
Comparing the Clinical Manifestations of Bell’s Palsy between Pre-COVID-19 Pandemic and COVID-19 Pandemic Periods
 , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Statistical Analysis
3. Results
3.1. Results of Electroneurography (ENoG) and Electromyography (EMG) (Table 2)

{kind=link}
{kind=link}
| Parameter | Pre-COVID-19 Period (n = 1719) | COVID-19 Period (n = 120) | p–Value |
|---|---|---|---|
| 1615 (93.9) | 115 (95.8) | 0.398 | |
| ENoG (Poor) | 104 (6.0) | 5 (4.1) | |
| EMG (Good) | 1099 (63.9) | 82 (68.3) | 0.331 |
| EMG (Poor) | 620 (36.0) | 38 (31.6) |
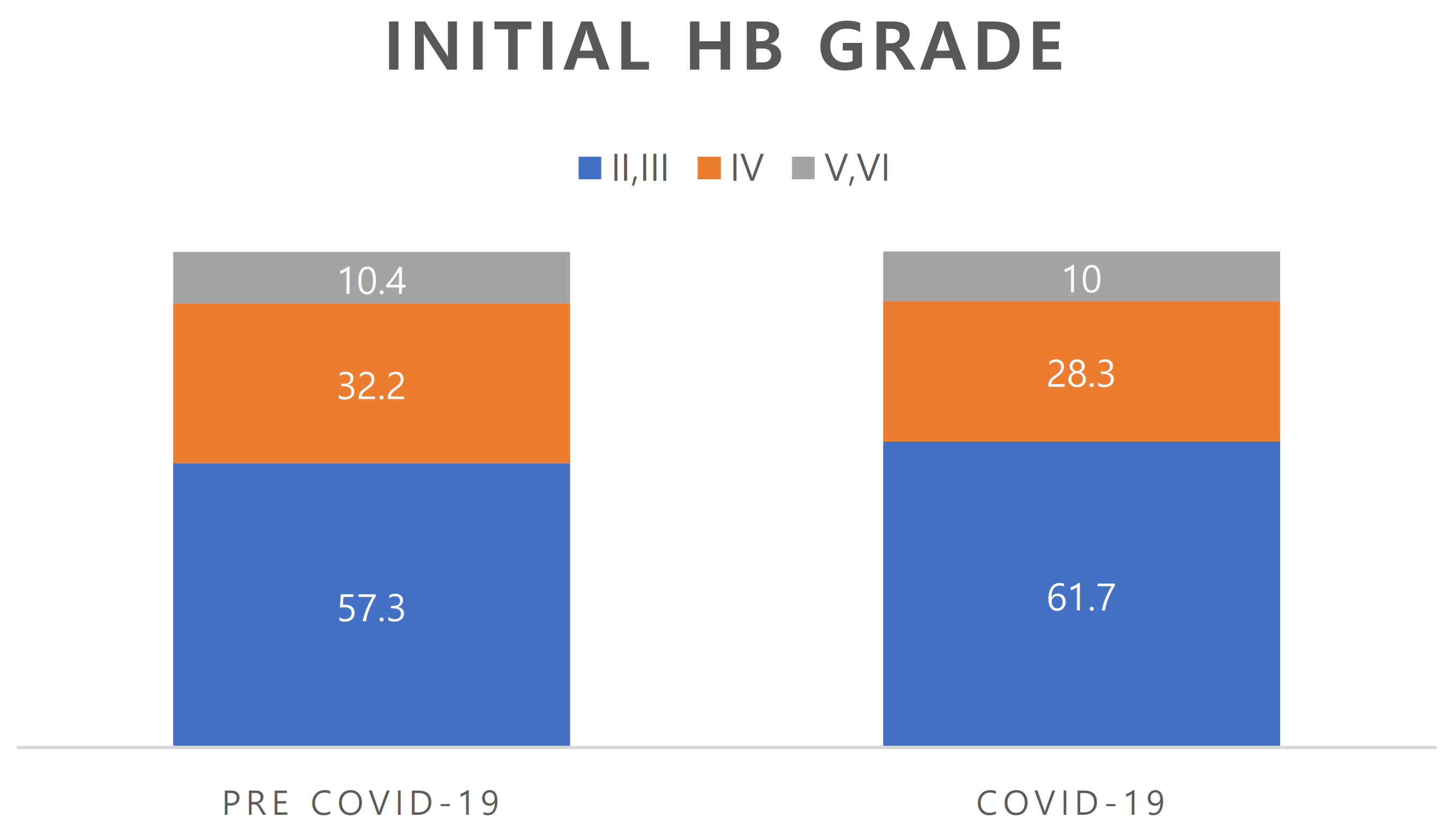
3.2. House-Brackmann Grade at First Visit (Figure 1)

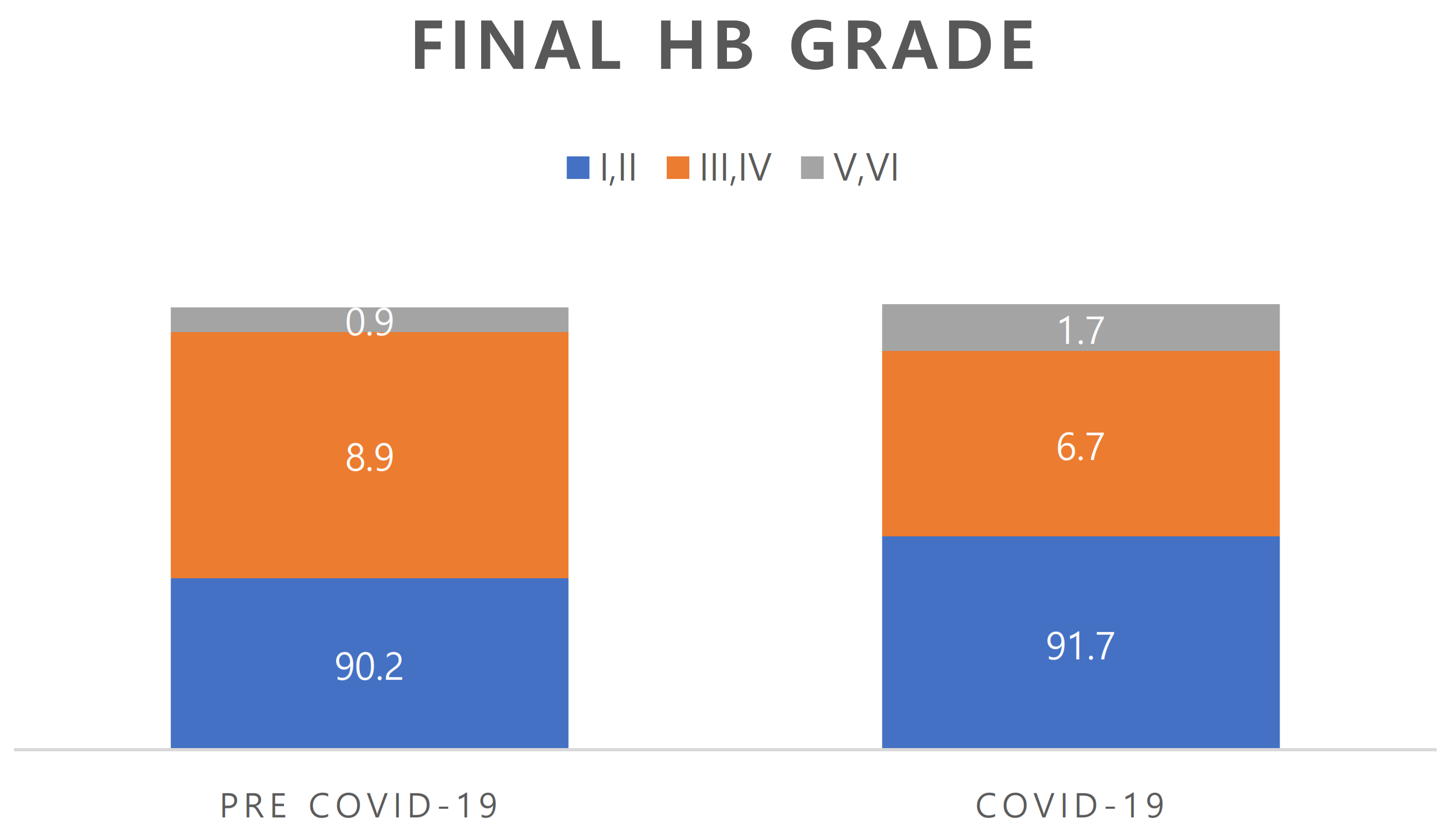
3.3. Recovery Rate (Figure 2)

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattox, D. Clinical Disorders of the Facial Nerve. W: Cummings Otolaryngology. Head Neck Surg. 2021, 5, 2391–2416. [Google Scholar]
- Murakami, S.; Mizobuchi, M.; Nakashiro, Y.; Doi, T.; Hato, N.; Yanagihara, N. Bell palsy and herpes simplex virus: Identification of viral DNA in endoneurial fluid and muscle. Ann. Intern. Med. 1996, 124, 27–30. [Google Scholar] [CrossRef]
- Song, K.; Chang, S.; Lee, J.; Shin, S.A.; Lee, H.Y. Clinical characteristics of dizziness associated with acute peripheral facial palsy. J. Audiol. Otol. 2018, 22, 148–153. [Google Scholar] [CrossRef]
- Zimmermann, J.; Jesse, S.; Kassubek, J.; Pinkhardt, E.; Ludolph, A.C. Differential diagnosis of peripheral facial nerve palsy: A retrospective clinical, MRI and CSF-based study. J. Neurol. 2019, 266, 2488–2494. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. COVID-19. Sejong: Ministry of Health and Welfare; 2022. Available online: http://ncov.mohw.go.kr/ (accessed on 13 November 2022).
- Kim, D.J.; Heo, J.Y.; Kim, H.S. COVID-19 Vaccine and Psychosocial Challenges. J. Korean Diabetes 2021, 22, 185–191. [Google Scholar] [CrossRef]
