
Distance Monitoring of Advanced Cancer Patients with Impaired Cardiac and Respiratory Function Assisted at Home: A Study Protocol in Italy
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
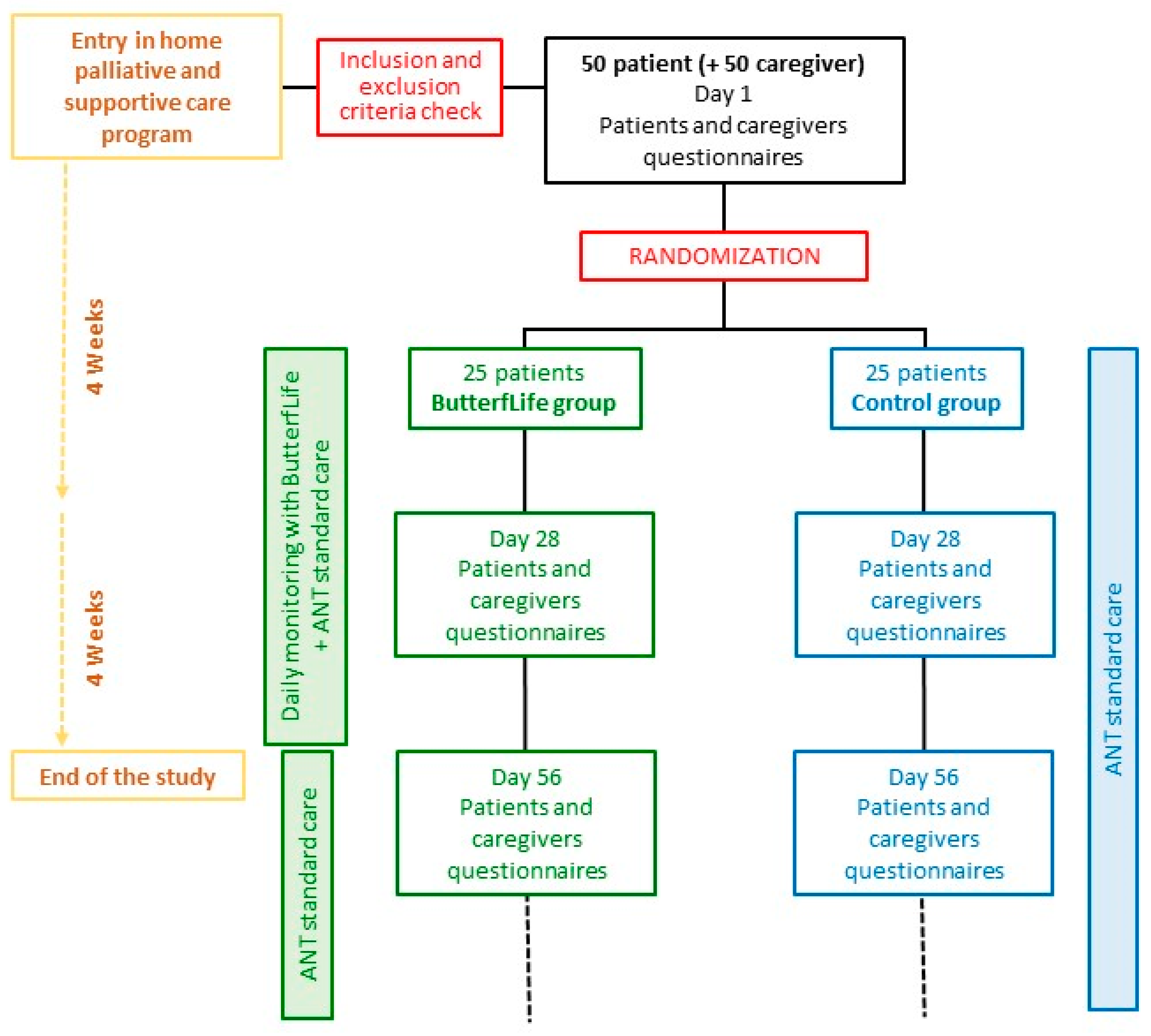
2.1. Study Design
2.2. Setting
2.3. Study Population
2.4. Recruitment and Randomization
2.5. Procedures and Data Collection
2.6. Measures and Outcomes
- The quality of life (QOL) of patients will be assessed by the EuroQoL-5D-3L questionnaire (EQ-5D-3L), Italian version [27,28], a generic instrument consisting of 2 distinct sections: patient’s subjective assessment of five dimensions of quality of life (mobility, self-care, daily activities, pain/discomfort, and anxiety/depression); each item has responses graded from 1 to 3, where level 1 indicates no problems and level 3 indicates extreme limitation. Assessment of the patient’s perceived health status will be made on a visual analogue scale (VAS) graded from 0 (the worst possible health status) to 100 (the best possible health status).
