
Weight-Based Bisphosphonate Administration for Multiple Myeloma Patients and the Risks of Skeletal Complications


Abstract
:1. Introduction
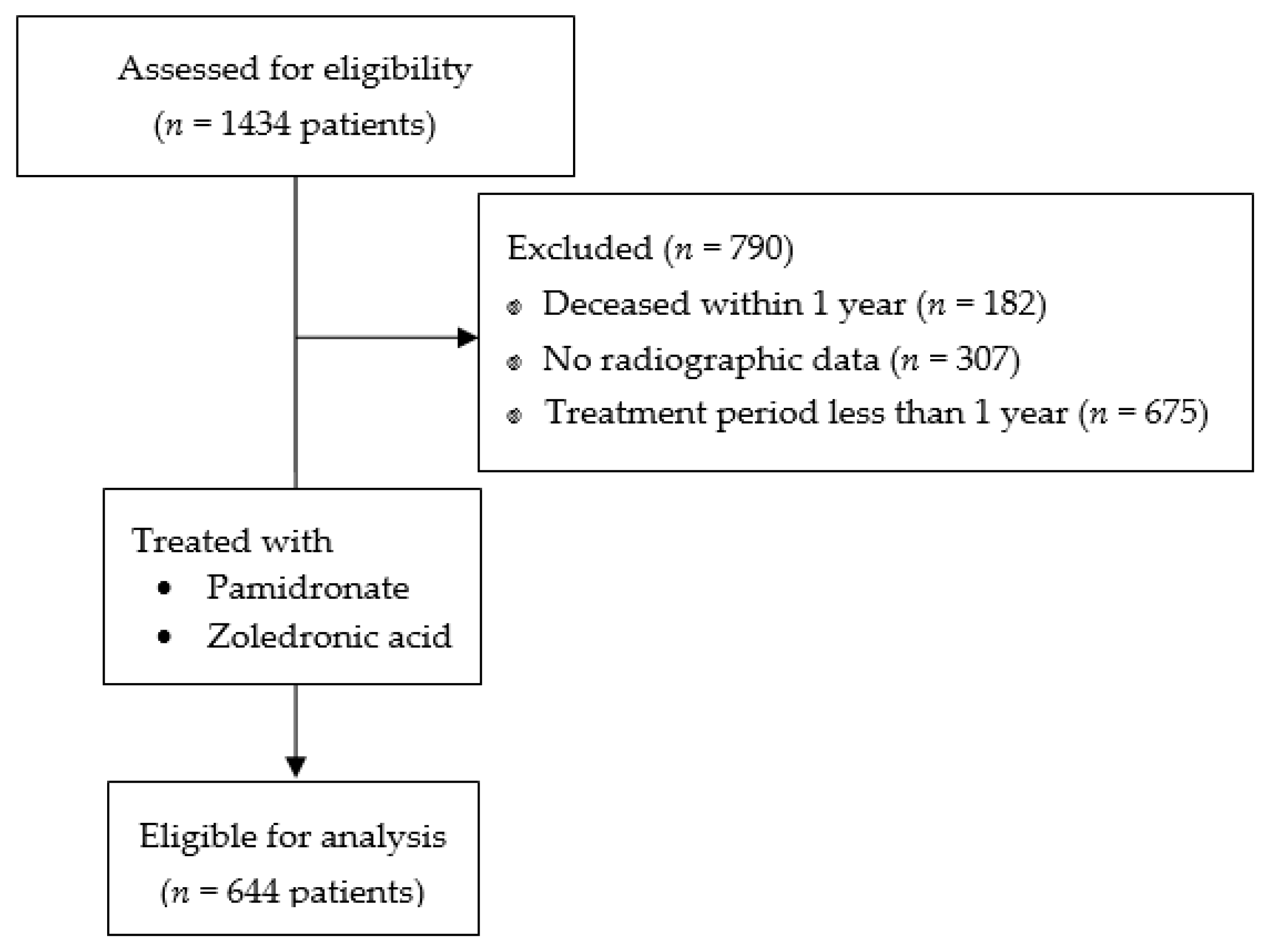
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kyle, R.A.; Gertz, M.A.; Witzig, T.E.; Lust, J.A.; Lacy, M.Q.; Dispenzieri, A.; Fonseca, R.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin. Proc. 2003, 78, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Dispenzieri, A.; Kyle, R.; Merlini, G.; Miguel, J.; Ludwig, H.; Hájek, R.; Palumbo, A.; Jagannath, S.; Bladé, J.; Lonial, S. International Myeloma Working Group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia 2009, 23, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, S.; Roodman, G.D. Multiple myeloma and bone: The fatal interaction. Cold Spring Harb. Perspect. Med. 2018, 8, a031286. [Google Scholar] [CrossRef]
- Giuliani, N.; Rizzoli, V.; Roodman, G.D. Multiple myeloma bone disease: Pathophysiology of osteoblast inhibition. Blood 2006, 108, 3992–3996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowan, A.J.; Green, D.J.; Kwok, M.; Lee, S.; Coffey, D.G.; Holmberg, L.A.; Tuazon, S.; Gopal, A.K.; Libby, E.N. Diagnosis and Management of Multiple Myeloma: A Review. JAMA 2022, 327, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Guenther, A.; Gordon, S.; Tiemann, M.; Burger, R.; Bakker, F.; Green, J.R.; Baum, W.; Roelofs, A.J.; Rogers, M.J.; Gramatzki, M. The bisphosphonate zoledronic acid has antimyeloma activity in vivo by inhibition of protein prenylation. Int. J. Cancer 2010, 126, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Kimachi, K.; Kajiya, H.; Nakayama, S.; Ikebe, T.; Okabe, K. Zoledronic acid inhibits rank expression and migration of osteoclast precursors during osteoclastogenesis. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2011, 383, 297–308. [Google Scholar] [CrossRef]
- Terpos, E.; Zamagni, E.; Lentzsch, S.; Drake, M.T.; García-Sanz, R.; Abildgaard, N.; Ntanasis-Stathopoulos, I.; Schjesvold, F.; de la Rubia, J.; Kyriakou, C. Treatment of multiple myeloma-related bone disease: Recommendations from the Bone Working Group of the International Myeloma Working Group. Lancet Oncol. 2021, 22, e119–e130. [Google Scholar] [CrossRef]
- Anderson, K.; Ismaila, N.; Flynn, P.J.; Halabi, S.; Jagannath, S.; Ogaily, M.S.; Omel, J.; Raje, N.; Roodman, G.D.; Yee, G.C. Role of bone-modifying agents in multiple myeloma: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2018, 36, 812–818. [Google Scholar] [CrossRef]
- Terpos, E.; Kleber, M.; Engelhardt, M.; Zweegman, S.; Gay, F.; Kastritis, E.; van de Donk, N.W.; Bruno, B.; Sezer, O.; Broijl, A. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica 2015, 100, 1254. [Google Scholar] [CrossRef] [Green Version]
