
Incidence of Invasive Fungal Infections in Liver Transplant Recipients under Targeted Echinocandin Prophylaxis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
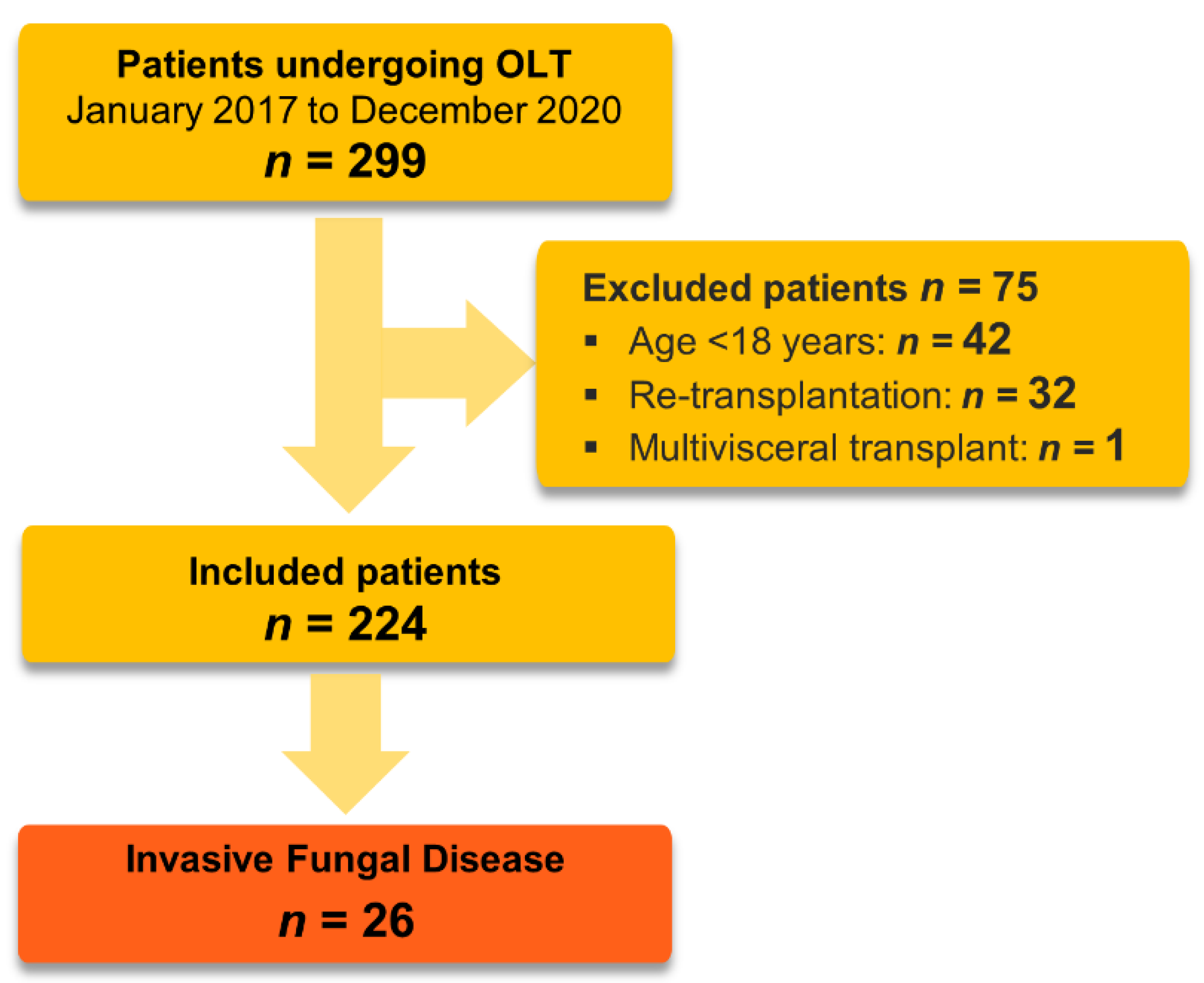
2.1. Study Design and Population
2.2. Definition of an Invasive Fungal Infection (IFI)
2.3. Immunosuppressive Regimen and Prophylaxis
2.4. Surgical Technique
- -
- Donor-related: in cases of ECD, especially if prolonged ischemia times are expected
- -
- Recipient-related: in cases of surgically highly complex recipients or high-risk patients
- -
- Logistic-related: in case of limited resources (e.g., parallel organ transplantations or overlap with other urgent interventions).
2.5. Data Acquisition
2.6. Outcomes
2.7. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Risk Factors for Infection
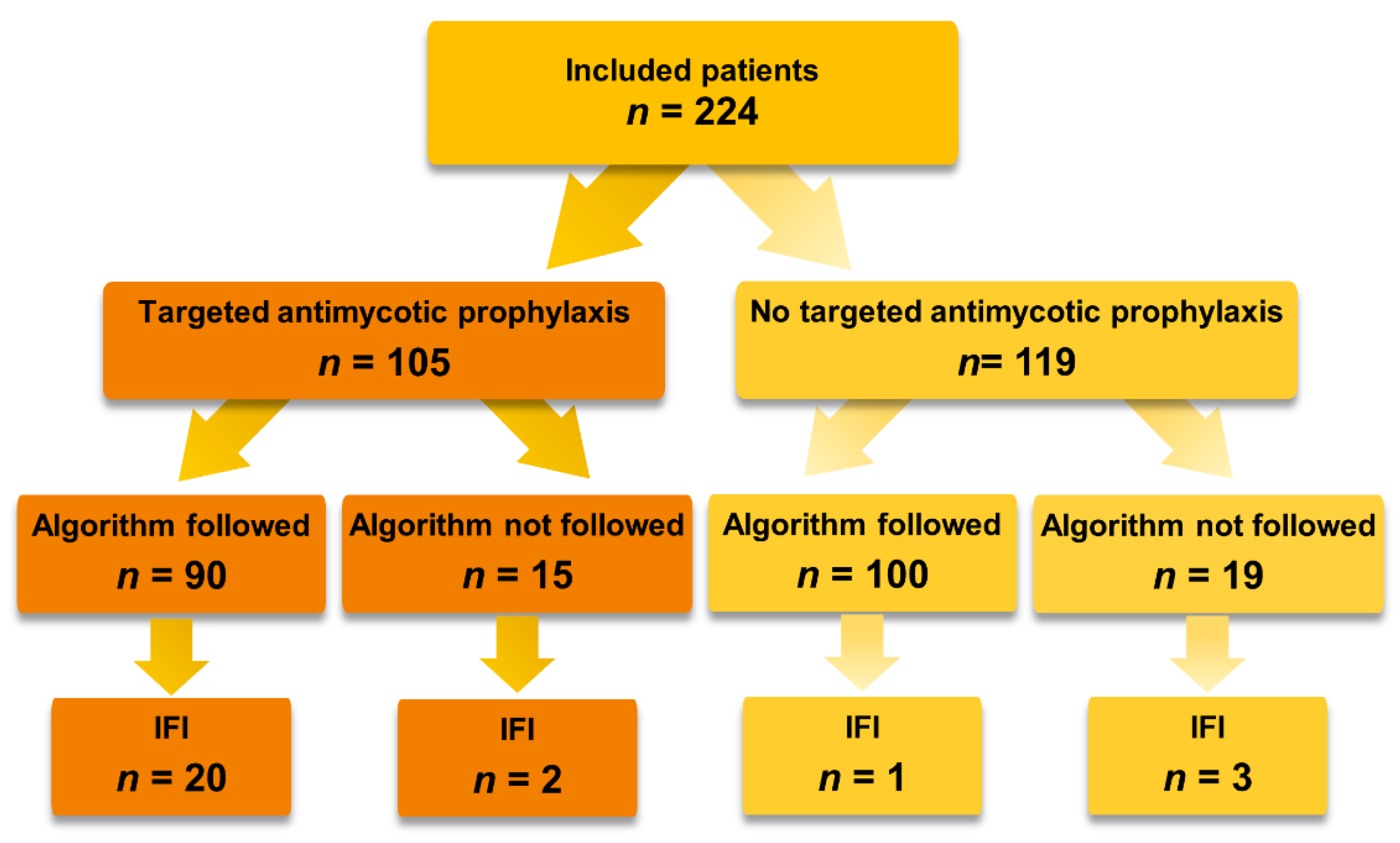
3.3. Targeted Antimycotic Prophylaxis
3.4. Incidence of Invasive Fungal Infections
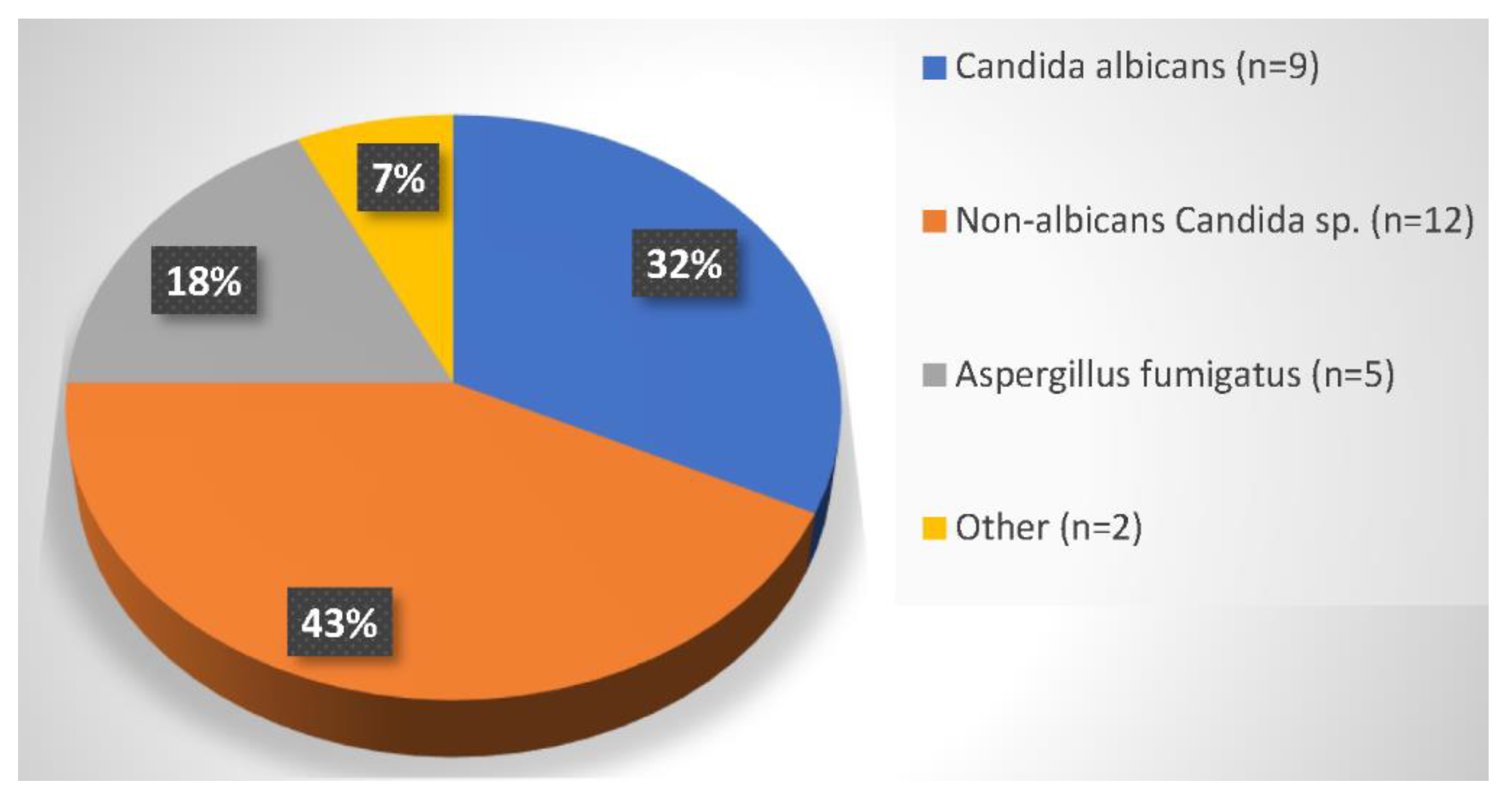
3.5. Composition and Sites of Pathogens
3.6. Time to Diagnosis
3.7. Outcome
4. Discussion
4.1. Incidence of Invasive Fungal Infections
4.2. Targeted Antimycotic Prophylaxis
4.3. Time to Diagnosis
4.4. Composition and Sites of Pathogens
4.5. Risk Factors for Infection
4.6. Outcomes
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adam, R.; Karam, V.; Delvart, V.; O’Grady, J.; Mirza, D.; Klempnauer, J.; Castaing, D.; Neuhaus, P.; Jamieson, N.; Salizzoni, M.; et al. Evolution of Indications and Results of Liver Transplantation in Europe. A Report from the European Liver Transplant Registry (ELTR). J. Hepatol. 2012, 57, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Reyes, J.; Kashyap, R.; Dodson, S.F.; Demetris, A.J.; Ruppert, K.; Abu-Elmagd, K.; Marsh, W.; Madariaga, J.; Mazariegos, G.; et al. Long-Term Survival after Liver Transplantation in 4,000 Consecutive Patients at a Single Center. Ann. Surg. 2000, 232, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Waki, K. UNOS Liver Registry: Ten Year Survivals. Clin. Transpl. 2006, 29–39. [Google Scholar]
- Rana, A.; Ackah, R.L.; Webb, G.J.; Halazun, K.J.; Vierling, J.M.; Liu, H.; Wu, M.F.; Yoeli, D.; Kueht, M.; Mindikoglu, A.L.; et al. No Gains in Long-Term Survival After Liver Transplantation Over the Past Three Decades. Ann. Surg. 2019, 269, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Baganate, F.; Beal, E.W.; Tumin, D.; Azoulay, D.; Mumtaz, K.; Black, S.M.; Washburn, K.; Pawlik, T.M. Early Mortality after Liver Transplantation: Defining the Course and the Cause. Surgery 2018, 164, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Agopian, V.G.; Harlander-Locke, M.P.; Markovic, D.; Dumronggittigule, W.; Xia, V.; Kaldas, F.M.; Zarrinpar, A.; Yersiz, H.; Farmer, D.G.; Hiatt, J.R.; et al. Evaluation of Early Allograft Function Using the Liver Graft Assessment Following Transplantation Risk Score Model. JAMA Surg. 2018, 153, 436–444. [Google Scholar] [CrossRef]
- Rana, A.; Kaplan, B.; Jie, T.; Porubsky, M.; Habib, S.; Rilo, H.; Gruessner, A.C.; Gruessner, R.W.G. A Critical Analysis of Early Death after Adult Liver Transplants. Clin. Transplant 2013, 27, E448–E453. [Google Scholar] [CrossRef]
- Watt, K.D.S.; Pedersen, R.A.; Kremers, W.K.; Heimbach, J.K.; Charlton, M.R. Evolution of Causes and Risk Factors for Mortality Post-Liver Transplant: Results of the NIDDK Long-Term Follow-up Study. Am. J. Transplant. 2010, 10, 1420–1427. [Google Scholar] [CrossRef]
- Cuervas-Mons, V.; Martinez, A.J.; Dekker, A.; Starzl, T.E.; van Thiel, D.H. Adult Liver Transplantation: An Analysis of the Early Causes of Death in 40 Consecutive Cases. Hepatology 1986, 6, 495–501. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.I.; Wie, S.H.; Kim, Y.R.; Hur, J.A.; Choi, J.Y.; Yoon, S.K.; Moon, I.S.; Kim, D.G.; Lee, M.D.; et al. Infectious Complications in Living-Donor Liver Transplant Recipients: A 9-Year Single-Center Experience. Transpl. Infect. Dis. 2008, 10, 316–324. [Google Scholar] [CrossRef]
