
Systematic Review and Meta-Analysis of Observational Studies on the Effectiveness and Safety of Ustekinumab among Patients with Inflammatory Bowel Disease in Eastern and Western Countries
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategies
2.2. Eligibility Criteria and Study Selection
2.3. Outcome Measures
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
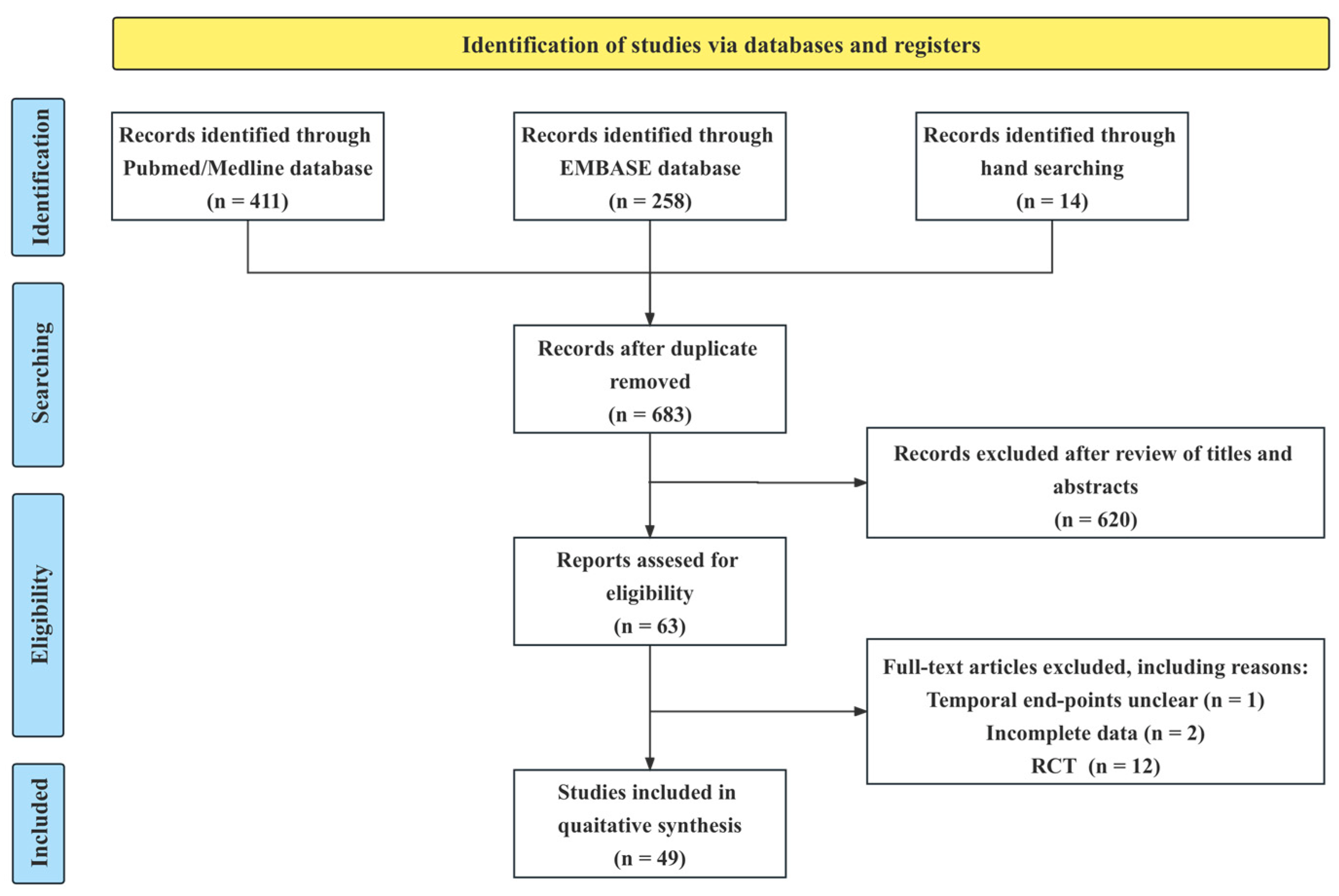
3.1. Study Selection and Characteristics
3.2. Clinical Outcomes at Induction
3.3. Clinical and Endoscopic Outcomes at Maintenance
3.4. Clinical Outcomes by Geographic Location
3.5. Safety
3.6. Clinical Remission of Biologics-Naive and Biologics-Experienced Patients
3.7. Publication Bias and Subgroup Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O’Brien, C.D.; Zhang, H.; Johanns, J.; Adedokun, O.J.; Li, K.; Peyrin-Biroulet, L.; Van Assche, G.; et al. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1201–1214. [Google Scholar] [CrossRef]
- Eberl, A.; Hallinen, T.; Af Bjorkesten, C.G.; Heikkinen, M.; Hirsi, E.; Kellokumpu, M.; Koskinen, I.; Moilanen, V.; Nielsen, C.; Nuutinen, H.; et al. Ustekinumab for Crohn’s disease: A nationwide real-life cohort study from Finland (FINUSTE). Scand. J. Gastroenterol. 2019, 54, 718–725. [Google Scholar] [CrossRef]
- Pugliese, D.; Daperno, M.; Fiorino, G.; Savarino, E.; Mosso, E.; Biancone, L.; Testa, A.; Sarpi, L.; Cappello, M.; Bodini, G.; et al. Real-life effectiveness of ustekinumab in inflammatory bowel disease patients with concomitant psoriasis or psoriatic arthritis: An IG-IBD study. Dig. Liver Dis. 2019, 51, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Engel, T.; Yung, D.E.; Ma, C.; Pariente, B.; Wils, P.; Eliakim, R.; Ungar, B.; Ben-Horin, S.; Kopylov, U. Effectiveness and safety of Ustekinumab for Crohn’s disease; systematic review and pooled analysis of real-world evidence. Dig. Liver Dis. 2019, 51, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Fedorak, R.N.; Kaplan, G.G.; Dieleman, L.A.; Devlin, S.M.; Stern, N.; Kroeker, K.I.; Seow, C.H.; Leung, Y.; Novak, K.L.; et al. Clinical, endoscopic and radiographic outcomes with ustekinumab in medically-refractory Crohn’s disease: Real world experience from a multicentre cohort. Aliment. Pharmacol. Ther. 2017, 45, 1232–1243. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Best, W.R.; Becktel, J.M.; Singleton, J.W.; Kern, F., Jr. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology 1976, 70, 439–444. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef] [PubMed]
- Daperno, M.; D’Haens, G.; Van Assche, G.; Baert, F.; Bulois, P.; Maunoury, V.; Sostegni, R.; Rocca, R.; Pera, A.; Gevers, A.; et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: The SES-CD. Gastrointest. Endosc. 2004, 60, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Alsoud, D.; De Hertogh, G.; Compernolle, G.; Tops, S.; Sabino, J.; Ferrante, M.; Thomas, D.; Vermeire, S.; Verstockt, B. Real-world Endoscopic and Histological Outcomes Are Correlated with Ustekinumab Exposure in Patients with Ulcerative Colitis. J. Crohn’s Colitis 2022, 16, 1562–1570. [Google Scholar] [CrossRef] [PubMed]
- Huntington, S.P. The Clash of Civilizations and the Remaking of World Order; Simon & Schuster: New York, NY, USA, 1996; 367p. [Google Scholar]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Kopylov, U.; Hanzel, J.; Liefferinckx, C.; De Marco, D.; Imperatore, N.; Plevris, N.; Baston-Rey, I.; Harris, R.J.; Truyens, M.; Domislovic, V.; et al. Effectiveness of ustekinumab dose escalation in Crohn’s disease patients with insufficient response to standard-dose subcutaneous maintenance therapy. Aliment. Pharmacol. Ther. 2020, 52, 135–142. [Google Scholar] [CrossRef]
- Khorrami, S.; Ginard, D.; Marin-Jimenez, I.; Chaparro, M.; Sierra, M.; Aguas, M.; Sicilia, B.; Garcia-Sanchez, V.; Suarez, C.; Villoria, A.; et al. Ustekinumab for the Treatment of Refractory Crohn’s Disease: The Spanish Experience in a Large Multicentre Open-label Cohort. Inflamm. Bowel Dis. 2016, 22, 1662–1669. [Google Scholar] [CrossRef]
