
Recovery of Corneal Innervation after Treatment in Dry Eye Disease: A Confocal Microscopy Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. In Vivo Confocal Microscopy (IVCM)
2.2. Tear Film Break Up Time
2.3. Schirmer Test
2.4. Diagnostic Questionnaires
2.5. Treatment
2.6. Statistical Analysis
3. Results
3.1. General Results
3.1.1. Corneal Nerve Quantification
3.1.2. Morphological Alterations and Cell Infiltration
3.1.3. Tear Film and Ocular Surface Disease Questionnaires
3.2. Subtypes of Dry Eye Disease
3.2.1. Difference between Subtypes of Dry Eye Disease
3.2.2. Evaporative Dry Eye Subtype
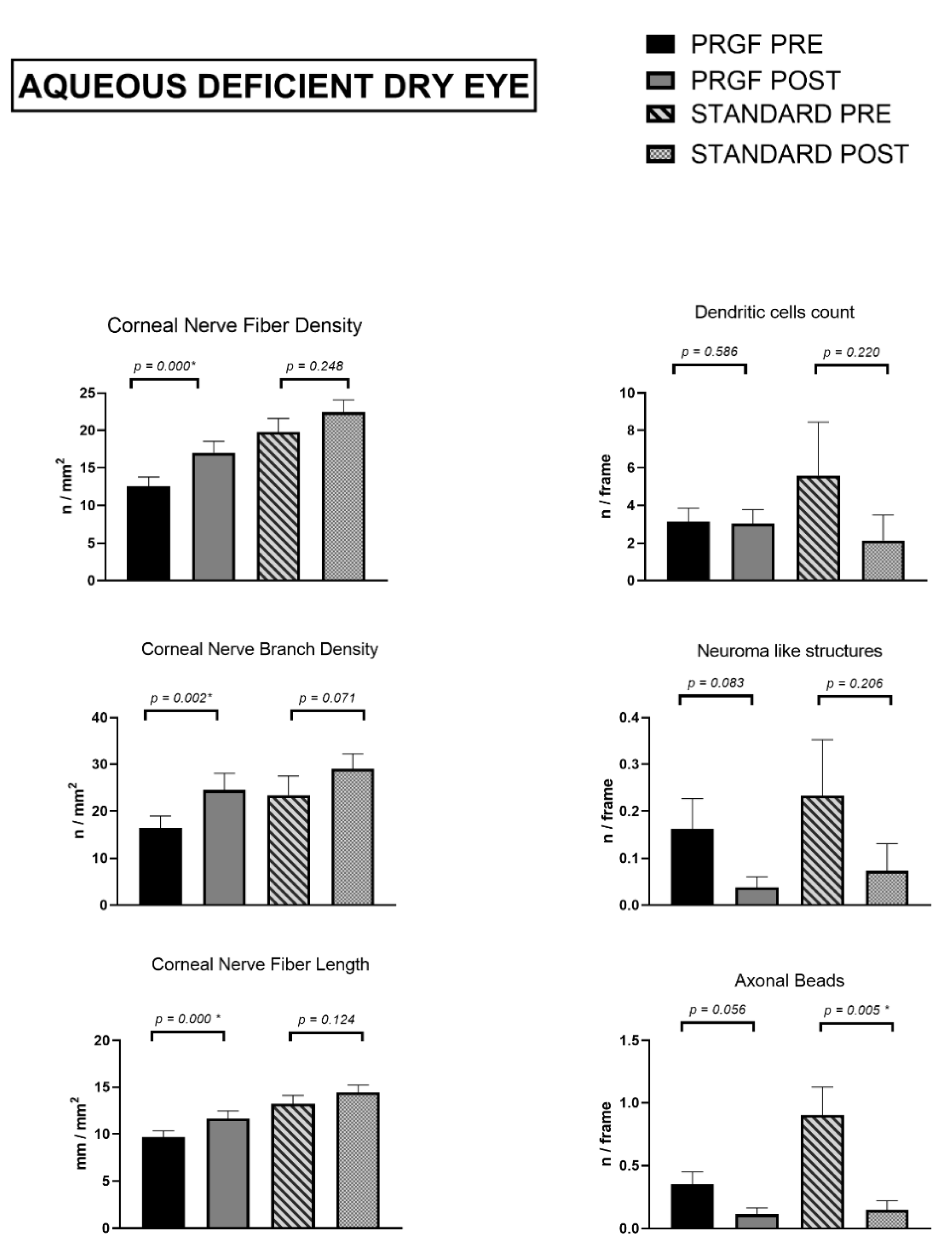
3.2.3. Aqueous Deficient Dry Eye Subtype
3.3. Effect Size
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marfurt, C.F.; Cox, J.; Deek, S.; Dvorscak, L. Anatomy of the Human Corneal Innervation. Exp. Eye Res. 2010, 90, 478–492. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.J.; Marfurt, C.F.; Kruse, F.; Tervo, T.M. Corneal Nerves: Structure, Contents and Function. Exp. Eye Res. 2003, 76, 521–542. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Merayo-Lloves, J. Management Strategies for Evaporative Dry Eye Disease and Future Perspective. Curr. Eye Res. 2022, 47, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology Report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II Pathophysiology Report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ibrahim, O.M.A. Application of in Vivo Confocal Microscopy in Dry Eye Disease. Invest. Ophthalmol. Vis. Sci. 2018, 59, DES41–DES47. [Google Scholar] [CrossRef] [Green Version]
- Said, D.G.; Liu, Y.; Chou, Y.; Dong, X.; Liu, Z.; Jiang, X.; Hao, R.; Li, X. Corneal Subbasal Nerve Analysis Using In Vivo Confocal Microscopy in Patients with Dry Eye: Analysis and Clinical Correlations. Cornea 2019, 38, 1253–1258. [Google Scholar] [CrossRef]
- Ma, B.; Xie, J.; Yang, T.; Su, P.; Liu, R.; Sun, T.; Zhou, Y.; Wang, H.; Feng, X.; Ma, S.; et al. Quantification of Increased Corneal Subbasal Nerve Tortuosity in Dry Eye Disease and Its Correlation with Clinical Parameters. Transl. Vis. Sci. Technol. 2021, 10, 26. [Google Scholar] [CrossRef]
- Cox, S.M.; Kheirkhah, A.; Aggarwal, S.; Abedi, F.; Cavalcanti, B.M.; Cruzat, A.; Hamrah, P. Alterations in Corneal Nerves in Different Subtypes of Dry Eye Disease: An in Vivo Confocal Microscopy Study. Ocul. Surf. 2021, 22, 135–142. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ibrahim, O.M.A.; Kojima, T.; Dogru, M.; Shimazaki, J.; Tsubota, K. Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome. Diagnostics 2020, 10, 497. [Google Scholar] [CrossRef]
- Ahuja, Y.; Baratz, K.H.; McLaren, J.W.; Bourne, W.M.; Patel, S.V. Decreased Corneal Sensitivity and Abnormal Corneal Nerves in Fuchs Endothelial Dystrophy. Cornea 2012, 31, 1257–1263. [Google Scholar] [CrossRef] [Green Version]
