
Deep Brain Stimulation Electrode Reconstruction: Comparison between Lead-DBS and Surgical Planning System
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Preoperative Assessment
2.2. Surgical Procedures
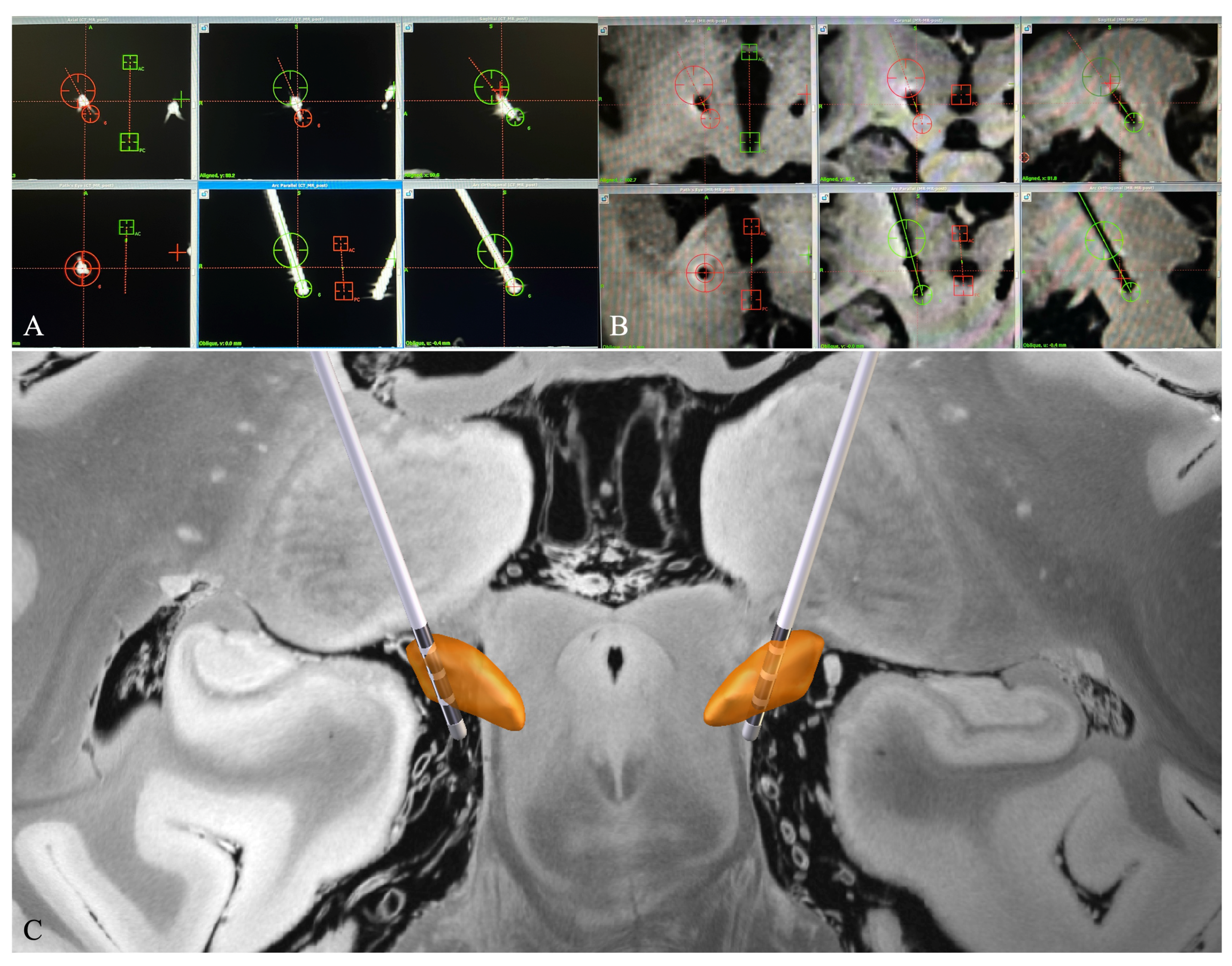
2.3. Postoperative Electrode Localization
2.3.1. Electrode Reconstruction in Surgiplan
2.3.2. Electrode Reconstruction in Lead-DBS
2.4. Relative Position between the Electrode and the DBS Target
2.5. Euclidean Distance between the Electrode Tip and the Pre-Defined Target
2.6. DBS Parameter Programming and Patient Follow-Up
2.7. Data Analysis and Statistics
3. Results
3.1. Patient Characteristics
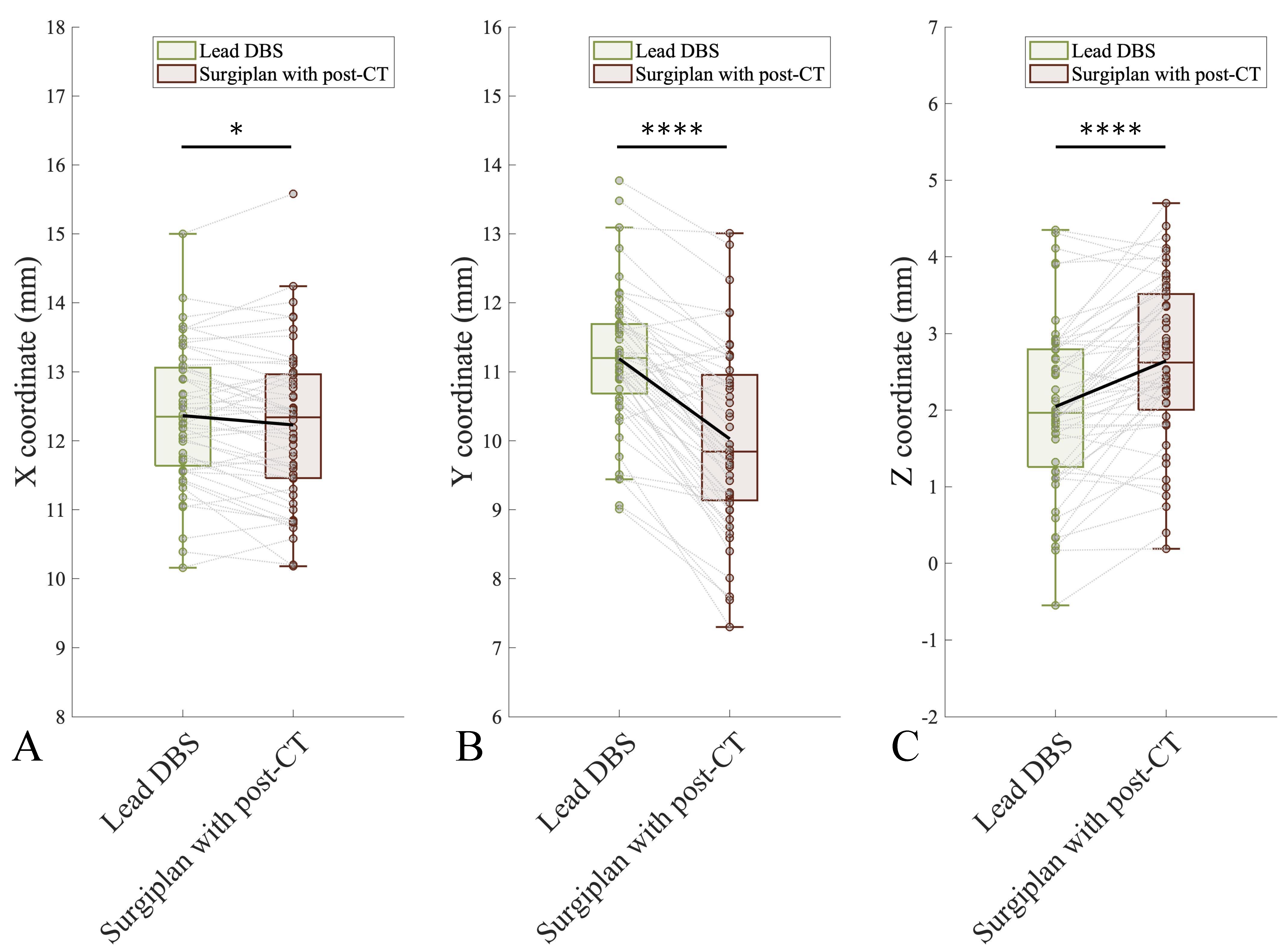
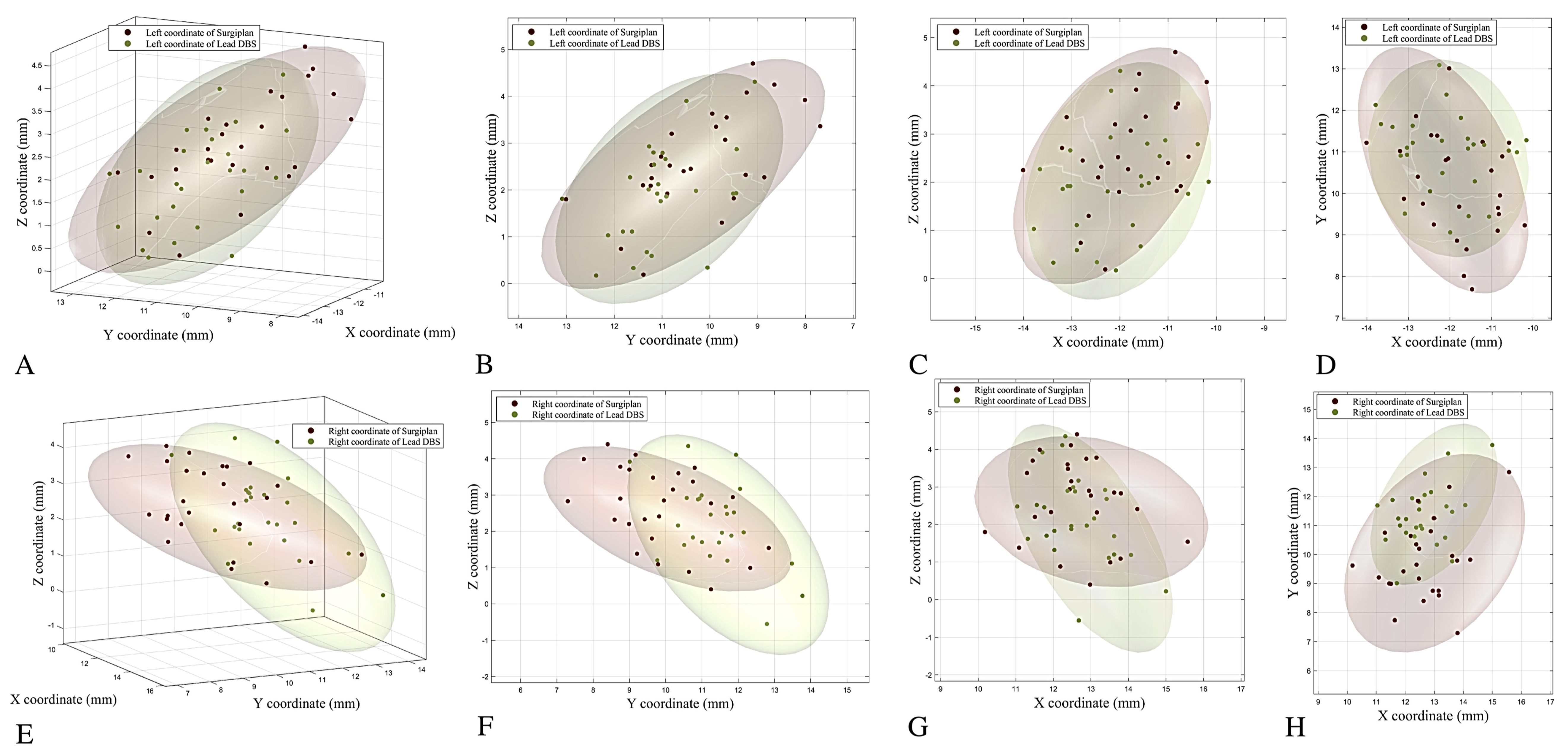
3.2. Comparison of the Coordinates between Lead-DBS and Surgiplan with Postoperative CT
3.3. Comparison of Calculated Coordinates between Lead-DBS, Surgiplan with Postoperative CT, and Surgiplan with MRI
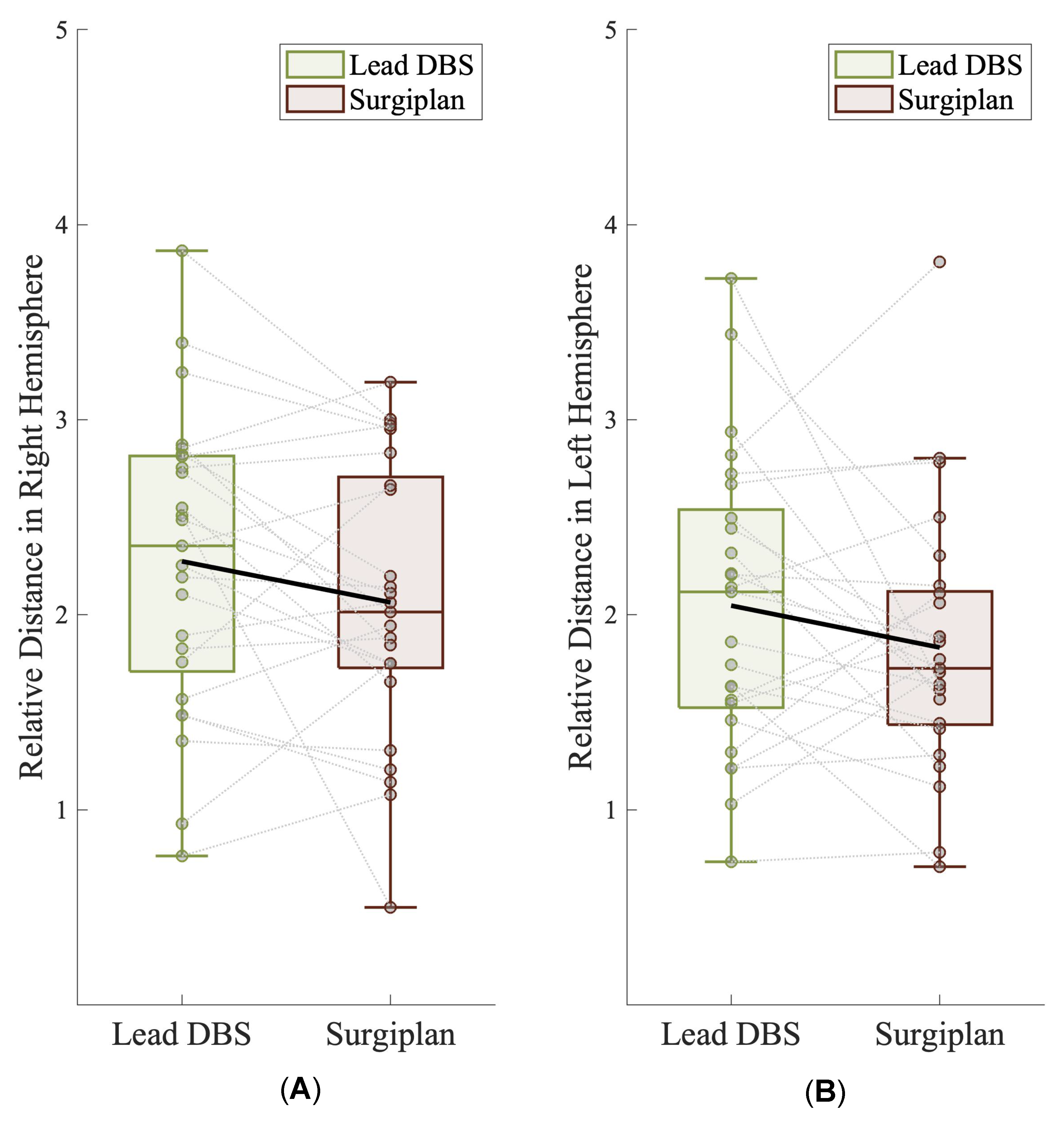
3.4. Relative Position of the Electrode and the DBS Target
3.5. Validation of Lead-DBS According to the Euclidean Distance and Clinical Follow-Up Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krauss, J.K.; Lipsman, N.; Aziz, T.; Boutet, A.; Brown, P.; Chang, J.W.; Davidson, B.; Grill, W.M.; Hariz, M.I.; Horn, A.; et al. Technology of deep brain stimulation: Current status and future directions. Nat. Rev. Neurol. 2021, 17, 75–87. [Google Scholar] [CrossRef]
- Okun, M.S.; Tagliati, M.; Pourfar, M.; Fernandez, H.H.; Rodriguez, R.L.; Alterman, R.L.; Foote, K.D. Management of referred deep brain stimulation failures: A retrospective analysis from 2 movement disorders centers. Arch. Neurol. 2005, 62, 1250–1255. [Google Scholar] [CrossRef] [Green Version]
