

Application of Neuromuscular Blockers in Patients with ARDS in ICU: A Retrospective Study Based on the MIMIC-III Database

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Data
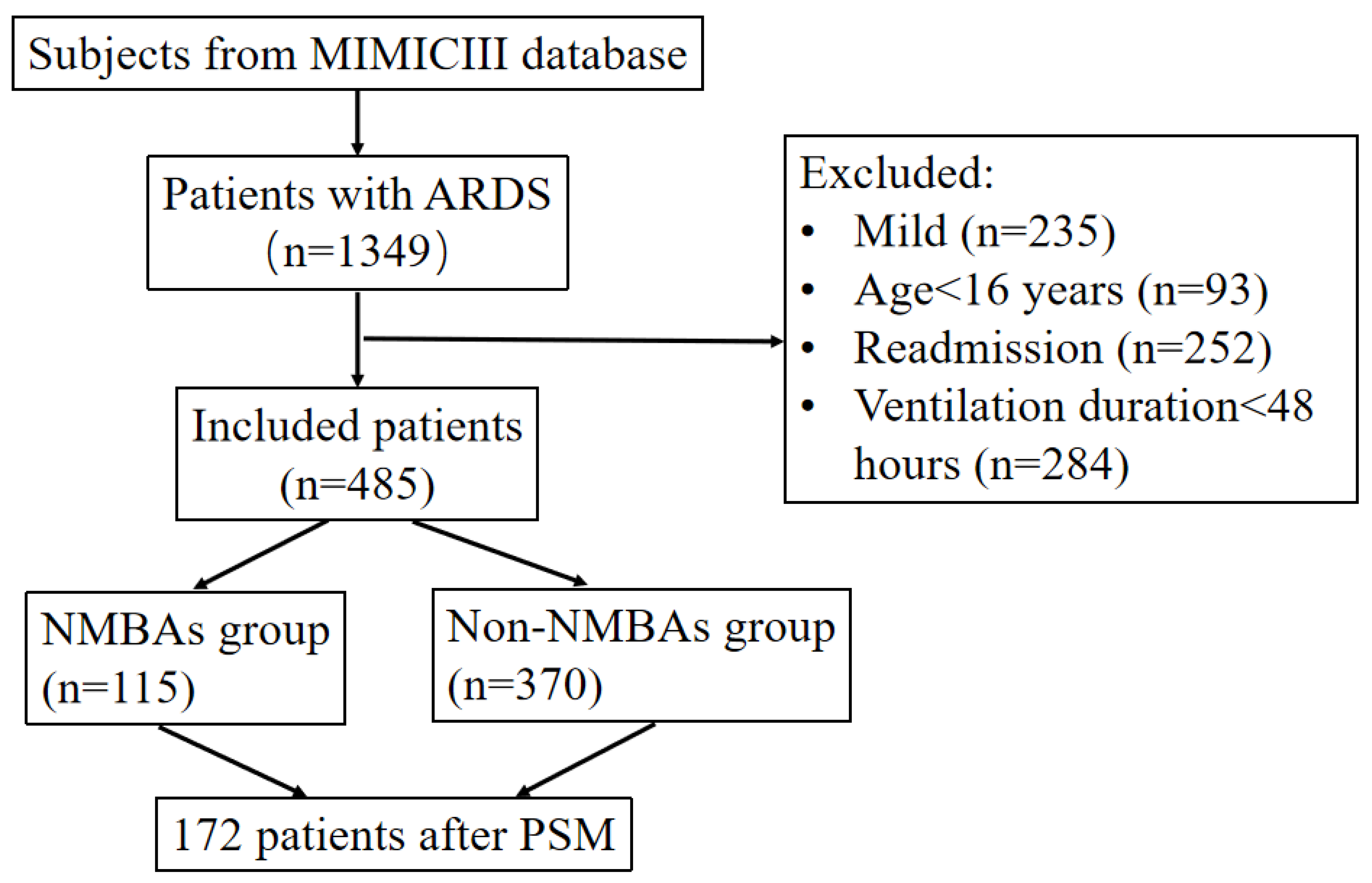
2.2. Study Cohort
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
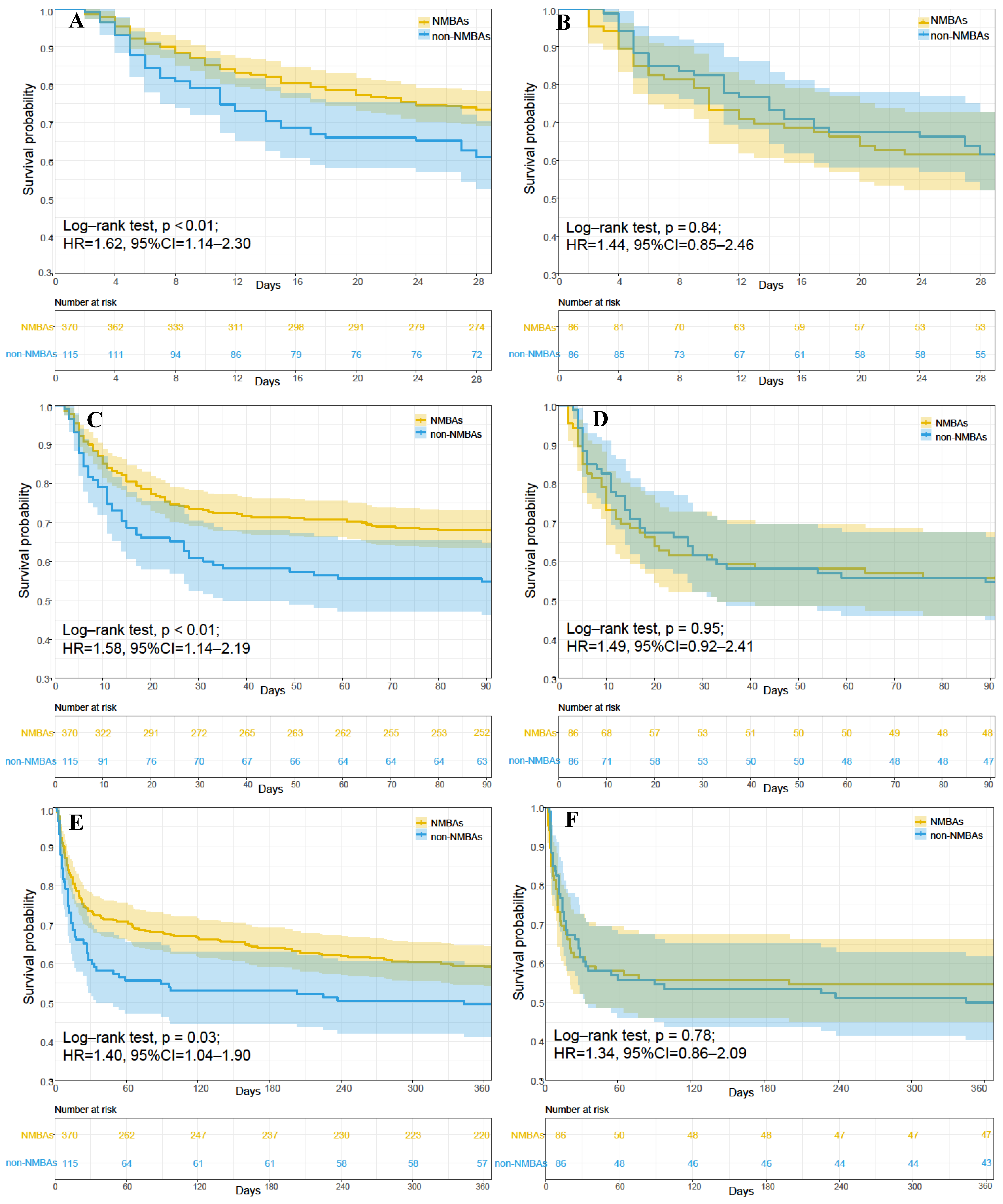
3.2. Relationship between NMBAs and Outcomes
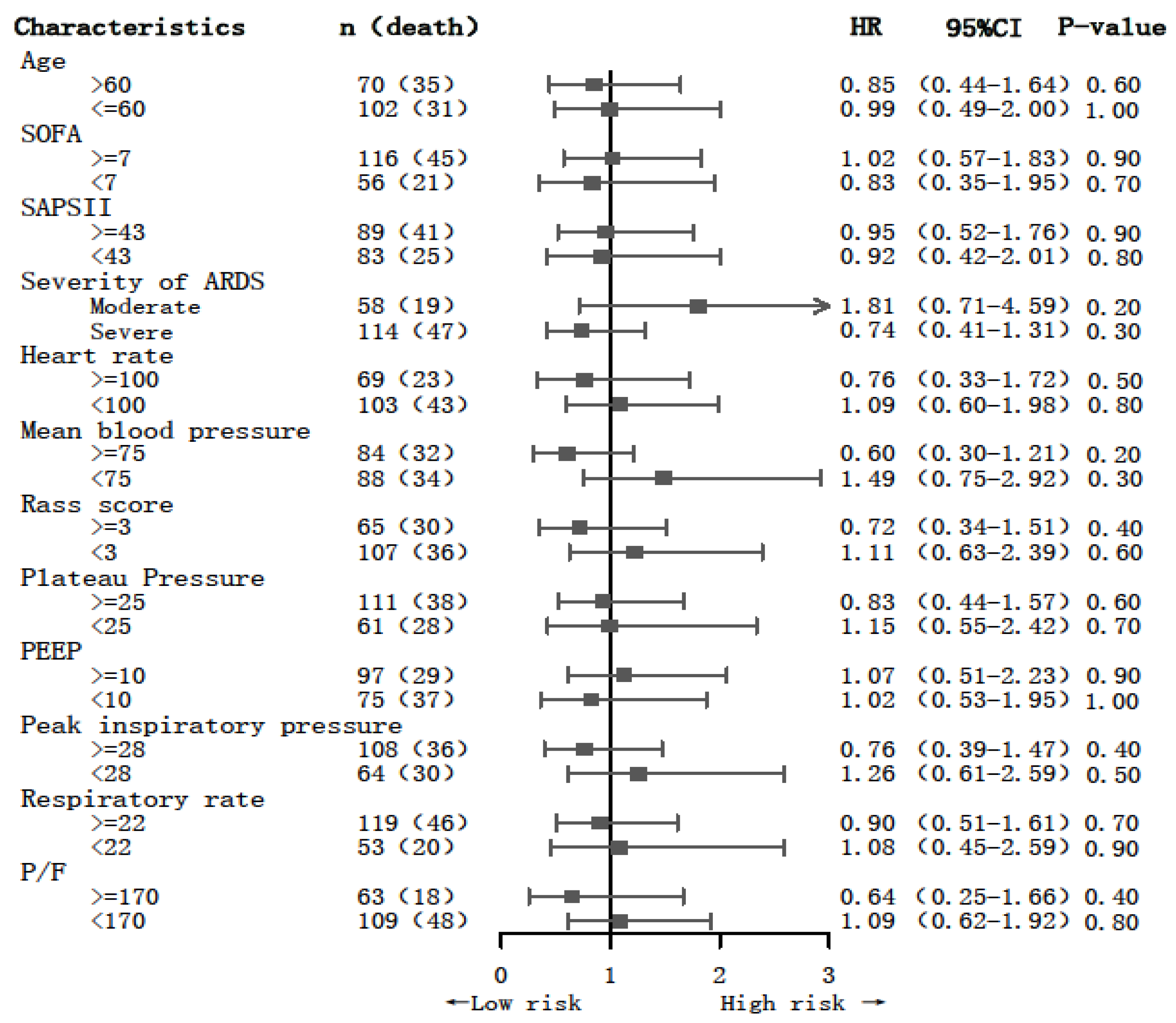
3.3. Subgroup Analysis
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. JAMA 2018, 319, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Bernard, G.R. Acute respiratory distress syndrome: A historical perspective. Am. J. Respir. Crit. Care. Med. 2005, 172, 798–806. [Google Scholar] [CrossRef] [Green Version]
- Brun-Buisson, C.; Minelli, C.; Bertolini, G.; Brazzi, L.; Pimentel, J.; Lewandowski, K.; Bion, J.; Romand, J.A.; Villar, J.; Thorsteinsson, A.; et al. Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med. 2004, 30, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteban, A.; Ferguson, N.D.; Meade, M.O.; Frutos-Vivar, F.; Apezteguia, C.; Brochard, L.; Raymondos, K.; Nin, N.; Hurtado, J.; Tomicic, V.; et al. Evolution of mechanical ventilation in response to clinical research. Am. J. Respir. Crit. Care Med. 2008, 177, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Esteban, A.; Anzueto, A.; Frutos, F.; Alia, I.; Brochard, L.; Stewart, T.E.; Benito, S.; Epstein, S.K.; Apezteguia, C.; Nightingale, P.; et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: A 28-day international study. JAMA 2002, 287, 345–355. [Google Scholar] [CrossRef] [Green Version]
- Sahetya, S.K.; Mallow, C.; Sevransky, J.E.; Martin, G.S.; Girard, T.D.; Brower, R.G.; Checkley, W.; Society of Critical Care Medicine Discovery Network Critical Illness Outcomes Study Investigators. Association between hospital mortality and inspiratory airway pressures in mechanically