
Association of GLIM Defined Malnutrition According to Preoperative Chronic Inflammation with Long-Term Prognosis after Gastrectomy in Patients with Advanced Gastric Cancer

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Definition of Malnutrition and Chronic Inflammation
2.3. Postoperative Adjuvant Chemotherapy
2.4. Endpoints
3. Results
3.1. Patient Background
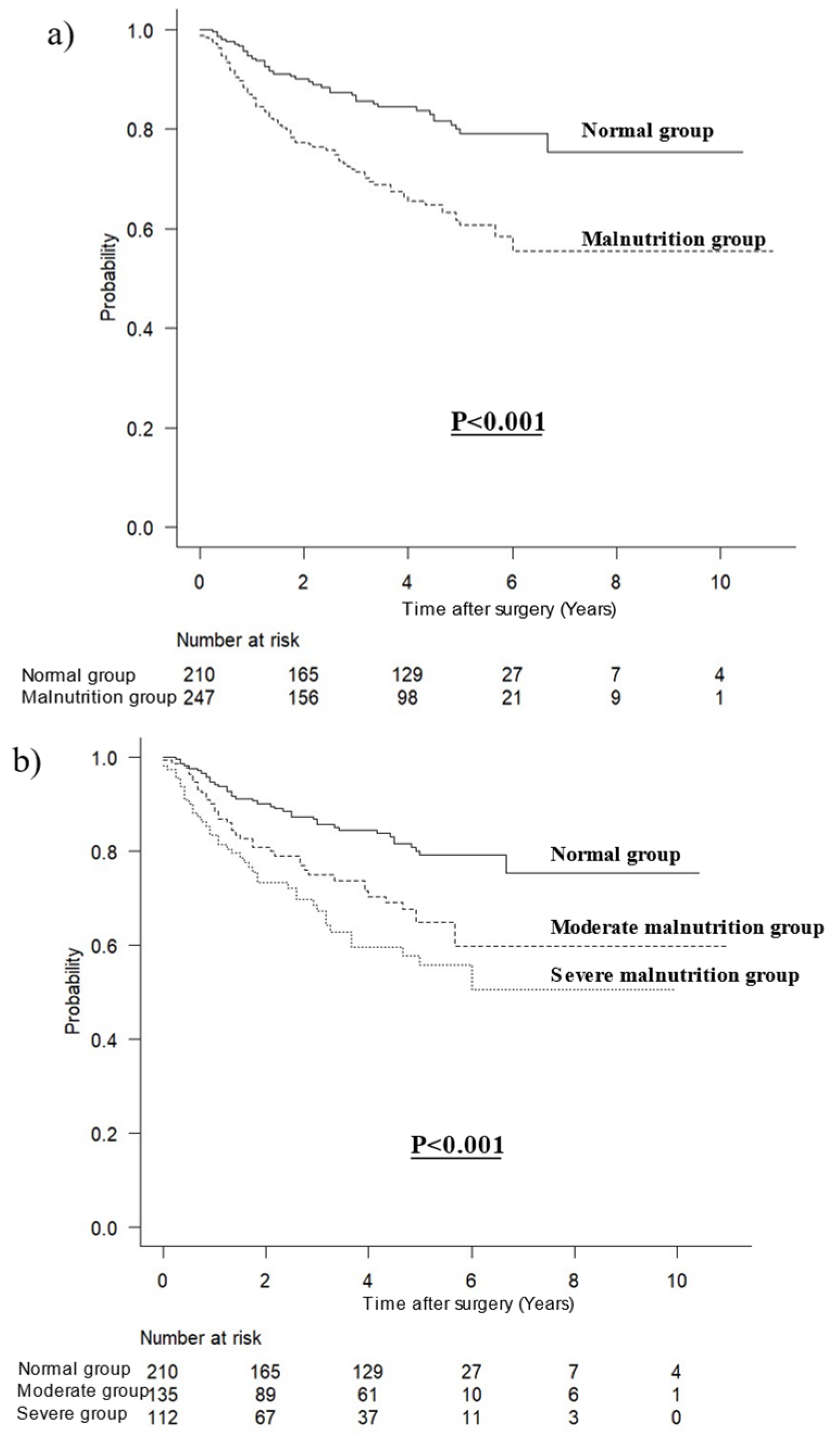
3.2. Overall Survival in All Patients
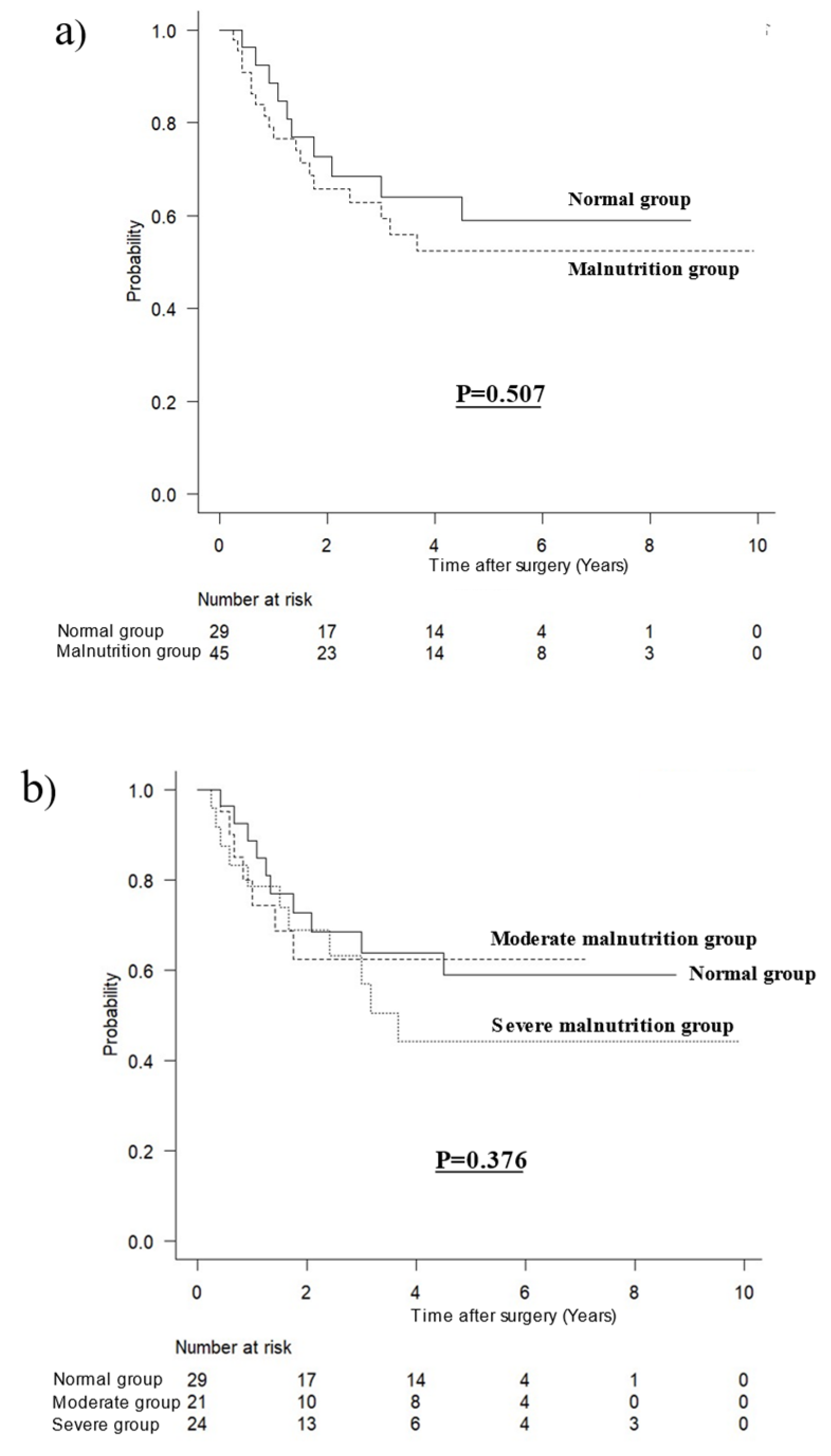
3.3. Overall Survival According to Malnutrition by Inflammation
3.4. Prognostic Factors for Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Shi, M.; Huang, Z.; Zhang, W.; Zhang, H.; Shen, X.; Chen, X. Impact of malnutrition diagnosed using Global Leadership Initiative on Malnutrition criteria on clinical outcomes of patients with gastric cancer. J. Parenter. Enter. Nutr. 2021, 46, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Matsui, R.; Inaki, N.; Tsuji, T. Impact of GLIM Defined Malnutrition on Long Term Prognosis in Patients with Gastric Cancer After Gastrectomy. Anticancer Res. 2022, 42, 4611–4618. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Xu, D.; Song, H.; Qiu, B.; Tian, D.; Li, Z.; Ji, Y.; Wang, J. Inflammation and nutrition-based biomarkers in the prognosis of oesophageal cancer: A systematic review and meta-analysis. BMJ Open 2021, 11, e048324. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; Laird, B.J.; Horgan, P.G.; McMillan, D.C. The prognostic value of the systemic inflammatory response in randomised clinical trials in cancer: A systematic review. Crit. Rev. Oncol. 2018, 132, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M.; Academy Malnutrition Work Group; ASPEN Malnutrition Task Force; ASPEN Board of Directors. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J. Parenter Enter. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of Baseline Inflammation With Effectiveness of Nutritional Support Among Patients With Disease-Related Malnutrition: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef] [PubMed]
