
The Effect of Sex on Disease Stage and Survival after Radical Cystectomy in Non-Urothelial Variant-Histology Bladder Cancer
 , , , ,
, , , ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Descriptive Characteristics of Study Population
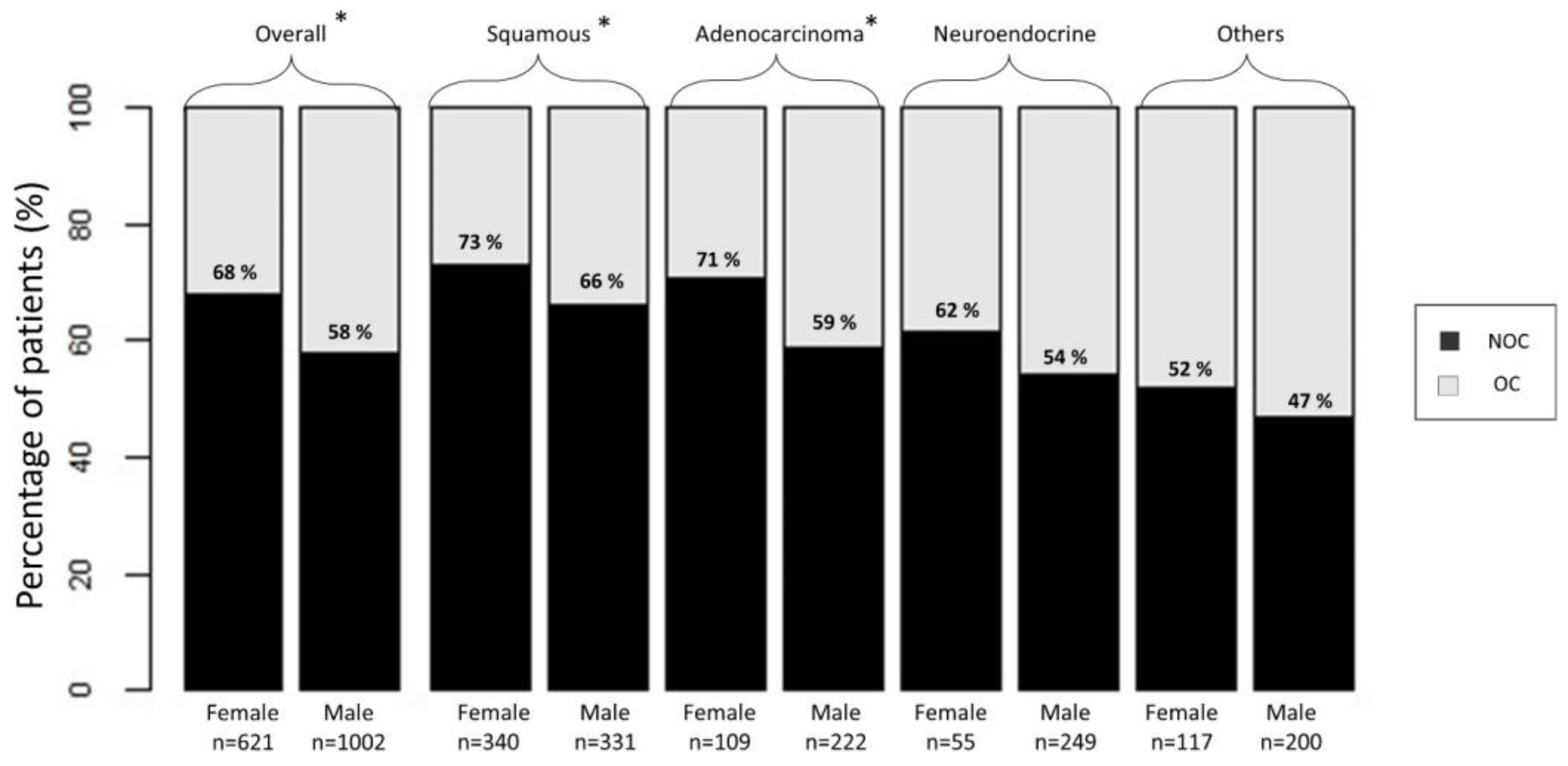
3.2. The Association of Sex with Non-Organ-Confined (NOC) VH BCa
3.3. Effect of Female Sex in Cancer-Specific Mortality (CSM)
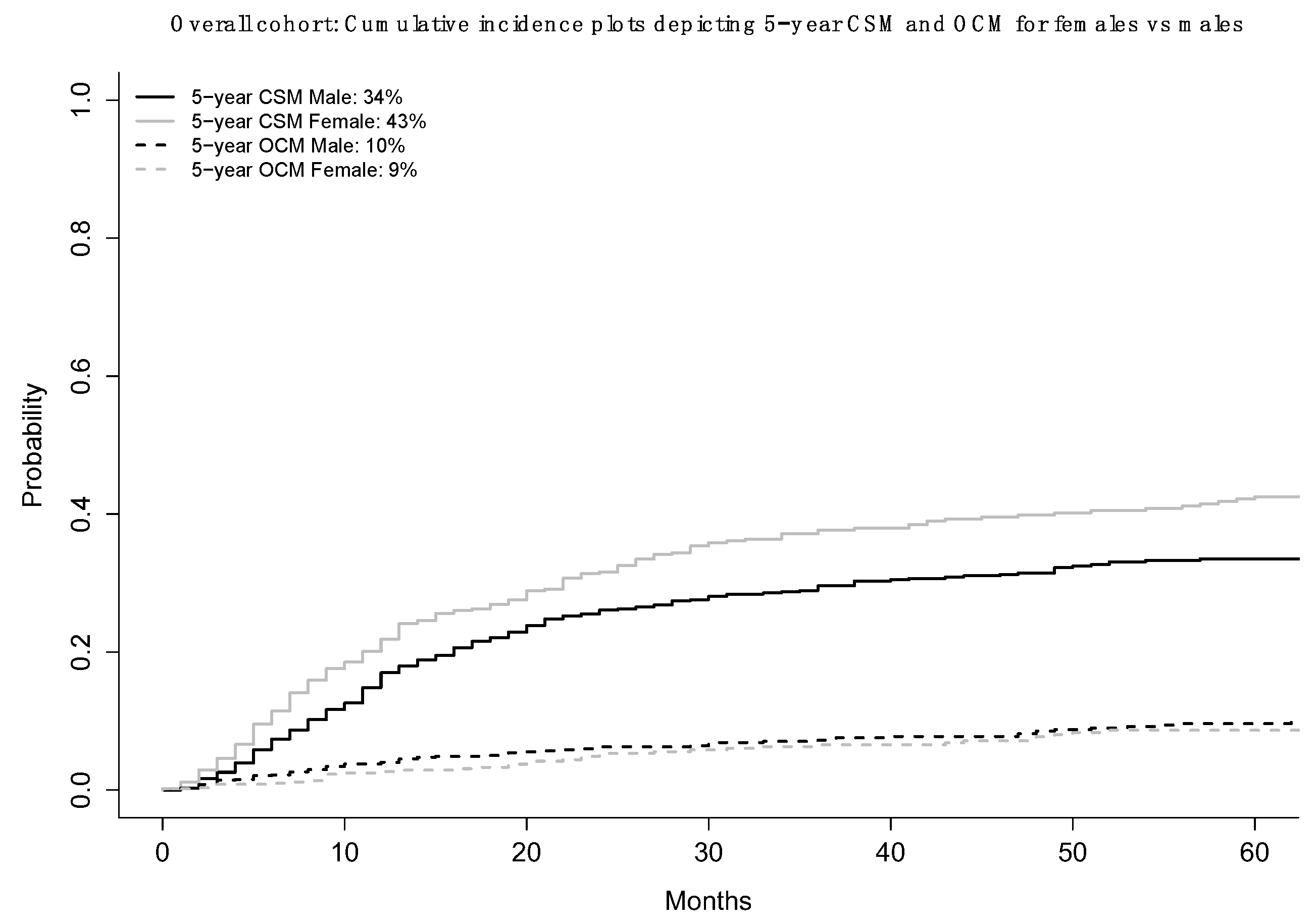
3.3.1. CSM in the Overall Cohort
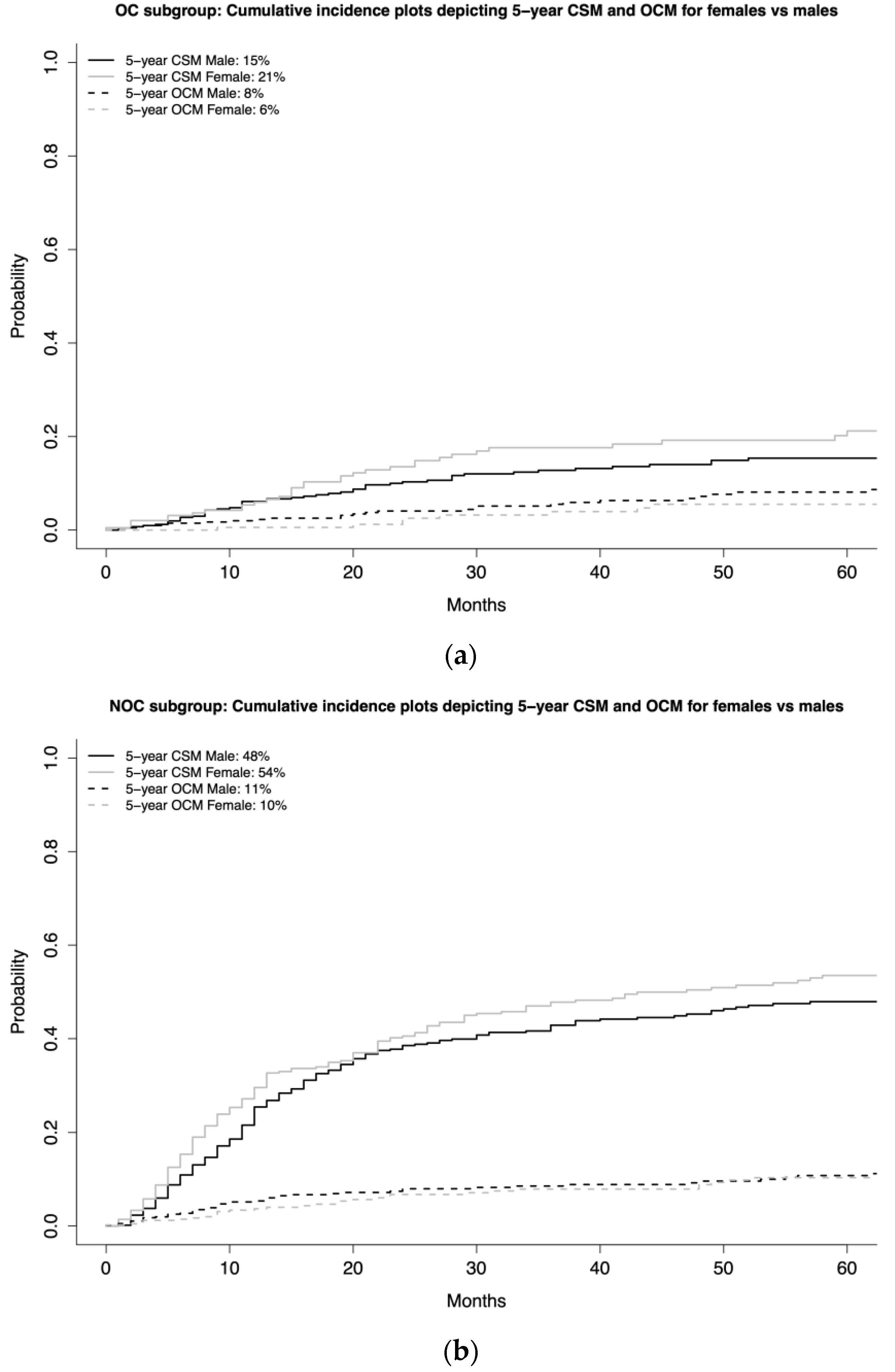
3.3.2. CSM according to Stage-Specific Subgroups (OC vs. NOC)
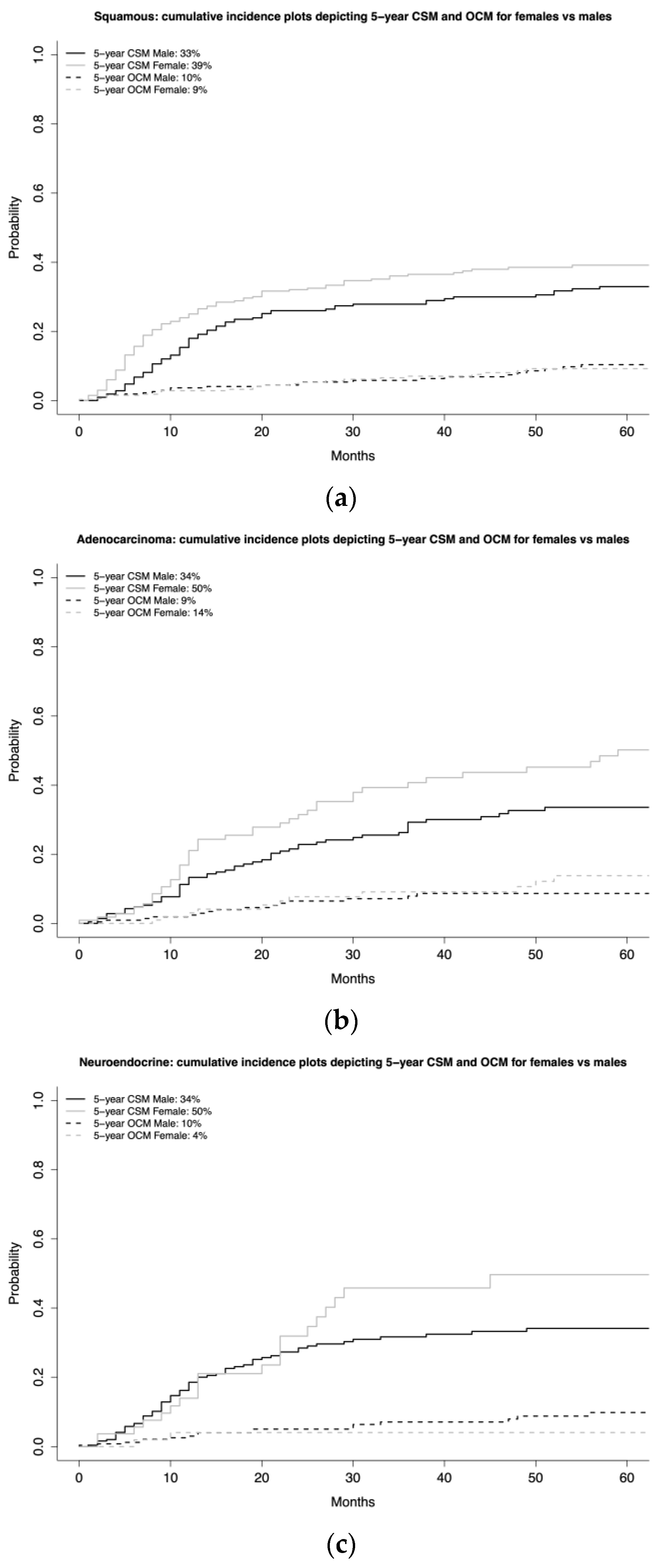
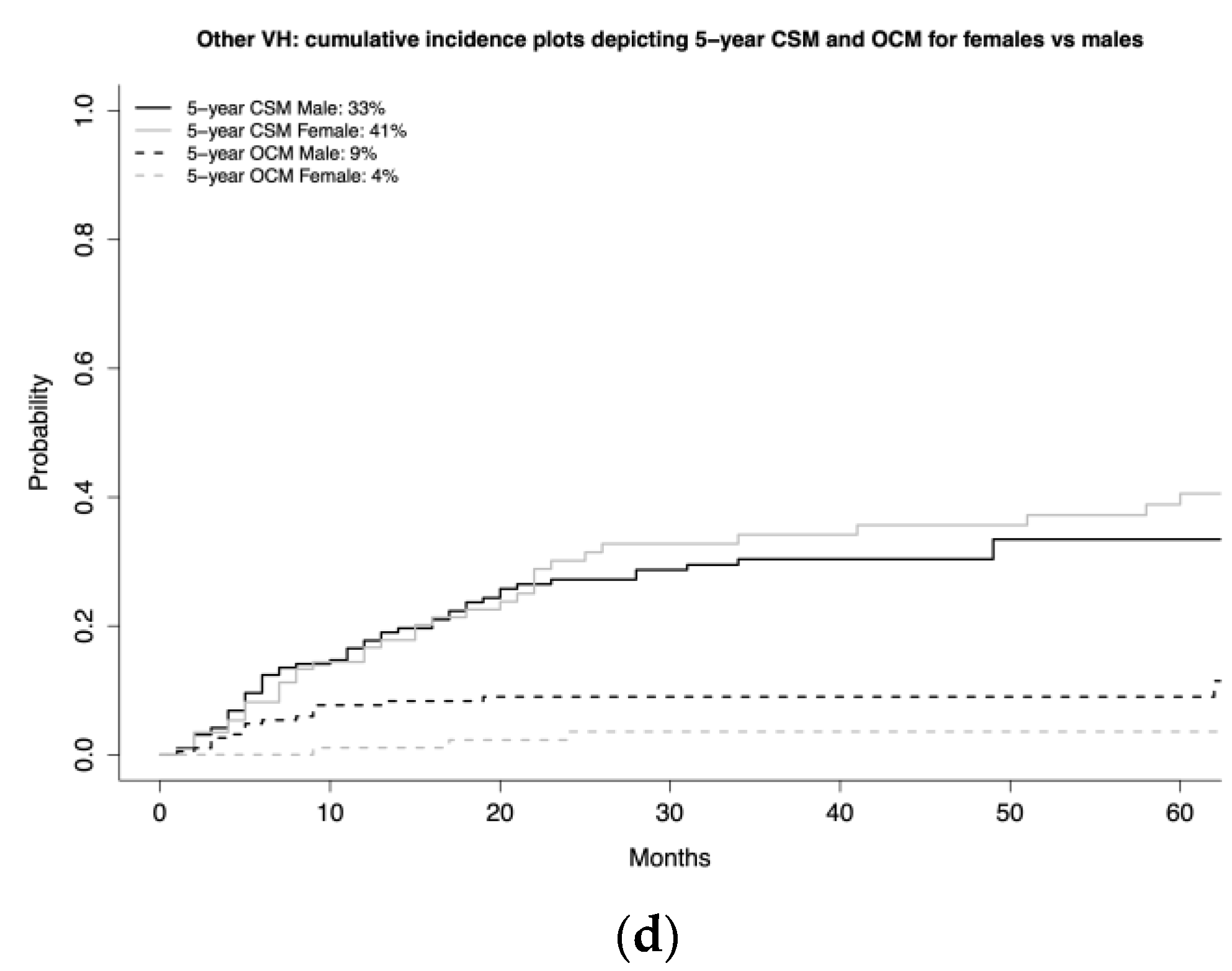
3.3.3. CSM according to VH-Specific Subgroups (SCC, ADK, NE, other VH)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scosyrev, E.; Noyes, K.; Feng, C.; Messing, E. Sex and racial differences in bladder cancer presentation and mortality in the US. Cancer 2009, 115, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Radkiewicz, C.; Edgren, G.; Johansson, A.L.V.; Jahnson, S.; Häggström, C.; Akre, O.; Lambe, M.; Dickman, P.W. Sex Differences in Urothelial Bladder Cancer Survival. Clin. Genitourin. Cancer 2020, 18, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, M.; Ito, Y.; Hatano, K.; Nakai, Y.; Kakimoto, K.; Miyashiro, I.; Nishimura, K. Impact of sex difference on survival of bladder cancer: A population-based registry data in Japan. Int. J. Urol. 2019, 26, 649–654. [Google Scholar] [CrossRef]
