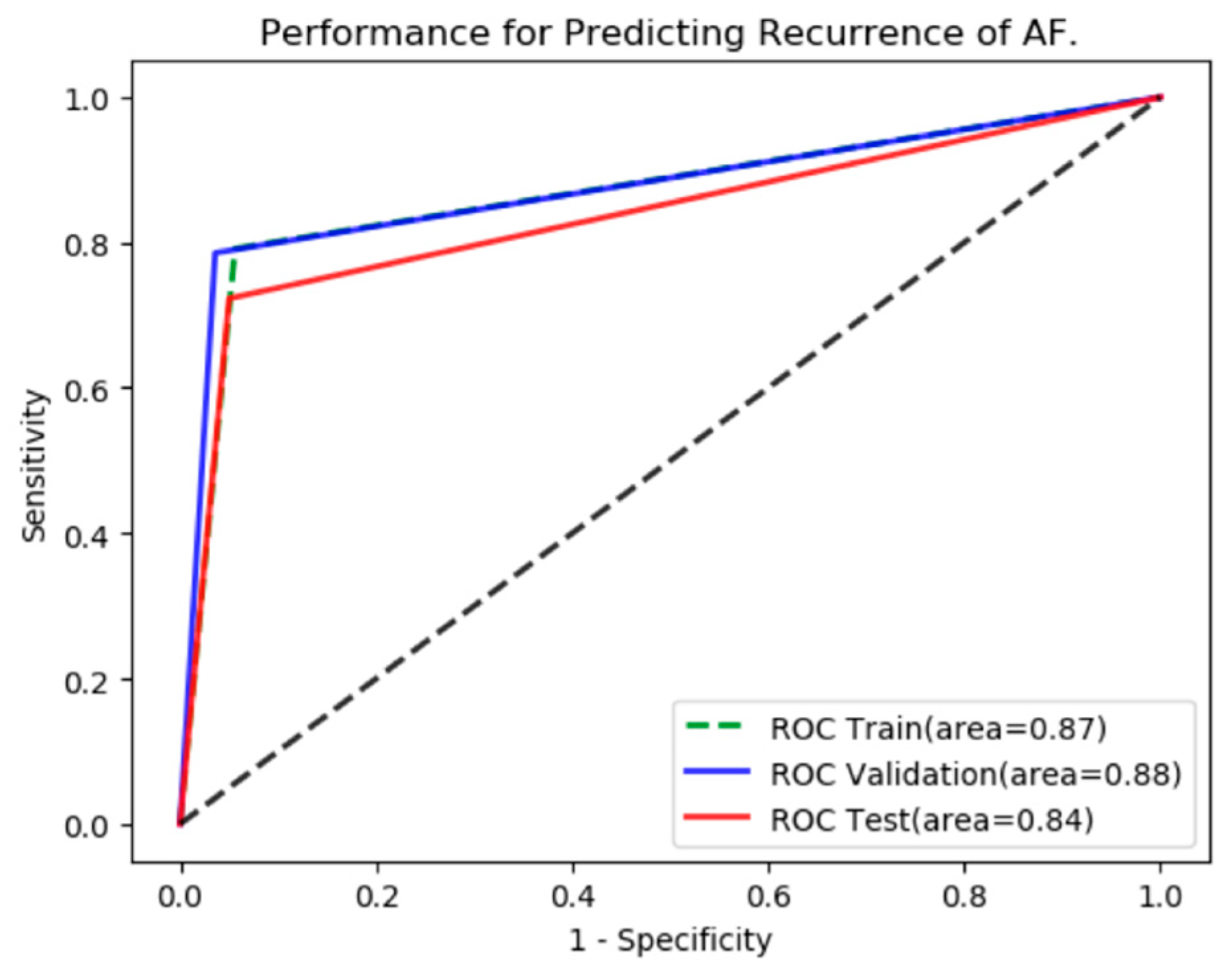
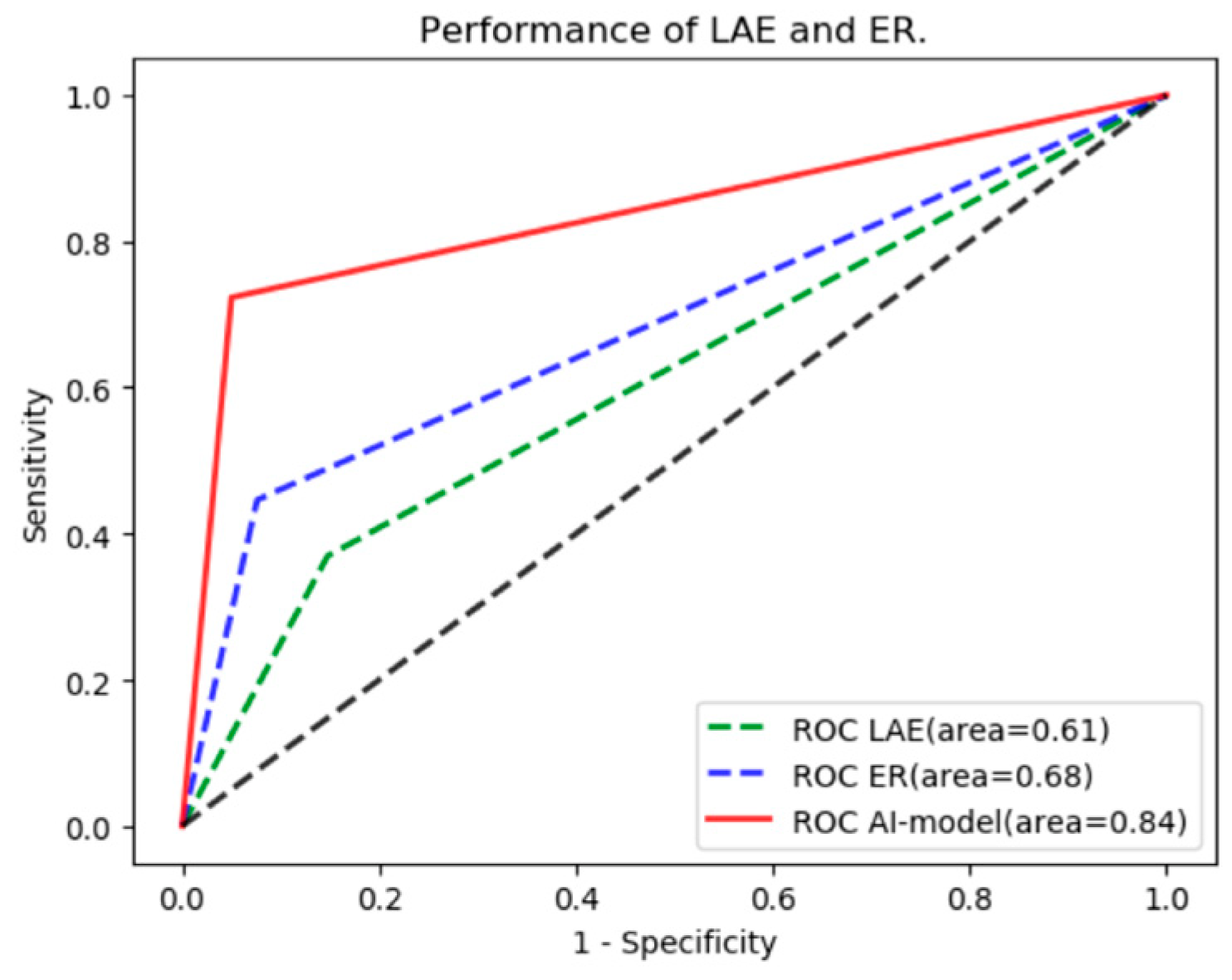
3.2. The Performance of the AI Algorithm
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scoring Systems | Number of Studies | Total Study Population | Variables | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | Heart Failure | Hypertension | Diabetes | Renal Insufficiency | Vascular Disease | Cardiomyopathy | Gender | AF Type | LAE | LVEF | Metabolic Syndrome | BMI | ER | Smoking | Duration of AF | Antiarrhythmic Drugs | Bundle Branch block | Left Atrial Sphericity | Structural Heart Disease | Stroke | |||
| CHADS2 | 4 | 2792 | √ | √ | √ | √ | √ | ||||||||||||||||
| CHA2DS2VASc | 2 | 2307 | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| ALARMEc | 4 | 1630 | √ | √ | √ | √ | √ | ||||||||||||||||
| APPLE | 6 | 4641 | √ | √ | √ | √ | √ | ||||||||||||||||
| ATLAS | 1 | 1934 | √ | √ | √ | √ | √ | ||||||||||||||||
| BASE-AF2 | 3 | 1779 | √ | √ | √ | √ | √ | ||||||||||||||||
| CAAP-AF | 3 | 3698 | √ | √ | √ | √ | √ | ||||||||||||||||
| DR-FLASH | 2 | 2016 | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| LAGO | 1 | 243 | √ | √ | √ | √ | |||||||||||||||||
| MB-LATER | 3 | 1769 | √ | √ | √ | √ | √ | ||||||||||||||||
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Staerk, L.; Sherer, J.A.; Ko, D.; Benjamin, E.J.; Helm, R.H. Atrial Fibrillation: Epidemiology, Pathophysiology, and Clinical Outcomes. Circ. Res. 2017, 120, 1501–1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Bai, Y.; Shantsila, A.; Fauchier, L.; Potpara, T.S.; Lip, G.Y.H. Clinical scores for outcomes of rhythm control or arrhythmia progression in patients with atrial fibrillation: A systematic review. