
Geriatric Assessment Implementation before Chemotherapy in MEtastatic Prostate Cancer, Results from the Real-Life Study GAMERS
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
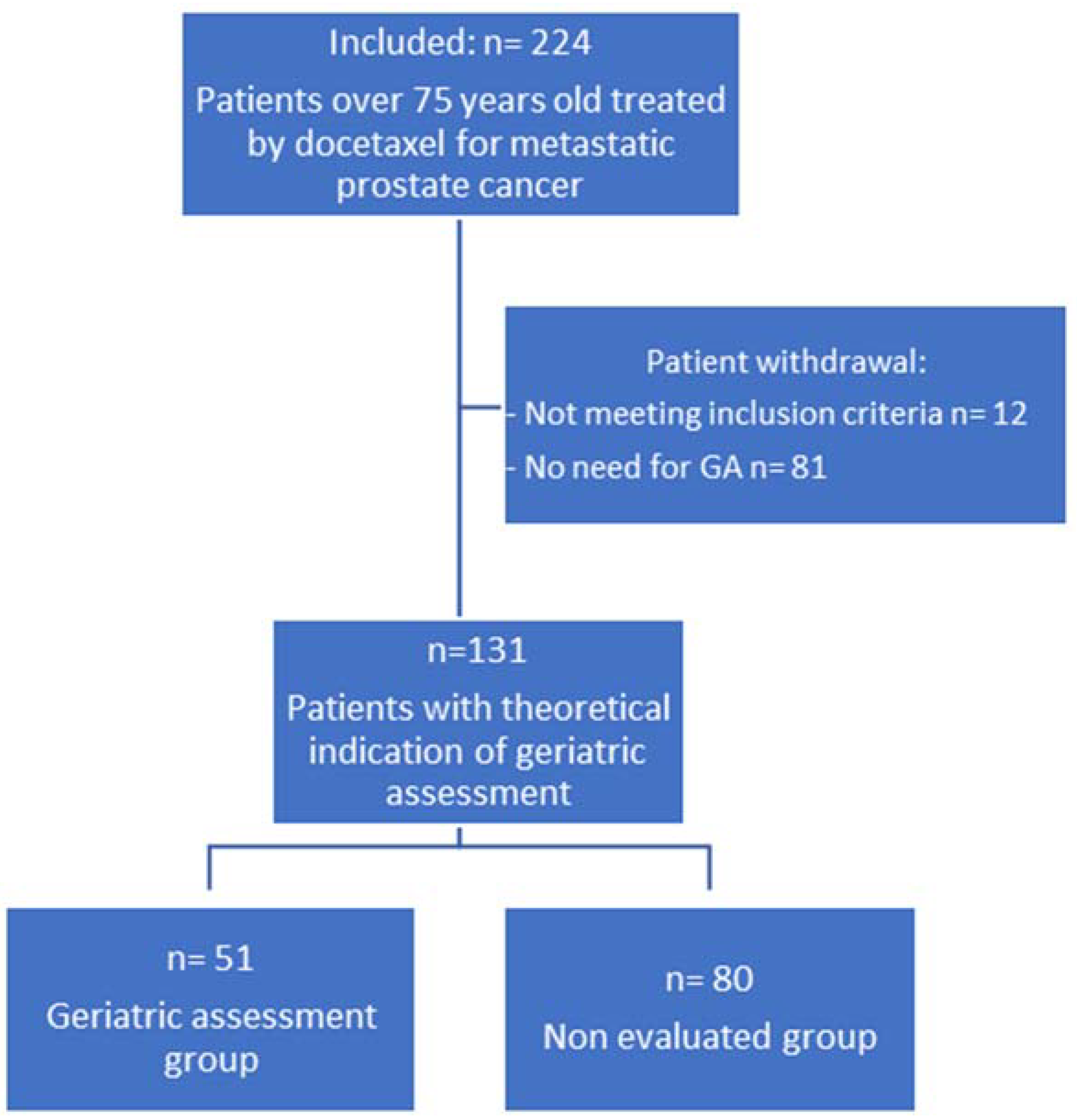
2.1. Patients
2.2. Geriatric Evaluation
2.3. Endpoint