- Ahn, S.H.; Lee, S.H. Updates on coronavirus disease 19 vaccine and its clinical application. Korean J. Fam. Pract. 2021, 11, 236–246. [Google Scholar] [CrossRef]
- Yoo, M.C.; Soh, Y.; Chon, J.; Lee, J.H.; Jung, J.; Kim, S.S.; You, M.-W.; Byun, J.Y.; Kim, S.H.; Yeo, S.G. Evaluation of factors associated with favorable outcomes in adults with Bell palsy. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 256–263. [Google Scholar] [CrossRef]
- Tsang, H.F.; Chan, L.W.C.; Cho, W.C.S.; Yu, A.C.S.; Yim, A.K.Y.; Chan, A.K.C.; Ng, L.P.W.; Wong, Y.K.E.; Pei, X.M.; Li, M.J.W. An update on COVID-19 pandemic: The epidemiology, pathogenesis, prevention and treatment strategies. Expert Rev. Anti-Infect. Ther. 2021, 19, 877–888. [Google Scholar] [CrossRef]
- Soy, M.; Atagündüz, P.; Atagündüz, I.; Sucak, G.T. Hemophagocytic lymphohistiocytosis: A review inspired by the COVID-19 pandemic. Rheumatol. Int. 2021, 41, 7–18. [Google Scholar] [CrossRef]
- Wong, K.; Shah, M.U.F.A.; Khurshid, M.; Ullah, I.; Tahir, M.J.; Yousaf, Z. COVID-19 associated vasculitis: A systematic review of case reports and case series. Ann. Med. Surg. 2022, 74, 103249. [Google Scholar] [CrossRef]
- Gupta, S.; Jawanda, M.K.; Taneja, N.; Taneja, T. A systematic review of Bell’s Palsy as the only major neurological manifestation in COVID-19 patients. J. Clin. Neurosci. 2021, 90, 284–292. [Google Scholar] [CrossRef]
- Islamoglu, Y.; Celik, B.; Kiris, M. Facial paralysis as the only symptom of COVID-19: A prospective study. Am. J. Otolaryngol. 2021, 42, 102956. [Google Scholar] [CrossRef]
- Codeluppi, L.; Venturelli, F.; Rossi, J.; Fasano, A.; Toschi, G.; Pacillo, F.; Cavallieri, F.; Giorgi Rossi, P.; Valzania, F. Facial palsy during the COVID-19 pandemic. Brain Behav. 2021, 11, e01939. [Google Scholar] [CrossRef]
- Mutlu, A.; Kalcioglu, M.T.; Gunduz, A.Y.; Bakici, B.; Yilmaz, U.; Cag, Y. Does the SARS-CoV-2 pandemic really increase the frequency of peripheral facial palsy? Am. J. Otolaryngol. 2021, 42, 103032. [Google Scholar] [CrossRef]