- Kyle, R.A.; Yee, G.C.; Somerfield, M.R.; Flynn, P.J.; Halabi, S.; Jagannath, S.; Orlowski, R.Z.; Roodman, D.G.; Twilde, P.; Anderson, K. American Society of Clinical Oncology 2007 clinical practice guideline update on the role of bisphosphonates in multiple myeloma. J. Clin. Oncol. 2007, 25, 2464–2472. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Moreau, P.; Terpos, E.; Mateos, M.-V.; Zweegman, S.; Cook, G.; Delforge, M.; Hájek, R.; Schjesvold, F.; Cavo, M. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.K.; Callander, N.S.; Hillengass, J.; Liedtke, M.; Baljevic, M.; Campagnaro, E.; Castillo, J.J.; Chandler, J.C.; Cornell, R.F.; Costello, C. NCCN guidelines insights: Multiple myeloma, version 1.2020: Featured updates to the NCCN guidelines. J. Natl. Compr. Cancer Netw. 2019, 17, 1154–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M. American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2020 update. Endocr. Pract. 2020, 26, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.G.; Chretien, K.C.; Meoni, L.A.; Liu, Y.-P.; Klag, M.J.; Levine, M.A. Comparison of intravenous pamidronate to standard therapy for osteoporosis: Use in patients unable to take oral bisphosphonates. J. Clin. Rheumatol. 2005, 11, 2–7. [Google Scholar] [CrossRef]
- Reyes, C.; Hitz, M.; Prieto-Alhambra, D.; Abrahamsen, B. Risks and benefits of bisphosphonate therapies. J. Cell. Biochem. 2016, 117, 20–28. [Google Scholar] [CrossRef]
- Schilcher, J.; Michaëlsson, K.; Aspenberg, P. Bisphosphonate use and atypical fractures of the femoral shaft. N. Engl. J. Med. 2011, 364, 1728–1737. [Google Scholar] [CrossRef] [Green Version]
- Black, D.M.; Geiger, E.J.; Eastell, R.; Vittinghoff, E.; Li, B.H.; Ryan, D.S.; Dell, R.M.; Adams, A.L. Atypical femur fracture risk versus fragility fracture prevention with bisphosphonates. N. Engl. J. Med. 2020, 383, 743–753. [Google Scholar] [CrossRef]
- Ruggiero. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw-2014 Update (vol 72, pg 1938, 2014). J. Oral Maxillofac. Surg. 2015, 73, 1879. [Google Scholar]
- Lee, Y.-K.; Ahn, S.; Kim, K.M.; Suh, C.S.; Koo, K.-H. Incidence rate of atypical femoral fracture after bisphosphonates treatment in Korea. J. Korean Med. Sci. 2018, 33, e38. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, Y.-K.; Kim, T.-Y.; Ha, Y.-C.; Jang, S.; Kim, H.Y. Incidence of and risk for osteonecrosis of the jaw in Korean osteoporosis patients treated with bisphosphonates: A nationwide cohort-study. Bone 2021, 143, 115650. [Google Scholar] [CrossRef] [PubMed]
- Shane, E.; Burr, D.; Abrahamsen, B.; Adler, R.A.; Brown, T.D.; Cheung, A.M.; Cosman, F.; Curtis, J.R.; Dell, R.; Dempster, D.W. Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American Society for Bone and Mineral Research. J. Bone Miner. Res. 2014, 29, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws—2009 update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar]
- Zacharis, C.K.; Tzanavaras, P.D. Determination of bisphosphonate active pharmaceutical ingredients in pharmaceuticals and biological material: A review of analytical methods. J. Pharm. Biomed. Anal. 2008, 48, 483–496. [Google Scholar] [CrossRef]