2.4. Statistical Analysis
3. Results
3.1. Patients
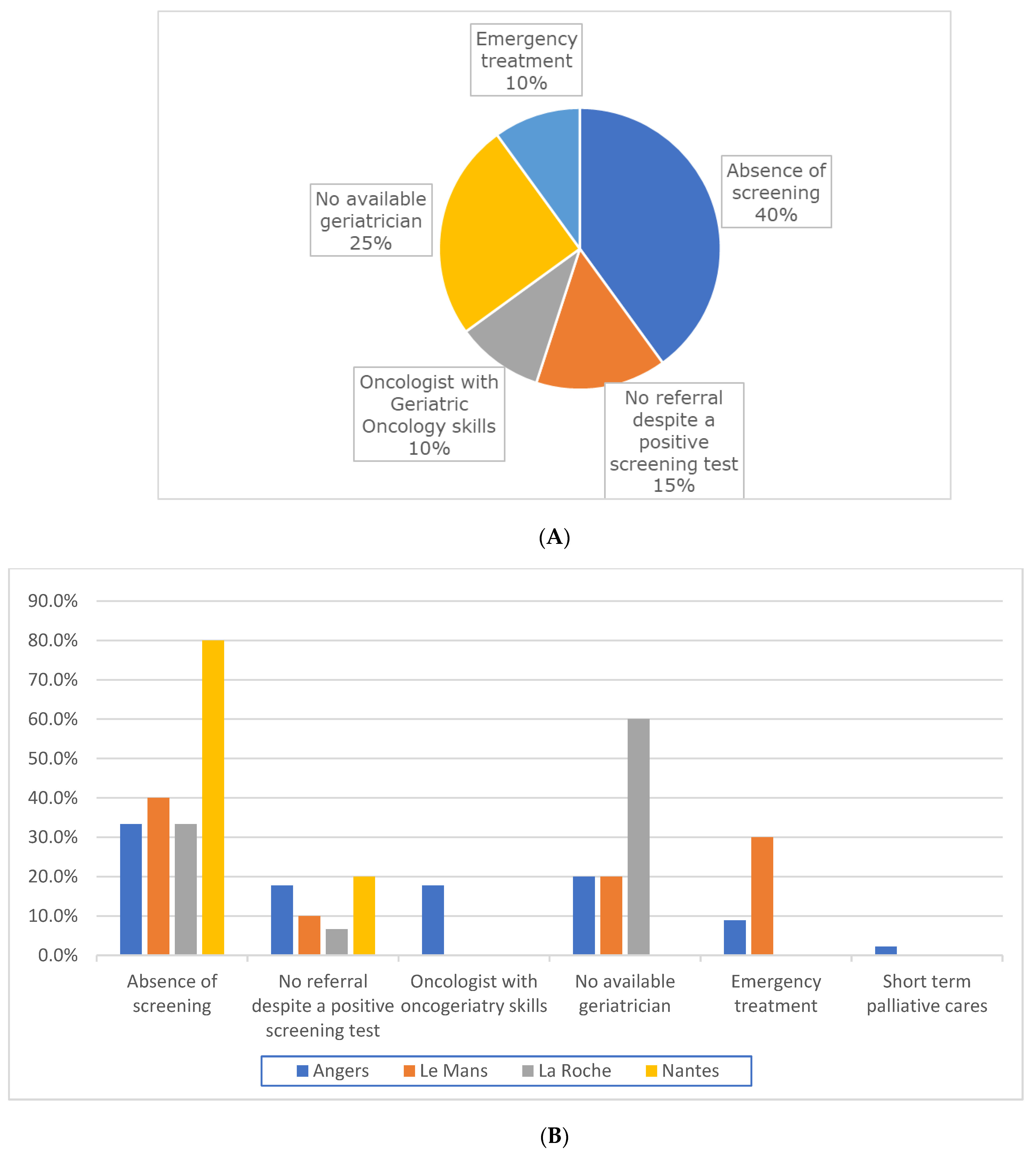
3.2. Geriatric Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- INCA—Les Cancers en France. Available online: https://www.e-cancer.fr/ressources/cancers_en_france/#page=59 (accessed on 8 March 2021).