ventilated patients without acute respiratory distress syndrome: A prospective cohort study. Crit. Care 2019, 23, 367. [Google Scholar] [CrossRef] [Green Version]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.; Hurford, W.E. When should sedation or neuromuscular blockade be used during mechanical ventilation? Respir. Care 2011, 56, 168–176; discussion 176–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papazian, L.; Forel, J.M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.M.; Perez, D.; Seghboyan, J.M.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terao, Y.; Miura, K.; Saito, M.; Sekino, M.; Fukusaki, M.; Sumikawa, K. Quantitative analysis of the relationship between sedation and resting energy expenditure in postoperative patients. Crit. Care Med. 2003, 31, 830–833. [Google Scholar] [CrossRef] [PubMed]
- Renew, J.R.; Ratzlaff, R.; Hernandez-Torres, V.; Brull, S.J.; Prielipp, R.C. Neuromuscular blockade management in the critically Ill patient. J. Intensive Care 2020, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Gainnier, M.; Roch, A.; Forel, J.M.; Thirion, X.; Arnal, J.M.; Donati, S.; Papazian, L. Effect of neuromuscular blocking agents on gas exchange in patients presenting with acute respiratory distress syndrome. Crit. Care Med. 2004, 32, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Forel, J.M.; Roch, A.; Marin, V.; Michelet, P.; Demory, D.; Blache, J.L.; Perrin, G.; Gainnier, M.; Bongrand, P.; Papazian, L. Neuromuscular blocking agents decrease inflammatory response in patients presenting with acute respiratory distress syndrome. Crit. Care Med. 2006, 34, 2749–2757. [Google Scholar] [CrossRef]
- Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; Hite, R.D.; et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [CrossRef]