- Kim, S., II. Bacterial Infection after Liver Transplantation. World J. Gastroenterol. 2014, 20, 6211–6220. [Google Scholar] [CrossRef] [PubMed]
- Bert, F.; Larroque, B.; Paugam-Burtz, C.; Janny, S.; Durand, F.; Dondero, F.; Valla, D.C.; Belghiti, J.; Moreau, R.; Nicolas-Chanoine, M.H. Microbial Epidemiology and Outcome of Bloodstream Infections in Liver Transplant Recipients: An Analysis of 259 Episodes. Liver Transpl. 2010, 16, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Romero, F.A.; Razonable, R.R. Infections in Liver Transplant Recipients. World J. Hepatol. 2011, 3, 83–92. [Google Scholar] [CrossRef]
- Vera, A.; Contreras, F.; Guevara, F. Incidence and Risk Factors for Infections after Liver Transplant: Single-Center Experience at the University Hospital Fundación Santa Fe de Bogotá, Colombia. Transpl. Infect. Dis. 2011, 13, 608–615. [Google Scholar] [CrossRef]
- Scolarici, M.; Jorgenson, M.; Saddler, C.; Smith, J. Fungal Infections in Liver Transplant Recipients. J. Fungi 2021, 7, 524. [Google Scholar] [CrossRef]
- Singh, N.; Wagener, M.M.; Marino, I.R.; Gayowski, T. Trends in Invasive Fungal Infections in Liver Transplant Recipients: Correlation with Evolution in Transplantation Practices. Transplantation 2002, 73, 63–67. [Google Scholar] [CrossRef]
- Silveira, F.P.; Husain, S. Fungal Infections in Solid Organ Transplantation. Med. Mycol. 2007, 45, 305–320. [Google Scholar] [CrossRef]
- Saliba, F.; Delvart, V.; Ichaï, P.; Kassis, N.; Botterel, F.; Mihaila, L.; Azoulay, D.; Adam, R.; Castaing, D.; Bretagne, S.; et al. Fungal Infections after Liver Transplantation: Outcomes and Risk Factors Revisited in the MELD Era. Clin. Transplant. 2013, 27, E454–E461. [Google Scholar] [CrossRef]
- Paterson, D.L.; Singh, N. Invasive Aspergillosis in Transplant Recipients. Medicine 1999, 78, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Nieto-Rodriguez, J.A.; Kusne, S.; Mañez, R.; Irish, W.; Linden, P.; Magnone, M.; Wing, E.J.; Fung, J.J.; Starzl, T.E. Factors Associated with the Development of Candidemia and Candidemia-Related Death among Liver Transplant Recipients. Ann. Surg. 1996, 223, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Singh, N. Antifungal Prophylaxis in Solid-Organ Transplant Recipients: Considerations for Clinical Trial Design. Clin. Infect. Dis. 2004, 39 (Suppl. S4), S200–S206. [Google Scholar] [CrossRef] [Green Version]
- Barchiesi, F.; Mazzocato, S.; Mazzanti, S.; Gesuita, R.; Skrami, E.; Fiorentini, A.; Singh, N. Invasive Aspergillosis in Liver Transplant Recipients: Epidemiology, Clinical Characteristics, Treatment, and Outcomes in 116 Cases. Liver Transplant. 2015, 21, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Nagao, M.; Fujimoto, Y.; Yamamoto, M.; Matsumura, Y.; Kaido, T.; Takakura, S.; Uemoto, S.; Ichiyama, S. Epidemiology of Invasive Fungal Infections after Liver Transplantation and the Risk Factors of Late-Onset Invasive Aspergillosis. J. Infect. Chemother. 2016, 22, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.; Rohal, S.; Carrigan, D.R.; Kusne, S.; Knox, K.K.; Gayowski, T.; Wagener, M.M.; Fung, J.J.; Singh, N. Human Herpesvirus-6 in Liver Transplant Recipients: Role in Pathogenesis of Fungal Infections, Neurologic Complications, and Outcome. Transplantation 2000, 69, 2566–2573. [Google Scholar] [CrossRef] [PubMed]
- Karchmer, A.W.; Samore, M.H.; Hadley, S.; Collins, L.A.; Jenkins, R.L.; Lewis, W.D. Fungal Infections Complicating Orthotopic Liver Transplantation. Trans. Am. Clin. Climatol. Assoc. 1995, 106, 38. [Google Scholar] [PubMed]
- Winston, D.J.; Pakrasi, A.; Busuttil, R.W. Prophylactic Fluconazole in Liver Transplant Recipients. A Randomized, Double-Blind, Placebo-Controlled Trial. Ann. Intern. Med. 1999, 131, 729–737. [Google Scholar] [CrossRef]
