
Real Life Data on OnabotulinumtoxinA for Treatment of Chronic Migraine in Pediatric Age
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F.; AMPP Advisory Group. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Steiner, T.J.; Stovner, L.J.; Vos, T.; Jensen, R.; Katsarava, Z. Migraine is first cause of disability in under 50 s: Will health politicians now take notice? J. Headache Pain 2018, 19, 17. [Google Scholar] [CrossRef] [PubMed]
- Wöber-Bingöl, C. Epidemiology of migraine and headache in children and adolescents. Curr. Pain Headache Rep. 2013, 17, 341. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Papetti, L.; Salfa, I.; Battan, B.; Moavero, R.; Termine, C.; Bartoli, B.; Di Nunzio, F.; Tarantino, S.; Alaimo Di Loro, P.; Vigevano, F.; et al. Features of Primary Chronic Headache in Children and Adolescents and Validity of Ichd 3 Criteria. Front. Neurol. 2019, 10, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papetti, L.; Ursitti, F.; Moavero, R.; Ferilli, M.A.N.; Sforza, G.; Tarantino, S.; Vigevano, F.; Valeriani, M. Prophylactic Treatment of Pediatric Migraine: Is There Anything New in the Last Decade? Front. Neurol. 2019, 10, 771. [Google Scholar] [CrossRef] [Green Version]
- Binder, W.J.; Brin, M.F.; Blitzer, A.; Schoenrock, L.D.; Pogoda, J.M. Botulinum toxin type A (BOTOX) for treatment of migraine headaches: An open-label study. Otolaryngol. Head Neck Surg. 2000, 123, 669–676. [Google Scholar] [CrossRef]
- Burstein, R.; Blumenfeld, A.M.; Silberstein, S.D.; Manack Adams, A.; Brin, M.F. Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review. Headache 2020, 60, 1259–1272. [Google Scholar] [CrossRef]
- Mahrhold, S.; Rummel, A.; Bigalke, H.; Davletov, B.; Binz, T. The synaptic vesicle protein 2C mediates the uptake of botulinum neurotoxin A into phrenic nerves. FEBS Lett. 2006, 580, 2011–2014. [Google Scholar] [CrossRef] [Green Version]
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–43. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef]
