
Platelet Reactivity and Cardiovascular Mortality Risk in the LURIC Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Participants and Clinical Characterization
2.2. Reagents
2.3. Platelet Reactivity Testing
2.4. Follow-Up and Endpoints
2.5. Statistical Analysis
3. Results
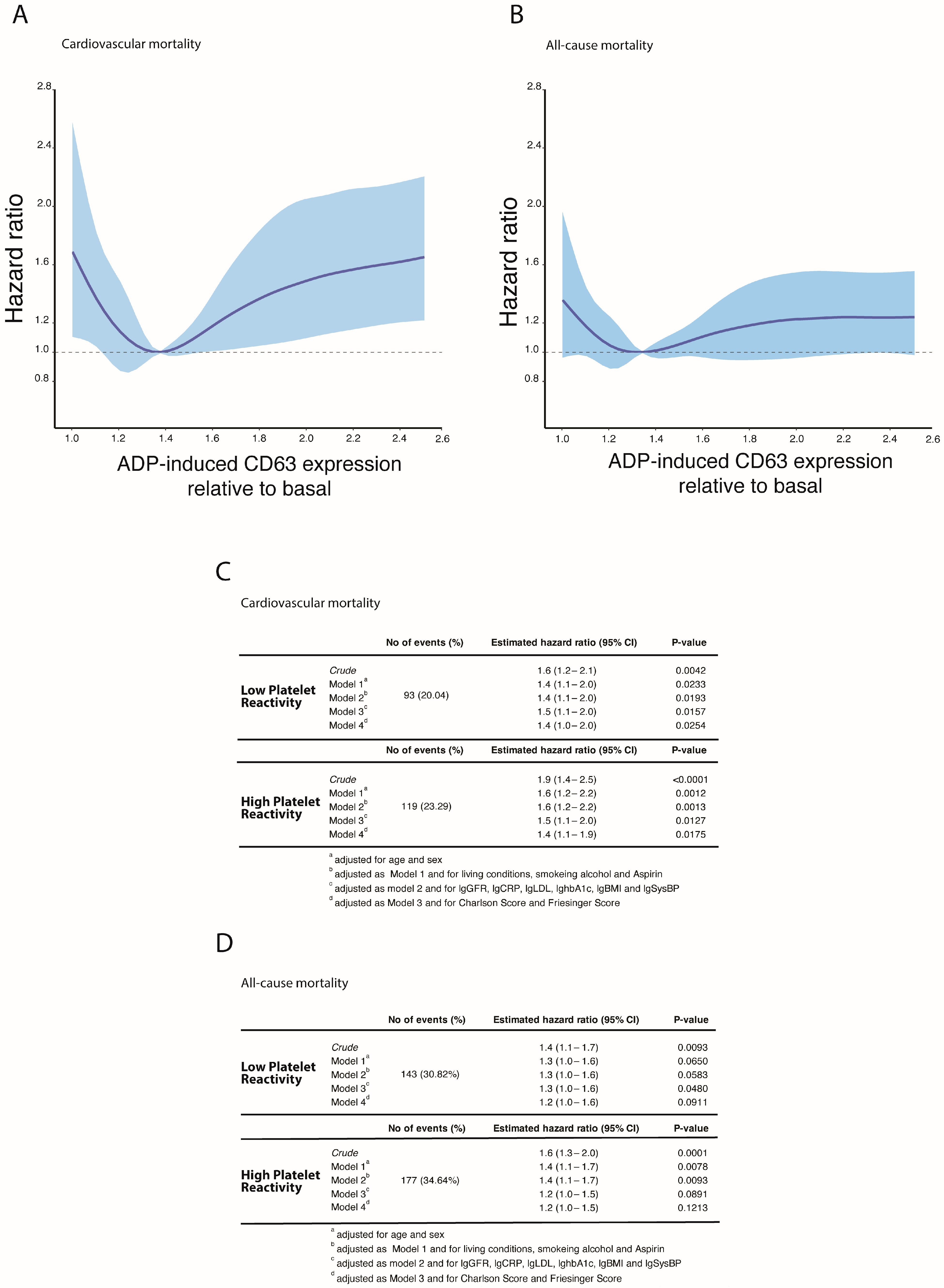
3.1. Platelet Reactivity and Cardiovascular and All-Cause Mortality in the LURIC Study
3.2. Baseline Characteristics in Patients with Abnormal Platelet Reactivity
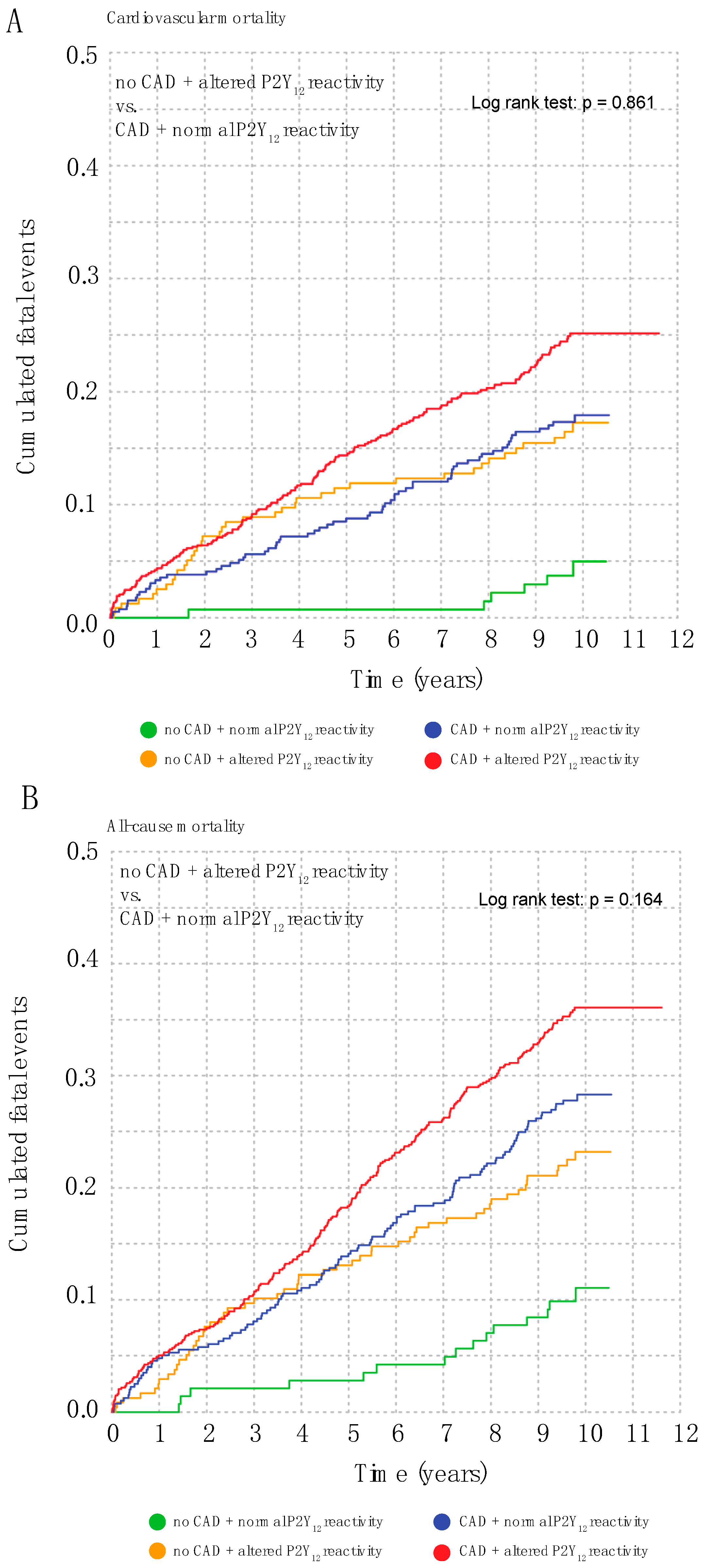
3.3. Abnormal Platelet Reactivity Is a Coronary Artery Disease Risk Equivalent
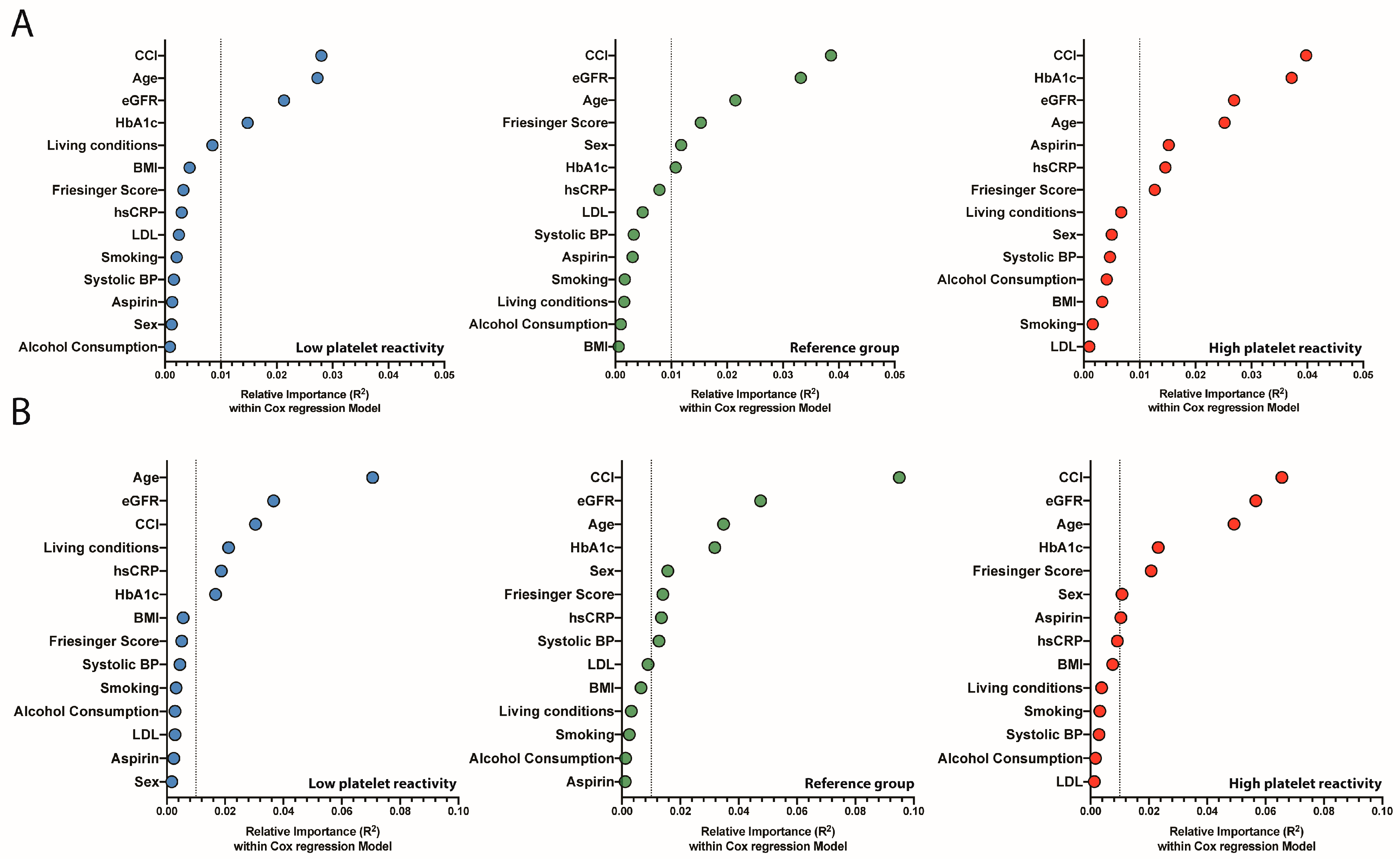
3.4. Relative Importance of Risk Markers in Patients with High- and Low-Platelet Reactivity
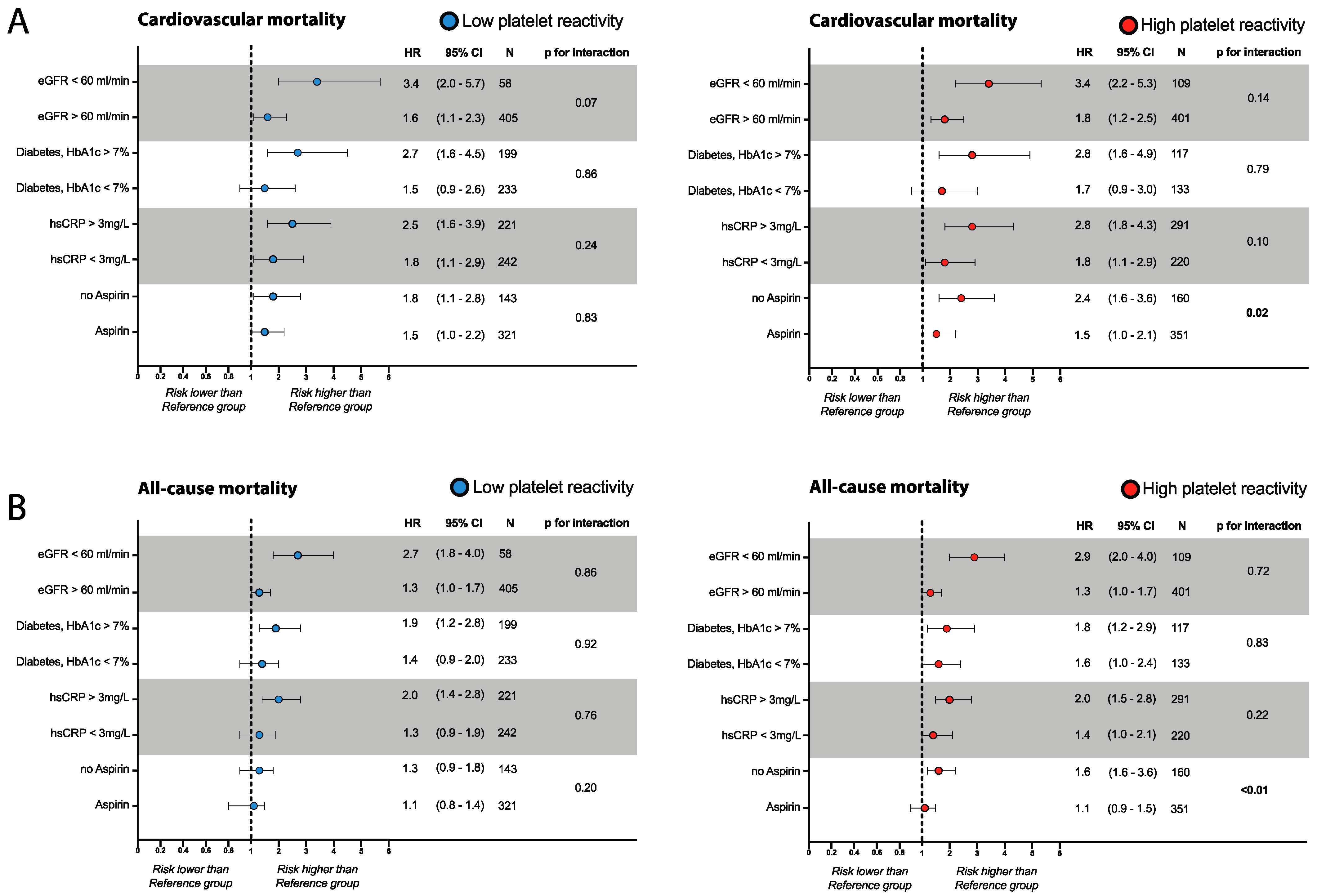
3.5. Risk Assessment in Patients with Abnormal Platelet Reactivity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, L.; Chang, L.; Zhang, Y.; Zhai, L.; Zhang, S.; Qi, Z.; Yan, H.; Yan, Y.; Luo, X.; Zhang, S.; et al. Platelets Express Activated P2Y12 Receptor in Patients With Diabetes Mellitus. Circulation 2017, 136, 817–833. [Google Scholar] [CrossRef] [PubMed]
- Puurunen, M.K.; Hwang, S.J.; Larson, M.G.; Vasan, R.S.; O’Donnell, C.J.; Tofler, G.; Johnson, A.D. ADP Platelet Hyperreactivity Predicts Cardiovascular Disease in the FHS (Framingham Heart Study). J. Am. Heart Assoc. 2018, 7, e008522. [Google Scholar] [CrossRef] [PubMed]
- Frere, C.; Cuisset, T.; Quilici, J.; Camoin, L.; Carvajal, J.; Morange, P.E.; Lambert, M.; Juhan-Vague, I.; Bonnet, J.L.; Alessi, M.C. ADP-induced platelet aggregation and platelet reactivity index VASP are good predictive markers for clinical outcomes in non-ST elevation acute coronary syndrome. Thromb. Haemost. 2007, 98, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.; Kleber, M.E.; Delgado, G.E.; Marz, W.; Andreas, M.; Hellstern, P.; Marx, N.; Schuett, K.A. Trimethylamine N-Oxide and Adenosine Diphosphate-Induced Platelet Reactivity Are Independent Risk Factors for Cardiovascular and All-Cause Mortality. Circ. Res. 2020, 126, 660–662. [Google Scholar] [CrossRef] [PubMed]