- Kluth, L.A.; Rieken, M.; Xylinas, E.; Kent, M.; Rink, M.; Rouprêt, M.; Sharifi, N.; Jamzadeh, A.; Kassouf, W.; Kaushik, D.; et al. Gender-specific differences in clinicopathologic outcomes following radical cystectomy: An international multi-institutional study of more than 8000 patients. Eur Urol. 2014, 66, 913. [Google Scholar] [CrossRef]
- Otto, W.; May, M.; Fritsche, H.-M.; Dragun, D.; Aziz, A.; Gierth, M.; Trojan, L.; Herrmann, E.; Moritz, R.; Ellinger, J.; et al. Analysis of sex differences in cancer-specific survival and perioperative mortality following radical cystectomy: Results of a large german multicenter study of nearly 2500 patients with urothelial carcinoma of the bladder. Gend. Med. 2012, 9, 481–489. [Google Scholar] [CrossRef]
- Tufano, A.; Cordua, N.; Nardone, V.; Ranavolo, R.; Flammia, R.S.; D’Antonio, F.; Borea, F.; Anceschi, U.; Leonardo, C.; Morrione, A.; et al. Prognostic Significance of Organ-Specific Metastases in Patients with Metastatic Upper Tract Urothelial Carcinoma. J. Clin. Med. 2022, 11, 5310. [Google Scholar] [CrossRef]
- Messer, J.C.; Shariat, S.F.; Dinney, C.P.; Novara, G.; Fradet, Y.; Kassouf, W.; Karakiewicz, P.I.; Fritsche, H.-M.; Izawa, J.I.; Lotan, Y.; et al. Female gender is associated with a worse survival after radical cystectomy for urothelial carcinoma of the bladder: A competing risk analysis. Urology 2014, 83, 863–868. [Google Scholar] [CrossRef]