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2017, 106, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Kosich, F.; Schumacher, K.; Potpara, T.; Lip, G.Y.; Hindricks, G.; Kornej, J. Clinical scores used for the prediction of negative events in patients undergoing catheter ablation for atrial fibrillation. Clin. Cardiol. 2019, 42, 320–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Kusunose, K.; Abe, T.; Haga, A.; Fukuda, D.; Yamada, H.; Harada, M.; Sata, M. A Deep Learning Approach for Assessment of Regional Wall Motion Abnormality From Echocardiographic Images. JACC Cardiovasc. Imaging 2020, 13, 374–381. [Google Scholar] [CrossRef]
- Attia, Z.I.; Kapa, S.; Lopez-Jimenez, F.; McKie, P.M.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Enriquez-Sarano, M.; Noseworthy, P.A.; Munger, T.M.; et al. Screening for cardiac contractile dysfunction using an artificial intelligence-enabled electrocardiogram. Nat. Med. 2019, 25, 70–74. [Google Scholar] [CrossRef]
- Furui, K.; Morishima, I.; Morita, Y.; Kanzaki, Y.; Takagi, K.; Yoshida, R.; Nagai, H.; Watanabe, N.; Yoshioka, N.; Yamauchi, R.; et al. Predicting long-term freedom from atrial fibrillation after catheter ablation by a machine learning algorithm: Validation of the CAAP-AF score. J. Arrhythmia 2020, 36, 297–303. [Google Scholar] [CrossRef]
- Mesquita, J.; Ferreira, A.M.; Cavaco, D.; Moscoso Costa, F.; Carmo, P.; Marques, H.; Morgado, F.; Mendes, M.; Adragão, P. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure—ATLAS score. Europace 2018, 20, f428–f435. [Google Scholar] [CrossRef]
- Budzianowski, J.; Hiczkiewicz, J.; Burchardt, P.; Pieszko, K.; Rzeźniczak, J.; Budzianowski, P.; Korybalska, K. Predictors of atrial fibrillation early recurrence following cryoballoon ablation of pulmonary veins using statistical assessment and machine learning algorithms. Heart Vessel. 2019, 34, 352–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela, M.; Bisbal, F.; Zacur, E.; Berruezo, A.; Aslanidi, O.V.; Mont, L.; Lamata, P. Novel Computational Analysis of Left Atrial Anatomy Improves Prediction of Atrial Fibrillation Recurrence after Ablation. Front. Physiol. 