- Husain, S.; Tollemar, J.; Dominguez, E.A.; Baumgarten, K.; Humar, A.; Paterson, D.L.; Wagener, M.M.; Kusne, S.; Singh, N. Changes in the Spectrum and Risk Factors for Invasive Candidiasis in Liver Transplant Recipients: Prospective, Multicenter, Case-Controlled Study. Transplantation 2003, 75, 2023–2029. [Google Scholar] [CrossRef]
- Viehman, J.A.; Clancy, C.J.; Clarke, L.; Shields, R.K.; Silveira, F.P.; Kwak, E.J.; Vergidis, P.; Hughes, C.; Humar, A.; Nguyen, M.H. Surgical Site Infections After Liver Transplantation: Emergence of Multidrug-Resistant Bacteria and Implications for Prophylaxis and Treatment Strategies. Transplantation 2016, 100, 2107–2114. [Google Scholar] [CrossRef]
- Cruciani, M.; Mengoli, C.; Malena, M.; Bosco, O.; Serpelloni, G.; Grossi, P. Antifungal Prophylaxis in Liver Transplant Patients: A Systematic Review and Meta-Analysis. Liver Transplant. 2006, 12, 850–858. [Google Scholar] [CrossRef]
- Sharpe, M.D.; Ghent, C.; Grant, D.; Horbay, G.L.A.; McDougal, J.; Colby, W.D. Efficacy and Safety of Itraconazole Prophylaxis for Fungal Infections after Orthotopic Liver Transplantation: A Prospective, Randomized, Double-Blind Study. Transplantation 2003, 76, 977–983. [Google Scholar] [CrossRef]
- Biancofiore, G.; Bindi, M.L.; Baldassarri, R.; Romanelli, A.M.; Catalano, G.; Filipponi, F.; Vagelli, A.; Mosca, F. Antifungal Prophylaxis in Liver Transplant Recipients: A Randomized Placebo-Controlled Study. Transpl. Int. 2002, 15, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Lumbreras, C.; Cuervas-Mons, V.; Jara, P.; del Palacio, A.; Turrión, V.S.; Barrios, C.; Moreno, E.; Noriega, A.R.; Paya, C.V. Randomized Trial of Fluconazole versus Nystatin for the Prophylaxis of Candida Infection Following Liver Transplantation. J. Infect. Dis. 1996, 174, 583–588. [Google Scholar] [CrossRef]
- Tollemar, J.; Höckerstedt, K.; Ericzon, B.G.; Jalanko, H.; Ringdén, O. Liposomal Amphotericin B Prevents Invasive Fungal Infections in Liver Transplant Recipients. A Randomized, Placebo-Controlled Study. Transplantation 1995, 59, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Playford, E.G.; Webster, A.C.; Craig, J.C.; Sorrell, T.C. Antifungal Agents for Preventing Fungal Infections in Solid Organ Transplant Recipients. Cochrane Database Syst. Rev. 2004, CD004291. [Google Scholar] [CrossRef]
- Singh, N. Antifungal Prophylaxis for Solid Organ Transplant Recipients: Seeking Clarity amidst Controversy. Clin. Infect. Dis. 2000, 31, 545–553. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008, 46, 1813. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Azoulay, E.; Kullberg, B.J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef]
- Blot, S.I.; Vandewoude, K.H.; de Waele, J.J. Candida Peritonitis. Curr. Opin. Crit. Care 2007, 13, 195–199. [Google Scholar] [CrossRef]
- Montravers, P.; Dupont, H.; Eggimann, P. Intra-Abdominal Candidiasis: The Guidelines—Forgotten Non-Candidemic Invasive Candidiasis. Intensive Care Med. 2013, 39, 2226–2230. [Google Scholar] [CrossRef]
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID* Guideline for the Diagnosis and Management of Candida Diseases 2012: Non-Neutropenic Adult Patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef]
- Carneiro, H.A.; Mavrakis, A.; Mylonakis, E. Candida Peritonitis: An Update on the Latest Research and Treatments. World J. Surg. 2011, 35, 2650–2659. [Google Scholar] [CrossRef] [PubMed]
- Nemes, B.; Gámán, G.; Polak, W.G.; Gelley, F.; Hara, T.; Ono, S.; Baimakhanov, Z.; Piros, L.; Eguchi, S. Extended Criteria Donors in Liver Transplantation Part I: Reviewing the Impact of Determining Factors. Expert. Rev. Gastroenterol. Hepatol. 2016, 10, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Cardini, B.; Oberhuber, R.; Fodor, M.; Hautz, T.; Margreiter, C.; Resch, T.; Scheidl, S.; Maglione, M.; Bösmüller, C.; Mair, H.; et al. Clinical Implementation of Prolonged Liver Preservation and Monitoring Through Normothermic Machine Perfusion in Liver Transplantation. Transplantation 2020, 104, 1917–1928. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Lto, J.; et al. Invasive Fungal Infections among Organ Transplant Recipients: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef]