- Rosiello, G.; Palumbo, C.; Pecoraro, A.; Luzzago, S.; Deuker, M.; Stolzenbach, L.F.; Tian, Z.; Gallina, A.; Gandaglia, G.; Montorsi, F.; et al. The effect of sex on disease stage and survival after radical cystectomy: A population-based analysis. Urol. Oncol. Semin. Orig. Investig. 2021, 39, e1–e236. [Google Scholar] [CrossRef]
- Uhlig, A.; Hosseini, A.S.A.; Simon, J.; Lotz, J.; Trojan, L.; Schmid, M.; Uhlig, J. Gender Specific Differences in Disease-Free, Cancer Specific and Overall Survival after Radical Cystectomy for Bladder Cancer: A Systematic Review and Meta-Analysis. J. Urol. 2018, 200, 48–60. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flammia, R.S.; Chierigo, F.; Würnschimmel, C.; Wenzel, M.; Horlemann, B.; Tian, Z.; Borghesi, M.; Leonardo, C.; Tilki, D.; Shariat, S.F.; et al. Sex-related differences in non-urothelial variant histology, non-muscle invasive bladder cancer. Cent. Eur. J. Urol. 2022, 75, 240–247. [Google Scholar] [CrossRef]
- Deuker, M.; Martin, T.; Stolzenbach, F.; Rosiello, G.; Collà Ruvolo, C.; Karakiewicz, P.I. Bladder Cancer: A Comparison Between Non-urothelial Variant Histology and Urothelial Carcinoma Across All Stages and Treatment Modalities. Clin. Genitourin. Cancer 2021, 19, 60–68.e1. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr Cancer Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef] [Green Version]