- Pal-Ghosh, S.; Tadvalkar, G.; Stepp, M.A. Alterations in Corneal Sensory Nerves During Homeostasis, Aging, and After Injury in Mice Lacking the Heparan Sulfate Proteoglycan Syndecan-1. Invest. Ophthalmol. Vis. Sci. 2017, 58, 4959–4975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopra, R.; Mulholland, P.J.; Hau, S.C. In Vivo Confocal Microscopy Morphological Features and Cyst Density in Acanthamoeba Keratitis. Am. J. Ophthalmol. 2020, 217, 38–48. [Google Scholar] [CrossRef]
- Zhao, H.; He, Y.; Ren, Y.R.; Chen, B.H. Corneal Alteration and Pathogenesis in Diabetes Mellitus. Int. J. Ophthalmol. 2019, 12, 1939–1950. [Google Scholar] [CrossRef]
- Tummanapalli, S.S.; Issar, T.; Kwai, N.; Poynten, A.; Krishnan, A.V.; Willcox, M.; Markoulli, M. Association of Corneal Nerve Loss with Markers of Axonal Ion Channel Dysfunction in Type 1 Diabetes. Clin. Neurophysiol. 2020, 131, 145–154. [Google Scholar] [CrossRef]
- Oudejans, L.; He, X.; Niesters, M.; Dahan, A.; Brines, M.; van Velzen, M. Cornea Nerve Fiber Quantification and Construction of Phenotypes in Patients with Fibromyalgia. Sci. Rep. 2016, 6, 23573. [Google Scholar] [CrossRef] [Green Version]
- Klitsch, A.; Evdokimov, D.; Frank, J.; Thomas, D.; Saffer, N.; Meyer Zu Altenschildesche, C.; Sisignano, M.; Kampik, D.; Malik, R.A.; Sommer, C.; et al. Reduced Association between Dendritic Cells and Corneal Sub-Basal Nerve Fibers in Patients with Fibromyalgia Syndrome. J. Peripher. Nerv. Syst. 2020, 25, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Badian, R.A.; Allgeier, S.; Scarpa, F.; Andréasson, M.; Bartschat, A.; Mikut, R.; Colonna, A.; Bellisario, M.; Utheim, T.P.; Köhler, B.; et al. Wide-Field Mosaics of the Corneal Subbasal Nerve Plexus in Parkinson’s Disease Using in Vivo Confocal Microscopy. Sci. Data 2021, 8, 306. [Google Scholar] [CrossRef]
- Jeziorska, M.; Atkinson, A.; Kass-Iliyya, L.; Kobylecki, C.; Gosal, D.; Marshall, A.; Malik, R.A.; Silverdale, M. Small Fibre Neuropathy in Parkinson’s Disease: Comparison of Skin Biopsies from the More Affected and Less Affected Sides. J. Parkinsons Dis. 2019, 9, 761–765. [Google Scholar] [CrossRef] [Green Version]
- Petropoulos, I.N.; Kamran, S.; Li, Y.; Khan, A.; Ponirakis, G.; Akhtar, N.; Deleu, D.; Shuaib, A.; Malik, R.A. Corneal Confocal Microscopy: An Imaging Endpoint for Axonal Degeneration in Multiple Sclerosis. Invest Ophthalmol. Vis. Sci. 2017, 58, 3677–3681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitirgen, G.; Akpinar, Z.; Uca, A.U.; Ozkagnici, A.; Petropoulos, I.N.; Malik, R.A. Progressive Loss of Corneal and Retinal Nerve Fibers in Patients with Multiple Sclerosis: A 2-Year Follow-up Study. Transl. Vis. Sci. Technol. 2020, 9, 37. [Google Scholar] [CrossRef]