- Thaulow, E.; Erikssen, J.; Sandvik, L.; Stormorken, H.; Cohn, P.F. Blood platelet count and function are related to total and cardiovascular death in apparently healthy men. Circulation 1991, 84, 613–617. [Google Scholar] [CrossRef] [Green Version]
- Capodanno, D.; Alfonso, F.; Levine, G.N.; Valgimigli, M.; Angiolillo, D.J. ACC/AHA Versus ESC Guidelines on Dual Antiplatelet Therapy: JACC Guideline Comparison. J. Am. Coll. Cardiol. 2018, 72, 2915–2931. [Google Scholar] [CrossRef]
- Trenk, D.; Stone, G.W.; Gawaz, M.; Kastrati, A.; Angiolillo, D.J.; Muller, U.; Richardt, G.; Jakubowski, J.A.; Neumann, F.J. A randomized trial of prasugrel versus clopidogrel in patients with high platelet reactivity on clopidogrel after elective percutaneous coronary intervention with implantation of drug-eluting stents: Results of the TRIGGER-PCI (Testing Platelet Reactivity In Patients Undergoing Elective Stent Placement on Clopidogrel to Guide Alternative Therapy With Prasugrel) study. J. Am. Coll. Cardiol. 2012, 59, 2159–2164. [Google Scholar] [CrossRef]
- Collet, J.P.; Cuisset, T.; Range, G.; Cayla, G.; Elhadad, S.; Pouillot, C.; Henry, P.; Motreff, P.; Carrie, D.; Boueri, Z.; et al. Bedside monitoring to adjust antiplatelet therapy for coronary stenting. N. Engl. J. Med. 2012, 367, 2100–2109. [Google Scholar] [CrossRef] [Green Version]
- Cayla, G.; Cuisset, T.; Silvain, J.; Leclercq, F.; Manzo-Silberman, S.; Saint-Etienne, C.; Delarche, N.; Bellemain-Appaix, A.; Range, G.; El Mahmoud, R.; et al. Platelet function monitoring to adjust antiplatelet therapy in elderly patients stented for an acute coronary syndrome (ANTARCTIC): An open-label, blinded-endpoint, randomised controlled superiority trial. Lancet 2016, 388, 2015–2022. [Google Scholar] [CrossRef]
- Price, M.J.; Berger, P.B.; Teirstein, P.S.; Tanguay, J.F.; Angiolillo, D.J.; Spriggs, D.; Puri, S.; Robbins, M.; Garratt, K.N.; Bertrand, O.F.; et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: The GRAVITAS randomized trial. JAMA 2011, 305, 1097–1105. [Google Scholar] [CrossRef]