- Green, J.R.; Müller, K.; Jaeggi, K.A. Preclinical pharmacology of CGP 42′ 446, a new, potent, heterocyclic bisphosphonate compound. J. Bone Miner. Res. 1994, 9, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Berenson, J.R.; Hillner, B.E.; Kyle, R.A.; Anderson, K.; Lipton, A.; Yee, G.C.; Biermann, J.S. American Society of Clinical Oncology clinical practice guidelines: The role of bisphosphonates in multiple myeloma. J. Clin. Oncol. 2002, 20, 3719–3736. [Google Scholar] [CrossRef]
- Zeng, C.; Wen, W.; Morgans, A.K.; Pao, W.; Shu, X.-O.; Zheng, W. Disparities by race, age, and sex in the improvement of survival for major cancers: Results from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program in the United States, 1990 to 2010. JAMA Oncol. 2015, 1, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Sneyd, M.J.; Gray, A.R.; Morison, I.M. Trends in survival from myeloma, 1990–2015: A competing risks analysis. BMC Cancer 2021, 21, 821. [Google Scholar] [CrossRef]
- Dickinson, M.; Prince, H.; Kirsa, S.; Zannettino, A.; Gibbs, S.; Mileshkin, L.; O’Grady, J.; Seymour, J.; Szer, J.; Horvath, N. Osteonecrosis of the jaw complicating bisphosphonate treatment for bone disease in multiple myeloma: An overview with recommendations for prevention and treatment. Intern. Med. J. 2009, 39, 304–316. [Google Scholar] [CrossRef]
- Bamias, A.; Kastritis, E.; Bamia, C.; Moulopoulos, L.A.; Melakopoulos, I.; Bozas, G.; Koutsoukou, V.; Gika, D.; Anagnostopoulos, A.; Papadimitriou, C. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J. Clin. Oncol. 2005, 23, 8580–8587. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Kastritis, E.; Anagnostopoulos, A.; Melakopoulos, I.; Gika, D.; Moulopoulos, L.A.; Bamia, C.; Terpos, E.; Tsionos, K.; Bamias, A. Osteonecrosis of the jaw in patients with multiple myeloma treated with bisphosphonates: Evidence of increased risk after treatment with zoledronic acid. Haematologica 2006, 91, 968–971. [Google Scholar] [PubMed]
- Chang, S.T.; Tenforde, A.S.; Grimsrud, C.D.; O’Ryan, F.S.; Gonzalez, J.R.; Baer, D.M.; Chandra, M.; Lo, J.C. Atypical femur fractures among breast cancer and multiple myeloma patients receiving intravenous bisphosphonate therapy. Bone 2012, 51, 524–527. [Google Scholar] [CrossRef]
- Wernecke, G.; Namduri, S.; DiCarlo, E.F.; Schneider, R.; Lane, J. Case report of spontaneous, nonspinal fractures in a multiple myeloma patient on long-term pamidronate and zoledronic acid. HSS J. 2008, 4, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Ota, S.; Inoue, R.; Shiozaki, T.; Yamamoto, Y.; Hashimoto, N.; Takeda, O.; Yoshikawa, K.; Ito, J.; Ishibashi, Y. Atypical femoral fracture after receiving antiresorptive drugs in breast cancer patients with bone metastasis. Breast Cancer 2017, 24, 601–607. [Google Scholar] [CrossRef] [Green Version]