- Aslan, M.; Çiçek, M.T. Can isolated sudden sensorineural hearing loss (SSNHL) and idiopathic acute facial paralysis (Bell's palsy) be symptoms of COVID-19? Am. J. Otolaryngol. 2021, 42, 103129. [Google Scholar] [CrossRef]
- Khurshid, A.; Khurshid, M.; Sohail, A.; Raza, I.M.; Ahsan, M.K.; Alam Shah, M.U.F.; Taseer, A.R.; Nashwan, A.J.; Ullah, I. Facial palsy as a manifestation of COVID-19: A systematic review of cases. Health Sci. Rep. 2022, 5, e887. [Google Scholar] [CrossRef]
- Finsterer, J.; Scorza, F.A.; Scorza, C.A.; Fiorini, A.C. COVID-19 associated cranial nerve neuropathy: A systematic review. Bosn. J. Basic Med. Sci. 2022, 22, 39. [Google Scholar] [CrossRef]
- Gupta, S.; Jawanda, M.K. Surge of Bell's Palsy in the era of COVID-19: Systematic review. Eur. J. Neurol. 2022, 29, 2526–2543. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef]
- Baig, A.M. Covert pathways to the cranial cavity: Could these be potential routes of SARS-CoV-2 to the brain? ACS Chem. Neurosci. 2020, 11, 3185–3187. [Google Scholar] [CrossRef]
- Lindan, C.E.; Mankad, K.; Ram, D.; Kociolek, L.K.; Silvera, V.M.; Boddaert, N.; Stivaros, S.M.; Palasis, S.; Akhtar, S.; Alden, D. Neuroimaging manifestations in children with SARS-CoV-2 infection: A multinational, multicentre collaborative study. Lancet Child Adolesc. Health 2021, 5, 167–177. [Google Scholar] [CrossRef]
- Kushlaf, H.A. Emerging toxic neuropathies and myopathies. Neurol. Clin. 2011, 29, 679–687. [Google Scholar] [CrossRef]
- Pilania, R.K.; Arora, A.; Agarwal, A.; Jindal, A.K.; Aggarwal, K.; Krishnan, G.; Suri, D.; Gupta, A.; Singh, S.; Gupta, V. Linezolid-induced mitochondrial toxicity presenting as retinal nerve fiber layer microcysts and optic and peripheral neuropathy in a patient with chronic granulomatous disease. Retin. Cases Brief Rep. 2021, 15, 224–229. [Google Scholar] [CrossRef]
- Khanlou, H.; Valdes-Sueiras, M.; Farthing, C. Peripheral neuropathy induced by lopinavir-saquinavir-ritonavir combination therapy in an HIV-infected patient. J. Int. Assoc. Physicians AIDS Care 2007, 6, 155. [Google Scholar] [CrossRef]