- Testa, V.; de Santis, N.; Scotto, R.; della Giustina, P.; Ferro Desideri, L.; Cellerino, M.; Cordano, C.; Inglese, M.; Uccelli, A.; Vagge, A.; et al. Corneal Epithelial Dendritic Cells in Patients with Multiple Sclerosis: An in Vivo Confocal Microscopy Study. J. Clin. Neurosci. 2020, 81, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.; Queiruga-Piñeiro, J.; Lozano-Sanroma, J.; Alcalde, I.; Gallar, J.; Fernández-Vega Cueto, L.; Alfonso, J.F.; Quirós, L.M.; Merayo-Lloves, J. Small Fiber Neuropathy in the Cornea of Covid-19 Patients Associated with the Generation of Ocular Surface Disease. Ocul. Surf. 2022, 23, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Kallab, M.; Szegedi, S.; Hommer, N.; Stegmann, H.; Kaya, S.; Werkmeister, R.M.; Schmidl, D.; Schmetterer, L.; Garhöfer, G. Topical Low Dose Preservative-Free Hydrocortisone Reduces Signs and Symptoms in Patients with Chronic Dry Eye: A Randomized Clinical Trial. Adv. Ther. 2020, 37, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, A.; van Setten, G.; Amrane, M.; Ismail, D.; Garrigue, J.-S.; Figueiredo, F.C.; Baudouin, C. Efficacy and Safety of 0.1% Cyclosporine a Cationic Emulsion in the Treatment of Severe Dry Eye Disease: A Multicenter Randomized Trial. Eur. J. Ophthalmol. 2016, 26, 287–296. [Google Scholar] [CrossRef] [Green Version]
- Giannaccare, G.; Pellegrini, M.; Sebastiani, S.; Bernabei, F.; Roda, M.; Taroni, L.; Versura, P.; Campos, E.C. Efficacy of Omega-3 Fatty Acid Supplementation for Treatment of Dry Eye Disease: A Meta-Analysis of Randomized Clinical Trials. Cornea 2019, 38, 565–573. [Google Scholar] [CrossRef]
- Fox, R.I.; Chan, R.; Michelson, J.B.; Belmont, J.B.; Michelson, P.E. Beneficial Effect of Artificial Tears Made with Autologous Serum in Patients with Keratoconjunctivitis Sicca. Arthritis Rheum. 1984, 27, 459–461. [Google Scholar] [CrossRef]
- Shtein, R.M.; Shen, J.F.; Kuo, A.N.; Hammersmith, K.M.; Li, J.Y.; Weikert, M.P. Autologous Serum-Based Eye Drops for Treatment of Ocular Surface Disease: A Report by the American Academy of Ophthalmology. Ophthalmology 2020, 127, 128–133. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.; de la Fuente, M.; Riestra, A.; Merayo-Lloves, J.; Orive, G. PRGF Exerts More Potent Proliferative and Anti-Inflammatory Effects than Autologous Serum on a Cell Culture Inflammatory Model. Exp. Eye. Res. 2016, 151, 115–121. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F. PRGF in Equine Corneal Cells: A Standardised Protocol Is the Key to Achieve Accurate Results. Equine Vet. J. 2018, 50, 274–275. [Google Scholar] [CrossRef]
- Sanchez-Avila, R.M.; Merayo-Lloves, J.; Riestra, A.C.; Fernandez-Vega Cueto, L.; Anitua, E.; Begoña, L.; Muruzabal, F.; Orive, G. Treatment of Patients with Neurotrophic Keratitis Stages 2 and 3 with Plasma Rich in Growth Factors (PRGF-Endoret) Eye-Drops. Int. Ophthalmol. 2018, 38, 1193–1204. [Google Scholar] [CrossRef]