2017, 8, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shade, J.K.; Ali, R.L.; Basile, D.; Popescu, D.; Akhtar, T.; Marine, J.E.; Spragg, D.D.; Calkins, H.; Trayanova, N.A. Preprocedure Application of Machine Learning and Mechanistic Simulations Predicts Likelihood of Paroxysmal Atrial Fibrillation Recurrence Following Pulmonary Vein Isolation. Circ. Arrhythmia Electrophysiol. 2020, 13, e008213. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Deng, H.; Xue, Y.; Liao, H.; Wu, S. Detection of Left Atrial Enlargement Using a Convolutional Neural Network-Enabled Electrocardiogram. Front. Cardiovasc. Med. 2020, 7, 609976. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Xiong, J.; Hou, Y.; Zhu, M.; Lu, Y.; Xu, Y.; Teliewubai, J.; Liu, W.; Xu, X.; Li, X.; et al. Early detection of ST-segment elevated myocardial infarction by artificial intelligence with 12-lead electrocardiogram. Int. J. Cardiol. 2020, 317, 223–230. [Google Scholar] [CrossRef]
- Kornej, J.; Hindricks, G.; Shoemaker, M.B.; Husser, D.; Arya, A.; Sommer, P.; Rolf, S.; Saavedra, P.; Kanagasundram, A.; Patrick Whalen, S.; et al. The APPLE score: A novel and simple score for the prediction of rhythm outcomes after catheter ablation of atrial fibrillation. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2015, 104, 871–876. [Google Scholar] [CrossRef] [Green Version]
- Kornej, J.; Hindricks, G.; Arya, A.; Sommer, P.; Husser, D.; Bollmann, A. The APPLE Score—A Novel Score for the Prediction of Rhythm Outcomes after Repeat Catheter Ablation of Atrial Fibrillation. PLoS ONE 2017, 12, e0169933. [Google Scholar] [CrossRef]