- Bourenne, J.; Hraiech, S.; Roch, A.; Gainnier, M.; Papazian, L.; Forel, J.M. Sedation and neuromuscular blocking agents in acute respiratory distress syndrome. Ann. Transl. Med. 2017, 5, 291. [Google Scholar] [CrossRef] [Green Version]
- Fodale, V.; Santamaria, L.B. Laudanosine, an atracurium and cisatracurium metabolite. Eur. J. Anaesthesiol. 2002, 19, 466–473. [Google Scholar] [CrossRef]
- Alhazzani, W.; Alshahrani, M.; Jaeschke, R.; Forel, J.M.; Papazian, L.; Sevransky, J.; Meade, M.O. Neuromuscular blocking agents in acute respiratory distress syndrome: A systematic review and meta-analysis of randomized controlled trials. Crit. Care 2013, 17, R43. [Google Scholar] [CrossRef] [Green Version]
- Meyer, N.J.; Gattinoni, L.; Calfee, C.S. Acute respiratory distress syndrome. Lancet 2021, 398, 622–637. [Google Scholar] [CrossRef]
- Brochard, L. Ventilation-induced lung injury exists in spontaneously breathing patients with acute respiratory failure: Yes. Intensive Care Med. 2017, 43, 250–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanelli, V.; Morita, Y.; Cappello, P.; Ghazarian, M.; Sugumar, B.; Delsedime, L.; Batt, J.; Ranieri, V.M.; Zhang, H.; Slutsky, A.S. Neuromuscular Blocking Agent Cisatracurium Attenuates Lung Injury by Inhibition of Nicotinic Acetylcholine Receptor-α1. Anesthesiology 2016, 124, 132–140. [Google Scholar] [CrossRef]
- Hurford, W.E. Neuromuscular Blockade Applicability in Early Acute Respiratory Distress Syndrome. Anesthesiology 2020, 132, 1577–1584. [Google Scholar] [CrossRef]
- Trapani, G.; Altomare, C.; Liso, G.; Sanna, E.; Biggio, G. Propofol in anesthesia. Mechanism of action, structure-activity relationships, and drug delivery. Curr. Med. Chem. 2000, 7, 249–271. [Google Scholar] [CrossRef] [PubMed]
- Latronico, N.; Bolton, C.F. Critical illness polyneuropathy and myopathy: A major cause of muscle weakness and paralysis. The Lancet. Neurology 2011, 10, 931–941. [Google Scholar] [CrossRef]