- Pottegård, A.; Kristensen, K.B.; Friis, S.; Hallas, J.; Jensen, J.B.; Nørgaard, M. Urinary tract infections and risk of squamous cell carcinoma bladder cancer: A Danish nationwide case-control study. Int. J. Cancer 2020, 146, 1930–1936. [Google Scholar] [CrossRef]
- Noon, A.; Albertsen, P.C.; Thomas, F.; Rosario, D.J.; Catto, J.W.F. Competing mortality in patients diagnosed with bladder cancer: Evidence of undertreatment in the elderly and female patients. Br. J. Cancer 2013, 108, 1534–1540. [Google Scholar] [CrossRef] [Green Version]
- Månsson, Å.; Anderson, H.; Colleen, S. Time lag to diagnosis of bladder cancer-influence of psychosocial parameters and level of health-care provision. Scand. J. Urol. Nephrol. 1993, 27, 363–369. [Google Scholar] [CrossRef]
- Ark, J.T.; Alvarez, J.R.; Koyama, T.; Bassett, J.C.; Blot, W.J.; Mumma, M.T.; Resnick, M.J.; You, C.; Penson, D.; Barocas, D.A. Variation in the Diagnostic Evaluation among Persons with Hematuria: Influence of Gender, Race and Risk Factors for Bladder Cancer. J. Urol. 2017, 198, 1033–1038. [Google Scholar] [CrossRef]
- Cohn, J.A.; Vekhter, B.; Lyttle, C.; Steinberg, G.D.; Large, M.C. Sex disparities in diagnosis of bladder cancer after initial resentation with hematuria: A nationwide claims-based investigation. Cancer 2014, 120, 555–561. [Google Scholar] [CrossRef] [Green Version]