- The psychological status of the patient will be evaluated by the Depression Anxiety Stress Scales-21 (DASS-21), Italian version [29,30], a self-assessment scale to detect depression, anxiety and stress. The scale consists of 21 items, 7 for each emotional state, assessed on a 4-point Likert scale (from 0 = never to 3 = always).
- Care burden perceived by the caregiver will be assessed by the Caregiver Burden Inventory (CBI) [31], a questionnaire consisting of 24 questions on 5 domains (time-dependent care burden, developmental burden, physical burden, social burden, and emotional burden). Completion requires ticking the box from 0 to 4 (0 = not at all, 1 = slightly, 2 = moderately, 3 = quite a lot, 4 = very much) that best describes the current condition or personal impression of the caregiver. The total score ranges from 0 to 100, where 100 indicates the highest perceived caregiver burden.
- Satisfaction with care stated by the caregiver will be assessed through the Family Satisfaction with Advanced Cancer Care-2 questionnaire (FAMCARE-2), Italian version [32,33], a specific validated instrument to measure family members’ satisfaction with the care received from a palliative care team for their relative with advanced cancer. The FAMCARE-2 consists of 17 questions whose answers, on a 5-point ordinal score ranging from 1 (very dissatisfied) to 5 (very satisfied), cover 5 domains (management of symptoms and patient comfort, information provided, support to the family, and psychological assistance to the patient). The total FAMCARE-2 score can range from 17 to 85, where 85 represents the highest satisfaction with the care received.
- The acceptability and ease of use of the device will be assessed by a questionnaire directed to the physician.
- The number of scheduled, unscheduled, and on-call visits (doctor and nurse), as well as the number of phone calls and emergency phone calls received by the doctor and nurse, will be assessed.
- The number of admissions to the emergency room will be assessed.
- Hospitalization days will be assessed.
2.7. Other Assessments
- Demographic data (sex, age).
- Primary site of disease (recorded according the International Classification of Diseases (9th revision) [34] and then classified as gastrointestinal, respiratory tract, genitourinary, breast, nervous system, haematological, and other), time since diagnosis, and presence of metastases.
- Disease stage (radically operated cancer (adjuvant therapy—supportive therapy); advanced cancer (early palliative care—supportive therapy); locally advanced cancer (adjuvant therapy); advanced cancer (palliative care only).
- KPS.
- Edmonton Symptom Assessment Scale (ESAS) [35].
- Cancer therapy (chemotherapy, hormone therapy, radiotherapy, immunotherapy) and pain therapy.
2.8. Training and Monitoring
2.9. Sample Size
2.10. Statistical Analysis
- Descriptive analysis of the characteristics of the recruited subjects. The following parameters are shown as frequencies: age, sex, KPS, diagnosis, time since diagnosis, presence of metastases, symptoms, current therapies, and stage of the disease.
- Analysis of acceptability and feasibility: percentage of eligible patients proposed for the study who agree to participate, percentage of drop out from the study, number of measurements/week per patient, patient assessment of ease of use, difficulties encountered, and usefulness.