- Shirai, Y.; Okugawa, Y.; Hishida, A.; Ogawa, A.; Okamoto, K.; Shintani, M.; Morimoto, Y.; Nishikawa, R.; Yokoe, T.; Tanaka, K.; et al. Fish oil-enriched nutrition combined with systemic chemotherapy for gastrointestinal cancer patients with cancer cachexia. Sci. Rep. 2017, 7, 4826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.-R.; Kim, A.-S.; Choi, H.-I.; Jung, J.-H.; Park, J.Y.; Ko, H.-J. Inflammatory markers for predicting overall survival in gastric cancer patients: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236445. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, X.; Wu, T.; Zhang, Y.; Yan, K.; Sun, X. Modified glasgow prognostic score as a prognostic factor in gastric cancer patients: A systematic review and meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 15222–15229. [Google Scholar] [PubMed]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic inflammation and cytokines in the tumor microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Xu, L.; Wang, Q.; Li, J.; Bai, B.; Li, Z.; Wu, X.; Yu, P.; Li, X.; Yin, J. Postoperative complications and prognosis after radical gastrectomy for gastric cancer: A systematic review and meta-analysis of observational studies. World J. Surg. Oncol. 2019, 17, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, L.; Wu, D.; Chen, Y.; Ni, J.; Qu, H.; Li, Z.; Chen, X. Associations of radiological features of adipose tissues with postoperative complications and overall survival of gastric cancer patients. Eur. Radiol. 2022, 32, 8569–8578. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Z.; Jiang, L.; Xue, Z.; Ma, Z.; Kang, W.; Ye, X.; Liu, Y.; Jin, Z.; Yu, J. Impact of body composition on clinical outcomes in people with gastric cancer undergoing radical gastrectomy after neoadjuvant treatment. Nutrition 2021, 85, 111135. [Google Scholar] [CrossRef] [PubMed]
- Marano, L.; Ambrosio, M.R.; Resca, L.; Carbone, L.; Carpineto Samorani, O.; Petrioli, R.; Savelli, V.; Costantini, M.; Malaspina, L.; Polom, K.; et al. The Percentage of Signet Ring Cells Is Inversely Related to Aggressive Behavior and Poor Prognosis in Mixed-Type Gastric Cancer. Front. Oncol. 2022, 12, 897218. [Google Scholar] [CrossRef] [PubMed]