- Montalescot, G.; Range, G.; Silvain, J.; Bonnet, J.L.; Boueri, Z.; Barthelemy, O.; Cayla, G.; Belle, L.; Van Belle, E.; Cuisset, T.; et al. High on-treatment platelet reactivity as a risk factor for secondary prevention after coronary stent revascularization: A landmark analysis of the ARCTIC study. Circulation 2014, 129, 2136–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lattuca, B.; Silvain, J.; Yan, Y.; Pouillot, C.; Cuisset, T.; Cayla, G.; Henry, P.; Diallo, A.; Elhadad, S.; Range, G.; et al. Reasons for the Failure of Platelet Function Testing to Adjust Antiplatelet Therapy: Pharmacodynamic Insights From the ARCTIC Study. Circ. Cardiovasc. Interv. 2019, 12, e007749. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, B.R.; Marz, W.; Boehm, B.O.; Zotz, R.; Hager, J.; Hellstern, P.; Senges, J.; Group, L.S. Rationale and design of the LURIC study—A resource for functional genomics, pharmacogenomics and long-term prognosis of cardiovascular disease. Pharmacogenomics 2001, 2, S1–S73. [Google Scholar] [CrossRef] [PubMed]
- Sitaru, A.G.; Holzhauer, S.; Speer, C.P.; Singer, D.; Obergfell, A.; Walter, U.; Grossmann, R. Neonatal platelets from cord blood and peripheral blood. Platelets 2005, 16, 203–210. [Google Scholar] [CrossRef]
- Heller, G. A measure of explained risk in the proportional hazards model. Biostatistics 2012, 13, 315–325. [Google Scholar] [CrossRef]
- Rawshani, A.; Rawshani, A.; Franzen, S.; Sattar, N.; Eliasson, B.; Svensson, A.M.; Zethelius, B.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2018, 379, 633–644. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; Rose, L.; Buring, J.E.; Cook, N.R. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N. Engl. J. Med. 2002, 347, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Matetzky, S.; Shenkman, B.; Guetta, V.; Shechter, M.; Beinart, R.; Goldenberg, I.; Novikov, I.; Pres, H.; Savion, N.; Varon, D.; et al. Clopidogrel resistance is associated with increased risk of recurrent atherothrombotic events in patients with acute myocardial infarction. Circulation 2004, 109, 3171–3175. [Google Scholar] [CrossRef]