- Boyle, H.J.; Alibhai, S.; Decoster, L.; Efstathiou, E.; Fizazi, K.; Mottet, N.; Oudard, S.; Payne, H.; Prentice, M.; Puts, M.; et al. Updated Recommendations of the International Society of Geriatric Oncology on Prostate Cancer Management in Older Patients. Eur. J. Cancer 2019, 116, 116–136. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [Green Version]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Clough-Gorr, K.M.; Thwin, S.S.; Stuck, A.E.; Silliman, R.A. Examining Five- and Ten-Year Survival in Older Women with Breast Cancer Using Cancer-Specific Geriatric Assessment. Eur. J. Cancer Oxf. Engl. 1990 2012, 48, 805–812. [Google Scholar] [CrossRef] [Green Version]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting Chemotherapy Toxicity in Older Adults With Cancer: A Prospective Multicenter Study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H.; Brown, R.H.; DeFelice, J.; Levine, R.M.; Lubiner, E.T.; Reyes, P.; Schreiber, F.J.; et al. Predicting the Risk of Chemotherapy Toxicity in Older Patients: The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) Score. Cancer 2012, 118, 3377–3386. [Google Scholar] [CrossRef]
- Kenis, C.; Bron, D.; Libert, Y.; Decoster, L.; Van Puyvelde, K.; Scalliet, P.; Cornette, P.; Pepersack, T.; Luce, S.; Langenaeken, C.; et al. Relevance of a Systematic Geriatric Screening and Assessment in Older Patients with Cancer: Results of a Prospective Multicentric Study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 1306–1312. [Google Scholar] [CrossRef]
- Corre, R.; Greillier, L.; Le Caër, H.; Audigier-Valette, C.; Baize, N.; Bérard, H.; Falchero, L.; Monnet, I.; Dansin, E.; Vergnenègre, A.; et al. Use of a Comprehensive Geriatric Assessment for the Management of Elderly Patients With Advanced Non-Small-Cell Lung Cancer: The Phase III Randomized ESOGIA-GFPC-GECP 08-02 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1476–1483. [Google Scholar] [CrossRef]
- Soto-Perez-de-Celis, E.; Aapro, M.; Muss, H. ASCO 2020: The Geriatric Assessment Comes of Age. Oncologist 2020, 25, 909–912. [Google Scholar] [CrossRef]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Curé, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; van Praagh, I.; et al. Screening for Vulnerability in Older Cancer Patients: The ONCODAGE Prospective Multicenter Cohort Study. PLoS ONE 2014, 9, e115060. [Google Scholar] [CrossRef]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- VanderWalde, N.; Jagsi, R.; Dotan, E.; Baumgartner, J.; Browner, I.S.; Burhenn, P.; Cohen, H.J.; Edil, B.H.; Edwards, B.; Extermann, M.; et al. NCCN Guidelines Insights: Older Adult Oncology, Version 2.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 1357–1370. [Google Scholar] [CrossRef]
- Le Plan Cancer 2003–2007—Les Plans Cancer. Available online: https://www.e-cancer.fr/Institut-national-du-cancer/Strategie-de-lutte-contre-les-cancers-en-France/Les-Plans-cancer/Le-Plan-cancer-2003-2007 (accessed on 9 March 2021).