- Grawe, E.S.; Bennett, S.; Hurford, W.E. Early Paralysis for the Management of ARDS. Respir. Care 2016, 61, 830–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, S.B.; Vender, J. The use of neuromuscular blocking agents in the ICU: Where are we now? Crit. Care Med. 2013, 41, 1332–1344. [Google Scholar] [CrossRef] [Green Version]
- Shao, S.; Kang, H.; Tong, Z. Early neuromuscular blocking agents for adults with acute respiratory distress syndrome: A systematic review, meta-analysis and meta-regression. BMJ Open 2020, 10, e037737. [Google Scholar] [CrossRef]
- Dodson, B.A.; Kelly, B.J.; Braswell, L.M.; Cohen, N.H. Changes in acetylcholine receptor number in muscle from critically ill patients receiving muscle relaxants: An investigation of the molecular mechanism of prolonged paralysis. Crit. Care Med. 1995, 23, 815–821. [Google Scholar] [CrossRef]
- Saccheri, C.; Morawiec, E.; Delemazure, J.; Mayaux, J.; Dubé, B.P.; Similowski, T.; Demoule, A.; Dres, M. ICU-acquired weakness, diaphragm dysfunction and long-term outcomes of critically ill patients. Ann. Intensive Care 2020, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Baek, M.S.; Kim, J.H.; Lim, Y.; Kwon, Y.S. Neuromuscular blockade in mechanically ventilated pneumonia patients with moderate to severe hypoxemia: A multicenter retrospective study. PloS ONE 2022, 17, e0277503. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.H.; Yu, B.X.; Sun, Y.B.; Fang, W.; Li, L. Effects of early rehabilitation therapy on patients with mechanical ventilation. World J. Emerg. Med. 2014, 5, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yosef-Brauner, O.; Adi, N.; Ben Shahar, T.; Yehezkel, E.; Carmeli, E. Effect of physical therapy on muscle strength, respiratory muscles and functional parameters in patients with intensive care unit-acquired weakness. Clin. Respir. J. 2015, 9, 1–6. [Google Scholar] [CrossRef]