- Lev, E.I.; Patel, R.T.; Maresh, K.J.; Guthikonda, S.; Granada, J.; DeLao, T.; Bray, P.F.; Kleiman, N.S. Aspirin and clopidogrel drug response in patients undergoing percutaneous coronary intervention: The role of dual drug resistance. J. Am. Coll. Cardiol. 2006, 47, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Gurbel, P.A.; Becker, R.C.; Mann, K.G.; Steinhubl, S.R.; Michelson, A.D. Platelet function monitoring in patients with coronary artery disease. J. Am. Coll. Cardiol. 2007, 50, 1822–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuisset, T.; Deharo, P.; Quilici, J.; Johnson, T.W.; Deffarges, S.; Bassez, C.; Bonnet, G.; Fourcade, L.; Mouret, J.P.; Lambert, M.; et al. Benefit of switching dual antiplatelet therapy after acute coronary syndrome: The TOPIC (timing of platelet inhibition after acute coronary syndrome) randomized study. Eur. Heart J. 2017, 38, 3070–3078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibbing, D.; Aradi, D.; Jacobshagen, C.; Gross, L.; Trenk, D.; Geisler, T.; Orban, M.; Hadamitzky, M.; Merkely, B.; Kiss, R.G.; et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): A randomised, open-label, multicentre trial. Lancet 2017, 390, 1747–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Witzenbichler, B.; Weisz, G.; Rinaldi, M.J.; Neumann, F.J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; Duffy, P.L.; Mazzaferri, E.; et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): A prospective multicentre registry study. Lancet 2013, 382, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Blair, P.; Flaumenhaft, R. Platelet alpha-granules: Basic biology and clinical correlates. Blood Rev. 2009, 23, 177–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishibori, M.; Cham, B.; McNicol, A.; Shalev, A.; Jain, N.; Gerrard, J.M. The protein CD63 is in platelet dense granules, is deficient in a patient with Hermansky-Pudlak syndrome, and appears identical to granulophysin. J. Clin. Investig. 