- Holl, E.M.; Petersen, E.A.; Foltynie, T.; Martinez-Torres, I.; Limousin, P.; Hariz, M.I.; Zrinzo, L. Improving targeting in image-guided frame-based deep brain stimulation. Neurosurgery 2010, 67, 437–447. [Google Scholar] [CrossRef]
- Haynes, W.I.; Haber, S.N. The organization of prefrontal-subthalamic inputs in primates provides an anatomical substrate for both functional specificity and integration: Implications for Basal Ganglia models and deep brain stimulation. J. Neurosci. 2013, 33, 4804–4814. [Google Scholar] [CrossRef] [Green Version]
- Mallet, L.; Schüpbach, M.; N’Diaye, K.; Remy, P.; Bardinet, E.; Czernecki, V.; Welter, M.L.; Pelissolo, A.; Ruberg, M.; Agid, Y.; et al. Stimulation of subterritories of the subthalamic nucleus reveals its role in the integration of the emotional and motor aspects of behavior. Proc. Natl. Acad. Sci. USA 2007, 104, 10661–10666. [Google Scholar] [CrossRef] [Green Version]
- Steigerwald, F.; Matthies, C.; Volkmann, J. Directional Deep Brain Stimulation. Neurotherapeutics 2019, 16, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Dembek, T.A.; Reker, P.; Visser-Vandewalle, V.; Wirths, J.; Treuer, H.; Klehr, M.; Roediger, J.; Dafsari, H.S.; Barbe, M.T.; Timmermann, L. Directional DBS increases side-effect thresholds-A prospective, double-blind trial. Mov. Disord. 2017, 32, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Barnaure, I.; Pollak, P.; Momjian, S.; Horvath, J.; Lovblad, K.O.; Boex, C.; Remuinan, J.; Burkhard, P.; Vargas, M.I. Evaluation of electrode position in deep brain stimulation by image fusion (MRI and CT). Neuroradiology 2015, 57, 903–908. [Google Scholar] [CrossRef]
- Pinsker, M.O.; Herzog, J.; Falk, D.; Volkmann, J.; Deuschl, G.; Mehdorn, M. Accuracy and distortion of deep brain stimulation electrodes on postoperative MRI and CT. Zentralbl. Neurochir. 2008, 69, 144–147. [Google Scholar] [CrossRef]