- Raghuram, A.; Restrepo, A.; Safadjou, S.; Cooley, J.; Orloff, M.; Hardy, D.; Butler, S.; Koval, C.E. Invasive Fungal Infections Following Liver Transplantation: Incidence, Risk Factors, Survival, and Impact of Fluconazole-Resistant Candida Parapsilosis (2003-2007). Liver Transplant. 2012, 18, 1100–1109. [Google Scholar] [CrossRef]
- Saliba, F.; Pascher, A.; Cointault, O.; Laterre, P.-F.; Cervera, C.; de Waele, J.J.; Cillo, U.; Langer, R.M.; Lugano, M.; Göran-Ericzon, B.; et al. Randomized Trial of Micafungin for the Prevention of Invasive Fungal Infection in High-Risk Liver Transplant Recipients. Clin. Infect. Dis. 2015, 60, 997. [Google Scholar] [CrossRef]
- Winston, D.J.; Limaye, A.P.; Pelletier, S.; Safdar, N.; Morris, M.I.; Meneses, K.; Busuttil, R.W.; Singh, N. Randomized, Double-Blind Trial of Anidulafungin versus Fluconazole for Prophylaxis of Invasive Fungal Infections in High-Risk Liver Transplant Recipients. Am. J. Transplant. 2014, 14, 2758–2764. [Google Scholar] [CrossRef]
- Fortún, J.; Martín-Dávila, P.; Montejo, M.; Muñoz, P.; Cisneros, J.M.; Ramos, A.; Aragón, C.; Blanes, M.; San Juan, R.; Gavaldá, J.; et al. Prophylaxis with Caspofungin for Invasive Fungal Infections in High-Risk Liver Transplant Recipients. Transplantation 2009, 87, 424–435. [Google Scholar] [CrossRef]
- Cabezuelo, J.B.; Ramirez, P.; Acosta, F.; Torres, D.; Sansano, T.; Pons, J.A.; Bru, M.; Montoya, M.; Rios, A.; Sánchez Bueno, F.; et al. Does the Standard vs Piggyback Surgical Technique Affect the Development of Early Acute Renal Failure after Orthotopic Liver Transplantation? Transplant. Proc. 2003, 35, 1913–1914. [Google Scholar] [CrossRef]
- Pappas, P.G.; Andes, D.; Schuster, M.; Hadley, S.; Rabkin, J.; Merion, R.M.; Kauffman, C.A.; Huckabee, C.; Cloud, G.A.; Dismukes, W.E.; et al. Invasive Fungal Infections in Low-Risk Liver Transplant Recipients: A Multi-Center Prospective Observational Study. Am. J. Transplant. 2006, 6, 386–391. [Google Scholar] [CrossRef]
- Patel, R.; Portela, D.; Badley, A.D.; Harmsen, W.S.; Larson-Keller, J.J.; Ilstrup, D.M.; Keating, M.R.; Wiesner, R.H.; Krom, R.A.F.; Paya, C.V. Risk Factors of Invasive Candida and Non-Candida Fungal Infections after Liver Transplantation. Transplantation 1996, 62, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Paya, C.V. Fungal Infections in Solid-Organ Transplantation. Clin. Infect. Dis. 1993, 16, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Arnow, P.M.; Bonham, A.; Dominguez, E.; Paterson, D.L.; Pankey, G.A.; Wagener, M.M.; Yu, V.L. Invasive Aspergillosis in Liver Transplant Recipients in the 1990s. Transplantation 1997, 64, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Avery, R.K.; Munoz, P.; Pruett, T.L.; Alexander, B.; Jacobs, R.; Tollemar, J.G.; Dominguez, E.A.; Yu, C.M.; Paterson, D.L.; et al. Trends in Risk Profiles for and Mortality Associated with Invasive Aspergillosis among Liver Transplant Recipients. Clin. Infect. Dis. 2003, 36, 46–52. [Google Scholar] [CrossRef]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef]
- Eschenauer, G.A.; Lam, S.W.; Carver, P.L. Antifungal Prophylaxis in Liver Transplant Recipients. Liver Transplant. 2009, 15, 842–858. [Google Scholar] [CrossRef]
- Silvestri, L.; van Saene, H.K.F.; Milanese, M.; Gregori, D. Impact of Selective Decontamination of the Digestive Tract on Fungal Carriage and Infection: Systematic Review of Randomized Controlled Trials. Intensive Care Med. 2005, 31, 898–910. [Google Scholar] [CrossRef]