1993, 91, 1775–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blann, A.D.; Nadar, S.K.; Lip, G.Y. The adhesion molecule P-selectin and cardiovascular disease. Eur. Heart J. 2003, 24, 2166–2179. [Google Scholar] [CrossRef] [Green Version]
- Dole, V.S.; Bergmeier, W.; Patten, I.S.; Hirahashi, J.; Mayadas, T.N.; Wagner, D.D. PSGL-1 regulates platelet P-selectin-mediated endothelial activation and shedding of P-selectin from activated platelets. Thromb. Haemost. 2007, 98, 806–812. [Google Scholar] [CrossRef] [Green Version]
- Marquardt, L.; Ruf, A.; Mansmann, U.; Winter, R.; Schuler, M.; Buggle, F.; Mayer, H.; Grau, A.J. Course of platelet activation markers after ischemic stroke. Stroke 2002, 33, 2570–2574. [Google Scholar] [CrossRef] [Green Version]
- Campo, G.; Parrinello, G.; Ferraresi, P.; Lunghi, B.; Tebaldi, M.; Miccoli, M.; Marchesini, J.; Bernardi, F.; Ferrari, R.; Valgimigli, M. Prospective evaluation of on-clopidogrel platelet reactivity over time in patients treated with percutaneous coronary intervention relationship with gene polymorphisms and clinical outcome. J. Am. Coll. Cardiol. 2011, 57, 2474–2483. [Google Scholar] [CrossRef] [Green Version]
- Sibbing, D.; Schulz, S.; Braun, S.; Morath, T.; Stegherr, J.; Mehilli, J.; Schomig, A.; von Beckerath, N.; Kastrati, A. Antiplatelet effects of clopidogrel and bleeding in patients undergoing coronary stent placement. J. Thromb. Haemost. 2010, 8, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Gurbel, P.A.; Bliden, K.P.; Navickas, I.A.; Mahla, E.; Dichiara, J.; Suarez, T.A.; Antonino, M.J.; Tantry, U.S.; Cohen, E. Adenosine diphosphate-induced platelet-fibrin clot strength: A new thrombelastographic indicator of long-term poststenting ischemic events. Am. Heart J. 2010, 160, 346–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonello, L.; Mancini, J.; Pansieri, M.; Maillard, L.; Rossi, P.; Collet, F.; Jouve, B.; Wittenberg, O.; Laine, M.; Michelet, P.; et al. Relationship between post-treatment platelet reactivity and ischemic and bleeding events at 1-year follow-up in patients receiving prasugrel. J. Thromb. Haemost. 2012, 10, 1999–2005. [Google Scholar] [CrossRef] [PubMed]