- The trend of secondary outcomes (QOL, psychological state, and caregiver care burden) over time (day 1, day 28 and day 56) will be analyzed using a general linear model for repeated measures.
- Comparison between the ButterfLife and Control groups: after analyzing the normality of the variables (Shapiro–Wilk test), the differences between the two groups for secondary outcomes (QOL, psychological state, caregiver care burden, caregiver satisfaction with the care received, number of scheduled visits, unscheduled visits, on-call visits, phone calls received by the doctor and nurse, number of visits to the emergency room, number of hospital admissions and hospitalization) will be analyzed with parametric (Student’s t-test) or non-parametric tests (Mann–Whitney test).
3. Expected Impact
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costantini, M.; Sleeman, K.E.; Peruselli, C.; Higginson, I.J. Response and role of palliative care during the COVID-19 pandemic: A national telephone survey of hospices in Italy. Palliat. Med. 2020, 34, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.K.; Smith, T.J. Palliative Care for Patients With Cancer in the COVID-19 Era. JAMA Oncol. 2020, 6, 1527. [Google Scholar] [CrossRef]
- Ting, R.; Edmonds, P.; Higginson, I.J.; Sleeman, K.E. Palliative care for patients with severe COVID-19. BMJ 2020, 370, m2710. [Google Scholar] [CrossRef] [PubMed]
- Shirke, M.M.; Shaikh, S.A.; Harky, A. Implications of Telemedicine in Oncology during the COVID-19 Pandemic. Acta Biomed. 2020, 91, e2020022. [Google Scholar] [CrossRef] [PubMed]
- Bitar, H.; Alismail, S. The role of eHealth, telehealth, and telemedicine for chronic disease patients during COVID-19 pandemic: A rapid systematic review. Digit. Health 2021, 7, 205520762110093. [Google Scholar] [CrossRef]
- Hanlon, P.; Daines, L.; Campbell, C.; McKinstry, B.; Weller, D.; Pinnock, H. Telehealth Interventions to Support Self-Management of Long-Term Conditions: A Systematic Metareview of Diabetes, Heart Failure, Asthma, Chronic Obstructive Pulmonary Disease, and Cancer. J. Med. Internet Res. 2017, 19, e172. [Google Scholar] [CrossRef]
- Kane, K.; Kennedy, F.; Absolom, K.L.; Harley, C.; Velikova, G. Quality of life support in advanced cancer—Web and technological interventions: Systematic review and narrative synthesis. BMJ Support. Palliat. Care 2020, 26, bmjspcare-2020-002820. [Google Scholar] [CrossRef]
- Goodman, W.; Bagnall, A.-M.; Ashley, L.; Azizoddin, D.; Muehlensiepen, F.; Blum, D.; Bennett, M.I.; Allsop, M. The Extent of Engagement With Telehealth Approaches by Patients With Advanced Cancer: Systematic Review. JMIR Cancer 2022, 8, e33355. [Google Scholar] [CrossRef]
- Finucane, A.M.; O’Donnell, H.; Lugton, J.; Gibson-Watt, T.; Swenson, C.; Pagliari, C. Digital health interventions in palliative care: A systematic meta-review. NPJ Digit. Med. 2021, 4, 61. [Google Scholar] [CrossRef]
- Sofia, M.; Pisciotta, M.; Gervasi, F.; Oldani, S.; Marzola, A.; Angelini, C. Fattibilità ed efficacia della telemedicina nel contesto delle cure palliative domiciliari. Riv It Cure Palliat. 2021, 23, 104–110. [Google Scholar] [CrossRef]