- Raje, N.; Terpos, E.; Willenbacher, W.; Shimizu, K.; García-Sanz, R.; Durie, B.; Legieć, W.; Krejčí, M.; Laribi, K.; Zhu, L. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: An international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018, 19, 370–381. [Google Scholar] [CrossRef]
- Hageman, K.; Patel, K.C.; Mace, K.; Cooper, M.R. The role of denosumab for prevention of skeletal-related complications in multiple myeloma. Ann. Pharmacother. 2013, 47, 1069–1074. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Morgan, G.; Dimopoulos, M.A.; Drake, M.T.; Lentzsch, S.; Raje, N.; Sezer, O.; García-Sanz, R.; Shimizu, K.; Turesson, I. International Myeloma Working Group recommendations for the treatment of multiple myeloma–related bone disease. J. Clin. Oncol. 2013, 31, 2347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, G.J.; Davies, F.E.; Gregory, W.M.; Cocks, K.; Bell, S.E.; Szubert, A.J.; Navarro-Coy, N.; Drayson, M.T.; Owen, R.G.; Feyler, S. First-line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma (MRC Myeloma IX): A randomised controlled trial. Lancet 2010, 376, 1989–1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Body, J.-J. Clinical research update: Zoledronate. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1997, 80, 1699–1701. [Google Scholar] [CrossRef]
- Lipton, A.; Small, E.; Saad, F.; Gleason, D.; Gordon, D.; Smith, M.; Rosen, L.; Ortu Kowalski, M.; Reitsma, D.; Seaman, J. The new bisphosphonate, Zometa®(zoledronic acid), decreases skeletal complications in both osteolytic and osteoblastic lesions: A comparison to pamidronate. Cancer Investig. 2002, 20, 45–54. [Google Scholar] [CrossRef]
- Rosen, L.S.; Gordon, D.; Kaminski, M.; Howell, A.; Belch, A.; Mackey, J.; Apffelstaedt, J.; Hussein, M.; Coleman, R.E.; Reitsma, D.J. Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: A phase III, double-blind, comparative trial. Cancer J. 2001, 7, 377–387. [Google Scholar] [PubMed]
- Piper, P.K., Jr.; Gruntmanis, U. Management of osteoporosis in the aging male: Focus on zoledronic acid. Clin. Interv. Aging 2009, 4, 289. [Google Scholar] [CrossRef] [Green Version]
- Dempster, D.W.; Bolognese, M.A. Ibandronate: The evolution of a once-a-month oral therapy for postmenopausal osteoporosis. J. Clin. Densitom. 2006, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Shaw, N.; Bishop, N. Bisphosphonate treatment of bone disease. Arch. Dis. Child. 2005, 90, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Morgan, G.J.; Child, J.A.; Gregory, W.M.; Szubert, A.J.; Cocks, K.; Bell, S.E.; Navarro-Coy, N.; Drayson, M.T.; Owen, R.G.; Feyler, S. Effects of zoledronic acid versus clodronic acid on skeletal morbidity in patients with newly diagnosed multiple myeloma (MRC Myeloma IX): Secondary outcomes from a randomised controlled trial. Lancet Oncol. 2011, 12, 743–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on medication-related osteonecrosis of the jaw–2022 update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Items | |