- Le Plan Cancer 2009–2013. Available online: https://www.e-cancer.fr/Institut-national-du-cancer/Strategie-de-lutte-contre-les-cancers-en-France/Les-Plans-cancer/Le-Plan-cancer-2009-2013 (accessed on 14 February 2023).
- Le Plan Cancer 2014–2019—Les Plans cancer. Available online: https://www.e-cancer.fr/Institut-national-du-cancer/Strategie-de-lutte-contre-les-cancers-en-France/Les-Plans-cancer/Le-Plan-cancer-2014-2019 (accessed on 9 March 2021).
- Dale, W.; Williams, G.R.; MacKenzie, A.R.; Soto-Perez-de-Celis, E.; Maggiore, R.J.; Merrill, J.K.; Katta, S.; Smith, K.T.; Klepin, H.D. How Is Geriatric Assessment Used in Clinical Practice for Older Adults With Cancer? A Survey of Cancer Providers by the American Society of Clinical Oncology. JCO Oncol. Pract. 2021, 17, 336–344. [Google Scholar] [CrossRef]
- Plotkin, E.; Lucas, L.; Burhenn, P.S.; Nightingale, G.; Loh, K.P.; Allen, P.D.; Dotan, E. Geriatric Assessment Adoption in Community Cancer Centers: Trends, Bariers, and Recommendations. Innov. Aging 2019, 3 (Suppl. 1), S122. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Toh, Y.; Tanimizu, M.; Nakagama, H.; Japanese Association of Clinical Cancer Centers. Geriatric Screening for Hospitalized Older Adults with Cancer: A Survey of the Japanese Association of Clinical Cancer Centers. Intern. Med. Tokyo Jpn. 2021, 60, 2927–2932. [Google Scholar] [CrossRef]
- Williams, G.R.; Weaver, K.E.; Lesser, G.J.; Dressler, E.; Winkfield, K.M.; Neuman, H.B.; Kazak, A.E.; Carlos, R.; Gansauer, L.J.; Kamen, C.S.; et al. Capacity to Provide Geriatric Specialty Care for Older Adults in Community Oncology Practices. Oncologist 2020, 25, 1032–1038. [Google Scholar] [CrossRef]
- Kenis, C.; Heeren, P.; Decoster, L.; Van Puyvelde, K.; Conings, G.; Cornelis, F.; Cornette, P.; Moor, R.; Luce, S.; Libert, Y.; et al. A Belgian Survey on Geriatric Assessment in Oncology Focusing on Large-Scale Implementation and Related Barriers and Facilitators. J. Nutr. Health Aging 2016, 20, 60–70. [Google Scholar] [CrossRef]
- Hurria, A.; Lichtman, S.M.; Gardes, J.; Li, D.; Limaye, S.; Patil, S.; Zuckerman, E.; Tew, W.; Hamlin, P.; Abou-Alfa, G.K.; et al. Identifying Vulnerable Older Adults with Cancer: Integrating Geriatric Assessment into Oncology Practice. J. Am. Geriatr. Soc. 2007, 55, 1604–1608. [Google Scholar] [CrossRef]
- Festen, S.; Kok, M.; Hopstaken, J.S.; van der Wal-Huisman, H.; van der Leest, A.; Reyners, A.K.L.; de Bock, G.H.; de Graeff, P.; van Leeuwen, B.L. How to Incorporate Geriatric Assessment in Clinical Decision-Making for Older Patients with Cancer. An Implementation Study. J. Geriatr. Oncol. 2019, 10, 951–959. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Hurria, A.; Hortobagyi, G.N.; Buchholz, T.A. Future of Cancer Incidence in the United States: Burdens upon an Aging, Changing Nation. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 2758–2765. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Geriatric Assessment | |||