- Group, A.S.C.; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar] [CrossRef]
- McNeil, J.J.; Nelson, M.R.; Woods, R.L.; Lockery, J.E.; Wolfe, R.; Reid, C.M.; Kirpach, B.; Shah, R.C.; Ives, D.G.; Storey, E.; et al. Effect of Aspirin on All-Cause Mortality in the Healthy Elderly. N. Engl. J. Med. 2018, 379, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Brotons, C.; Coppolecchia, R.; Cricelli, C.; Darius, H.; Gorelick, P.B.; Howard, G.; Pearson, T.A.; Rothwell, P.M.; Ruilope, L.M.; et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): A randomised, double-blind, placebo-controlled trial. Lancet 2018, 392, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Unstable angina. A classification. Circulation 1989, 80, 410–414. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | Low P2Y12 Reactivity | Reference Group | High P2Y12 Reactivity | p Value |
|---|---|---|---|---|---|
| (n = 1520) | (n = 464) | (n = 545) | (n = 511) | ||
| ADP-induced CD63 expression (relative to basal) | <1.22 | 1.22–1.50 | >1.50 | ||
| Age (Years) | 64.05 (56.92–71.02) | 63.65 (57.15–71.05) | 63.5 (55.28–69.98) | 65.79 (58.32–71.91) | 0.0001 |
| Sex (male) | 1037 (68.22%) | 325 (70.04%) | 382 (70.09%) | 330 (64.58%) | 0.0975 |
| Body Mass Index | 27.2 (24.87–29.88) | 27.02 (25.09–29.96) | 27.26 (24.74–29.57) | 27.4 (24.71–30.41) | 0.6664 |
| Cardiovascular risk factors | |||||
| Hypertension | 868 (57.11%) | 256 (55.17%) | 311 (57.06%) | 301 (58.9%) | 0.4993 |
| Hypercholesterolemia | 1043 (68.62%) | 316 (68.1%) | 372 (68.26%) | 355 (69.47%) | 0.8767 |
| Diabetes mellitus | 648 (42.63%) | 182 (39.22%) | 215 (39.45%) | 251 (49.12%) | 0.0014 |
| Chronic kidney disease | 223 (15.33%) | 57 (12.72%) | 61 (11.75%) | 105 (21.52%) | <0.0001 |
| Family History of premature MI | 163 (10.72%) | 59 (12.72%) | 63 (11.56%) | 41 (8.02%) | 0.0405 |