- Shehabi, Y.; Bellomo, R.; Reade, M.C.; Bailey, M.; Bass, F.; Howe, B.; McArthur, C.; Seppelt, I.M.; Webb, S.; Weisbrodt, L. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shehabi, Y.; Chan, L.; Kadiman, S.; Alias, A.; Ismail, W.N.; Tan, M.A.; Khoo, T.M.; Ali, S.B.; Saman, M.A.; Shaltut, A.; et al. Sedation depth and long-term mortality in mechanically ventilated critically ill adults: A prospective longitudinal multicentre cohort study. Intensive Care Med. 2013, 39, 910–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shehabi, Y.; Bellomo, R.; Kadiman, S.; Ti, L.K.; Howe, B.; Reade, M.C.; Khoo, T.M.; Alias, A.; Wong, Y.L.; Mukhopadhyay, A.; et al. Sedation Intensity in the First 48 Hours of Mechanical Ventilation and 180-Day Mortality: A Multinational Prospective Longitudinal Cohort Study. Crit. Care Med. 2018, 46, 850–859. [Google Scholar] [CrossRef]
- Balzer, F.; Weiß, B.; Kumpf, O.; Treskatsch, S.; Spies, C.; Wernecke, K.D.; Krannich, A.; Kastrup, M. Early deep sedation is associated with decreased in-hospital and two-year follow-up survival. Crit. Care 2015, 19, 197. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All (n = 485) | Non-NMBAs (n = 370) | NMBAs (n = 115) | p-Value | |
|---|---|---|---|---|
| Weight | 80.00 [68.45, 95.00] | 80.20 [68.00, 95.00] | 80.00 [69.15, 94.95] | 0.90 |
| Gender (%) | 0.05 | |||
| Male | 284 (58.56) | 207 (55.95) | 77 (66.96) | |
| Female | 201 (41.44) | 163 (44.05) | 38 (33.04) | |
| Age (years) | 58.52 [46.04, 72.22] | 59.85 [47.02, 75.20] | 56.47 [40.64, 66.45] | 0.01 |
| Admission type (%) | 0.42 | |||
| Elective | 31 (6.39) | 22 (5.95) | 9 (7.83) | |
| Emergency | 432 (89.07) | 329 (88.92) | 103 (89.57) | |
| Urgent | 22 (4.54) | 19 (5.14) | 3 (2.61) | |
| Ethnicity (%) | 0.96 | |||
| White | 307 (63.30) | 236 (63.78) | 71 (61.74) | |
| Hispanic | 17 (3.51) | 13 (3.51) | 4 (3.48) | |
| Black | 31 (6.39) | 24 (6.49) | 7 (6.09) | |
| Other | 130 (26.80) | 97 (26.22) | 33 (28.70) | |