- Roviello, F.; Marano, L.; Ambrosio, M.R.; Resca, L.; D’Ignazio, A.; Petrelli, F.; Petrioli, R.; Costantini, M.; Polom, K.; Macchiarelli, R.; et al. Signet ring cell percentage in poorly cohesive gastric cancer patients: A potential novel predictor of survival. Eur. J. Surg. Oncol. (EJSO) 2021, 48, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Pozzo, C.; Strippoli, A.; Bria, E.; Tortora, G.; Gasbarrini, A.; Mele, M.C. Muscle mass, assessed at diagnosis by L3-CT scan as a prog nostic marker of clinical outcomes in patients with gastric cancer: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 2045–2054. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity Grade | Phenotypic Criteria | ||
|---|---|---|---|
| Weight Loss Before Surgery (%) | Low-Body Mass Index (kg/m2) | Reduced Muscle Mass (SMI) | |
| Moderate malnutrition | 5–10% within the past 6 months, or 10–20% beyond 6 months | <20.0 if <70 years old, or <22.0 if ≥70 years old | Male: 40.8 cm2/m2 Female: 34.9 cm2/m2 |
| Severe malnutrition | >10% within the past 6 months, or >20% beyond 6 months | <18.5 if <70 years old, or <20.0 if ≥70 years old | Male: 34.5 cm2/m2 Female: 28.9 cm2/m2 |
| Total | Non-Inflammation Group | Inflammation Group | p Value | ||
|---|---|---|---|---|---|
| (N = 457) | (n = 383) | (n = 74) | |||
| Age, mean ± SD | 67.88 ± 11.00 | 67.12 ± 10.98 | 71.82 ± 10.30 | 0.001 | |
| Sex | Male | 301 (65.9%) | 252 (65.8%) | 49 (66.2%) | 1 |
| Female | 156 (34.1%) | 131 (34.2%) | 25 (33.8%) | ||
| Body mass index, mean ± SD | 22.90 ± 3.52 | 22.92 ± 3.45 | 22.79 ± 3.91 | 0.782 | |
| Surgical approach | |||||
| Laparoscopic | 253 (55.4%) | 226 (59.0%) | 27 (36.5%) | 0.001 | |
| Open | 204 (44.6%) | 157 (41.0%) | 47 (63.5%) | ||
| Performed procedure | |||||
| Distal gastrectomy | 255 (55.8%) | 223 (58.2%) | 32 (43.2%) | 0.034 | |
| Proximal gastrectomy | 24 (5.3%) | 21 (5.5%) | 3 (4.1%) | ||
| Total gastrectomy | 178 (38.9%) | 139 (36.3%) | 39 (52.7%) | ||
| Lymph node dissection | 0.158 | ||||
| D1+ | 198 (43.3%) | 160 (41.8%) | 38 (51.4%) | ||
| D2 | 259 (56.7%) | 223 (58.2%) | 36 (48.6%) | ||
| Clinical stage | I | 87 (19.0%) | 74 (19.3%) | 13 (17.6%) | 0.72 |
| II | 72 (15.8%) | 58 (15.1%) | 14 (18.9%) | ||
| III | 298 (65.2%) | 251 (65.5%) | 47 (63.5%) | ||