- Lopez-Plandolit, S.; Morales, M.C.; Freire, V.; Etxebarria, J.; Duran, J.A. Plasma Rich in Growth Factors as a Therapeutic Agent for Persistent Corneal Epithelial Defects. Cornea 2010, 29, 843–848. [Google Scholar] [CrossRef]
- Ibares-Frias, L.; Gallego-Munoz, P.; Orive, G.; Anitua, E.; Cantalapiedra-Rodriguez, R.; Merayo-Lloves, J.; Martinez-Garcia, M.C. Potential Effect of Plasma Rich in Growth Factors-Endoret in Stromal Wound Healing in Additive Surgery. Ophthalmic. Res. 2020, 63, 203–212. [Google Scholar] [CrossRef]
- Sanchez-Avila, R.M.; Merayo-Lloves, J.; Fernandez, M.L.; Rodriguez-Gutierrez, L.A.; Jurado, N.; Muruzabal, F.; Orive, G.; Anitua, E. Plasma Rich in Growth Factors for the Treatment of Dry Eye after LASIK Surgery. Int. J. Mol. Sci. 2018, 60, 80–86. [Google Scholar] [CrossRef]
- Merayo-Lloves, J.; Sanchez-Avila, R.M.; Riestra, A.C.; Anitua, E.; Begoña, L.; Orive, G.; Fernandez-Vega, L. Safety and Efficacy of Autologous Plasma Rich in Growth Factors Eye Drops for the Treatment of Evaporative Dry Eye. Ophthalmic. Res. 2016, 56, 68–73. [Google Scholar] [CrossRef]
- Lopez-Plandolit, S.; Morales, M.C.; Freire, V.; Grau, A.E.; Duran, J.A. Efficacy of Plasma Rich in Growth Factors for the Treatment of Dry Eye. Cornea 2011, 30, 1312–1317. [Google Scholar] [CrossRef]
- Jongkhajornpong, P.; Numthavaj, P.; Anothaisintawee, T.; Lekhanont, K.; Mckay, G.; Attia, J.; Thakkinstian, A. Comparison of Treatment Efficacy between 100% Platelet-Rich Plasma and 100% Serum Eye Drops in Moderate-to-Severe Dry Eye Disease: A Randomised Controlled Trial Protocol. BMJ Open 2021, 11, 479. [Google Scholar] [CrossRef]
- Willcox, M.D.P.; Argueso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Dabbah, M.A.; Graham, J.; Petropoulos, I.; Tavakoli, M.; Malik, R.A. Dual-Model Automatic Detection of Nerve-Fibres in Corneal Confocal Microscopy Images. Med. Image Comput. Comput. Assist. Interv. 2010, 13, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Petropoulos, I.N.; Manzoor, T.; Morgan, P.; Fadavi, H.; Asghar, O.; Alam, U.; Ponirakis, G.; Dabbah, M.A.; Chen, X.; Graham, J.; et al. Repeatability of in Vivo Corneal Confocal Microscopy to Quantify Corneal Nerve Morphology. Cornea 2013, 32, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’brien, J.; Hayder, H.; Peng, C. Automated Quantification and Analysis of Cell Counting Procedures Using ImageJ Plugins. J. Vis. Exp. 2016, 117, e54719. [Google Scholar] [CrossRef]
- Stepp, M.A.; Pal-Ghosh, S.; Downie, L.E.; Zhang, A.C.; Chinnery, H.R.; Machet, J.; di Girolamo, N. Corneal Epithelial “Neuromas”: A Case of Mistaken Identity? Cornea 2020, 39, 930–934. [Google Scholar] [CrossRef] [PubMed]
- Moein, H.R.; Akhlaq, A.; Dieckmann, G.; Abbouda, A.; Pondelis, N.; Salem, Z.; Müller, R.T.; Cruzat, A.; Cavalcanti, B.M.; Jamali, A.; et al. Visualization of Microneuromas by Using in Vivo Confocal Microscopy: An Objective Biomarker for the Diagnosis of Neuropathic Corneal Pain? Ocular Surf. 2020, 18, 651–656. [Google Scholar] [CrossRef]