- Iborra, M.; Beltran, B.; Fernandez-Clotet, A.; Iglesias-Flores, E.; Navarro, P.; Rivero, M.; Gutierrez, A.; Sierra-Ausin, M.; Mesonero, F.; Ferreiro-Iglesias, R.; et al. Real-world long-term effectiveness of ustekinumab in Crohn’s disease: Results from the ENEIDA registry. Aliment. Pharmacol. Ther. 2020, 52, 1017–1030. [Google Scholar] [CrossRef]
- Iborra, M.; Beltran, B.; Fernandez-Clotet, A.; Gutierrez, A.; Antolin, B.; Huguet, J.M.; De Francisco, R.; Merino, O.; Carpio, D.; Garcia-Lopez, S.; et al. Real-world short-term effectiveness of ustekinumab in 305 patients with Crohn’s disease: Results from the ENEIDA registry. Aliment. Pharmacol. Ther. 2019, 50, 278–288. [Google Scholar] [CrossRef]
- Bermejo, F.; Jimenez, L.; Algaba, A.; Vela, M.; Bastida, G.; Merino, O.; Lopez-Garcia, A.; Melcarne, L.; Rodriguez-Lago, I.; de la Maza, S.; et al. Re-induction With Intravenous Ustekinumab in Patients With Crohn’s Disease and a Loss of Response to This Therapy. Inflamm. Bowel Dis. 2022, 28, 41–47. [Google Scholar] [CrossRef]
- Hoffmann, P.; Krisam, J.; Wehling, C.; Kloeters-Plachky, P.; Leopold, Y.; Belling, N.; Gauss, A. Ustekinumab: "Real-world" outcomes and potential predictors of nonresponse in treatment-refractory Crohn’s disease. World J. Gastroenterol. 2019, 25, 4481–4492. [Google Scholar] [CrossRef]
- Kubesch, A.; Rueter, L.; Farrag, K.; Krause, T.; Stienecker, K.; Hausmann, J.; Filmann, N.; Dignass, A.; Stein, J.; Blumenstein, I. Short and Long-Term Effectiveness of Ustekinumab in Patients with Crohn’s Disease: Real-World Data from a German IBD Cohort. J. Clin. Med. 2019, 8, 2140. [Google Scholar] [CrossRef] [Green Version]
- Thomann, A.K.; Schulte, L.A.; Globig, A.M.; Hoffmann, P.; Klag, T.; Itzel, T.; Teufel, A.; Schreiner, R.; Scheffe, N.; Ebert, M.P.; et al. Ustekinumab serum concentrations are associated with clinical outcomes in Crohn’s disease-a regional multi-center pilot study. Z. Für Gastroenterol. 2020, 58, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Ollech, J.E.; Normatov, I.; Peleg, N.; Wang, J.; Patel, S.A.; Rai, V.; Yi, Y.; Singer, J.; Dalal, S.R.; Sakuraba, A.; et al. Effectiveness of Ustekinumab Dose Escalation in Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2021, 19, 104–110. [Google Scholar] [CrossRef]
- Dalal, R.S.; Njie, C.; Marcus, J.; Gupta, S.; Allegretti, J.R. Predictors of Ustekinumab Failure in Crohn’s Disease After Dose Intensification. Inflamm. Bowel Dis. 2021, 27, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Weaver, K.N.; Gregory, M.; Syal, G.; Hoversten, P.; Hicks, S.B.; Patel, D.; Christophi, G.; Beniwal-Patel, P.; Isaacs, K.L.; Raffals, L.; et al. Ustekinumab Is Effective for the Treatment of Crohn’s Disease of the Pouch in a Multicenter Cohort. Inflamm. Bowel Dis. 2019, 25, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.A.; Yadav, A.; Perry, C.; Su, L.; Akanbi, O.; Kudaravalli, P.; Tripathi, N.; Hashim, M.A.; Abdelsalam, M.; Hussein, M.; et al. Ustekinumab dose escalation improves clinical responses in refractory Crohn’s disease. Therap. Adv. Gastroenterol. 2020, 13, 1756284820959245. [Google Scholar] [CrossRef]
- Garg, R.; Aggarwal, M.; Butler, R.; Achkar, J.P.; Lashner, B.; Philpott, J.; Cohen, B.; Qazi, T.; Rieder, F.; Regueiro, M.; et al. Real-World Effectiveness and Safety of Ustekinumab in Elderly Crohn’s Disease Patients. Dig. Dis. Sci. 2022, 67, 3138–3147. [Google Scholar] [CrossRef]
- Forss, A.; Clements, M.; Myrelid, P.; Strid, H.; Soderman, C.; Wagner, A.; Andersson, D.; Hjelm, F.; Olen, O.; et al.; PROSE SWIBREG Study Group Prospective observational study on Stelara (ustekinumab) assessing effectiveness in Crohn’s disease (PROSE): A 16-week follow-up. Scand. J. Gastroenterol. 2021, 56, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Plevris, N.; Fulforth, J.; Siakavellas, S.; Robertson, A.; Hall, R.; Tyler, A.; Jenkinson, P.W.; Campbell, I.; Chuah, C.S.; Kane, C.; et al. Real-world effectiveness and safety of ustekinumab for the treatment of Crohn’s disease: The Scottish ustekinumab cohort. J. Gastroenterol. Hepatol. 2021, 36, 2067–2075. [Google Scholar] [CrossRef]