| Pathological stage | I | 88 (19.3%) | 75 (19.6%) | 13 (17.6%) | 0.067 |
| II | 176 (38.5%) | 155 (40.5%) | 21 (28.4%) | ||
| III | 193 (42.2%) | 153 (39.9%) | 40 (54.1%) | ||
| Serosal invasion | Absent | 347 (75.9%) | 294 (76.8%) | 53 (71.6%) | 0.373 |
| Present | 110 (24.1%) | 89 (23.2%) | 21 (28.4%) | ||
| Lymph node metastasis | Absent | 132 (28.9%) | 107 (27.9%) | 25 (33.8%) | 0.328 |
| N1 | 116 (25.4%) | 104 (27.2%) | 12 (16.2%) | ||
| N2 | 100 (21.9%) | 82 (21.4%) | 18 (24.3%) | ||
| N3 | 109 (23.9%) | 90 (23.5%) | 19 (25.7%) | ||
| Histological type | 1 | ||||
| Differentiated | 199 (43.5%) | 167 (43.6%) | 32 (43.2%) | ||
| Undifferentiated | 258 (56.5%) | 216 (56.4%) | 42 (56.8%) | ||
| Comorbidity | CKD | 80 (17.5%) | 65 (17.0%) | 15 (20.3%) | 0.505 |
| COPD | 99 (21.7%) | 77 (20.1%) | 22 (29.7%) | 0.089 | |
| Diabetes | 84 (18.4%) | 70 (18.3%) | 14 (18.9%) | 0.871 | |
| CHF | 24 (5.3%) | 20 (5.2%) | 4 (5.4%) | 1 | |
| GLIM malnutrition | Normal | 210 (46.0%) | 181 (47.3%) | 29 (39.2%) | 0.208 |
| Moderate | 135 (29.5%) | 114 (29.8%) | 21 (28.4%) | ||
| Severe | 112 (24.5%) | 88 (23.0%) | 24 (32.4%) | ||
| Geriatric Nutritional Risk Index | 103.9 | 104.7 | 96.85 | <0.001 | |
| (96.45–111.7) | (98.00–112.4) | (89.08–104.7) | |||
| Prognostic Nutritional Index | 49.26 | 49.78 | 43.27 | <0.001 | |
| (44.89–53.31) | (46.20–53.96) | (39.55–47.49) | |||
| SMI (cm2/m2), median (IQR) | 39.25 (34.25−45.39) | 39.17 (34.47−45.67) | 39.59 (32.64−44.11) | 0.209 | |
| VFA (cm2), median (IQR) | 85.00 (46.60−137.1) | 83.02 (45.05−137.9) | 86.00 (55.36−125.3) | 0.607 | |
| ≥100 cm2 | 181 (42.0%) | 152 (42.2%) | 29 (40.8%) | 0.896 | |
| Postoperative complications | |||||
| Total complications | 100 (21.9%) | 73 (19.1%) | 27 (36.5%) | 0.002 | |
| Severe complications | 45 (9.8%) | 35 (9.1%) | 10 (13.5%) | 0.285 | |
| Abdominal abscess | 53 (11.6%) | 41 (10.7%) | 12 (16.2%) | 0.17 | |
| Pneumonia | 16 (3.5%) | 11 (2.9%) | 5 (6.8%) | 0.155 | |
| Incisional SSI | 10 (2.2%) | 8 (2.1%) | 2 (2.7%) | 0.668 | |
| Anastomotic leakage | 21 (4.6%) | 13 (3.4%) | 8 (10.8%) | 0.011 | |
| Pancreatic leakage | 30 (6.6%) | 26 (6.8%) | 4 (5.4%) | 0.802 | |