- Li, N.; Deng, X.-G.; He, M.-F. Comparison of the Schirmer I Test with and without Topical Anesthesia for Diagnosing Dry Eye. Int. J. Ophthalmol. 2012, 5, 478–481. [Google Scholar] [CrossRef]
- Tsubota, K.; Kaido, M.; Yagi, Y.; Fujihara, T.; Shimmura, S. Diseases Associated with Ocular Surface Abnormalities: The Importance of Reflex Tearing. Br. J. Ophthalmol. 1999, 83, 89–91. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Muruzabal, F.; de la Fuente, M.; Merayo, J.; Duran, J.; Orive, G. Plasma Rich in Growth Factors for the Treatment of Ocular Surface Diseases. Curr. Eye Res. 2016, 41, 875–882. [Google Scholar] [CrossRef]
- Anitua, E.; de la Fuente, M.; Riestra, A.; Merayo-Lloves, J.; Muruzábal, F.; Orive, G. Preservation of Biological Activity of Plasma and Platelet-Derived Eye Drops After Their Different Time and Temperature Conditions of Storage. Cornea 2015, 34, 1144–1148. [Google Scholar] [CrossRef]
- Anitua, E.; de la Fuente, M.; Muruzabal, F.; Riestra, A.; Merayo-Lloves, J.; Orive, G. Plasma Rich in Growth Factors (PRGF) Eye Drops Stimulates Scarless Regeneration Compared to Autologous Serum in the Ocular Surface Stromal Fibroblasts. Exp. Eye Res. 2015, 135, 118–126. [Google Scholar] [CrossRef]
- Celebi, A.R.C.; Ulusoy, C.; Mirza, G.E. The Efficacy of Autologous Serum Eye Drops for Severe Dry Eye Syndrome: A Randomized Double-Blind Crossover Study. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 619–626. [Google Scholar] [CrossRef]
- Giannaccare, G.; Pellegrini, M.; Bernabei, F.; Moscardelli, F.; Buzzi, M.; Versura, P.; Campos, E.C. In Vivo Confocal Microscopy Automated Morphometric Analysis of Corneal Subbasal Nerve Plexus in Patients With Dry Eye Treated With Different Sources of Homologous Serum Eye Drops. Cornea 2019, 38, 1412–1417. [Google Scholar] [CrossRef]
- Mahelkova, G.; Jirsova, K.; Seidler Stangova, P.; Palos, M.; Vesela, V.; Fales, I.; Jiraskova, N.; Dotrelova, D. Using Corneal Confocal Microscopy to Track Changes in the Corneal Layers of Dry Eye Patients after Autologous Serum Treatment. Clin. Exp. Optom. 2017, 100, 243–249. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.; de la Fuente, M.; Merayo-Lloves, J.; Orive, G. Effects of Heat-Treatment on Plasma Rich in Growth Factors-Derived Autologous Eye Drop. Exp. Eye Res. 2014, 119, 27–34. [Google Scholar] [CrossRef]