- Harris, R.J.; McDonnell, M.; Young, D.; Bettey, M.; Downey, L.; Pigott, L.; Felwick, R.; Gwiggner, M.; Cummings, J.R.F. Early real-world effectiveness of ustekinumab for Crohn’s disease. Frontline Gastroenterol. 2020, 11, 111–116. [Google Scholar] [CrossRef]
- Ten Bokkel Huinink, S.; Biemans, V.; Duijvestein, M.; Pierik, M.; Hoentjen, F.; West, R.L.; van der Woude, C.J.; de Vries, A.C. Re-induction with intravenous Ustekinumab after secondary loss of response is a valid optimization strategy in Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2021, 33, e783–e788. [Google Scholar] [CrossRef] [PubMed]
- Biemans, V.B.C.; van der Meulen-de Jong, A.E.; van der Woude, C.J.; Lowenberg, M.; Dijkstra, G.; Oldenburg, B.; de Boer, N.K.H.; van der Marel, S.; Bodelier, A.G.L.; Jansen, J.M.; et al. Ustekinumab for Crohn’s Disease: Results of the ICC Registry, a Nationwide Prospective Observational Cohort Study. J. Crohn’s Colitis 2020, 14, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Straatmijer, T.; Biemans, V.B.C.; Hoentjen, F.; de Boer, N.K.H.; Bodelier, A.G.L.; Dijkstra, G.; van Dop, W.A.; Haans, J.J.L.; Jansen, J.M.; Maljaars, P.W.J.; et al. Ustekinuma b for Crohn’s Disease: Two-Year Results of the Initiative on Crohn and Colitis (ICC) Registry, a Nationwide Prospective Observational Cohort Study. J. Crohn’s Colitis 2021, 15, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- Wils, P.; Bouhnik, Y.; Michetti, P.; Flourie, B.; Brixi, H.; Bourrier, A.; Allez, M.; Duclos, B.; Serrero, M.; Buisson, A.; et al. Long-term efficacy and safety of ustekinumab in 122 refractory Crohn’s disease patients: A multicentre experience. Aliment. Pharmacol. Ther. 2018, 47, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Wils, P.; Bouhnik, Y.; Michetti, P.; Flourie, B.; Brixi, H.; Bourrier, A.; Allez, M.; Duclos, B.; Grimaud, J.C.; Buisson, A.; et al. Subcutaneous Ustekinumab Provides Clinical Benefit for Two-Thirds of Patients With Crohn’s Disease Refractory to Anti-Tumor Necrosis Factor Agents. Clin. Gastroenterol. Hepatol. 2016, 14, 242–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battat, R.; Kopylov, U.; Bessissow, T.; Bitton, A.; Cohen, A.; Jain, A.; Martel, M.; Seidman, E.; Afif, W. Association Between Ustekinumab Trough Concentrations and Clinical, Biomarker, and Endoscopic Outcomes in Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2017, 15, 1427–1434. [Google Scholar] [CrossRef]
- Greenup, A.J.; Rosenfeld, G.; Bressler, B. Ustekinumab use in Crohn’s disease: A Canadian tertiary care centre experience. Scand. J. Gastroenterol. 2017, 52, 1354–1359. [Google Scholar] [CrossRef]
- Ma, C.; Fedorak, R.N.; Kaplan, G.G.; Dieleman, L.A.; Devlin, S.M.; Stern, N.; Kroeker, K.I.; Seow, C.H.; Leung, Y.; Novak, K.L.; et al. Long-term Maintenance of Clinical, Endoscopic, and Radiographic Response to Ustekinumab in Moderate-to-Severe Crohn’s Disease: Real-world Experience from a Multicenter Cohort Study. Inflamm. Bowel Dis. 2017, 23, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Liefferinckx, C.; Verstockt, B.; Gils, A.; Noman, M.; Van Kemseke, C.; Macken, E.; De Vos, M.; Van Moerkercke, W.; Rahier, J.F.; Bossuyt, P.; et al. Long-term Clinical Effectiveness of Ustekinumab in Patients with Crohn’s Disease Who Failed Biologic Therapies: A National Cohort Study. J. Crohn’s Colitis 2019, 13, 1401–1409. [Google Scholar] [CrossRef]
- Tursi, A.; Mocci, G.; Cuomo, A.; Allegretta, L.; Aragona, G.; Colucci, R.; Della Valle, N.; Ferronato, A.; Forti, G.; Gaiani, F.; et al. Real-life efficacy and safety of Ustekinumab as second- or third-line therapy in Crohn’s disease: Results from a large Italian cohort study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2099–2108. [Google Scholar] [CrossRef]