- Lorber, M. A case of possible darunavir/ritonavir-induced peripheral neuropathy: Case description and review of the literature. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2013, 12, 162–165. [Google Scholar] [CrossRef]
- Becerra Cuñat, J.; Coll Cantí, J.; Gelpí Mantius, E.; Ferrer Avellí, X.; Lozano Sánchez, M.; Millán Torné, M.; Ojanguren, I.; Ariza, A.; Olivé, A. Miopatía y neuropatía inducida por cloroquina: Tetraparesia progresiva con arreflexia que simula una polirradiculoneuropatía. A propósito de dos casos. Rev. Neurol. (Ed. Impr.) 2003, 36, 523–526. [Google Scholar] [CrossRef]
- Fodale, V.; Praticò, C.; Girlanda, P.; Baradello, A.; Lucanto, T.; Rodolico, C.; Nicolosi, C.; Rovere, V.; Santamaria, L.; Dattola, R. Acute motor axonal polyneuropathy after a cisatracurium infusion and concomitant corticosteroid therapy. Br. J. Anaesth. 2004, 92, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.J. Neurotoxicity of antibacterial therapy. South. Med. J. 1994, 87, 869–874. [Google Scholar] [CrossRef]
- Sugiura, F.; Kojima, T.; Oguchi, T.; Urata, S.; Yuzawa, Y.; Sakakibara, A.; Hayashi, H.; Nishimoto, N.; Ishiguro, N. A case of peripheral neuropathy and skin ulcer in a patient with rheumatoid arthritis after a single infusion of tocilizumab. Mod. Rheumatol. 2009, 19, 199–203. [Google Scholar] [CrossRef]
- Zorowitz, R.D. ICU–acquired weakness: A rehabilitation perspective of diagnosis, treatment, and functional management. Chest 2016, 150, 966–971. [Google Scholar] [CrossRef] [Green Version]
- Paliwal, V.K.; Garg, R.K.; Gupta, A.; Tejan, N. Neuromuscular presentations in patients with COVID-19. Neurol. Sci. 2020, 41, 3039–3056. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef]
- Cardona, G.C.; Pájaro, L.D.Q.; Marzola, I.D.Q.; Villegas, Y.R.; Salazar, L.R.M. Neurotropism of SARS-CoV 2: Mechanisms and manifestations. J. Neurol. Sci. 2020, 412, 116824. [Google Scholar] [CrossRef]