- Kornej, J.; Büttner, P.; Sommer, P.; Dagres, N.; Dinov, B.; Schumacher, K.; Bollmann, A.; Hindricks, G. Prediction of electro-anatomical substrate using APPLE score and biomarkers. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2019, 21, 54–59. [Google Scholar] [CrossRef]
- Canpolat, U.; Aytemir, K.; Yorgun, H.; Şahiner, L.; Kaya, E.B.; Oto, A. A proposal for a new scoring system in the prediction of catheter ablation outcomes: Promising results from the Turkish Cryoablation Registry. Int. J. Cardiol. 2013, 169, 201–206. [Google Scholar] [CrossRef]
- Winkle, R.A.; Jarman, J.W.; Mead, R.H.; Engel, G.; Kong, M.H.; Fleming, W.; Patrawala, R.A. Predicting atrial fibrillation ablation outcome: The CAAP-AF score. Heart Rhythm 2016, 13, 2119–2125. [Google Scholar] [CrossRef] [Green Version]
- Kosiuk, J.; Dinov, B.; Kornej, J.; Acou, W.J.; Schönbauer, R.; Fiedler, L.; Buchta, P.; Myrda, K.; Gąsior, M.; Poloński, L.; et al. Prospective, multicenter validation of a clinical risk score for left atrial arrhythmogenic substrate based on voltage analysis: DR-FLASH score. Heart Rhythm 2015, 12, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Mujović, N.; Marinković, M.; Marković, N.; Shantsila, A.; Lip, G.Y.; Potpara, T.S. Prediction of very late arrhythmia recurrence after radiofrequency catheter ablation of atrial fibrillation: The MB-LATER clinical score. Sci. Rep. 2017, 7, 40828. [Google Scholar] [CrossRef] [Green Version]
- Deng, H.; Shantsila, A.; Xue, Y.; Potpara, T.S.; Bai, Y.; Zhan, X.; Fang, X.; Liao, H.; Wei, W.; Wu, S.; et al. Using the MB-LATER score for predicting arrhythmia outcome after catheter ablation for atrial fibrillation: The Guangzhou atrial fibrillation project. Int. J. Clin. Pract. 2018, 72, e13247. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Mujovic, N.; Sivasambu, B.; Shantsila, A.; Marinkovic, M.; Calkins, H.; Spragg, D.; Lip, G.Y.H. Validation of the MB-LATER score for prediction of late recurrence after catheter-ablation of atrial fibrillation. Int. J. Cardiol. 