- Hanzel, J.; Zdovc, J.; Kurent, T.; Sever, N.; Javornik, K.; Tuta, K.; Kozelj, M.; Smrekar, N.; Novak, G.; Stabuc, B.; et al. Peak Concentrations of Ustekinumab After Intravenous Induction Therapy Identify Patients With Crohn’s Disease Likely to Achieve Endoscopic and Biochemical Remission. Clin. Gastroenterol. Hepatol. 2021, 19, 111–118. [Google Scholar] [CrossRef]
- Yao, J.; Yu, Q.; Chen, Y.; Guo, H.; Zhi, M.; Zhang, M. Analysis of the short-term efficacy of ustekinumab for intractable Crohn′s disease: A multicenter retrospective observational study. Chin. J. Inflamm. Bowel Dis. 2021, 5, 151–155. [Google Scholar]
- Yao, J.Y.; Zhang, M.; Wang, W.; Peng, X.; Zhao, J.Z.; Liu, T.; Li, Z.W.; Sun, H.T.; Hu, P.; Zhi, M. Ustekinumab trough concentration affects clinical and endoscopic outcomes in patients with refractory Crohn’s disease: A Chinese real-world study. BMC Gastroenterol. 2021, 21, 380. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Zhu, X.; Shao, B.; Liu, R.; Li, Z.; Wu, L.; Chen, J.; Cao, Q. Reasons and Factors Contributing to Chinese Patients’ Preference for Ustekinumab in Crohn’s Disease: A Multicenter Cross-Sectional Study. Front. Pharmacol. 2021, 12, 736149. [Google Scholar] [CrossRef]
- Yokoyama, S.; Asano, T.; Nagano, K.; Tsuchiya, H.; Takagishi, M.; Tsujioka, S.; Miura, N.; Matsumoto, T. Safety and effectiveness of ustekinumab in Crohn’s disease: Interim results of post-marketing surveillance in Japan. J. Gastroenterol. Hepatol. 2021, 36, 3069–3076. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, K.; Kawamoto, A.; Hibiya, S.; Suzuki, K.; Fujii, T.; Motobayashi, M.; Shimizu, H.; Nagahori, M.; Saito, E.; Okamoto, R.; et al. Higher concentrations of cytokine blockers are needed to obtain small bowel mucosal healing during maintenance therapy in Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 54, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Watanabe, K.; Kojima, K.; Koshiba, R.; Fujimoto, K.; Sato, T.; Kawai, M.; Kamikozuru, K.; Yokoyama, Y.; Hida, N.; et al. Efficacies and Related Issues of Ustekinumab in Japanese Patients with Crohn’s Disease: A Preliminary Study. Digestion 2020, 101, 53–59. [Google Scholar] [CrossRef]
- Hyun, H.K.; Zhang, H.S.; Yu, J.; Kang, E.A.; Park, J.; Park, S.J.; Park, J.J.; Kim, T.I.; Kim, W.H.; Cheon, J.H. Comparative effectiveness of second-line biological therapies for ulcerative colitis and Crohn’s disease in patients with prior failure of anti-tumour necrosis factor treatment. BMC Gastroenterol. 2022, 22, 143. [Google Scholar] [CrossRef] [PubMed]
- Altuwaijri, M.; Hakami, L.; Alharbi, O.; Almadi, M.; Alshankiti, S.; Aljebreen, A.; Azzam, N. The Long-Term Clinical Effectiveness of Ustekinumab in Antitumor Necrosis Factor-Experienced Crohn’s Disease Patients. Cureus 2022, 14, e28536. [Google Scholar] [CrossRef]
- Chaparro, M.; Garre, A.; Iborra, M.; Sierra-Ausin, M.; Barreiro-de Acosta, M.; Fernandez-Clotet, A.; de Castro, L.; Bosca-Watts, M.; Casanova, M.J.; Lopez-Garcia, A.; et al. Effectiveness and Safety of Ustekinumab in Ulcerative Colitis: Real-world Evidence from the ENEIDA Registry. J. Crohn’s Colitis 2021, 15, 1846–1851. [Google Scholar] [CrossRef]
- Amiot, A.; Filippi, J.; Abitbol, V.; Cadiot, G.; Laharie, D.; Serrero, M.; Altwegg, R.; Bouhnik, Y.; Peyrin-Biroulet, L.; Gilletta, C.; et al. Effectiveness and safety of ustekinumab induction therapy for 103 patients with ulcerative colitis: A GETAID multicentre real-world cohort study. Aliment. Pharmacol. Ther. 2020, 51, 1039–1046. [Google Scholar] [CrossRef] [Green Version]
- Fumery, M.; Filippi, J.; Abitbol, V.; Biron, A.; Laharie, D.; Serrero, M.; Altwegg, R.; Bouhnik, Y.; Peyrin-Biroulet, L.; Gilletta, C.; et al. Effectiveness and safety of ustekinumab maintenance therapy in 103 patients with ulcerative colitis: A GETAID cohort study. Aliment. Pharmacol. Ther. 2021, 54, 944–951. [Google Scholar] [CrossRef]