- Lanteri-Minet, M.; Ducros, A.; Francois, C.; Olewinska, E.; Nikodem, M.; Dupont-Benjamin, L. Effectiveness of onabotulinumtoxinA (BOTOX®) for the preventive treatment of chronic migraine: A meta-analysis on 10 years of real-world data. Cephalalgia 2022, 42, 1543–1564. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Frishberg, B.M.; Schim, J.D.; Iannone, A.; Schneider, G.; Yedigarova, L.; Manack Adams, A. Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA: A Retrospective Chart Review. Pain Ther. 2021, 10, 809–826. [Google Scholar] [CrossRef]
- Goenka, A.; Grace Yu, S.; Chikkannaiah, M.; George, M.C.; MacDonald, S.; Stolfi, A.; Kumar, G. Generalized Anxiety Disorder: A Predictor for Poor Responsiveness to Botulinum Toxin Type A Therapy for Pediatric Migraine. Pediatr. Neurol. 2022, 130, 21–27. [Google Scholar] [CrossRef]
- Shah, S.; Calderon, M.D.; Wu, W.; Grant, J.; Rinehart, J. Onabotulinumtoxin A (BOTOX®) for Prophylactic Treatment of Pediatric Migraine: A Retrospective Longitudinal Analysis. J. Child Neurol. 2018, 33, 580–586. [Google Scholar] [CrossRef]
- Kabbouche, M.; O’Brien, H.; Hershey, A.D. OnabotulinumtoxinA in pediatric chronic daily headache. Curr. Neurol. Neurosci. Rep. 2012, 12, 114–117. [Google Scholar] [CrossRef]
- Shah, S.; Calderon, M.D.; Crain, N.; Pham, J.; Rinehart, J. Effectiveness of onabotulinumtoxinA (BOTOX) in pediatric patients experiencing migraines: A randomized, double-blinded, placebo controlled crossover study in the pediatric pain population. Reg. Anesth. Pain Med. 2021, 46, 41–48. [Google Scholar] [CrossRef]
- Winner, P.K.; Kabbouche, M.; Yonker, M.; Wangsadipura, V.; Lum, A.; Brin, M.F. A Randomized Trial to Evaluate OnabotulinumtoxinA for Prevention of Headaches in Adolescents with Chronic Migraine. Headache 2020, 60, 564–575. [Google Scholar] [CrossRef] [Green Version]
- Marshall, A.; Lindsay, R.; Clementi, M.A.; Gelfand, A.A.; Orr, S.L. Outpatient Approach to Resistant and Refractory Migraine in Children and Adolescents: A Narrative Review. Curr. Neurol. Neurosci. Rep. 2022, 22, 611–624. [Google Scholar] [CrossRef]
- Greene, K.A.; Gentile, C.P.; Szperka, C.L.; Yonker, M.; Gelfand, A.A.; Grimes, B.; Irwin, S.L. Calcitonin Gene-Related Peptide Monoclonal Antibody Use for the Preventive Treatment of Refractory Headache Disorders in Adolescents. Pediatr. Neurol. 2021, 114, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med. Assoc. J. 2012, 184, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Herd, C.P.; Tomlinson, C.L.; Rick, C.; Scotton, W.J.; Edwards, J.; Ives, N.J.; Clarke, C.E.; Sinclair, A.J. Cochrane systematic review and meta-analysis of botulinum toxin for the prevention of migraine. BMJ Open 2019, 9, e027953. [Google Scholar] [CrossRef] [Green Version]
- Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Diener, H.C.; DeGryse, R.E.; Lipton, R.B.; Turkel, C.C. Per cent of patients with chronic migraine who responded per onabotulinumtoxinA treatment cycle: PREEMPT. J. Neurol. Neurosurg. Psychiatry 2015, 86, 996–1001. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Diener, H.C.; DeGryse, R.E.; Turkel, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Winner, P.K.; Blumenfeld, A.M.; Eross, E.J.; Orejudos, A.C.; Mirjah, D.L.; Adams, A.M.; Brin, M.F. Long-Term Safety and Tolerability of OnabotulinumtoxinA Treatment in Patients with Chronic Migraine: Results of the COMPEL Study. Drug Saf. 2019, 42, 1013–1024. [Google Scholar] [CrossRef] [Green Version]
- Ornello, R.; Baraldi, C.; Ahmed, F.; Negro, A.; Miscio, A.M.; Santoro, A.; Alpuente, A.; Russo, A.; Silvestro, M.; Cevoli, S.; et al. Excellent Response to OnabotulinumtoxinA: Different Definitions, Different Predictors. Int. J. Environ. Res. Public Health 2022, 19, 10975. [Google Scholar] [CrossRef]
- Lee, M.J.; Lee, C.; Choi, H.; Chung, C.S. Factors associated with favourable outcome in botulinum toxin A treatment for chronic migraine: A clinic-based prospective study. J. Neurol. Sci 2016, 363, 51–54. [Google Scholar] [CrossRef]
- Alpuente, A.; Gallardo, V.J.; Torres-Ferrús, M.; Álvarez-Sabin, J.; Pozo-Rosich, P. Short and mid-term predictors of response to onabotulinumtoxinA: Real-life experience observational study. Headache 2020, 60, 677–685. [Google Scholar] [CrossRef]
- Domínguez, C.; Pozo-Rosich, P.; Leira, Y.; Leira, R. Unilateral pain and shorter duration of chronic migraine are significant predictors of response to onabotulinumtoxin A. Eur. J. Neurol. 2018, 25, e48. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Mean 14.7 ± 1.5 SD Range: 12–17 |
| Sex | 9 males (19.6%) 37 females (80.4%) |
| Duration of migraine history (months) Concomitant medication overuse headache (MOH) | Mean 29.3 ± 9.1 SD Range: 8–36 7 subjects (15%) |