- Periman, L.M.; Perez, V.L.; Saban, D.R.; Lin, M.C.; Neri, P. The Immunological Basis of Dry Eye Disease and Current Topical Treatment Options. J. Ocul. Pharmacol. Ther. 2020, 36, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Muruzabal, F.; Alcalde, I.; Merayo-Lloves, J.; Orive, G. Plasma Rich in Growth Factors (PRGF-Endoret) Stimulates Corneal Wound Healing and Reduces Haze Formation after PRK Surgery. Exp. Eye Res. 2013, 115, 153–161. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Merayo-Lloves, J.; de la Fuente, M.; Muruzabal, F.; Orive, G. Plasma Rich in Growth Factors (PRGF-Endoret) Stimulates Proliferation and Migration of Primary Keratocytes and Conjunctival Fibroblasts and Inhibits and Reverts TGF-Beta1-Induced Myodifferentiation. Invest. Ophthalmol. Vis. Sci. 2011, 52, 6066–6073. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.; Tayebba, A.; Riestra, A.; Perez, V.L.; Merayo-Lloves, J.; Orive, G. Autologous Serum and Plasma Rich in Growth Factors in Ophthalmology: Preclinical and Clinical Studies. Acta Ophthalmol. 2015, 93, e605–e614. [Google Scholar] [CrossRef]
- Lambiase, A.; Manni, L.; Bonini, S.; Rama, P.; Micera, A.; Aloe, L. Nerve Growth Factor Promotes Corneal Healing: Structural, Biochemical, and Molecular Analyses of Rat and Human Corneas. Invest Ophthalmol. Vis. Sci. 2000, 41, 1063–1069. [Google Scholar]
- Tepelus, T.C.; Chiu, G.B.; Huang, J.; Huang, P.; Sadda, S.V.R.; Irvine, J.; Lee, O.L. Correlation between Corneal Innervation and Inflammation Evaluated with Confocal Microscopy and Symptomatology in Patients with Dry Eye Syndromes: A Preliminary Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 1771–1778. [Google Scholar] [CrossRef]
- Merayo-Lloves, J.; Rushton, J.O. Effects of Three Blood Derived Products on Equine Corneal Cells, an in Vitro Study. Equine Vet. J. 2018, 50, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Kheirkhah, A.; Dohlman, T.H.; Amparo, F.; Arnoldner, M.A.; Jamali, A.; Hamrah, P.; Dana, R. Effects of Corneal Nerve Density on the Response to Treatment in Dry Eye Disease. Ophthalmology 2015, 122, 662–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villani, E.; Garoli, E.; Termine, V.; Pichi, F.; Ratiglia, R.; Nucci, P. Corneal Confocal Microscopy in Dry Eye Treated with Corticosteroids. Optom. Vis. Sci. 2015, 92, e290–e295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, O.; Labbé, A.; Borderie, V.; Hamiche, T.; Dupas, B.; Laroche, L.; Baudouin, C.; Bouheraoua, N. Increased Corneal Sub-Basal Nerve Density in Patients with Sjögren Syndrome Treated with Topical Cyclosporine A. Clin. Exp. Ophthalmol. 2017, 45, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaccheri, B.; Torroni, G.; Cagini, C.; Fiore, T.; Cerquaglia, A.; Lupidi, M.; Cillino, S.; Dua, H.S. Corneal Confocal Scanning Laser Microscopy in Patients with Dry Eye Disease Treated with Topical Cyclosporine. Eye 2017, 31, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Tian, Y.; Wang, S. The Correlation of Cytokines and Sensory Hypersensitivity in Mild Dry Eye Patients Characterized by Symptoms Outweighing Signs—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/32476816/ (accessed on 23 January 2023).