| Mechanical ventilation (%) | 426 (87.84) | 323 (87.30) | 103 (89.57) | 0.63 |
| Vasopressors (%) | 249 (51.34) | 173 (46.76) | 76 (66.09) | <0.01 |
| RRT (%) | 30 (6.19) | 20 (5.41) | 10 (8.70) | 0.29 |
| ARDS severity (%) | <0.01 | |||
| Moderate | 250 (51.55) | 214 (57.84) | 36 (31.30) | |
| Severe | 235 (48.45) | 156 (42.16) | 79 (68.70) | |
| SAPS II | 43.00 [33.00, 54.00] | 43.00 [33.00, 53.00] | 44.00 [34.50, 59.00] | 0.28 |
| SOFA | 7.00 [5.00, 10.00] | 7.00 [5.00, 9.00] | 9.00 [6.00, 12.00] | <0.01 |
| Heart rate (bpm) | 93.27 (17.94) | 92.12 (16.99) | 96.99 (20.35) | 0.01 |
| SpO2 | 96.73 [95.43, 97.89] | 97.03 [95.70, 98.08] | 96.08 [94.67, 97.40] | <0.01 |
| Respiratory rate (bpm) | 22.35 (4.93) | 21.64 (4.85) | 24.61 (4.52) | <0.01 |
| PEEP | 8.78 [5.84, 11.22] | 8.33 [5.00, 10.24] | 11.70 [8.57, 14.94] | <0.01 |
| RASS score | −1.20 [−1.44, −0.83] | −1.07 [−1.20, −0.75] | −1.72 [−2.30, −1.20] | <0.01 |
| Co-morbidities (%) | ||||
| CHF | 171 (35.26) | 142 (37.40) | 29 (25.22) | 0.08 |
| AFIB | 115 (23.71) | 92 (24.86) | 23 (20.00) | 0.34 |
| CAD | 44 (9.07) | 35 (9.46) | 9 (7.83) | 0.73 |
| Malignancy | 85 (17.53) | 71 (19.19) | 14 (12.17) | 0.11 |
| Kidney | 36 (7.42) | 28 (7.57) | 8 (6.96) | >0.99 |
| Liver | 31 (6.39) | 24 (6.49) | 7 (6.09) | >0.99 |
| COPD | 66 (13.60) | 60 (16.22) | 6 (5.22) | 0.01 |
| Stroke | 44 (9.07) | 34 (9.19) | 10 (8.70) | >0.99 |
| Matched Cohort | |||
|---|---|---|---|
| Non-NMBAs | NMBAs | SMD | |
| n | 86 | 86 | |
| Gender (%) | 0.12 | ||
| Male | 58 (67.44) | 53 (61.63) | |
| Female | 28 (32.56) | 33 (38.37) | |
| Age (years) | 52.69 (19.88) | 54.45 (16.28) | 0.10 |
| Admission type (%) | 0.14 | ||
| Elective | 5 (5.81) | 7 (8.14) | |
| Emergency | 76 (88.37) | 76 (88.37) | |
| Urgent | 5 (5.81) | 3 (3.49) | |
| Ethnicity (%) | 0.08 | ||
| White | 52 (60.47) | 54 (62.79) | |
| Hispanic | 5 (5.81) | 4 (4.65) | |