| Premature MI | 254 (16.71%) | 71 (15.3%) | 106 (19.45%) | 77 (15.07%) | 0.1065 |
| Alcohol intake | 912 (60%) | 300 (64.66%) | 315 (57.8%) | 297 (58.12%) | 0.0479 |
| Smoking | 340(22.1%) | 110(23.7%) | 118(21.7%) | 109(21.3%) | 0.6290 |
| Scores | |||||
| Friesinger Score | 5 (2–8) | 5 (2–8) | 4 (1–8) | 5 (2–8) | 0.1994 |
| Framingham Score | 15 (13–17) | 15 (13–16) | 15 (12–16) | 15 (14–17) | 0.0002 |
| Marschner Score | 0.14 (0.1–0.2) | 0.14 (0.09–0.2) | 0.15 (0.1–0.21) | 0.14 (0.1–0.19) | 0.2498 |
| Charlson Score | 1 (1–2) | 1 (1–2) | 1 (1–2) | 2 (1–3) | 0.0002 |
| Death | |||||
| All-cause death | 452 (29.74%) | 143 (30.82%) | 132 (24.22%) | 177 (34.64%) | 0.0008 |
| Cardiovascular death | 284 (18.68%) | 93 (20.04%) | 72 (13.21%) | 119 (23.29%) | 0.0001 |
| Medical History | |||||
| Acute Coronary Syndrom at baseline | 410 (27.61%) | 128 (28.38%) | 139 (26.18%) | 143 (28.43%) | 0.6560 |
| Coronary artery disease | 1141 (75.07%) | 347 (74.78%) | 403 (73.94%) | 391 (76.52%) | 0.6222 |
| Coronary artery bypass graft | 184 (12.11%) | 50 (10.78%) | 66 (12.11%) | 68 (13.31%) | 0.4761 |
| History of PTCA | 335 (22.04%) | 110 (23.71%) | 114 (20.92%) | 111 (21.72%) | 0.5526 |
| Peripheral artery disease | 114 (7.5%) | 37 (7.97%) | 36 (6.61%) | 41 (8.02%) | 0.6152 |
| Stroke | 120 (7.89%) | 35 (7.54%) | 37 (6.79%) | 48 (9.39%) | 0.2819 |
| Heartfailure | 500(32.6%) | 158(34.1%) | 178(32.7%) | 160(31.3%) | 0.6590 |
| HFpEF | 264(17.2%) | 74/15.9%) | 78(14.3%) | 82(16.0%) | 0.6750 |
| HFrEF | 236(15.4%) | 84(18.1%) | 100(18.3%) | 78(15.3%) | 0.3430 |
| Laboratory parameters | |||||
| Platelets (nL) | 225 (186–270) | 223 (184–266) | 227 (189–268) | 226 (185–273.5) | 0.6755 |
| Mean platelet volume (fl) | 8.9 (8.2–9.6) | 9 (8.2–9.7) | 8.9 (8.2–9.6) | 8.8 (8.25–9.6) | 0.3991 |
| High sensitive CRP (mg/dL) | 3.08 (1.29–7.82) | 2.86 (1.24–6.79) | 2.7 (1.18–7.58) | 3.83 (1.63–9.04) | 0.0002 |
| Glycosylated hemoglobin (%) | 6.2 (5.8–6.8) | 6.1 (5.75–6.7) | 6.2 (5.8–6.7) | 6.3 (5.8–6.97) | 0.0116 |