- Hancock, S.; Preston, N.; Jones, H.; Gadoud, A. Telehealth in palliative care is being described but not evaluated: A systematic review. BMC Palliat. Care 2019, 18, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Head, B.A.; Schapmire, T.J. A Systematic Review of Telehealth in Palliative Care: Caregiver Outcomes. Telemed. e-Health 2016, 22, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Head, B.A.; Schapmire, T.J.; Zheng, Y. Telehealth in Palliative Care. J. Hosp. Palliat. Nurs. 2017, 19, 130–139. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Cossarizza, A.; Boriani, G. COVID-19 pandemic: Usefulness of telemedicine in management of arrhythmias in elderly people. J. Geriatr. Cardiol. 2020, 17, 593–596. [Google Scholar] [CrossRef]
- Abelsson, T.; Morténius, H.; Bergman, S.; Karlsson, A.-K. Quality and availability of information in primary healthcare: The patient perspective. Scand. J. Prim. Health Care 2020, 38, 33–41. [Google Scholar] [CrossRef]
- Hall, J. The impact of COVID-19 on critical cardiac care and what is to come postpandemic. Future Cardiol. 2021, 17, 7–10. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Han, X.; Sun, J.; Li, C.; Adhikari, B.K.; Zhang, J.; Miao, X.; Chen, Z. Cardio-Oncology: A Myriad of Relationships Between Cardiovascular Disease and Cancer. Front. Cardiovasc. Med. 2022, 9, 561. [Google Scholar] [CrossRef]
- Muhandiramge, J.; Zalcberg, J.R.; van Londen, G.J.; Warner, E.T.; Carr, P.R.; Haydon, A.; Orchard, S.G. Cardiovascular Disease in Adult Cancer Survivors: A Review of Current Evidence, Strategies for Prevention and Management, and Future Directions for Cardio-oncology. Curr. Oncol. Rep. 2022, 24, 1579–1592. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Ministero della Salute. Approvazione delle Linee Guida per i Servizi di Telemedicina-Requisiti Funzionali e Livelli di Servizio; Gazzetta Ufficiale della Repubblica Italiana: Roma, Italy, 2022; Volume 256. [Google Scholar]
- Casadio, M.; Biasco, G.; Abernethy, A.; Bonazzi, V.; Pannuti, R.; Pannuti, F. The National Tumor Association Foundation (ANT): A 30 year old model of home palliative care. BMC Palliat. Care 2010, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Ostan, R.; Varani, S.; Pannuti, F.; Pannuti, R.; Biasco, G.; Bruera, E. End of life care for patients with cancer: Clinical, geographical, and socio-cultural differences. Palliat. Support. Care, 2023, in press.
- Moscato, S.; Palumbo, P.; Sichi, V.; Giannelli, A.; Varani, S.; Chiari, L. Objective assessment of pain in uncontrolled environment through electrodermal activity in oncological population. In Proceedings of the IASP Virtual Series on Pain and Expo, Online, September 2020–March 2021. [Google Scholar]
- Moscato, S.; Sichi, V.; Giannelli, A.; Palumbo, P.; Ostan, R.; Varani, S.; Pannuti, R.; Chiari, L. Virtual Reality in Home Palliative Care: Brief Report on the Effect on Cancer-Related Symptomatology. Front. Psychol. 2021, 24, 709154. [Google Scholar] [CrossRef] [PubMed]
- Franchini, L.; Varani, S.; Ostan, R.; Bocchi, I.; Pannuti, R.; Biasco, G.; Bruera, E. Home palliative care professionals perception of challenges during the COVID-19 outbreak: A qualitative study. Palliat. Med. 2021, 35, 862–874. [Google Scholar] [CrossRef] [PubMed]
- Hajesmaeel-Gohari, S.; Bahaadinbeigy, K. The most used questionnaires for evaluating telemedicine services. BMC Med. Inform. Decis. Mak. 2021, 21, 36. [Google Scholar] [CrossRef] [PubMed]
- EuroQol Research Foundation EQ-5D-3L User Guide (Version 6.0). Available online: https://euroqol.org/publications/user-guides/ (accessed on 24 August 2021).