- Boutet, A.; Chow, C.T.; Narang, K.; Elias, G.J.B.; Neudorfer, C.; Germann, J.; Ranjan, M.; Loh, A.; Martin, A.J.; Kucharczyk, W.; et al. Improving Safety of MRI in Patients with Deep Brain Stimulation Devices. Radiology 2020, 296, 250–262. [Google Scholar] [CrossRef]
- Zhao, S.; Li, G.; Tong, C.; Chen, W.; Wang, P.; Dai, J.; Fu, X.; Xu, Z.; Liu, X.; Lu, L.; et al. Full activation pattern mapping by simultaneous deep brain stimulation and fMRI with graphene fiber electrodes. Nat. Commun. 2020, 11, 1788. [Google Scholar] [CrossRef] [Green Version]
- Horn, A.; Li, N.; Dembek, T.A.; Kappel, A.; Boulay, C.; Ewert, S.; Tietze, A.; Husch, A.; Perera, T.; Neumann, W.J.; et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. Neuroimage 2019, 184, 293–316. [Google Scholar] [CrossRef]
- Horn, A.; Kühn, A.A. Lead-DBS: A toolbox for deep brain stimulation electrode localizations and visualizations. Neuroimage 2015, 107, 127–135. [Google Scholar] [CrossRef]
- Alkemade, A.; Groot, J.M.; Forstmann, B.U. Do We Need a Human post mortem Whole-Brain Anatomical Ground Truth in in vivo Magnetic Resonance Imaging? Front. Neuroanat. 2018, 12, 110. [Google Scholar] [CrossRef] [Green Version]
- Ewert, S.; Horn, A.; Finkel, F.; Li, N.; Kühn, A.A.; Herrington, T.M. Optimization and comparative evaluation of nonlinear deformation algorithms for atlas-based segmentation of DBS target nuclei. NeuroImage 2019, 184, 586–598. [Google Scholar] [CrossRef] [PubMed]
- Vogel, D.; Shah, A.; Coste, J.; Lemaire, J.-J.; Wårdell, K.; Hemm, S. Anatomical brain structures normalization for deep brain stimulation in movement disorders. NeuroImage Clin. 2020, 27, 102271. [Google Scholar] [CrossRef] [PubMed]