- Ochsenkuhn, T.; Tillack, C.; Szokodi, D.; Janelidze, S.; Schnitzler, F. Clinical outcomes with ustekinumab as rescue treatment in therapy-refractory or therapy-intolerant ulcerative colitis. United Eur. Gastroenterol. J. 2020, 8, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiappetta, M.F.; Viola, A.; Mastronardi, M.; Turchini, L.; Carparelli, S.; Orlando, A.; Biscaglia, G.; Miranda, A.; Guida, L.; Costantino, G.; et al. One-year effectiveness and safety of ustekinumab in ulcerative colitis: A multicenter real-world study from Italy. Expert Opin. Biol. Ther. 2021, 21, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Dalal, R.S.; Esckilsen, S.; Barnes, E.L.; Pruce, J.C.; Marcus, J.; Allegretti, J.R. Predictors and Outcomes of Ustekinumab Dose Intensification in Ulcerative Colitis: A Multicenter Cohort Study. Clin. Gastroenterol. Hepatol. 2022, 20, 2399–2401. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.Z.S.; Axelrad, J.; Chang, S.; Hudesman, D. P087 Real-world effectiveness of ustekinumab in ulcerative colitis. Inflam. Bowel Dis. 2020, 26, S73–S74. [Google Scholar] [CrossRef]
- Thunberg, J.; Bjorkqvist, O.; Hedin, C.R.H.; Forss, A.; Soderman, C.; Bergemalm, D.; Group, S.S.; Olen, O.; Hjortswang, H.; Strid, H.; et al. Ustekinumab treatment in ulcerative colitis: Real-world data from the Swedish inflammatory bowel disease quality register. United Eur. Gastroenterol. J. 2022, 10, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Honap, S.; Al-Hillawi, L.; Baillie, S.; Bancil, A.; Matini, L.; Lau, R.; Kok, K.B.; Patel, K.; Walsh, A.; Irving, P.M.; et al. Ustekinumab for the treatment of moderate to severe ulcerative colitis: A multicentre UK cohort study. Frontline Gastroenterol. 2022, 13, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Pilon, D.; Zhao, R.; Manceur, A.M.; Ding, Z.; Kachroo, S.; Vermette-Laforme, M.; Lefebvre, P. Persistence and adherence among patients with ulcerative colitis initiated on ustekinumab. Gastroenterology 2022, 162, S-417. [Google Scholar] [CrossRef]
- Rowan, C.R.; Keegan, D.; Byrne, K.; Cullen, G.; Mulcahy, H.E.; Sheridan, J.; Ryan, E.J.; de Vries, A.; D’Haens, G.; Doherty, G.A. Subcutaneous rather than intravenous ustekinumab induction is associated with comparable circulating drug levels and early clinical response: A pilot study. Aliment. Pharmacol. Ther. 2018, 48, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayan, J.R.; Dolinger, M.; Benkov, K.; Dunkin, D.; Jossen, J.; Lai, J.; Phan, B.L.; Pittman, N.; Dubinsky, M.C. Real World Experience With Ustekinumab in Children and Young Adults at a Tertiary Care Pediatric Inflammatory Bowel Disease Center. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 61–67. [Google Scholar] [CrossRef]
- Biemans, V.B.C.; van der Woude, C.J.; Dijkstra, G.; van der Meulen-de Jong, A.E.; Lowenberg, M.; de Boer, N.K.; Oldenburg, B.; Srivastava, N.; Jansen, J.M.; Bodelier, A.G.L.; et al. Ustekinumab is associated with superior effectiveness outcomes compared to vedolizumab in Crohn’s disease patients with prior failure to anti-TNF treatment. Aliment. Pharmacol. Ther. 2020, 52, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, I.; Arai, K.; Kyodo, R.; Sato, T.; Tokita, K.; Hirano, Y.; Shimizu, H. Ustekinumab for children and adolescents with inflammatory bowel disease at a tertiary children’s hospital in Japan. J. Gastroenterol. Hepatol. 2021, 36, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, O.H.; Ainsworth, M.A. Tumor necrosis factor inhibitors for inflammatory bowel disease. N. Engl. J. Med. 2013, 369, 754–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Pardi, D.S. Update on anti-tumor necrosis factor agents in Crohn disease. Gastroenterol. Clin. N. Am. 2014, 43, 457–478. [Google Scholar] [CrossRef]
- Yanai, H.; Hanauer, S.B. Assessing response and loss of response to biological therapies in IBD. Am. J. Gastroenterol. 2011, 106, 685–698. [Google Scholar] [CrossRef]
- Ford, A.C.; Sandborn, W.J.; Khan, K.J.; Hanauer, S.B.; Talley, N.J.; Moayyedi, P. Efficacy of biological therapies in inflammatory bowel disease: Systematic review and meta-analysis. Am. J. Gastroenterol. 2011, 106, 644–660. [Google Scholar] [CrossRef]