| Black | 5 (5.81) | 4 (4.65) | |
| Other | 24 (27.91) | 24 (27.91) | |
| Ventilation (%) | 77 (89.53) | 77 (89.53) | <0.01 |
| RRT (%) | 6 (6.98) | 7 (8.14) | 0.04 |
| Vasopressors (%) | 57 (66.28) | 51 (59.30) | 0.15 |
| ARDS severity (%) | <0.01 | ||
| Moderate | 29 (33.72) | 29 (33.72) | |
| Severe | 57 (66.28) | 57 (66.28) | |
| SAPS II | 45.00 (14.68) | 45.62 (16.83) | 0.04 |
| SOFA | 8.65 (3.60) | 8.63 (3.85) | <0.01 |
| Heart rate (bpm) | 94.52 (18.08) | 95.94 (19.27) | 0.08 |
| Respiratory rate (bpm) | 24.49 (4.77) | 24.21 (4.24) | 0.06 |
| RASS | 2.69 (0.62) | 2.65 (0.48) | 0.07 |
| Co-morbidities (%) | |||
| CHF | 24 (27.91) | 21 (24.42) | 0.08 |
| Renal | |||
| Liver | 7 (8.14) | 6 (6.98) | 0.04 |
| COPD | 3 (3.49) | 5 (5.81) | 0.11 |
| Stroke | 9 (10.47) | 9 (10.47) | <0.01 |
| HR | Low 95% CI | High 95% CI | p-Value | |
|---|---|---|---|---|
| Pre-matched cohort | ||||
| 28-day mortality | 1.62 | 1.14 | 2.30 | <0.01 |
| Adjusted model I | 1.78 | 1.23 | 2.56 | <0.01 |
| Adjusted model II | 1.39 | 0.94 | 2.04 | <0.01 |
| 90-day mortality | 1.58 | 1.14 | 2.19 | <0.01 |
| Adjusted model I | 1.75 | 1.25 | 2.45 | <0.01 |
| Adjusted model II | 1.49 | 1.03 | 2.14 | <0.01 |
| One-year mortality | 1.40 | 1.04 | 1.90 | 0.03 |
| Adjusted model I | 1.41 | 1.03 | 1.92 | <0.01 |
| Adjusted model II | 1.39 | 1.00 | 1.95 | <0.01 |
| Hospital mortality | 1.41 | 0.99 | 2.00 | 0.06 |
| Adjusted model I | 1.60 | 1.11 | 2.30 | <0.01 |
| Adjusted model II | 1.32 | 0.90 | 1.95 | <0.01 |
| Matched cohort | ||||
| 28-day mortality | 1.44 | 0.85 | 2.46 | 0.20 |
| Adjusted model I | 1.39 | 0.81 | 2.39 | 0.23 |
| Adjusted model II | 1.47 | 0.84 | 2.56 | 0.17 |
| 90-day mortality | 1.49 | 0.92 | 2.41 | 0.10 |
| Adjusted model I | 1.54 | 0.94 | 2.54 | 0.09 |
| Adjusted model II | 1.61 | 0.97 | 2.67 | 0.06 |
| One-year mortality | 1.34 | 0.86 | 2.09 | 0.20 |
| Adjusted model I | 1.34 | 0.85 | 2.10 | 0.20 |