- Lofredi, R.; Auernig, C.G.; Ewert, S.; Irmen, F.; Steiner, L.A.; Scheller, U.; van Wijk, B.C.M.; Oxenford, S.; Kuhn, A.A.; Horn, A. Interrater reliability of deep brain stimulation electrode localizations. Neuroimage 2022, 262, 119552. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Gao, G.; Feng, T.; Zhang, J. Chinese expert consensus on programming deep brain stimulation for patients with Parkinson’s disease. Transl. Neurodegener. 2018, 7, 11. [Google Scholar] [CrossRef]
- Xiao, Y.; Lau, J.C.; Hemachandra, D.; Gilmore, G.; Khan, A.R.; Peters, T.M. Image Guidance in Deep Brain Stimulation Surgery to Treat Parkinson’s Disease: A Comprehensive Review. IEEE Trans. Biomed. Eng. 2021, 68, 1024–1033. [Google Scholar] [CrossRef]
- Fan, S.; Zhang, Q.; Meng, F.; Fang, H.; Yang, G.; Shi, Z.; Liu, H.; Zhang, H.; Yang, A.; Zhang, J.; et al. Comparison of dural puncture and dural incision in deep brain stimulation surgery: A simple but worthwhile technique modification. Front. Neurosci. 2022, 16, 988661. [Google Scholar] [CrossRef]
- Pollo, C.; Villemure, J.G.; Vingerhoets, F.; Ghika, J.; Maeder, P.; Meuli, R. Magnetic resonance artifact induced by the electrode Activa 3389: An in vitro and in vivo study. Acta Neurochir. 2004, 146, 161–164. [Google Scholar] [CrossRef]
- Avants, B.B.; Tustison, N.J.; Song, G.; Cook, P.A.; Klein, A.; Gee, J.C. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage 2011, 54, 2033–2044. [Google Scholar] [CrossRef] [Green Version]
- Ewert, S.; Plettig, P.; Li, N.; Chakravarty, M.M.; Collins, D.L.; Herrington, T.M.; Kuhn, A.A.; Horn, A. Toward defining deep brain stimulation targets in MNI space: A subcortical atlas based on multimodal MRI, histology and structural connectivity. Neuroimage 2018, 170, 271–282. [Google Scholar] [CrossRef]
- Horn, A.; Kühn, A.A.; Merkl, A.; Shih, L.; Alterman, R.; Fox, M. Probabilistic conversion of neurosurgical DBS electrode coordinates into MNI space. NeuroImage 2017, 150, 395–404. [Google Scholar] [CrossRef]