| Postoperative chemotherapy | |||||
| Absent | 176 (38.5%) | 139 (36.3%) | 37 (50.0%) | 0.036 | |
| Present | 281 (61.5%) | 244 (63.7%) | 37 (50.0%) | ||
| Variables | Multivariate Analysis | |||
|---|---|---|---|---|
| HR | 95% CI | p Value | ||
| Age (years) | <70 | 1 | ||
| ≥70 | 3.53 | 1.337–9.318 | 0.011 | |
| Serosal invasion | Absent | 1 | ||
| Present | 3.12 | 1.191–8.173 | 0.021 | |
| Lymph node metastasis | Absent | 1 | ||
| N3 | 4.124 | 1.815–9.370 | <0.001 | |
| Histological type | Differentiated | 1 | ||
| Undifferentiated | 0.422 | 0.188–0.945 | 0.036 | |
| Variables | Multivariate Analysis | |||
|---|---|---|---|---|
| HR | 95% CI | p Value | ||
| Age (years) | <70 | 1 | ||
| ≥70 | 1.956 | 1.263–3.029 | 0.003 | |
| Surgical approach | Laparoscopic | 1 | ||
| Open | 1.927 | 1.229–3.021 | 0.004 | |
| Lymph node metastasis | Absent | 1 | ||
| N3 | 2.767 | 1.765–4.338 | <0.001 | |
| GLIM malnutrition | Normal | 1 | ||
| Moderate | 1.749 | 1.037–2.949 | 0.036 | |
| Severe | 1.971 | 1.130–3.439 | 0.017 | |
| Postoperative complication | Absent | 1 | ||
| Severe complications | 2.627 | 1.474–4.681 | 0.001 | |
| VFA (cm2) | <100 | 1 | ||
| ≥100 | 0.531 | 0.326–0.866 | 0.011 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsui, R.; Inaki, N.; Tsuji, T.; Fukunaga, T. Association of GLIM Defined Malnutrition According to Preoperative Chronic Inflammation with Long-Term Prognosis after Gastrectomy in Patients with Advanced Gastric Cancer. J. Clin. Med. 2023, 12, 1579. https://doi.org/10.3390/jcm12041579
Matsui R, Inaki N, Tsuji T, Fukunaga T. Association of GLIM Defined Malnutrition According to Preoperative Chronic Inflammation with Long-Term Prognosis after Gastrectomy in Patients with Advanced Gastric Cancer. Journal of Clinical Medicine. 2023; 12(4):1579. https://doi.org/10.3390/jcm12041579
Chicago/Turabian StyleMatsui, Ryota, Noriyuki Inaki, Toshikatsu Tsuji, and Tetsu Fukunaga. 2023. "Association of GLIM Defined Malnutrition According to Preoperative Chronic Inflammation with Long-Term Prognosis after Gastrectomy in Patients with Advanced Gastric Cancer" Journal of Clinical Medicine 12, no. 4: 1579. https://doi.org/10.3390/jcm12041579