| Adjusted model II | 1.41 | 0.89 | 2.22 | 0.15 |
| Hospital mortality | 1.34 | 0.81 | 2.24 | 0.30 |
| Adjusted model I | 1.39 | 0.83 | 2.32 | 0.21 |
| Adjusted model II | 1.48 | 0.87 | 2.52 | 0.15 |
| Overall | Non-NMBAs | NMBAs | p-Value | |
|---|---|---|---|---|
| Pre-matched cohort | N = 485 | N = 370 | N = 115 | |
| Length of hospital stay (days) | 17.09 [10.11, 24.90] | 16.80 [10.12, 23.76] | 18.09 [9.48, 29.80] | 0.21 |
| Length of ICU stay (days) | 10.98 [6.14, 18.76] | 10.20 [5.96, 16.18] | 14.92 [7.29, 26.79] | <0.01 |
| Duration of ventilation (days) | 7.59 [4.42, 14.00] | 7.12 [4.17, 11.97] | 12.29 [5.53, 20.33] | <0.01 |
| Matched cohort | N = 172 | N = 86 | N = 86 | |
| Length of hospital stay (days) | 17.15 [9.62, 26.70] | 14.92 [9.43, 22.02] | 18.05 [11.56, 28.95] | 0.06 |
| Length of ICU stay (days) | 11.22 [6.02, 19.94] | 9.37 [5.47, 12.86] | 14.67 [7.96, 26.22] | <0.01 |
| Duration of ventilation (days) | 8.72 [4.42, 15.59] | 6.40 [3.40, 10.48] | 12.38 [5.55, 19.77] | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, X.; Liu, J.; Zhang, S.; Huang, S.; Chen, L.; Shen, X.; Chen, D. Application of Neuromuscular Blockers in Patients with ARDS in ICU: A Retrospective Study Based on the MIMIC-III Database. J. Clin. Med. 2023, 12, 1878. https://doi.org/10.3390/jcm12051878
Pan X, Liu J, Zhang S, Huang S, Chen L, Shen X, Chen D. Application of Neuromuscular Blockers in Patients with ARDS in ICU: A Retrospective Study Based on the MIMIC-III Database. Journal of Clinical Medicine. 2023; 12(5):1878. https://doi.org/10.3390/jcm12051878
Chicago/Turabian StylePan, Xiaojun, Jiao Liu, Sheng Zhang, Sisi Huang, Limin Chen, Xuan Shen, and Dechang Chen. 2023. "Application of Neuromuscular Blockers in Patients with ARDS in ICU: A Retrospective Study Based on the MIMIC-III Database" Journal of Clinical Medicine 12, no. 5: 1878. https://doi.org/10.3390/jcm12051878