- Scalone, L.; Cortesi, P.A.; Ciampichini, R.; Belisari, A.; D’Angiolella, L.S.; Cesana, G.; Mantovani, L.G. Italian Population-Based Values of EQ-5D Health States. Value Health 2013, 16, 814–822. [Google Scholar] [CrossRef] [Green Version]
- Osman, A.; Wong, J.L.; Bagge, C.L.; Freedenthal, S.; Gutierrez, P.M.; Lozano, G. The Depression Anxiety Stress Scales-21 (DASS-21): Further Examination of Dimensions, Scale Reliability, and Correlates. J. Clin. Psychol. 2012, 68, 1322–1338. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Novak, M.; Guest, C. Application of a Multidimensional Caregiver Burden Inventory. Gerontologist 1989, 29, 798–803. [Google Scholar] [CrossRef]
- Aoun, S.; Bird, S.; Kristjanson, L.J.; Currow, D. Reliability testing of the FAMCARE-2 scale: Measuring family carer satisfaction with palliative care. Palliat. Med. 2010, 24, 674–681. [Google Scholar] [CrossRef]
- D’Angelo, D.; Punziano, A.C.; Mastroianni, C.; Marzi, A.; Latina, R.; Ghezzi, V.; Piredda, M.; De Marinis, M.G. Translation and Testing of the Italian Version of FAMCARE-2: Measuring Family Caregivers’ Satisfaction With Palliative Care. J. Fam. Nurs. 2017, 23, 252–272. [Google Scholar] [CrossRef]
- Ministero del Lavoro della Salute e delle Politiche Sociali. Classificazione delle Malattie, dei Traumatismi, degli Interventi Chirurgici e delle Procedure Diagnostiche e Terapeutiche-“International Classification of Diseases-9th Revision-Clinical Modification” (Italian version); Istituto Poligrafico e Zecca dello Stato: Roma, Itay, 2007; pp. 1–1116. [Google Scholar]
- Bruera, E.; Kuehn, N.; Miller, M.J.; Selmser, P.; Macmillan, K. The Edmonton Symptom Assessment System (ESAS): A simple method for the assessment of palliative care patients. J. Palliat. Care 1991, 7, 6–9. [Google Scholar] [CrossRef]
- Raisi-Estabragh, Z.; Kobo, O.; Freeman, P.; Petersen, S.E.; Kolman, L.; Miller, R.J.H.; Roguin, A.; Van Spall, H.G.C.; Vuong, J.; Yang, E.H.; et al. Temporal trends in disease-specific causes of cardiovascular mortality amongst patients with cancer in the USA between 1999 and 2019. Eur. Heart J.-Qual. Care Clin. Outcomes 2022, 9, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Narsavage, G.L.; Frick, K.D.; Petitte, T.M. Home-Telemonitoring Lung Cancer Intervention in Appalachia: A Pilot Study. Int. J. Chronic Dis. Ther. 2016, 2, 21–30. [Google Scholar] [PubMed]
- Pang, L.; Liu, Z.; Lin, S.; Liu, Z.; Liu, H.; Mai, Z.; Liu, Z.; Chen, C.; Zhao, Q. The effects of telemedicine on the quality of life of patients with lung cancer: A systematic review and meta-analysis. Ther. Adv. Chronic Dis. 2020, 11, 204062232096159. [Google Scholar] [CrossRef] [PubMed]
- Hennemann-Krause, L.; Lopes, A.J.; Araújo, J.A.; Petersen, E.M.; Nunes, R.A. The assessment of telemedicine to support outpatient palliative care in advanced cancer. Palliat. Support. Care 2015, 13, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Donnem, T.; Ervik, B.; Magnussen, K.; Andersen, S.; Pastow, D.; Andreassen, S.; Nørstad, T.; Helbekkmo, N.; Bremnes, R.M.; Nordoy, T. Bridging the distance: A prospective tele-oncology study in Northern Norway. Support. Care Cancer 2012, 20, 2097–2103. [Google Scholar] [CrossRef]