- Deuschl, G.; Schade-Brittinger, C.; Krack, P.; Volkmann, J.; Schäfer, H.; Bötzel, K.; Daniels, C.; Deutschländer, A.; Dillmann, U.; Eisner, W.; et al. A randomized trial of deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2006, 355, 896–908. [Google Scholar] [CrossRef] [Green Version]
- Draz, H.H.; Gabran, S.R.I.; Basha, M.; Mostafa, H.; Abu-Elyazeed, M.F.; Zaki, A. Comparative mechanical analysis of deep brain stimulation electrodes. BioMedical Eng. OnLine 2018, 17, 123. [Google Scholar] [CrossRef] [Green Version]
- Niederer, J.; Patriat, R.; Rosenberg, O.; Palnitkar, T.; Darrow, D.; Park, M.C.; Schrock, L.; Eberly, L.E.; Harel, N. Factors Influencing Electrode Position and Bending of the Proximal Lead in Deep Brain Stimulation for Movement Disorders. Stereotact. Funct. Neurosurg. 2020, 98, 300–312. [Google Scholar] [CrossRef]
- Contarino, M.F.; Bot, M.; Speelman, J.D.; de Bie, R.M.; Tijssen, M.A.; Denys, D.; Bour, L.J.; Schuurman, P.R.; van den Munckhof, P. Postoperative displacement of deep brain stimulation electrodes related to lead-anchoring technique. Neurosurgery 2013, 73, 681–688. [Google Scholar] [CrossRef] [Green Version]
- Goransson, N.; Johansson, J.D.; Wardell, K.; Zsigmond, P. Postoperative Lead Movement after Deep Brain Stimulation Surgery and the Change of Stimulation Volume. Stereotact. Funct. Neurosurg. 2021, 99, 221–229. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, J.W.; Lee, J.Y.; Lim, Y.H.; Kim, C.; Kim, D.G.; Jeon, B.S.; Paek, S.H. Is MRI a reliable tool to locate the electrode after deep brain stimulation surgery? Comparison study of CT and MRI for the localization of electrodes after DBS. Acta Neurochir. 2010, 152, 2029–2036. [Google Scholar] [CrossRef]
- Roth, A.; Buttrick, S.S.; Cajigas, I.; Jagid, J.R.; Ivan, M.E. Accuracy of frame-based and frameless systems for deep brain stimulation: A meta-analysis. J. Clin. Neurosci. 2018, 57, 1–5. [Google Scholar] [CrossRef]