- Zwaveling, J.H.; Maring, J.K.; Klompmaker, I.J.; Haagsma, E.B.; Bottema, J.T.; Laseur, M.; Winter, H.L.J.; van Enckevort, P.J.; TenVergert, E.M.; Metselaar, H.J.; et al. Selective Decontamination of the Digestive Tract to Prevent Postoperative Infection: A Randomized Placebo-Controlled Trial in Liver Transplant Patients. Crit. Care Med. 2002, 30, 1204–1209. [Google Scholar] [CrossRef]
- Wiesner, R.H.; Hermans, P.E.; Rakela, J.; Washington, J.A.; Perkins, J.D.; Dicecco, S.; Krom, R. Selective Bowel Decontamination to Decrease Gram-Negative Aerobic Bacterial and Candida Colonization and Prevent Infection after Orthotopic Liver Transplantation. Transplantation 1988, 45, 570–574. [Google Scholar] [CrossRef]
- Barkholt, L.M.; Andersson, J.; Ericzon, B.G.; Palmgren, A.C.; Broomé, U.; Duraj, F.; Bergquist, A.; Herlenius, G.; Nord, C.E. Stool Cultures Obtained before Liver Transplantation Are Useful for Choice of Perioperative Antibiotic Prophylaxis. Transpl. Int. 1997, 10, 432–438. [Google Scholar] [CrossRef]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery. Am. J. Health Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [Green Version]
- Lortholary, O.; Renaudat, C.; Sitbon, K.; Madec, Y.; Denoeud-Ndam, L.; Wolff, M.; Fontanet, A.; Bretagne, S.; Dromer, F.; Bouges-Michel, C.; et al. Worrisome Trends in Incidence and Mortality of Candidemia in Intensive Care Units (Paris Area, 2002–2010). Intensive Care Med. 2014, 40, 1303–1312. [Google Scholar] [CrossRef]
- Gleason, T.G.; May, A.K.; Caparelli, D.; Farr, B.M.; Sawyer, R.G. Emerging Evidence of Selection of Fluconazole-Tolerant Fungi in Surgical Intensive Care Units. Arch. Surg. 1997, 132, 1197–1202. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Peacock, J.E.; Morris, A.J.; Tanner, D.C.; Nguyen, M.L.; Snydman, D.R.; Wagener, M.M.; Rinaldi, M.G.; Yu, V.L. The Changing Face of Candidemia: Emergence of Non-Candida Albicans Species and Antifungal Resistance. Am. J. Med. 1996, 100, 617–623. [Google Scholar] [CrossRef]
- Rocco, T.R.; Reinert, S.E.; Simms, H.H. Effects of Fluconazole Administration in Critically Ill Patients: Analysis of Bacterial and Fungal Resistance. Arch. Surg. 2000, 135, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Glöckner, A. Treatment and Prophylaxis of Invasive Candidiasis with Anidulafungin, Caspofungin and Micafungin:Review of the Literature. Eur. J. Med. Res. 2011, 16, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Silveira, F.P. Candida in Solid Organ Transplant Recipients. Am. J. Transplant. 2009, 9 (Suppl. S4), S173–S179. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Husain, S. Invasive Aspergillosis in Solid Organ Transplant Recipients. Am. J. Transplant. 2009, 9 (Suppl. S4), S180–S191. [Google Scholar] [CrossRef] [PubMed]
- Gavaldà, J.; Meije, Y.; Fortún, J.; Roilides, E.; Saliba, F.; Lortholary, O.; Muñoz, P.; Grossi, P.; Cuenca-Estrella, M. Invasive Fungal Infections in Solid Organ Transplant Recipients. Clin. Microbiol. Infect. 2014, 20 (Suppl. S7), 27–48. [Google Scholar] [CrossRef]
- Chen, S.C.A.; Slavin, M.A.; Sorrell, T.C. Echinocandin Antifungal Drugs in Fungal Infections: A Comparison. Drugs 2011, 71, 11–41. [Google Scholar] [CrossRef]
- Eschenauer, G.; DePestel, D.D.; Carver, P.L. Comparison of Echinocandin Antifungals. Ther. Clin. Risk Manag. 2007, 3, 71–97. [Google Scholar] [CrossRef]
- Hebert, M.F.; Townsend, R.W.; Austin, S.; Balan, G.; Blough, D.K.; Buell, D.; Keirns, J.; Bekersky, I. Concomitant Cyclosporine and Micafungin Pharmacokinetics in Healthy Volunteers. J. Clin. Pharmacol. 2005, 45, 954–960. [Google Scholar] [CrossRef]