2019, 276, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Latchamsetty, R.; Morady, F. Atrial Fibrillation Ablation. Annu. Rev. Med. 2018, 69, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, M.; Berkowitsch, A.; Greiss, H.; Zaltsberg, S.; Pajitnev, D.; Deubner, N.; Hamm, C.W.; Pitschner, H.F.; Kuniss, M.; Neumann, T. Repeated catheter ablation of atrial fibrillation: How to predict outcome? Circ. J. Off. J. Jpn. Circ. Soc. 2013, 77, 2271–2279. [Google Scholar] [CrossRef] [Green Version]
- Bisbal, F.; Alarcón, F.; Ferrero-de-Loma-Osorio, A.; González-Ferrer, J.J.; Alonso, C.; Pachón, M.; Tizón, H.; Cabanas-Grandío, P.; Sanchez, M.; Benito, E.; et al. Left atrial geometry and outcome of atrial fibrillation ablation: Results from the multicentre LAGO-AF study. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1002–1009. [Google Scholar] [CrossRef]
- Kornej, J.; Schumacher, K.; Dinov, B.; Kosich, F.; Sommer, P.; Arya, A.; Husser, D.; Bollmann, A.; Lip, G.Y.H.; Hindricks, G. Prediction of electro-anatomical substrate and arrhythmia recurrences using APPLE, DR-FLASH and MB-LATER scores in patients with atrial fibrillation undergoing catheter ablation. Sci. Rep. 2018, 8, 12686. [Google Scholar] [CrossRef]
- Makimoto, H.; Höckmann, M.; Lin, T.; Glöckner, D.; Gerguri, S.; Clasen, L.; Schmidt, J.; Assadi-Schmidt, A.; Bejinariu, A.; Müller, P.; et al. Performance of a convolutional neural network derived from an ECG database in recognizing myocardial infarction. Sci. Rep. 2020, 10, 8445. [Google Scholar] [CrossRef]
- Phillips, M.; Marsden, H.; Jaffe, W.; Matin, R.N.; Wali, G.N.; Greenhalgh, J.; McGrath, E.; James, R.; Ladoyanni, E.; Bewley, A.; et al. Assessment of Accuracy of an Artificial Intelligence Algorithm to Detect Melanoma in Images of Skin Lesions. JAMA Netw. Open 2019, 2, e1913436. [Google Scholar] [CrossRef] [Green Version]