- Yelnik, J.; Damier, P.; Demeret, S.; Gervais, D.; Bardinet, E.; Bejjani, B.P.; François, C.; Houeto, J.L.; Arnule, I.; Dormont, D.; et al. Localization of stimulating electrodes in patients with Parkinson disease by using a three-dimensional atlas-magnetic resonance imaging coregistration method. J. Neurosurg. 2003, 99, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Santiesteban, F.M.; Swanson, S.D.; Noll, D.C.; Anderson, D.J. Magnetic field perturbation of neural recording and stimulating microelectrodes. Phys. Med. Biol. 2007, 52, 2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutet, A.; Rashid, T.; Hancu, I.; Elias, G.J.B.; Gramer, R.M.; Germann, J.; Dimarzio, M.; Li, B.; Paramanandam, V.; Prasad, S.; et al. Functional MRI Safety and Artifacts during Deep Brain Stimulation: Experience in 102 Patients. Radiology 2019, 293, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Golestanirad, L.; Kirsch, J.; Bonmassar, G.; Downs, S.; Elahi, B.; Martin, A.; Iacono, M.I.; Angelone, L.M.; Keil, B.; Wald, L.L.; et al. RF-induced heating in tissue near bilateral DBS implants during MRI at 1.5 T and 3T: The role of surgical lead management. Neuroimage 2019, 184, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Hamid, N.A.; Mitchell, R.D.; Mocroft, P.; Westby, G.W.; Milner, J.; Pall, H. Targeting the subthalamic nucleus for deep brain stimulation: Technical approach and fusion of pre- and postoperative MR images to define accuracy of lead placement. J. Neurol. Neurosurg. Psychiatry 2005, 76, 409–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rooijen, B.D.; Backes, W.H.; Schijns, O.E.; Colon, A.; Hofman, P.A. Brain imaging in chronic epilepsy patients after depth electrode (stereoelectroencephalography) implantation: Magnetic resonance imaging or computed tomography? Neurosurgery 2013, 73, 543–549. [Google Scholar] [CrossRef]
