
Effect of Helicobacter pylori Eradication Treatment on Metachronous Gastric Neoplasm Prevention Following Endoscopic Submucosal Dissection for Gastric Adenoma
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
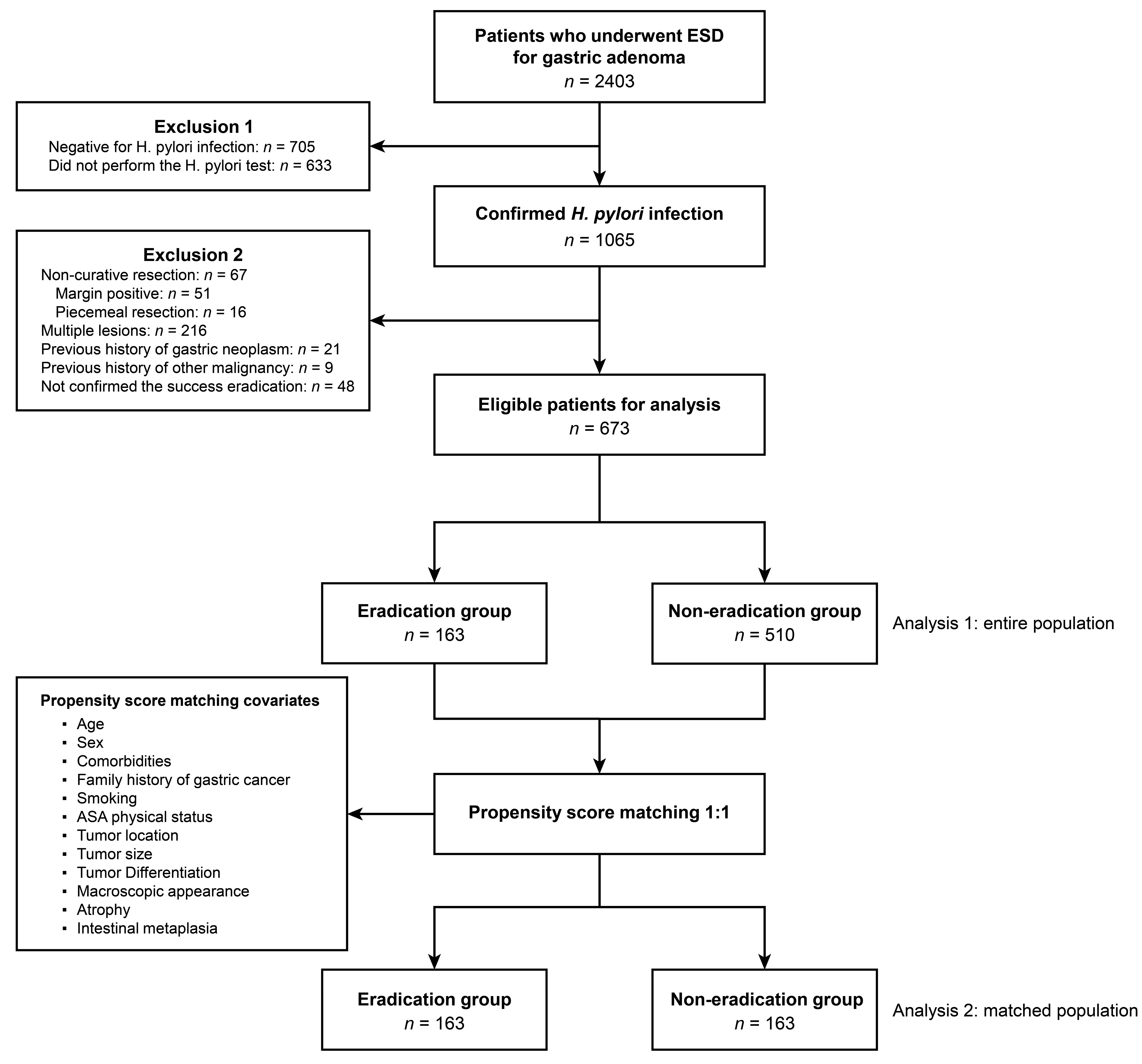
2.1. Study Design and Patients
2.2. Endoscopic Submucosal Dissection
2.3. Tumor Evaluation and Variable Definition
2.4. Confirmation of H. pylori Infection and Eradication Treatment
2.5. Follow-Up Schedules after ESD
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Eradication and Non-Eradication Groups
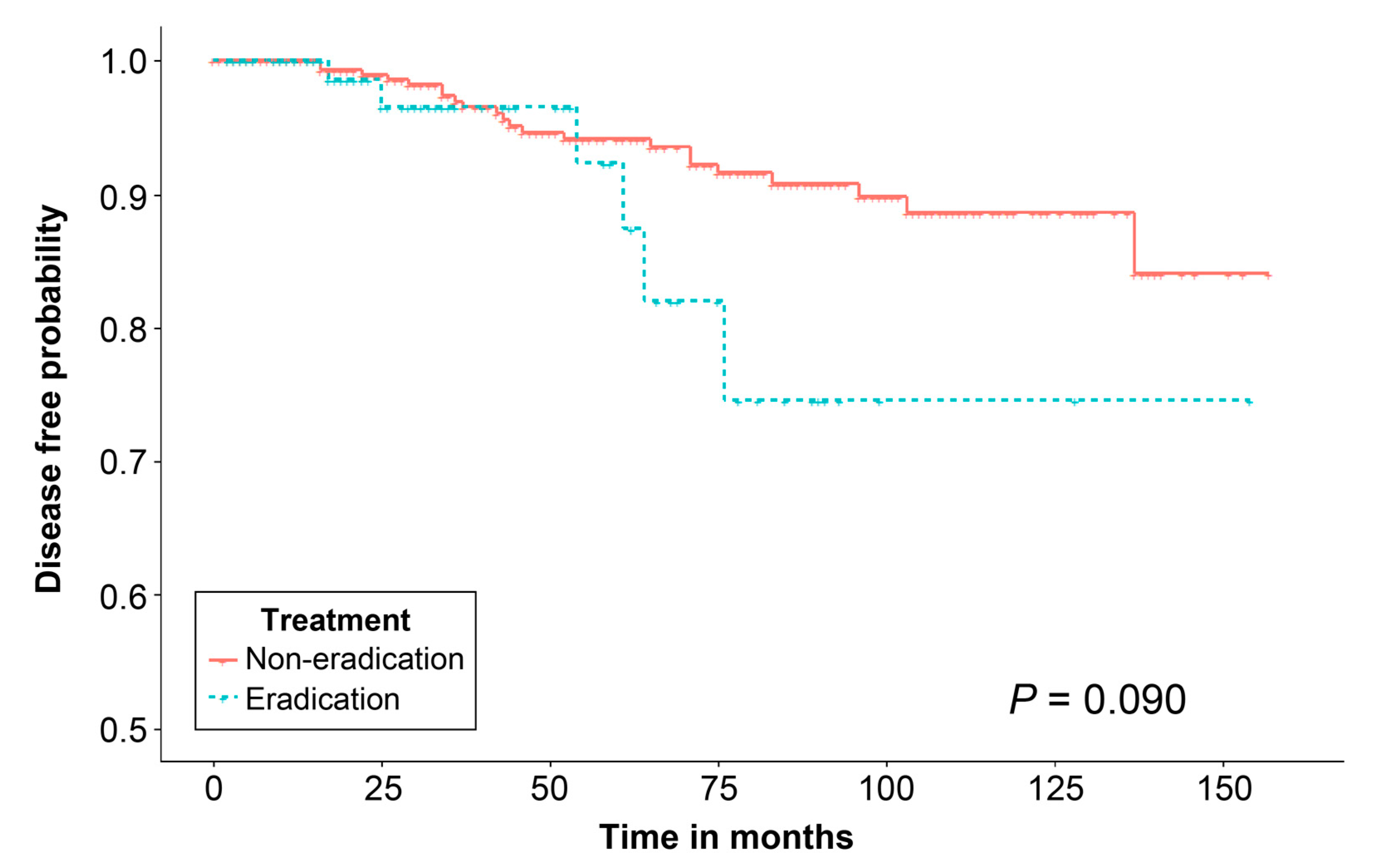
3.2. Metachronous Gastric Neoplasm after ESD and Risk Factors Associated with Metachronous Gastric Neoplasm
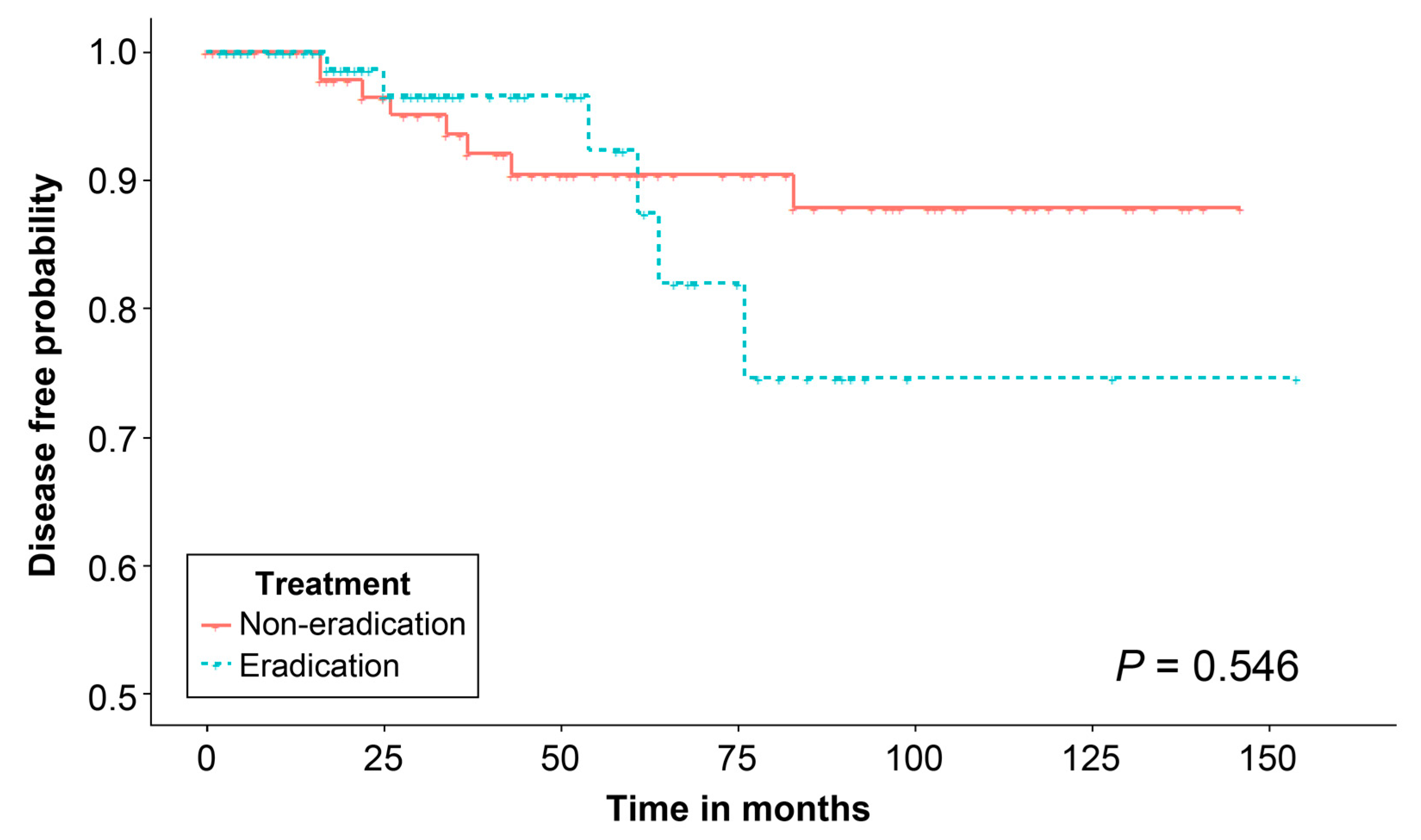
3.3. Effect of H. pylori Eradication Treatment on Propensity Score-Matched Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IARC. Schistosomes, Liver Flukes and Helicobacter pylori; IARC: Lyon, France, 1994; Volume 61, pp. 1–241. [Google Scholar]