| No Recurrence | Recurrence | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| Age (Mean) (Year) | 59.6 | 58.5 | 0.27 | —— | |
| Gender | Male | 910 | 142 | 0.97 | —— |
| Female | 490 | 76 | |||
| BMI Grade (kg/m2) | <18.5 | 33 | 8 | 0.37 | —— |
| 18.5–25 | 1012 | 146 | |||
| 25–30 | 323 | 58 | |||
| ≥30 | 32 | 6 | |||
| Smoking | yes | 197 | 27 | 0.50 | —— |
| no | 1203 | 191 | |||
| Alcohol | yes | 73 | 14 | 0.46 | —— |
| no | 1327 | 204 | |||
| Hypertension | yes | 517 | 78 | 0.74 | —— |
| no | 883 | 140 | |||
| Diabetes | yes | 140 | 19 | 0.55 | —— |
| no | 1260 | 199 | |||
| Stroke | yes | 106 | 17 | 0.91 | —— |
| no | 1294 | 201 | |||
| Vascular Disease | yes | 93 | 11 | 0.37 | —— |
| no | 1307 | 207 | |||
| Coronary Artery Disease | yes | 127 | 21 | 0.79 | —— |
| no | 1273 | 197 | |||
| Bundle Branch Block | yes | 113 | 20 | 0.58 | —— |
| no | 1287 | 198 | |||
| Cardiomyopathy | yes | 17 | 4 | 0.45 | —— |
| no | 1383 | 214 | |||
| Left Atrial Enlargement | yes | 258 | 74 | <0.01 | <0.01 |
| no | 1142 | 144 | |||
| Left Ventricular Enlargement | yes | 16 | 2 | 0.77 | —— |
| no | 1384 | 216 | |||
| LVEF | ≥50% | 1357 | 9 | 0.41 | —— |
| <50% | 43 | 209 | |||
| eGFR | ≥60 | 1304 | 204 | 0.81 | —— |
| <60 | 96 | 14 | |||
| AF Duration (years) | ≤6 | 1255 | 192 | 0.48 | —— |
| >6 | 145 | 26 | |||
| Early Recurrence | yes | 118 | 79 | <0.01 | <0.01 |
| no | 1282 | 139 | |||
| Predicted | Se (%) | Sp (%) | Acc (%) | Pre (%) | F1 Scores | p Value | |||
|---|---|---|---|---|---|---|---|---|---|
| No R. | R. | ||||||||
| CNN Model | no R. | 399 | 21 | 72.3 | 95.0 | 92.0 | 69.1 | 0.71 | —— |
| R. | 18 | 47 | |||||||
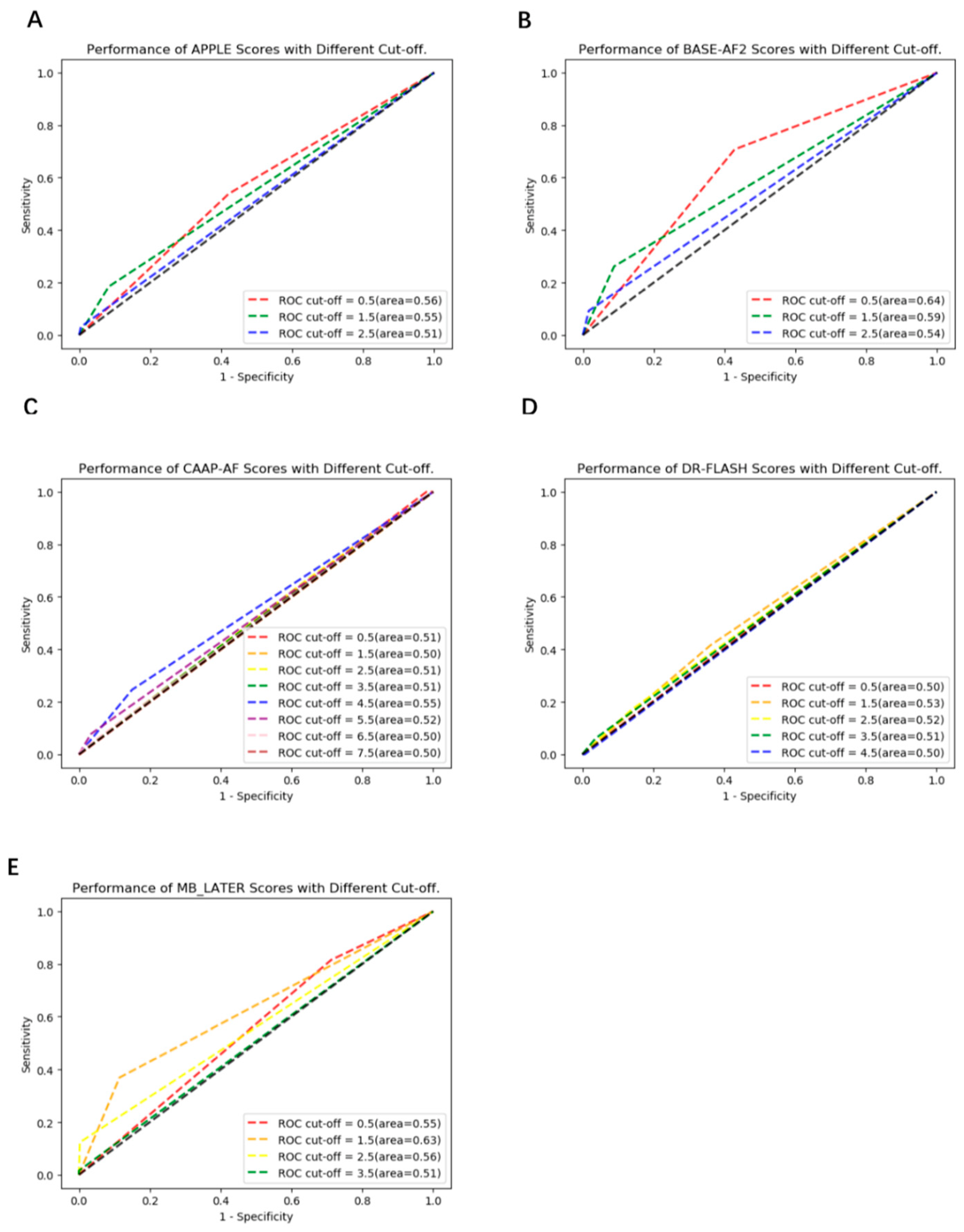
| APPLE | no R. | 243 | 177 | 53.8 | 57.9 | 57.3 | 16.5 | 0.25 | <0.01 |
| R. | 30 | 35 | |||||||