- Santos, F.; Dragomir, A.; Kassouf, W.; Franco, E.; Aprikian, A. Urologist referral delay and its impact on survival after radical cystectomy for bladder cancer. Curr. Oncol. 2015, 22, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Barocas, D.A.; Boorjian, S.A.; Alvarez, R.D.; Downs, T.M.; Gross, C.P.; Hamilton, B.D.; Kobashi, K.C.; Lipman, R.R.; Lotan, Y.; Ng, C.K.; et al. Microhematuria: AUA/SUFU Guideline. J. Urol. 2020, 204, 778–786. [Google Scholar] [CrossRef]
- Woldu, S.L.; Ng, C.K.; Loo, R.K.; Slezak, J.M.; Jacobsen, S.J.; Tan, W.S.; Kelly, J.D.; Lough, T.; Darling, D.; van Kessel, K.E.M.; et al. Evaluation of the New American Urological Association Guidelines Risk Classification for Hematuria. J. Urol. 2021, 205, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Mir, C.; Shariat, S.F.; Van der Kwast, T.; Ashfaq, R.; Lotan, Y.; Evans, A.; Skeldon, S.; Hanna, S.; Vajpeyi, R.; Kuk, C.; et al. Loss of androgen receptor expression is not associated with pathological stage, grade, gender or outcome in bladder cancer: A large multi-institutional study. BJU Int. 2011, 108, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, F.; Busetto, G.M.; Gross, M.S.; Maggi, M.; Sciarra, A.; Salciccia, S.; Ferro, M.; Sperduti, I.; Flammia, S.; Canale, V.; et al. Efficacy of three BCG strains (Connaught, TICE and RIVM) with or without secondary resection (re-TUR) for intermediate/high-risk non-muscle-invasive bladder cancers: Results from a retrospective single-institution cohort analysis. J. Cancer Res. Clin. Oncol. 