- Fukuoka, N.; Imataki, O.; Ohnishi, H.; Kitanaka, A.; Kubota, Y.; Ishida, T.; Tanaka, T. Micafungin Does Not Influence the Concentration of Tacrolimus in Patients after Allogeneic Hematopoietic Stem Cell Transplantation. Transplant. Proc. 2010, 42, 2725–2730. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Saito, T.; Ogawa, K.; Nishio, Y.; Kosugi, S.; Suzuki, Y.; Kato, M.; Sakai, T.; Takahashi, M.; Miura, I. Drug Interactions between Micafungin at High Doses and Cyclosporine A in Febrile Neutropenia Patients after Allogeneic Hematopoietic Stem Cell Transplantation. Int. J. Clin. Pharmacol. Ther. 2012, 50, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Hebert, M.F.; Blough, D.K.; Townsend, R.W.; Allison, M.; Buell, D.; Keirns, J.; Bekersky, I. Concomitant Tacrolimus and Micafungin Pharmacokinetics in Healthy Volunteers. J. Clin. Pharmacol. 2005, 45, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Muhl, E.; Martens, T.; Iven, H.; Rob, P.; Bruch, H.P. Influence of Continuous Veno-Venous Haemodiafiltration and Continuous Veno-Venous Haemofiltration on the Pharmacokinetics of Fluconazole. Eur. J. Clin. Pharmacol. 2000, 56, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Fortún, J.; Martín-Dvila, P.; Moreno, S.; de Vicente, E.; Nuño, J.; Candelas, A.; Brcena, R.; García, M. Risk Factors for Invasive Aspergillosis in Liver Transplant Recipients. Liver Transplant. 2002, 8, 1065–1070. [Google Scholar] [CrossRef]
- Chang, F.Y.; Singh, N.; Gayowski, T.; Wagener, M.M.; Mietzner, S.M.; Stout, J.E.; Marino, I.R. Thrombocytopenia in Liver Transplant Recipients: Predictors, Impact on Fungal Infections, and Role of Endogenous Thrombopoietin. Transplantation 2000, 69, 70–75. [Google Scholar] [CrossRef]
- Eschenauer, G.A.; Kwak, E.J.; Humar, A.; Potoski, B.A.; Clarke, L.G.; Shields, R.K.; Abdel-Massih, R.; Silveira, F.P.; Vergidis, P.; Clancy, C.J.; et al. Targeted Versus Universal Antifungal Prophylaxis Among Liver Transplant Recipients. Am. J. Transplant. 2015, 15, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Rotstein, C. Candida Infections in Solid Organ Transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13623. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Preoperative | Intraoperative | Postoperative |
|---|---|---|
| MELD Score > 30 | High-urgency transplantation | Early re-transplantation within 90 days after transplant |
| Pretransplant serum creatinine > 2 mg/dL | Split-liver transplantation | Relaparotomy after transplant |
| Fungal colonization at baseline | Intraoperative transfusion of ≥ 40 units of cellular blood products, including platelets, PRBC, and autotransfusion | Post-transplant dialysis |
| Antiinfective pretreatment within 3 months before transplant | Transplantation time > 10 h | Biliary leak |
| Roux-en-y choledochojejunostomy | Cytomegalovirus viremia | |
| Donor-Derived Infection |
| Characteristics | All Patients (n = 224) | No IFI (n = 198) | IFI (n = 26) | p-Value | Missing Data (n/Total) | |
|---|---|---|---|---|---|---|
| Age (years) | 57.2 ± 11.1 | 58.0 ± 10.5 | 51.8 ± 13.9 | 0.038 | 0/224 | |
| Male sex | 172 (76.8) | 154 (77.8) | 18 (69.2) | 0.459 | 0/224 | |
| Weight (kg) | 81.5 ± 16.4 | 81.7 ± 16.0 | 80.2 ± 19.8 | 0.680 | 0/224 | |
| Height (cm) | 174.4 ± 8.5 | 174.3 ± 8.4 | 175.5 ± 8.9 | 0.480 | 0/224 | |
| Body mass index (kg/m2) | 26.8 ± 5.0 | 26.9 ± 4.9 | 25.9 ± 5.7 | 0.343 | 0/224 | |
| SAPS III score | 45.0 ± 8.5 | 44.9 ± 8.6 | 45.8 ± 8.3 | 0.635 | 7/224 | |
| MELD score | 14 (6–40) | 14 (6–40) | 16 (6–40) | 0.174 | 7/224 | |
| Charlson comorbidity index | 4 (0–12) | 4 (0–12) | 4 (0–9) | 0.672 | 2/224 | |
| Underlying disease | 0.198 | 0/224 | ||||
| Alcoholic liver disease | 56 (25.0) | 50 (25.3) | 6 (23.1) | 1.000 | 0/224 | |
| Malignancy and other tumors | 92 (41.1) | 83 (41.9) | 9 (34.6) | 0.531 | 0/224 | |
| Hepatocellular carcinoma | 85 (92.4) | 76 (91.6) | 9 (100.0) | 0.710 | ||
| Cholangiocellular carcinoma | 3 (3.3) | 3 (3.6) | 0 (0.0) | 0.528 | ||
| Neuroendocrine tumor | 3 (3.3) | 3 (3.6) | 0 (0.0) | 0.528 | ||
| Polycystic liver disease | 1 (1.1) | 1 (1.2) | 0 (0.0) | 0.716 | ||