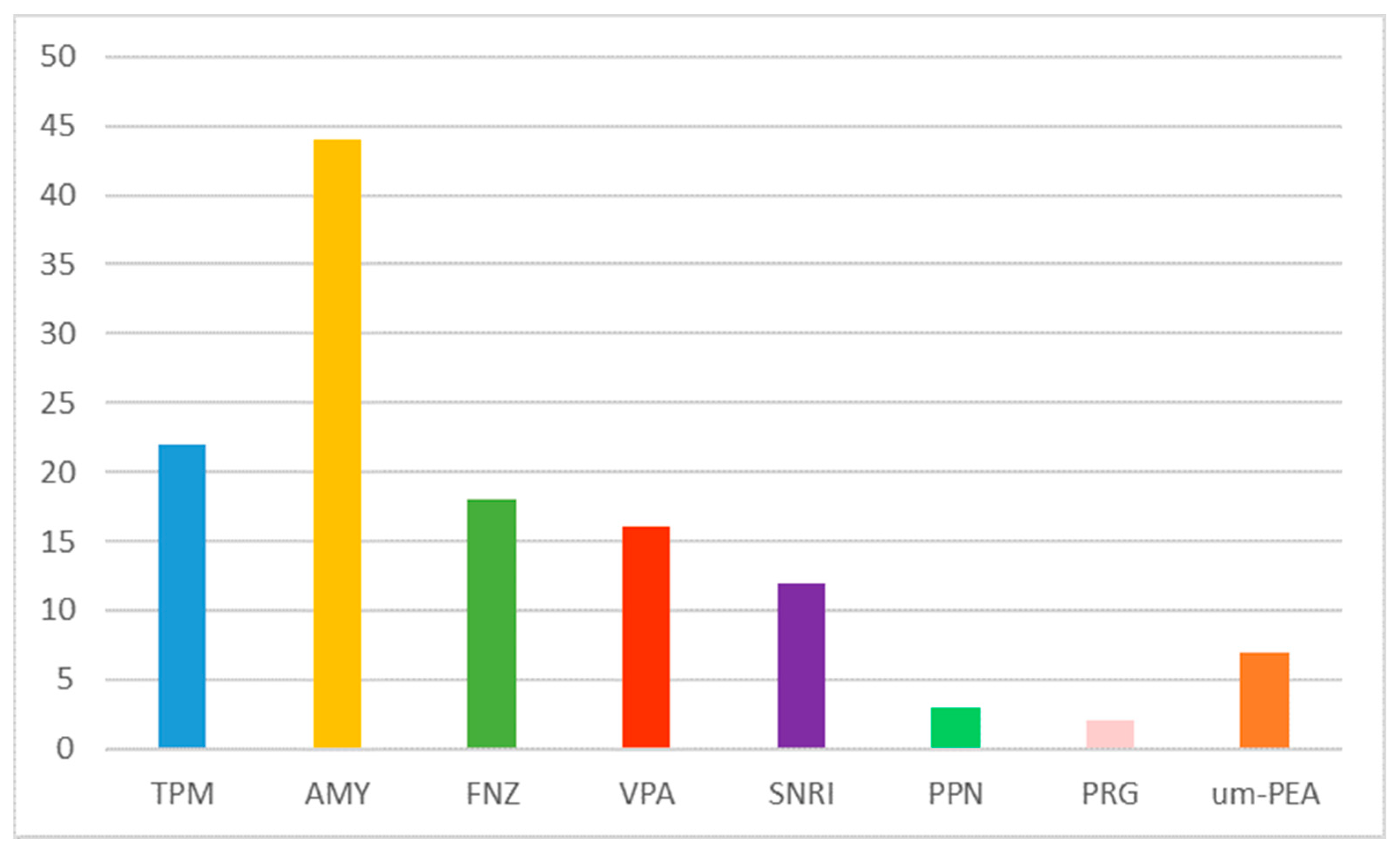
| Previous prophylactic treatment n° (%) | Amitriptyline 44 (95.7%) Topiramate 22 (47.8%) Flunarizine 18 (39.1%) Valproate 16 (34.8%) Duloxetine 12 (26.1%) Propanolol 3 (6.5%) Pregabalin 2 (4.3%) Ultra-micronized palmitoylethanolamide (um-PEA) 7 (15.2%) Cognitive behavioral therapy 30 (65.2%) |
| Day with headache for month | Mean: 26.5 ± 5.8 SD Range: 15–31 |
| Number of inoculums (mean + SD; range) | Mean: 3.4 ± 3 SD Range: 1–17 |
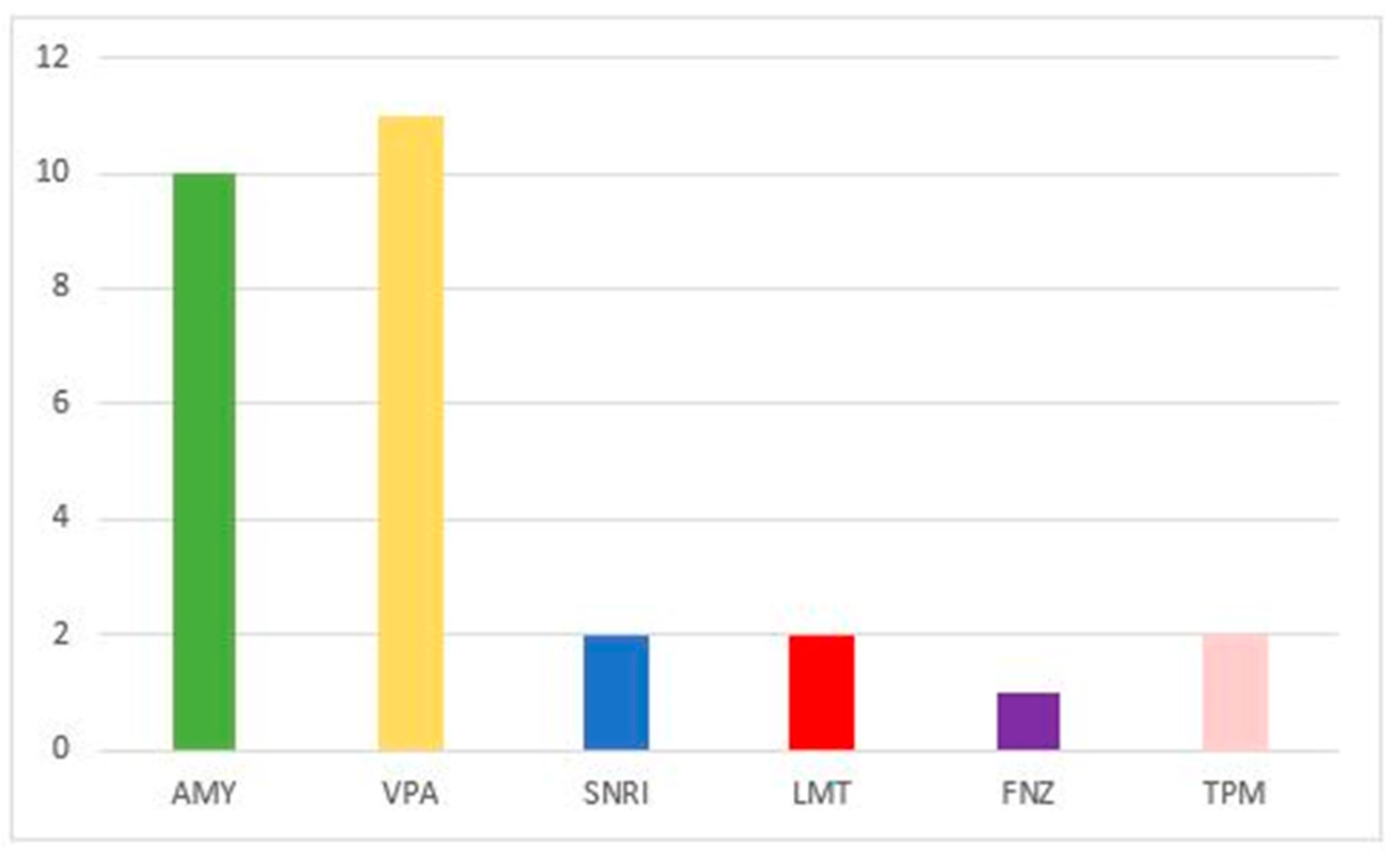
| Associated drug n° (%) | None 18 (39.1%) Amitriptyline 10 (21.7%) Valproate 11 (23.9%) Duloxetine 2 (4.3%) Lamotrigine 2 (4.3%) Flunarizine 1 (2.2%) Topiramate 1 (2.2%) |
| Patients Performed Tests (n° 37) | Total | Non-Responder (n° 14) | Responder (n° 23) | Sig. p |
|---|---|---|---|---|
| No Depression | 8 | 4 (28.6%) | 4 (17.4%) | 0.343 |
| Mild Depression | 11 | 3 (21.4%) | 8 (34.8%) | 0.316 |
| Moderate Depression | 10 | 4 (28.6%) | 6 (26.1%) | 0.58 |
| Severe Depression | 8 | 3 (21.4%) | 5 (21.7%) | 0.657 |
| No Anxiety | 7 | 3 (21.4%) | 4 (17.4%) | 0.541 |
| Mild Anxiety | 10 | 2 (14.3%) | 8 (34.8%) | 0.164 |
| Moderate Anxiety | 11 | 5 (35.7%) | 6 (26.1%) | 0.397 |
| Severe Anxiety | 9 | 4 (28.6%) | 5 (21.7%) | 0.464 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papetti, L.; Frattale, I.; Ursitti, F.; Sforza, G.; Monte, G.; Ferilli, M.A.N.; Tarantino, S.; Proietti Checchi, M.; Valeriani, M. Real Life Data on OnabotulinumtoxinA for Treatment of Chronic Migraine in Pediatric Age. J. Clin. Med. 2023, 12, 1802. https://doi.org/10.3390/jcm12051802
Papetti L, Frattale I, Ursitti F, Sforza G, Monte G, Ferilli MAN, Tarantino S, Proietti Checchi M, Valeriani M. Real Life Data on OnabotulinumtoxinA for Treatment of Chronic Migraine in Pediatric Age. Journal of Clinical Medicine. 2023; 12(5):1802. https://doi.org/10.3390/jcm12051802
Chicago/Turabian StylePapetti, Laura, Ilaria Frattale, Fabiana Ursitti, Giorgia Sforza, Gabriele Monte, Michela Ada Noris Ferilli, Samuela Tarantino, Martina Proietti Checchi, and Massimiliano Valeriani. 2023. "Real Life Data on OnabotulinumtoxinA for Treatment of Chronic Migraine in Pediatric Age" Journal of Clinical Medicine 12, no. 5: 1802. https://doi.org/10.3390/jcm12051802