|---|---|
| Patients for assessment | 644 |
| Sex | |
| Male | 325 (50.5%) |
| Female | 319 (49.5%) |
| Mean follow-up ± SD (range), months | 69.8 ± 33.1 (12.1–128.3) |
| Mean age ± SD (range), years | 67.2 ± 9.5 (18–89) |
| Mean body weight ± SD (range), kg | 60.8 ± 13.1 (31.2–108) |
| Mean BMI ± SD (range), kg/m2 | 23.7 ± 3.6 (13.5–62.2) |
| Bisphosphonate treatment options | |
| Pamidronate only | 381 (59.2%) |
| Zoledronic acid only | 18 (2.8%) |
| Pamidronate + zoledronic acid | 245 (38.0%) |
| Atypical Femoral Fracture (AFF) | Medication-Related Osteonecrosis of the Jaw (MRONJ) | |||||
|---|---|---|---|---|---|---|
| Item | OR | 95% C.I. | p | OR | 95% C.I. | p |
| Age | 1.024 | 0.937–1.120 | 0.594 | 1.012 | 0.981–1.045 | 0.444 |
| Sex (women: men) | 2.063 | 0.375–11.349 | 0.405 | 0.511 | 0.245–1.064 | 0.073 |
| Body weight (kg) | 0.990 | 0.919–1.066 | 0.792 | 0.982 | 0.922–1.046 | 0.580 |
| BMI (kg/m2) | 0.983 | 0.778–1.241 | 0.885 | 1.014 | 0.865–1.189 | 0.863 |
| Accumulative treatment dose (mg) | ||||||
| Pamidronate | 1.000 | 1.000–1.001 | 0.755 | 1.000 | 0.999–1.001 | 0.786 |
| Zoledronate | 1.017 | 1.004–1.029 | 0.009 † | 1.008 | 0.972–1.044 | 0.675 |
| Accumulative dose(mg)/BMI (kg/m2) | ||||||
| Pamidronate | 1.013 | 0.947–1.083 | 0.716 | 1.002 | 0.998–1.006 | 0.351 |
| Zoledronate | 1.441 | 1.085–1.914 | 0.012 † | 1.262 | 1.110–1.435 | <0.001 † |
| Accumulative dose(mg)/Bwt (kg) | ||||||
| Pamidronate | 1.005 | 0.976–1.034 | 0.762 | 1.004 | 0.994–1.014 | 0.401 |
| Zoledronate | 2.641 | 1.277–5.462 | 0.009 † | 1.816 | 1.313–2.513 | <0.001 † |
| Potency-weighted accumulative dose (mg)/Bwt (kg) | ||||||
| Pamidronate | 1.010 | 0.976–1.034 | 0.762 | 1.004 | 0.994–1.014 | 0.401 |
| Zoledronate | 1.010 | 1.002–1.017 | 0.009 † | 1.006 | 1.003–1.009 | <0.001 † |
| Pamidronate + zoledronate total dose | 1.010 | 1.003–1.017 | 0.005 † | 1.007 | 1.003–1.010 | <0.001 † |
| ⸫ for AFF: pamidronate ∗ 90 mg + zoledronate ∗ 4 mg ∗ 100 ≥ 77 ∗ Bwt (kg) |
| ⸫ for MRONJ: pamidronate ∗ 90 mg + zoledronate ∗ 4 mg ∗ 100 ≥ 57.70 ∗ Bwt (kg) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahk, J.H.; Jo, W.-L.; Kwon, S.-Y.; Park, H.C.; Lim, Y.W. Weight-Based Bisphosphonate Administration for Multiple Myeloma Patients and the Risks of Skeletal Complications. J. Clin. Med. 2023, 12, 1637. https://doi.org/10.3390/jcm12041637
Bahk JH, Jo W-L, Kwon S-Y, Park HC, Lim YW. Weight-Based Bisphosphonate Administration for Multiple Myeloma Patients and the Risks of Skeletal Complications. Journal of Clinical Medicine. 2023; 12(4):1637. https://doi.org/10.3390/jcm12041637
Chicago/Turabian StyleBahk, Ji Hoon, Woo-Lam Jo, Soon-Yong Kwon, Hyung Chul Park, and Young Wook Lim. 2023. "Weight-Based Bisphosphonate Administration for Multiple Myeloma Patients and the Risks of Skeletal Complications" Journal of Clinical Medicine 12, no. 4: 1637. https://doi.org/10.3390/jcm12041637