| Glomerular Filtration Rate (mL/min/1.73m2) | 81.97 (67.64–94.75) | 83.15 (69.21–97.03) | 83.61 (70.57–97.18) | 78.26 (61.96–89.5) | <0.0001 |
| Triglycerides (mg/dL) | 145 (109–200.5) | 150 (112–209) | 143 (108–196) | 143 (110.5–198.5) | 0.1380 |
| LDL Cholesterol (mg/dL) | 112 (90–135) | 112 (93–136) | 113 (92–138) | 109 (88–132) | 0.0865 |
| HDL Cholesterol (mg/dL) | 38 (31–45) | 38 (31–45) | 38 (32–45) | 38 (31–45) | 0.7093 |
| Baseline Medication | All Patients | Low P2Y12 Reactivity | Reference Group | High P2Y12 Reactivity | p Value |
|---|---|---|---|---|---|
| (n = 1520) | (n = 464) | (n = 545) | (n = 511) | ||
| Aspirin | 1046 (68.82%) | 321 (69.18%) | 374 (68.62%) | 351 (68.69%) | 0.9799 |
| Phenprocoumon/Warfarin | 108 (7.11%) | 37 (7.97%) | 36 (6.61%) | 35 (6.85%) | 0.6794 |
| Statin | 727 (47.83%) | 221 (47.63%) | 259 (47.52%) | 247 (48.34%) | 0.9635 |
| Calcium Channel blocker | 77 (5.07%) | 13 (2.8%) | 25 (4.59%) | 39 (7.63%) | 0.0024 |
| ACEi/ARB | 809 (53.22%) | 236 (50.86%) | 290 (53.21%) | 283 (55.38%) | 0.3724 |
| Diuretic | 454 (29.87%) | 129 (27.8%) | 148 (27.16%) | 177 (34.64%) | 0.0159 |
| Beta Blocker | 934 (61.45%) | 286 (61.64%) | 332 (60.92%) | 316 (61.84%) | 0.9572 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berger, M.; Dressel, A.; Kleber, M.E.; März, W.; Hellstern, P.; Marx, N.; Schütt, K. Platelet Reactivity and Cardiovascular Mortality Risk in the LURIC Study. J. Clin. Med. 2023, 12, 1913. https://doi.org/10.3390/jcm12051913
Berger M, Dressel A, Kleber ME, März W, Hellstern P, Marx N, Schütt K. Platelet Reactivity and Cardiovascular Mortality Risk in the LURIC Study. Journal of Clinical Medicine. 2023; 12(5):1913. https://doi.org/10.3390/jcm12051913
Chicago/Turabian StyleBerger, Martin, Alexander Dressel, Marcus E. Kleber, Winfried März, Peter Hellstern, Nikolaus Marx, and Katharina Schütt. 2023. "Platelet Reactivity and Cardiovascular Mortality Risk in the LURIC Study" Journal of Clinical Medicine 12, no. 5: 1913. https://doi.org/10.3390/jcm12051913