- Sands, B.E.; Irving, P.M.; Hoops, T.; Izanec, J.L.; Gao, L.L.; Gasink, C.; Greenspan, A.; Allez, M.; Danese, S.; Hanauer, S.B.; et al. Ustekinumab versus adalimumab for induction and maintenance therapy in biologic-naive patients with moderately to severely active Crohn’s disease: A multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet 2022, 399, 2200–2211. [Google Scholar] [CrossRef]
- Johnson, A.M.; Barsky, M.; Ahmed, W.; Zullow, S.; Galati, J.; Jairath, V.; Narula, N.; Peerani, F.; Click, B.H.; Coburn, E.S.; et al. The Real-World Effectiveness and Safety of Ustekinumab in the Treatment of Crohn’s Disease: Results from the SUCCESS Consortium. Am. J. Gastroenterol. 2022, 118, 317–328. [Google Scholar] [CrossRef]
- Yubei, G.; Lei, T.; Tianyu, Z.; Jie, Z.; Huan, W.; Liangru, Z. The efficacy and safety of ustekinumab in special cases with Crohn′s disease. Chin. J. Inflamm. Bowel Dis. 2021, 262–266. [Google Scholar] [CrossRef]
- Li, H.; Xie, L.; Yao, H.; Zhang, L.; Liang, S.; Lyu, W. Successful Non-Operative Treatment of Enterovesical and Enterocutaneous Fistulas Due to Crohn’s Disease. Int. Med. Case Rep. J. 2022, 15, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Huang, Y.H. Successful treatment of Crohn’s disease, aseptic liver abscess and psoriasis with ustekinumab. Rev. Esp. Enferm. Dig. 2022. [Google Scholar] [CrossRef]
- Abraham, C.; Cho, J. Interleukin-23/Th17 pathways and inflammatory bowel disease. Inflamm. Bowel. Dis. 2009, 15, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.A.; Langrish, C.L.; Chen, Y.; Blumenschein, W.; McClanahan, T.; Kastelein, R.A.; Sedgwick, J.D.; Cua, D.J. Divergent pro- and antiinflammatory roles for IL-23 and IL-12 in joint autoimmune inflammation. J. Exp. Med. 2003, 198, 1951–1957. [Google Scholar] [CrossRef]
- Langrish, C.L.; Chen, Y.; Blumenschein, W.M.; Mattson, J.; Basham, B.; Sedgwick, J.D.; McClanahan, T.; Kastelein, R.A.; Cua, D.J. IL-23 drives a pathogenic T cell population that induces autoimmune inflammation. J. Exp. Med. 2005, 201, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, S.L.; Schreiner, B.; McMahon, E.J.; Miller, S.D. CNS myeloid DCs presenting endogenous myelin peptides ‘preferentially’ polarize CD4+ T(H)-17 cells in relapsing EAE. Nat. Immunol. 2007, 8, 172–180. [Google Scholar] [CrossRef]
- Schmidt-Weber, C.B.; Akdis, M.; Akdis, C.A. TH17 cells in the big picture of immunology. J. Allergy Clin. Immunol. 2007, 120, 247–254. [Google Scholar] [CrossRef]
- Lappalainen, M.; Halme, L.; Turunen, U.; Saavalainen, P.; Einarsdottir, E.; Farkkila, M.; Kontula, K.; Paavola-Sakki, P. Association of IL23R, TNFRSF1A, and HLA-DRB1*0103 allele variants with inflammatory bowel disease phenotypes in the Finnish population. Inflamm. Bowel Dis. 2008, 14, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Einarsdottir, E.; Koskinen, L.L.; Dukes, E.; Kainu, K.; Suomela, S.; Lappalainen, M.; Ziberna, F.; Korponay-Szabo, I.R.; Kurppa, K.; Kaukinen, K.; et al. IL23R in the Swedish, Finnish, Hungarian and Italian populations: Association with IBD and psoriasis, and linkage to celiac disease. BMC Med. Genet. 2009, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Magyari, L.; Melegh, B. Susceptibility genetic variants in Hungarian morbus Crohn and ulcerative colitis patients. Orv. Hetil. 2009, 150, 81–88. [Google Scholar] [CrossRef]
- Song, L.; Zhou, R.; Huang, S.; Zhou, F.; Xu, S.; Wang, W.; Yi, F.; Wang, X.; Xia, B. High intestinal and systemic levels of interleukin-23/T-helper 17 pathway in Chinese patients with inflammatory bowel disease. Mediat. Inflamm. 2013, 2013, 425915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.; Qian, Y.Z.; Qian, H.H. Interleukin-12B gene rs6887695 and rs2288831 polymorphisms are associated with an increased risk of ulcerative colitis development in Chinese Han population: A case-control study. J. Clin. Lab. Anal. 2020, 34, e23472. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.K.; Chen, Z.R.; Zhu, J.Y.; Xu, Y.; Hua, X. Analysis of the association of single nucleotide polymorphisms of interleukin-23 receptor (IL-23R) and inflammatory bowel disease in a Chinese Han cohort. Oncotarget 2016, 7, 67851–67856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, K.; Onouchi, Y.; Takazoe, M.; Kubo, M.; Nakamura, Y.; Hata, A. Association analysis of genetic variants in IL23R, ATG16L1 and 5p13.1 loci with Crohn’s disease in Japanese patients. J. Hum. Genet. 2007, 52, 575–583. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study | Country and Region | IBD Type | Sample Size, N | Mean Age, Years (±SD, IQR) | Age at Onset, % | Male Sex,% | Mean Disease Duration, Years (±SD, IQR) | MINORS Scale | ||