2021, 147, 3073–3080. [Google Scholar] [CrossRef]
- Sorce, G.; Chierigo, F.; Flammia, R.S.; Hoeh, B.; Hohenhorst, L.; Tian, Z.; Goyal, J.A.; Graefen, M.; Terrone, C.; Gallucci, M.; et al. Survival trends in chemotherapy exposed metastatic bladder cancer patients and chemotherapy effect across different age, sex, and race/ethnicity. Urol. Oncol. 2022, 40, e19–e380. [Google Scholar] [CrossRef] [PubMed]
- Flammia, R.S.; Chierigo, F.; Würnschimmel, C.; Horlemann, B.; Gallucci, M.; Karakiewicz, P.I. Survival benefit of chemotherapy in a contemporary cohort of metastatic urachal carcinoma. Urol. Oncol. 2022, 40, 165.e9–165.e15. [Google Scholar] [CrossRef]
- Sorce, G.; Flammia, R.S.; Hoeh, B.; Chierigo, F.; Briganti, A.; Karakiewicz, P.I. Plasmacytoid variant urothelial carcinoma of the bladder: Effect of radical cystectomy and chemotherapy in non-metastatic and metastatic patients. World J. Urol. 2022, 40, 1481–1488. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n | Overall n = 1623 | Females n = 621 (38%) | Males n = 1002 (62%) | p-Value 2 |
|---|---|---|---|---|---|
| Age | 1623 | 67 (58–75) 1 | 67 (57–75) 1 | 68 (59–75) 1 | 0.084 |
| Histological Variants 3 | 1623 | <0.001 | |||