|---|---|---|---|
| Yes | No | ||
| (n = 51) | (n = 80) | p-Value | |
| Age | |||
| Mean ± SD | 81.4 ± 3.8 | 79.4 ± 3.9 | 0.006 |
| ≥80 years, n (%) | 33 (64.7) | 34 (42.5) | 0.013 |
| Performance status | |||
| 0–1, n (%) | 16 (31.4) | 42 (52.5) | 0.018 |
| ≥2, n (%) | 35 (68.6) | 38 (47.5) | 0.018 |
| Comorbidities | |||
| CIRS | |||
| Mean ± SD | 9.9 ± 4.4 | 9.77 ± 4.6 | 0.874 |
| Charlson Comorbidity Index | |||
| Mean ± SD | 1.2 ± 1.5 | 0.75 ± 1.0 | 0.062 |
| 0–1, n (%) | 31 (60.8) | 61 (76.3) | 0.059 |
| ≥2, n (%) | 20 (39.2) | 19 (23.8) | 0.059 |
| Chronic heart failure, n (%) | 5 (9.8) | 8 (10.0) | 0.999 |
| Polypharmacy | |||
| Mean ± SD | 8.25 ± 3.3 | 8.05 ± 2.6 | 0.709 |
| >5, n (%) | 40 (78.4) | 70 (87.5) | 0.168 |
| Prostate disease, n (%) | |||
| Low volume | 2 (3.9) | 2 (2.5) | 0.642 |
| High volume | 49 (96.1) | 78 (97.5) | 0.642 |
| Visceral metastasis | 20 (39.2) | 21 (26.3) | 0.127 |
| PSA (ng/mL) | |||
| Median (range) | 101 (0.5–1739) | 74 (0.1–5000) | |
| Mean ± SD | 263.3 (399.2) | 323.8 (737.8) | 0.545 |
| Hormonal status, n (%) | |||
| Hormone-sensitive | 6 (11.8) | 19 (23.8) | 0.112 |
| Hormone-refractory | 45 (88.2) | 61 (76.3) | 0.112 |
| G8 screening | |||
| Available, n (%) | 41 (80.4) | 37 (46.3) | <0.001 |
| Mean ± SD | 10.5 ± 3.0 | 11.6 ± 2.6 | 0.066 |
| Cognitive troubles, n (%) | 10 (19.6) | 4 (5.0) | 0.017 |
| Severe undernutrition, n (%) | 13 (25.5) | 14 (17.5) | 0.27 |
| ADL score ≤ 4 /6, n (%) | 6 (11.7) | 4 (5.0) | 0.186 |
| IADL score ≤ 3/4, n (%) | 23 (45.1) | 13 (16.5) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gluszak, C.; Campion, L.; Seegers, V.; Cojocarasu, O.; Commer, J.-M.; Priou, F.; Rolland, F.; Terret, C.; Abadie-Lacourtoisie, S. Geriatric Assessment Implementation before Chemotherapy in MEtastatic Prostate Cancer, Results from the Real-Life Study GAMERS. J. Clin. Med. 2023, 12, 1636. https://doi.org/10.3390/jcm12041636
Gluszak C, Campion L, Seegers V, Cojocarasu O, Commer J-M, Priou F, Rolland F, Terret C, Abadie-Lacourtoisie S. Geriatric Assessment Implementation before Chemotherapy in MEtastatic Prostate Cancer, Results from the Real-Life Study GAMERS. Journal of Clinical Medicine. 2023; 12(4):1636. https://doi.org/10.3390/jcm12041636
Chicago/Turabian StyleGluszak, Cassandre, Loïc Campion, Valérie Seegers, Oana Cojocarasu, Jean-Marie Commer, Frank Priou, Frédéric Rolland, Catherine Terret, and Sophie Abadie-Lacourtoisie. 2023. "Geriatric Assessment Implementation before Chemotherapy in MEtastatic Prostate Cancer, Results from the Real-Life Study GAMERS" Journal of Clinical Medicine 12, no. 4: 1636. https://doi.org/10.3390/jcm12041636