|---|---|---|---|---|---|---|---|---|---|---|
| <17 | 17–40 | >40 | ||||||||
| Kopylov et al. 2020 [16] | Europe and Canada | CD | 142 | 35 (26–49) | NR | NR | NR | 38.7 | 10 (5–17) | 16 |
| Khorrami et al. 2016 [17] | Spain | CD | 116 | 37 (28–48) | 20.7 | 69 | 10.3 | 37.1 | 10 (6–17) | 16 |
| Iborra et al. 2020 [18] | Spain | CD | 407 | 45.28 (34.86–55.93) | NR | NR | NR | 48 | 11.06 (5.7–19.03) | 18 |
| Iborra et al. 2019 [19] | Spain | CD | 305 | 43.7 (34.4, 53.6) | NR | NR | NR | 49 | 11.7 (5.6, 18.8) | 16 |
| Bermejo et al. 2022 [20] | Spain | CD | 53 | 45 ± 12 | NR | NR | NR | 49.1 | 14 ± 6.4 | 19 |
| Hoffmann et al. 2019 [21] | Germany | CD | 57 | 43.0 (21–68) | 7 | 70 | 23 | 52.6 | 43 (21–68) | 17 |
| Kubesch et al. 2019 [22] | Germany | CD | 106 | 39.5(19–73) | NR | NR | NR | 41.5 | 11 (2–39) | 16 |
| Thomann et al. 2020 [23] | Germany | CD | 72 | 38.9 (14.2) | NR | NR | NR | 37.5 | NR | 19 |
| Ollech et al. 2021 [24] | US | CD | 506 | 35.8 (27.2–51.4) | 33.6 | 60 | 4.5 | NR | NR | 17 |
| Dalal et al. 2020 [25] | US | CD | 64 | 42.2 | NR | NR | NR | 39.1 | 15.5 | 19 |
| Weaver et al. 2019 [26] | US | CD | 56 | 24.2 (11.7) | NR | NR | NR | 43 | NR | 19 |
| Haider et al. 2020 [27] | US | CD | 143 | 42.2 (18–83) | NR | NR | NR | 44.1 | 14.3 (1–38) | 18 |
| Garg et al. 2022 [28] | US | CD | 78 | 37.6 ± 13.5 | 32.1 | 55.1 | 12.8 | 52.6 | 13.3 ± 7.9 | 18 |
| Forss et al. 2021 [29] | Sweden | CD | 114 | 40 (31–54) | 15 | 66 | 19 | 53 | NR | 19 |
| Plevris et al. 2021 [30] | UK | CD | 216 | 39.0 (28.8–51.8) | NR | NR | NR | NR | 9.9 (6.0–16.5) | 19 |
| Harris et al. 2020 [31] | UK | CD | 84 | 41.6 (14.7) | NR | NR | NR | 46.9 | 12.3 (8.9) | 17 |
| Huinink et al. 2021 [32] | Netherlands | CD | 31 | 37 (30–48) | 13 | 77.3 | 9.7 | 35.5 | NR | 19 |
| Biemans et al. 2020 [33] | Netherlands | CD | 221 | 38.2 (29.3–52.2) | NR | NR | NR | 39.8 | 12.3 (7.5–19.3) | 18 |
| Straatmijer et al. 2021 [34] | Netherlands | CD | 252 | NR | NR | NR | NR | 39.7 | 15 (10–22) | 17 |
| Wils et al. 2017 [35] | France | CD | 88 | 32.5 (25.8–39.3) | NR | NR | NR | 27 | 11.8 (7.7–17.1) | 17 |
| Wils et al. 2016 [36] | France | CD | 122 | 33.8 (27.5–43.9) | NR | NR | NR | 29 | 11.5 (6.9–17.1) | 16 |
| Battat et al. 2016 [37] | Canada | CD | 62 | NR | 33.9 | 53.2 | 12.6 | 38.7 | NR | 17 |
| Greenup et al. 2017 [38] | Canada | CD | 73 | 37 (30–50) | NR | NR | NR | 38 | 17 (10–23) | 16 |
| Ma et al. 2017 [39] | Canada | CD | 104 | 44.6 (32.2–57.5) | NR | NR | NR | 43.3 | 13.8 (9.1–22.9) | 18 |
| Rowan et al. 2018 [61] | Ireland | CD | 19 | 36.2 (25.4–40.8) | NR | NR | NR | 15.8 | 18.9 (5.9–23.2) | 17 |
| Eberl et al. 2019 [3] | Finland | CD | 48 | 42.2 ± 14.9 | NR | NR | NR | 54.2 | 13.9 ± 10.3 | 16 |
| Liefferinckx et al. 2019 [40] | Belgium | CD | 152 | 41 (19–74) | 3.3 | 67.8 | 27.7 | 30.9 | NR | 19 |
| Pugliese et al. 2019 [4] | Italy | CD | 64 | 41.75 (20.3–72.3) | NR | NR | NR | 35.7 | 10 (0.50–33.8) | 16 |
| Tursi et al. 2021 [41] | Italy | CD | 194 | 48 (38–58) | NR | NR | NR | 55.7 | 13 (7–22) | 19 |
| Hanzel et al. 2021 [42] | Slovenia | CD | 41 | 48 (31–55) | NR | NR | NR | NR | 16 (7–26) | 18 |
| Yao et al. 2021 [43] | China | CD | 18 | 30.5 (26.0, 38.0) | NR | NR | NR | 66.7 | 6.5 (1.9, 10.0) | 16 |
| Yao et al. 2021 [45] | China | CD | 127 | 31.0 ± 11.3 | NR | NR | NR | 57.5 | NR | 18 |
| Yao et al. 2021 [44] | China | CD | 19 | 29.1 ± 9.1 | 0 | 89.5 | 10.5 | 57.9 | 5.5 ± 4.7 | 18 |