- Lemp, M.A.; Baudouin, C.; Baum, J.; Dogru, M.; Foulks, G.N.; Kinoshita, S.; Laibson, P.; McCulley, J.; Murube, J.; Pflugfelder, S.C.; et al. The Definition and Classification of Dry Eye Disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf 2007, 5, 75–92. [Google Scholar] [CrossRef]
- Aragona, P.; Giannaccare, G.; Mencucci, R.; Rubino, P.; Cantera, E.; Rolando, M. Modern Approach to the Treatment of Dry Eye, a Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board Review. Br. J. Ophthalmol. 2021, 105, 446–453. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standard Treatment | PRGF Treatment | ||||
|---|---|---|---|---|---|
| n/Mean | ±SEM | n/Mean | ±SEM | p Value | |
| Number of subjects | 32 | - | 51 | - | - |
| Age | 55.13 | 2.08 | 56.08 | 2.29 | 0.766 |
| Sex distribution (female/male) | 23/9 | - | 39/12 | - | 0.639 |
| Previous OSDI Score | 36.12 | 3.38 | 43.17 | 3.52 | 0.219 |
| Previous Break Up Time | 5.27 | 0.58 | 4.93 | 0.47 | 0.581 |
| Time of treatment (months) | 4.75 | 0.62 | 4.80 | 0.55 | 0.621 |
| Standard Treatment | PRGF Treatment | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | |||||
| Mean (±SEM) | Mean (±SEM) | p Value | Effect Size | Mean (±SEM) | Mean (±SEM) | p Value | Effect Size | |
| OSDI SCORE | 36.119 ± 3.386 | 25.456 ± 3.680 | 0.002* | 0.412 | 43.169 ± 3.520 | 31.553 ± 2.926 | 0.005 * | 0.366 |
| SCHIRMER (mm) | 7.193 ± 1.277 | 5.875 ± 1.159 | 0.194 | 0.136 | 5.340 ± 0.561 | 6.125 ± 0.738 | 0.685 | 0.121 |
| FBut (sec) | 5.269 ± 0.588 | 4.875 ± 0.595 | 0.654 | 0.087 | 4.935 ± 0.468 | 6.106 ± 0.463 | 0.003 * | 0.262 |
| SANDE Frequency | 65.000 ± 4.512 | 41.093 ± 4.455 | 0.000* | 0.666 | 70.102 ± 4.196 | 39.591 ± 3.263 | 0.000 * | 0.820 |
| SANDE Severity | 56.719 ± 4.113 | 34.687 ± 4.312 | 0.000* | 0.654 | 65.510 ± 3.557 | 35.102 ± 3.142 | 0.000 * | 0.915 |
| CNFD (n/mm2) | 19.572 ± 1.188 | 19.340 ± 1.615 | 0.859 | 0.020 | 13.827 ± 1.019 | 17.556 ± 1.162 | 0.000 * | 0.338 |
| CNBD (n/mm2) | 22.874 ± 2.728 | 24.672 ± 2.925 | 0.432 | 0.079 | 17.440 ± 2.092 | 23.796 ± 2.762 | 0.002 * | 0.257 |
| CNFL (mm/mm2) | 13.087 ± 0.590 | 12.965 ± 0.677 | 0.832 | 0.024 | 10.177 ± 0.537 | 11.863 ± 0.603 | 0.000 * | 0.293 |
| CTBD (n/mm2) | 38.181 ± 3.751 | 41.022 ± 4.118 | 0.466 | 0.190 | 32.257 ± 3.158 | 40.925 ± 4.148 | 0.012 * | 0.233 |
| CNFA (mm2/mm2) | 0.0059 ± 0.0003 | 0.0057 ± 0.0003 | 0.607 | 0.078 | 0.0053 ± 0.0003 | 0.0057 ± 0.0003 | 0.004 * | 0.123 |