| Squamous | 671 (41%) | 340 (51%) | 331 (49%) | ||
| Adenocarcinoma | 331 (20%) | 109 (33%) | 222 (67%) | ||
| Neuroendocrine | 304 (19%) | 55 (18%) | 249 (82%) | ||
| Other | 317 (20%) | 117 (37%) | 200 (63%) | ||
| T-stage | 1623 | 0.001 | |||
| Ta/Tis | 51 (3.1%) | 17 (2.7%) | 34 (3.4%) | ||
| T1 | 133 (8.2%) | 44 (7.1%) | 89 (8.9%) | ||
| T2 | 492 (30.3%) | 159 (25.6%) | 333 (33.2%) | ||
| T3-T4 | 947 (59%) | 401 (64%) | 546(54%) | ||
| N-stage | 1623 | 0.3 | |||
| N+ | 407 (25%) | 165 (27%) | 242 (24%) | ||
| Stage | 1623 | <0.001 | |||
| Non-organ-confined | 100 (62%) | 421 (68%) | 579 (58%) | ||
| Perioperative Chemotherapy | 1623 | <0.001 | |||
| Yes | 554 (34.1%) | 176 (28.3%) | 378 (37.7%) |
| Multivariable Logistic Regression (Non-Organ- Confined, NOC) | Multivariable Competing Risks Regression (Cancer-Specific Mortality, CSM) | |||||
|---|---|---|---|---|---|---|
| OR (95%CI) | p-Value | HR (95%CI) | p-Value | |||
| Overall cohort | (n = 1623) Females | 1.55 (1.26–1.92) | 0.0001 | (n = 1623) Females | 1.25 (1.04–1.50) | 0.02 |
| Stage-specific subgroup analyses | OC (n = 623) Females | 1.65 (1.08–2.52) | 0.02 | |||
| NOC (n = 1000) Females | 1.17 (0.96–1.43) | 0.1 | ||||
| VH-specific subgroup analyses | SCC (n = 671) Females | 1.40 (1.01–1.95) | 0.047 | SCC (n = 671) Females | 1.33 (1.01–1.75) | 0.045 |
| ADK (n = 331) Females | 1.66 (1.02–2.74) | 0.044 | ADK (n = 331) Females | 1.39 (0.94–2.06) | 0.1 | |