| Yokoyama et al. 2021 [46] | Japan | CD | 339 | 37.2 (13.4) | NR | NR | NR | 67.3 | 11.0 (9.1) | 19 |
| Takenaka et al. 2021 [47] | Japan | CD | 143 | 36 (26–46) | NR | NR | NR | 71 | 10 (4– 15) | 17 |
| Miyazaki et al. 2019 [48] | Japan | CD | 47 | 42 (35–49) | NR | NR | NR | 51.1 | 15.3 (10.5–24.5) | 17 |
| Hyun et al. 2022 [49] | Republic of Korea | CD | 18 | 34.4 (26.1–40.8) | NR | NR | NR | 43.8 | 19.7 (17.1–24.6) | 18 |
| Altuwaijri et al. 2022 [50] | Saudi Arabia | CD | 30 | 34.2 ± 17.9 | NR | NR | NR | 50 | 10.6 ± 4.9 | 18 |
| Chaparro et al. 2021 [51] | Spain | UC | 95 | 47(16) | NR | NR | NR | 44 | NR | 17 |
| Amiot et al. 2020 [52] | France | UC | 103 | 39.3 (29.1–52.3) | 7.8 | 66 | 26.2 | 60.2 | 7.6 (3.6–12.9) | 18 |
| Fumery et al. 2021 [53] | France | UC | 103 | 39.3 (29.1–52.3) | 7.8 | 66 | 26.2 | 60.2 | 7.6 (3.6–12.9) | 16 |
| Ochsenkuhn et al. 2020 [54] | Germany | UC | 19 | 46 (26–81) | NR | NR | NR | 55 | 5 (2–15) | 16 |
| Chiappetta et al. 2021 [55] | Italy | UC | 68 | 30 (2–65) | NR | NR | NR | 63 | NR | 17 |
| Dalal et al. 2021 [56] | US | UC | 108 | 39 (30–56) | NR | NR | NR | 43.5 | 9 (4–16) | 18 |
| Hong et al. 2020 [57] | US | UC | 19 | 42.7 ± 17.0 | NR | NR | NR | 47.4 | 9.6 ± 8.4 | 16 |
| Alsoud et al. 2022 [12] | Belgium | UC | 42 | 40 (30–53) | NR | NR | NR | 43 | 8 (4–15) | 18 |
| Thunberg et al. 2022 [58] | Sweden | UC | 133 | 38 (28–48) | NR | NR | NR | 60 | 7 (3–12) | 19 |
| Honap et al. 2022 [59] | UK | UC | 110 | 40 (29–59) | NR | NR | NR | 59 | 7 (3–13) | 18 |
| Pilon et al. 2022 [60] | Canada | UC | 2645 | 44.0 ± 15.9 | NR | NR | NR | 52.6 | NR | 17 |
| UC Patients | CD Patients | ||||
|---|---|---|---|---|---|
| N | Effect Size | N | Effect Size | ||
| Studies | Studies | ||||
| Clinical response | |||||
| Week 12 | 6 | 61% (95% CI: 55–67%; I2 = 34.62%) | 17 | 55% (95% CI: 46–65%; I2 = 93.71%) | |
| Week 24 | 8 | 66% (95% CI: 53–78%; I2 = 92.90%) | |||
| Week 52 | 9 | 55% (95% CI: 47–62%; I2 = 75.96%) | |||
| Clinical remission | |||||
| Week 12 | 7 | 34% (95% CI: 24–45%; I2 = 79.18%) | 23 | 46% (95% CI: 36–59%; I2 = 97.50%) | |
| Week 24 | 6 | 40% (95% CI:30–50%; I2 = 62.78%) | 14 | 51% (95% CI: 37–66%; I2 = 95.92%) | |
| Week 52 | 5 | 37% (95% CI: 30–43%; I2 = 0.00%) | 10 | 47% (95% CI: 32–62%; I2 = 96.54%) | |
| CS-free remission | |||||
| Week 12 | 5 | 38% (95% CI: 23–55%; I2 = 86.11%) | 6 | 44% (95% CI: 32–56%; I2 = 88.83%) | |
| Week 24 | 5 | 38% (95% CI: 28–48%; I2 = 69.87%) | 8 | 49% (95% CI: 39–59%; I2 = 85.39%) | |
| Week 52 | 6 | 37% (95% CI: 24–51%; I2 = 91.09%) | 7 | 52% (95% CI: 41–62%; I2 = 87.16%) | |
| Endoscopic response | |||||
| Week 52 | 9 | 65% (95% CI: 57–71%; I2 = 45.54%) | |||
| Endoscopic remission | |||||
| Week 52 | 9 | 29% (95% CI: 18–40%; I2 = 80.35%) | |||
| Mucosal healing | |||||
| Week 52 | 7 | 31% (95% CI: 19–44%; I2 = 79.88%) | |||
| Adverse events | 5 | 5% (95% CI: 3–8%; I2 = 13.69%) | 10 | 11% (95% CI: 6–18%; I2 = 91.38%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Wang, F.; Wan, J.; Su, S.; Shi, Y.; Li, X.; Wu, T.; Liang, J. Systematic Review and Meta-Analysis of Observational Studies on the Effectiveness and Safety of Ustekinumab among Patients with Inflammatory Bowel Disease in Eastern and Western Countries. J. Clin. Med. 2023, 12, 1894. https://doi.org/10.3390/jcm12051894
Zhou H, Wang F, Wan J, Su S, Shi Y, Li X, Wu T, Liang J. Systematic Review and Meta-Analysis of Observational Studies on the Effectiveness and Safety of Ustekinumab among Patients with Inflammatory Bowel Disease in Eastern and Western Countries. Journal of Clinical Medicine. 2023; 12(5):1894. https://doi.org/10.3390/jcm12051894
Chicago/Turabian StyleZhou, He, Fang Wang, Jian Wan, Song Su, Yanting Shi, Xiaofei Li, Tong Wu, and Jie Liang. 2023. "Systematic Review and Meta-Analysis of Observational Studies on the Effectiveness and Safety of Ustekinumab among Patients with Inflammatory Bowel Disease in Eastern and Western Countries" Journal of Clinical Medicine 12, no. 5: 1894. https://doi.org/10.3390/jcm12051894