| BASE-AF2 | no R. | 240 | 180 | 70.8 | 57.1 | 59.0 | 20.4 | 0.32 | <0.01 |
| R. | 19 | 46 | |||||||
| CAAP-AF | no R. | 357 | 63 | 24.6 | 85.0 | 76.9 | 20.3 | 0.22 | <0.01 |
| R. | 49 | 16 | |||||||
| DR-FLASH | no R. | 268 | 152 | 41.5 | 63.8 | 60.8 | 15.1 | 0.22 | <0.01 |
| R. | 38 | 27 | |||||||
| MB-LATER | no R. | 372 | 48 | 36.9 | 88.6 | 81.6 | 33.3 | 0.35 | <0.01 |
| R. | 41 | 24 | |||||||
| Predicted | Se (%) | Sp (%) | Acc (%) | Pre (%) | F1 Scores | p Value | |||
|---|---|---|---|---|---|---|---|---|---|
| no R. | R. | ||||||||
| AI Model | No R. | 399 | 21 | 72.3 | 95.0 | 92.0 | 69.1 | 0.71 | —— |
| R. | 18 | 47 | |||||||
| LAE | no R. | 358 | 62 | 36.9 | 85.2 | 78.8 | 27.9 | 0.32 | <0.01 |
| R. | 41 | 24 | |||||||
| ER | no R. | 388 | 32 | 44.6 | 92.4 | 86.0 | 47.5 | 0.46 | <0.01 |
| R. | 36 | 29 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, J.; Deng, H.; Liao, H.; Fang, X.; Zhan, X.; Wei, W.; Wu, S.; Xue, Y. An Artificial Intelligence-Enabled ECG Algorithm for Predicting the Risk of Recurrence in Patients with Paroxysmal Atrial Fibrillation after Catheter Ablation. J. Clin. Med. 2023, 12, 1933. https://doi.org/10.3390/jcm12051933
Jiang J, Deng H, Liao H, Fang X, Zhan X, Wei W, Wu S, Xue Y. An Artificial Intelligence-Enabled ECG Algorithm for Predicting the Risk of Recurrence in Patients with Paroxysmal Atrial Fibrillation after Catheter Ablation. Journal of Clinical Medicine. 2023; 12(5):1933. https://doi.org/10.3390/jcm12051933
Chicago/Turabian StyleJiang, Junrong, Hai Deng, Hongtao Liao, Xianhong Fang, Xianzhang Zhan, Wei Wei, Shulin Wu, and Yumei Xue. 2023. "An Artificial Intelligence-Enabled ECG Algorithm for Predicting the Risk of Recurrence in Patients with Paroxysmal Atrial Fibrillation after Catheter Ablation" Journal of Clinical Medicine 12, no. 5: 1933. https://doi.org/10.3390/jcm12051933