- Dubé, M.; Le Coupanec, A.; Wong, A.H.; Rini, J.M.; Desforges, M.; Talbot, P.J. Axonal transport enables neuron-to-neuron propagation of human coronavirus OC43. J. Virol. 2018, 92, e00404–e00418. [Google Scholar] [CrossRef] [Green Version]
| Parameter | Pre-COVID-19 Period (n = 1719) | COVID-19 Period (n = 120) | p-Value |
|---|---|---|---|
| Age, yr | 47.60 ± 16.70 | 51.45 ± 16.26 | 0.062 |
| Sex, n (%) | |||
| Male | 797 (46.3) | 50 (41.7) | 0.103 |
| Female | 922 (53.6) | 70 (58.3) | |
| Underlying disease | |||
| Hypertension, n (%) | 352 (20.4) | 22 (18.3) | 0.632 |
| Diabetes mellitus, n (%) | 216 (12.5) | 16 (13.3) | 0.807 |
| Accompanying symptoms, n (%) | |||
| Otalgia | 177 (10.3) | 16 (13.3) | 0.304 |
| Dizziness | 42 (2.4) | 2 (1.6) | 0.59 |
| Tinnitus | 158 (9.1) | 8 (6.6) | 0.351 |
| Hyperacusis | 106 (6.1) | 6 (5.0) | 0.605 |
| Hearing disturbance | 30 (1.7) | 2 (1.6) | 0.949 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, G.W.; Yon, D.K.; Choi, Y.S.; Lee, J.; Park, K.H.; Lee, Y.J.; Park, D.C.; Kim, S.H.; Byun, J.Y.; Yeo, S.G. Comparing the Clinical Manifestations of Bell’s Palsy between Pre-COVID-19 Pandemic and COVID-19 Pandemic Periods. J. Clin. Med. 2023, 12, 1700. https://doi.org/10.3390/jcm12041700
Choi GW, Yon DK, Choi YS, Lee J, Park KH, Lee YJ, Park DC, Kim SH, Byun JY, Yeo SG. Comparing the Clinical Manifestations of Bell’s Palsy between Pre-COVID-19 Pandemic and COVID-19 Pandemic Periods. Journal of Clinical Medicine. 2023; 12(4):1700. https://doi.org/10.3390/jcm12041700
Chicago/Turabian StyleChoi, Gang Won, Dong Keon Yon, Yong Sung Choi, Jinseok Lee, Ki Ho Park, Young Ju Lee, Dong Choon Park, Sang Hoon Kim, Jae Young Byun, and Seung Geun Yeo. 2023. "Comparing the Clinical Manifestations of Bell’s Palsy between Pre-COVID-19 Pandemic and COVID-19 Pandemic Periods" Journal of Clinical Medicine 12, no. 4: 1700. https://doi.org/10.3390/jcm12041700