| Virus related | 9 (4.0) | 8 (4.0) | 1 (3.8) | 1.000 | 0/224 | |
| Non-alcoholic fatty liver disease | 14 (6.3) | 14 (7.1) | 0 (0.0) | 0.380 | 0/224 | |
| Budd-Chiari syndrome | 6 (2.7) | 6 (3.0) | 0 (0.0) | 1.000 | 0/224 | |
| Acute liver failure | 10 (4.5) | 7 (3.5) | 3 (11.5) | 0.096 | 0/224 | |
| Cholestatic | 17 (7.6) | 14 (7.1) | 3 (11.5) | 0.426 | 0/224 | |
| Autoimmune hepatitis | 8 (3.6) | 6 (3.0) | 2 (7.7) | 0.234 | 0/224 | |
| Metabolic Liver Disease | 10 (4.5) | 9 (4.5) | 1 (3.8) | 1.000 | 0/224 | |
| Other | 2 (0.9) | 1 (0.5) | 1 (3.8) | 0.219 | 0/224 | |
| Risk Factors | All Patients (n = 224) | No IFI (n = 198) | IFI (n = 26) | p-Value | Missing Data (n/Total) | |
|---|---|---|---|---|---|---|
| Preoperative risk factors | ||||||
| MELD Score > 30 | 20 (8.9) | 16 (8.1) | 4 (15.4) | 0.263 | 7/224 | |
| Fungal colonization at baseline | 15 (6.7) | 10 (5.1) | 5 (19.2) | 0.019 | 0/224 | |
| Anti-infective pretreatment | 30 (13.4) | 25 (12.6) | 5 (19.2) | 0.360 | 0/224 | |
| Pretransplant serum creatinine > 2 mg/dL | 21 (9.4) | 19 (9.6) | 2 (7.7) | 1.000 | 0/224 | |
| Intraoperative risk factors | ||||||
| Choledochojejunostomy, any time | 24 (10.7) | 15 (7.6) | 9 (34.6) | <0.001 | 1/224 | |
| Choledochojejunostomy, primary | 15 (6.7) | 11 (5.6) | 4 (15.4) | 0.080 | 1/224 | |
| Transplantation time > 11 h | 4 (1.8) | 4 (2.0) | 0 (0.0) | 1.000 | 2/224 | |
| Intraoperative blood transfusion > 40 PRBC | 2 (0.9) | 1 (0.5) | 1 (3.8) | 0.220 | 2/224 | |
| Split liver transplantation | 6 (2.7) | 3 (1.5) | 3 (11.5) | 0.022 | 0/224 | |
| Donor-derived infection | 7 (3.1) | 2 (1.0) | 5 (19.2) | <0.001 | 0/224 | |
| High-urgency transplantation | 9 (4.0) | 6 (3.0) | 3 (11.5) | 0.079 | 0/224 | |
| Postoperative risk factors | ||||||
| Bile leak | 34 (15.2) | 22 (11.2) | 12 (46.2) | <0.001 | 1/224 | |
| Choledochojejunostomy, secondary | 9 (4.0) | 4 (2.0) | 5 (19.2) | 0.001 | 1/224 | |
| Relaparotomy, any reason | 77 (34.4) | 57 (28.8) | 20 (76.9) | <0.001 | 1/224 | |
| Relaparotomy, bile leak related | 29 (12.9) | 19 (9.6) | 10 (38.5) | <0.001 | 1/224 | |
| Relaparotomy, not bile leak related | 48 (21.4) | 38 (19.2) | 10 (38.5) | 0.039 | 1/224 | |
| Early re-transplantation | 6 (2.7) | 2 (1.0) | 4 (15.4) | 0.002 | 0/224 | |
| Posttransplant dialysis | 99 (44.2) | 80 (40.4) | 19 (73.1) | 0.003 | 0/224 | |
| CMV viremia | 64 (28.6) | 54 (27.3) | 10 (38.5) | 0.252 | 0/224 | |
| Nondependent Variable | B-Coefficient | p-Value | HR | 95% CI | Multivariate Analysis | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | HR (95% CI) | p-Value | |||||
| Age (years) | −0.039 | 0.007 | 0.96 | 0.94 | 0.99 | 0.97 (0.94; 0.99) | 0.027 | |
| Sex (male) | 0.427 | 0.315 | 1.53 | 0.67 | 3.53 | |||
| Height (cm) | 0.015 | 0.523 | 1.02 | 0.97 | 1.06 | |||
| Weight (kg) | −0.006 | 0.626 | 0.99 | 0.97 | 1.02 | |||
| Body mass index (kg/m2) | −0.042 | 0.319 | 0.96 | 0.88 | 1.04 | |||
| SAPS III score | 0.015 | 0.556 | 1.02 | 0.97 | 1.07 | |||
| MELD score | 0.036 | 0.110 | 1.04 | 0.99 | 1.08 | |||
| Charlson comorbidity index | 0.046 | 0.580 | 1.05 | 0.89 | 1.23 | |||
| Underlying disease malignancy and other tumors (reference category) | ||||||||
| Alcoholic liver disease | 0.040 | 0.939 | 1.04 | 0.371 | 2.925 | |||
| Virus related | 0.041 | 0.969 | 1.04 | 0.132 | 8.224 | |||
| Non-alcoholic fatty liver disease | - | - | - | - | - | |||
| Budd-Chiari syndrome | - | - | - | - | - | |||
| Acute liver failure | 1.337 | 0.051 | 3.81 | 1.030 | 14.079 | |||
| Cholestatic | 0.593 | 0.374 | 1.81 | 0.490 | 6.683 | |||
| Autoimmune hepatitis | 0.961 | 0.219 | 2.61 | 0.565 | 12.104 | |||
| Metabolic Liver Disease | 0.137 | 0.897 | 1.15 | 0.145 | 9.051 | |||
| Other | 1.986 | 0.060 | 7.28 | 0.920 | 57.692 | |||
| Preoperative risk factors | ||||||||
| MELD Score > 30 | 0.767 | 0.158 | 2.15 | 0.74 | 6.25 | |||