| CNFW (mm/mm2) | 0.0213 ± 0.0002 | 0.0215 ± 0.0002 | 0.400 | 0.091 | 0.0222 ± 0.0003 | 0.0220 ± 0.0002 | 0.368 | 0.060 |
| CNFrD | 1.4638 ± 0.009 | 1.4684 ± 0.006 | 0.801 | 0.072 | 1.4331 ± 0.010 | 1.4500 ± 0.009 | 0.004 * | 0.229 |
| Dendritic cells (n/frame) | 4.9519 ± 1.810 | 2.3541 ± 1.252 | 0.039 * | 0.209 | 3.1908 ± 0.549 | 2.5806 ± 0.545 | 0.077 | 0.110 |
| Neuroma (n/frame) | 0.1984 ± 0.075 | 0.0519 ± 0.034 | 0.064 | 0.315 | 0.1465 ± 0.049 | 0.0692 ± 0.042 | 0.104 | 0.167 |
| Axonal Beads (n/frame) | 0.6694 ± 0.147 | 0.1669 ± 0.561 | 0.002 * | 0.564 | 0.3890 ± 0.078 | 0.1278 ± 0.052 | 0.008 * | 0.389 |
| Evaporative Dry Eye | Aqueous Deficient Dry Eye | |||
|---|---|---|---|---|
| Standard Treatment | PRGF Treatment | Standard Treatment | PRGF Treatment | |
| CNFD | 0.366 ↓ | 0.288 ↑ | 0.263 ↑ | 0.413 ↑ |
| CNBD | 0.135 ↓ | 0.111 ↑ | 0.253 ↑ | 0.308 ↑ |
| CNFL | 0.402 ↓ | 0.162 ↑ | 0.243 ↑ | 0.322 ↑ |
| Dendritic cells | 0.130 ↓ | 0.432 ↓ | 0.258 ↓ | 0.054 ↓ |
| Neuromas | 0.141 ↓ | 0.117 ↑ | 0.282 ↓ | 0.321 ↓ |
| Beadings | 0.277 ↓ | 0.184 ↓ | 0.756 ↓ | 0.379 ↓ |
| Break Up Time | 0.096 ↑ | 0.052 ↓ | 0.274 ↓ | 0.464 ↑ |
| Schirmer | 0.521 ↓ | 0.261 ↓ | 0.272 ↑ | 0.379 ↑ |
| OSDI Score | 0.183 ↓ | 0.015 ↑ | 0.539 ↓ | 0.509 ↓ |
| SANDE Frequency | 0.661 ↓ | 1.398 ↓ | 0.663 ↓ | 0.874 ↓ |
| SANDE Intensity | 0.822 ↓ | 1.235 ↓ | 0.506 ↓ | 0.948 ↓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barros, A.; Lozano-Sanroma, J.; Queiruga-Piñeiro, J.; Fernández-Vega Cueto, L.; Anitua, E.; Alcalde, I.; Merayo-Lloves, J. Recovery of Corneal Innervation after Treatment in Dry Eye Disease: A Confocal Microscopy Study. J. Clin. Med. 2023, 12, 1841. https://doi.org/10.3390/jcm12051841
Barros A, Lozano-Sanroma J, Queiruga-Piñeiro J, Fernández-Vega Cueto L, Anitua E, Alcalde I, Merayo-Lloves J. Recovery of Corneal Innervation after Treatment in Dry Eye Disease: A Confocal Microscopy Study. Journal of Clinical Medicine. 2023; 12(5):1841. https://doi.org/10.3390/jcm12051841
Chicago/Turabian StyleBarros, Alberto, Javier Lozano-Sanroma, Juan Queiruga-Piñeiro, Luis Fernández-Vega Cueto, Eduardo Anitua, Ignacio Alcalde, and Jesús Merayo-Lloves. 2023. "Recovery of Corneal Innervation after Treatment in Dry Eye Disease: A Confocal Microscopy Study" Journal of Clinical Medicine 12, no. 5: 1841. https://doi.org/10.3390/jcm12051841