- Tang, M.; Reddy, A. Telemedicine and Its Past, Present, and Future Roles in Providing Palliative Care to Advanced Cancer Patients. Cancers 2022, 14, 1884. [Google Scholar] [CrossRef] [PubMed]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef] [Green Version]
- Gill, P.; Kaur, J.S.; Rummans, T.; Novotny, P.J.; Sloan, J.A. The hospice patient’s primary caregiver. J. Psychosom. Res. 2003, 55, 445–451. [Google Scholar] [CrossRef]
- Clark, M.M.; Rummans, T.A.; Sloan, J.A.; Jensen, A.; Atherton, P.J.; Frost, M.H.; Richardson, J.W.; Bostwick, J.M.; Johnson, M.E.; Hanson, J.M.; et al. Quality of Life of Caregivers of Patients With Advanced-Stage Cancer. Am. J. Hosp. Palliat. Med. 2006, 23, 185–191. [Google Scholar] [CrossRef]
- Watanabe, S.M.; Fairchild, A.; Pituskin, E.; Borgersen, P.; Hanson, J.; Fassbender, K. Improving access to specialist multidisciplinary palliative care consultation for rural cancer patients by videoconferencing: Report of a pilot project. Support. Care Cancer 2013, 21, 1201–1207. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria |
|---|
| Men and women with solid and hematologic malignancies in an advanced stage, i.e., a locally advanced or metastatic cancer disease that is unlikely to be cured or controlled with treatment. |
| Aged ≥ 18 years. |
| Able to understand the objectives of the study and sign the informed consent. |
| Able to speak and understand the Italian language. |
| Karnofsky Performance Status (KPS) ≥ 50. |
Presence of at least one of the following comorbidities:
The severity of these comorbidities must be relevant to the patient’s clinical profile as expressed in at least one of the following conditions:
|
| Exclusion criteria |
| Patients with a diagnosis of dementia or cognitive impairment hampering the comprehension of the study information and/or signing of informed consent. |
| End-of-life patients. |
| Patients refusing to participate. |
| Timeline | Day 1 | Day 28 | Day 56 |
|---|---|---|---|
| Patient | EQ-5D-3L DASS-21 | EQ-5D-3L DASS-21 | EQ-5D-3L DASS-21 Evaluation of the ButterfLife device * |
| Caregiver | CBI | CBI | CBI FAMCARE-2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ostan, R.; Varani, S.; Giannelli, A.; Malavasi, I.; Pannuti, F.; Pannuti, R.; Biasco, G.; Mattioli, A.V.; on behalf of the ANT Collaborative Group. Distance Monitoring of Advanced Cancer Patients with Impaired Cardiac and Respiratory Function Assisted at Home: A Study Protocol in Italy. J. Clin. Med. 2023, 12, 1922. https://doi.org/10.3390/jcm12051922
Ostan R, Varani S, Giannelli A, Malavasi I, Pannuti F, Pannuti R, Biasco G, Mattioli AV, on behalf of the ANT Collaborative Group. Distance Monitoring of Advanced Cancer Patients with Impaired Cardiac and Respiratory Function Assisted at Home: A Study Protocol in Italy. Journal of Clinical Medicine. 2023; 12(5):1922. https://doi.org/10.3390/jcm12051922
Chicago/Turabian StyleOstan, Rita, Silvia Varani, Andrea Giannelli, Italo Malavasi, Francesco Pannuti, Raffaella Pannuti, Guido Biasco, Anna Vittoria Mattioli, and on behalf of the ANT Collaborative Group. 2023. "Distance Monitoring of Advanced Cancer Patients with Impaired Cardiac and Respiratory Function Assisted at Home: A Study Protocol in Italy" Journal of Clinical Medicine 12, no. 5: 1922. https://doi.org/10.3390/jcm12051922