| Fungal colonization at baseline | 1.293 | 0.009 | 3.65 | 1.37 | 9.67 | 1.75 (0.61; 5.04) | 0.300 | |
| Anti-infective pretreatment | 0.519 | 0.297 | 1.68 | 0.63 | 4.46 | |||
| Pretransplant serum creatinine > 2 mg/dL | −0.223 | 0.762 | 0.80 | 0.19 | 3.39 | |||
| Operative risk factors | ||||||||
| Choledochojejunostomy, primary | 0.983 | 0.071 | 2.67 | 0.92 | 7.76 | |||
| Transplantation time > 11 h | −3.022 | 0.678 | 0.05 | 0.00 | 77.12 | |||
| Intraoperative blood transfusion > 40 PRBC | 2.211 | 0.031 | 9.12 | 1.22 | 68.19 | 24.08 (2.72; 213.01) | 0.004 | |
| Split liver transplantation | 1.779 | 0.004 | 5.93 | 1.77 | 19.81 | 5.18 (1.40; 19.16) | 0.014 | |
| Donor-derived infection | 2.657 | <0.001 | 14.25 | 5.34 | 38.01 | 9.70 (3.24; 29.04) | <0.001 | |
| High-urgency transplantation | 1.406 | 0.022 | 4.08 | 1.22 | 13.60 | 1.72 (0.43; 6.95) | 0.448 | |
| Postoperative risk factors | ||||||||
| Bile leak | 1.690 | <0.001 | 5.42 | 2.50 | 11.73 | |||
| Relaparotomy, any reason | 1.960 | <0.001 | 7.10 | 2.85 | 17.69 | 4.62 (1.67; 12.77) | 0.003 | |
| Early re-transplantation | 1.156 | <0.001 | 3.18 | 1.86 | 5.42 | |||
| Posttransplant dialysis | 1.312 | 0.003 | 3.71 | 1.56 | 8.84 | 1.83 (0.69; 4.87) | 0.224 | |
| CMV viremia | 0.488 | 0.226 | 1.63 | 0.74 | 3.59 | |||
| Year | Transplantations (n = 224) | IFI% (95% CI) |
|---|---|---|
| 2017 | 54 | 18.5 (10.4–30.8) |
| 2018 | 70 | 4.3 (1.5–11.9) |
| 2019 | 46 | 4.4 (1.2–14.5) |
| 2020 | 54 | 20.4 (11.8–32.9) |
| Entity of Invasive Candidiasis | Number of Patients (%) | Comment | |
|---|---|---|---|
| Proven infections | 15 (71) | ||
| Candidemia without deep-seated candidiasis | 3 (14) | All catheter-associated | |
| Candidemia with deep-seated candidiasis | 5 (24) | ||
| Deep-seated candidiasis without candidemia | 7 (33) | ||
| Probable infections | Recovery of Candida spp. in an intra-abdominal specimen obtained surgically or within 24 h from external drainage | ||
| Deep-seated candidiasis without candidemia | 6 (29) | ||
| Diagnostic Criteria | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Patient | Histopathologic Examination | Clinical Symptoms | Radiological Abnormalities | Culture | Galactomannan in BALF | PCR in Blood and BALF | Fungal Co-Infection | Time to Diagnosis (Day) | Time of Death (Day) |
| 1 | ● | ● | ● | Candida dubliensis | 43 | 57 | |||
| 2 | ● | ● | ● | ● | Candida orthopsilosis *, Candida krusei *, Mucor circinelloides | 78 | 110 | ||
| 3 | ● | ● | ● | Candida glabrata | 36 | 43 | |||
| 4 | ● | ● | ● | ● | ● | Fusarium spp., Penicillium spp. | 26 | 29 | |
| 5 | ● | ● | ● | ● | ● | ● | - | 9 | 15 |
| Time from Transplantation | |||
|---|---|---|---|
| Pathogen | Less than 14 Days (n = 14) | 15–30 Days (n = 4) | 31–90 Days (n = 8) |
| Candida spp. | 6 (43) | 2 (50) | 1 (13) |
| Non-albicans | 6 (43) | 1 (25) | 3 (38) |
| Aspergillus fumigatus | 1 (7) | 1 (25) | 3 (38) |
| Other | 1 (7) | - | 1 (13) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breitkopf, R.; Treml, B.; Simmet, K.; Bukumirić, Z.; Fodor, M.; Senoner, T.; Rajsic, S. Incidence of Invasive Fungal Infections in Liver Transplant Recipients under Targeted Echinocandin Prophylaxis. J. Clin. Med. 2023, 12, 1520. https://doi.org/10.3390/jcm12041520
Breitkopf R, Treml B, Simmet K, Bukumirić Z, Fodor M, Senoner T, Rajsic S. Incidence of Invasive Fungal Infections in Liver Transplant Recipients under Targeted Echinocandin Prophylaxis. Journal of Clinical Medicine. 2023; 12(4):1520. https://doi.org/10.3390/jcm12041520
Chicago/Turabian StyleBreitkopf, Robert, Benedikt Treml, Katharina Simmet, Zoran Bukumirić, Margot Fodor, Thomas Senoner, and Sasa Rajsic. 2023. "Incidence of Invasive Fungal Infections in Liver Transplant Recipients under Targeted Echinocandin Prophylaxis" Journal of Clinical Medicine 12, no. 4: 1520. https://doi.org/10.3390/jcm12041520