- Yoshida, F.; Miyagi, Y.; Morioka, T.; Hashiguchi, K.; Murakami, N.; Matsumoto, K.; Nagata, S.; Sasaki, T. Assessment of contact location in subthalamic stimulation for Parkinson’s disease by co-registration of computed tomography images. Stereotact. Funct. Neurosurg. 2008, 86, 162–166. [Google Scholar] [CrossRef]
- Wodarg, F.; Herzog, J.; Reese, R.; Falk, D.; Pinsker, M.O.; Steigerwald, F.; Jansen, O.; Deuschl, G.; Mehdorn, H.M.; Volkmann, J. Stimulation site within the MRI-defined STN predicts postoperative motor outcome. Mov. Disord. 2012, 27, 874–879. [Google Scholar] [CrossRef]
- Bot, M.; Schuurman, P.R.; Odekerken, V.J.J.; Verhagen, R.; Contarino, F.M.; De Bie, R.M.A.; van den Munckhof, P. Deep brain stimulation for Parkinson’s disease: Defining the optimal location within the subthalamic nucleus. J. Neurol. Neurosurg. Psychiatry 2018, 89, 493–498. [Google Scholar] [CrossRef]
- Roediger, J.; Dembek, T.A.; Wenzel, G.; Butenko, K.; Kuhn, A.A.; Horn, A. StimFit-A Data-Driven Algorithm for Automated Deep Brain Stimulation Programming. Mov. Disord. 2022, 37, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Roediger, J.; Dembek, T.A.; Achtzehn, J.; Busch, J.L.; Kramer, A.P.; Faust, K.; Schneider, G.H.; Krause, P.; Horn, A.; Kuhn, A.A. Automated deep brain stimulation programming based on electrode location: A randomised, crossover trial using a data-driven algorithm. Lancet Digit. Health 2022, 5, E59–E70. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD Patients | DT Patients | |
|---|---|---|
| Number of patients | 21 | 5 |
| Age (year, mean ± SD) | 58.4 ± 7.4 | 53.6 ± 13.0 |
| Gender (male/female) | 8/13 | 4/1 |
| Age of disease onset (year, mean ± SD) | 51.1 ± 7.4 | 47.4 ± 15.5 |
| Disease duration (year, mean ± SD) | 7.4 ± 3 | 6.2 ± 5.1 |