| NE (n = 304) Females | 1.38 (0.76–2.55) | 0.3 | NE (n = 304) Females | 1.24 (0.77–2.00) | 0.4 | |
| Other VH (n = 317) Females | 1.29 (0.81–2.06) | 0.3 | Other VH (n = 317) Females | 1.06 (0.69–1.63) | 0.8 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flammia, R.S.; Tufano, A.; Chierigo, F.; Würnschimmel, C.; Hoeh, B.; Sorce, G.; Tian, Z.; Anceschi, U.; Leonardo, C.; Del Giudice, F.; et al. The Effect of Sex on Disease Stage and Survival after Radical Cystectomy in Non-Urothelial Variant-Histology Bladder Cancer. J. Clin. Med. 2023, 12, 1776. https://doi.org/10.3390/jcm12051776
Flammia RS, Tufano A, Chierigo F, Würnschimmel C, Hoeh B, Sorce G, Tian Z, Anceschi U, Leonardo C, Del Giudice F, et al. The Effect of Sex on Disease Stage and Survival after Radical Cystectomy in Non-Urothelial Variant-Histology Bladder Cancer. Journal of Clinical Medicine. 2023; 12(5):1776. https://doi.org/10.3390/jcm12051776
Chicago/Turabian StyleFlammia, Rocco Simone, Antonio Tufano, Francesco Chierigo, Christoph Würnschimmel, Benedikt Hoeh, Gabriele Sorce, Zhen Tian, Umberto Anceschi, Costantino Leonardo, Francesco Del Giudice, and et al. 2023. "The Effect of Sex on Disease Stage and Survival after Radical Cystectomy in Non-Urothelial Variant-Histology Bladder Cancer" Journal of Clinical Medicine 12, no. 5: 1776. https://doi.org/10.3390/jcm12051776