| LEDD (mg/day) | 1050.3 ± 589.1 | - |
| Preoperative assessment | ||
| UPDRS-III med off (mean ± SD) | 44.7 ± 18.9 | - |
| UPDRS-III med on (mean ± SD) | 20.5 ± 11.3 | - |
| UPDRS-III improvement (%) | 55.4 ± 16.7 | - |
| BFMDRS (mean ± SD) | - | 22.7 ± 15.1 |
| GRS (mean ± SD) | - | 23 ± 6.7 |
| Lead-DBS | Surgiplan | Mean Discrepancy | p Value | ||
|---|---|---|---|---|---|
| X coordinate | All | 12.36 ± 0.98 | 12.23 ± 1.11 | −0.13 | 0.0251 |
| Right | 12.62 ± 0.91 | 12.64 ± 1.12 | 0.02 | 0.8019 | |
| Left | −12.11 ± 1.00 | −11.82 ± 0.95 | −0.29 | 0.0002 | |
| Y coordinate | All | 11.19 ± 1.00 | 10.03 ± 1.29 | −1.16 | <0.0001 |
| Right | 11.38 ± 1.03 | 9.86 ± 1.35 | −1.52 | <0.0001 | |
| Left | −11.00 ± 0.94 | −10.19 ± 1.24 | −0.81 | <0.0001 | |
| Z coordinate | All | 2.05 ± 1.09 | 2.64 ± 1.08 | 0.59 | <0.0001 |
| Right | 2.18 ± 1.12 | 2.65 ± 1.106 | 0.47 | <0.0001 | |
| Left | −1.93 ± 1.05 | −2.64 ± 1.06 | 0.71 | 0.0012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Qin, G.; Tan, B.; Fan, S.; An, Q.; Gao, Y.; Fan, H.; Xie, H.; Wu, D.; Liu, H.; et al. Deep Brain Stimulation Electrode Reconstruction: Comparison between Lead-DBS and Surgical Planning System. J. Clin. Med. 2023, 12, 1781. https://doi.org/10.3390/jcm12051781
Xu Y, Qin G, Tan B, Fan S, An Q, Gao Y, Fan H, Xie H, Wu D, Liu H, et al. Deep Brain Stimulation Electrode Reconstruction: Comparison between Lead-DBS and Surgical Planning System. Journal of Clinical Medicine. 2023; 12(5):1781. https://doi.org/10.3390/jcm12051781
Chicago/Turabian StyleXu, Yichen, Guofan Qin, Bojing Tan, Shiying Fan, Qi An, Yuan Gao, Houyou Fan, Hutao Xie, Delong Wu, Huanguang Liu, and et al. 2023. "Deep Brain Stimulation Electrode Reconstruction: Comparison between Lead-DBS and Surgical Planning System" Journal of Clinical Medicine 12, no. 5: 1781. https://doi.org/10.3390/jcm12051781