- Parsonnet, J.; Friedman, G.D.; Vandersteen, D.P.; Chang, Y.; Vogelman, J.H.; Orentreich, N.; Sibley, R.K. Helicobacter pylori infection and the risk of gastric carcinoma. N. Engl. J. Med. 1991, 325, 1127–1131. [Google Scholar] [CrossRef] [PubMed]
- Sugano, K. Effect of Helicobacter pylori eradication on the incidence of gastric cancer: A systematic review and meta-analysis. Gastric Cancer 2019, 22, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Matsuzaki, J. Gastric cancer: Evidence boosts Helicobacter pylori eradication. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P. Helicobacter pylori treatment for gastric cancer prevention. N. Engl. J. Med. 2018, 378, 1154–1156. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer: Systematic review and meta-analysis. Gut 2020, 69, 2113–2121. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-J.; Choi, I.J.; Kook, M.-C.; Nam, B.-H.; Kim, C.G.; Lee, J.Y.; Ryu, K.W.; Kim, Y.-W. Staging of intestinal- and diffuse-type gastric cancers with the OLGA and OLGIM staging systems. Aliment. Pharmacol. Ther. 2013, 38, 1292–1302. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.; Lin, S.R.; Ching, J.Y.; Zhou, L.Y.; To, K.F.; Wang, R.T.; Leung, W.K.; Enders, K.W.; Lau, J.Y.; Lee, Y.T.; et al. Atrophy and intestinal metaplasia one year after cure of H. pylori infection: A prospective, randomized study. Gastroenterology 2000, 119, 7–14. [Google Scholar] [CrossRef]
- Leung, W.K.; Lin, S.R.; Ching, J.Y.L.; To, K.F.; Ng, E.K.W.; Chan, F.K.L.; Lau, J.Y.W.; Sung, J.J.Y. Factors predicting progression of gastric intestinal metaplasia: Results of a randomised trial on Helicobacter pylori eradication. Gut 2004, 53, 1244–1249. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.-M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef]
- Suerbaum, S.; Michetti, P. Helicobacter pylori infection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Correa, P. Helicobacter pylori and gastric carcinogenesis. Am. J. Surg. Pathol. 1995, 19 (Suppl. S1), S37–S43. [Google Scholar] [PubMed]
- Li, W.-Q.; Ma, J.-L.; Zhang, L.; Brown, L.M.; Li, J.-Y.; Shen, L.; Pan, K.-F.; Liu, W.-D.; Hu, Y.; Han, Z.-X.; et al. Effects of Helicobacter pylori treatment on gastric cancer incidence and mortality in subgroups. J. Natl. Cancer Inst. 2014, 106, dju116. [Google Scholar] [CrossRef]
- Wang, J.; Xu, L.; Shi, R.; Huang, X.; Li, S.W.H.; Huang, Z.; Zhang, G. Gastric atrophy and intestinal metaplasia before and after Helicobacter pylori eradication: A meta-analysis. Digestion 2011, 83, 253–260. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libânio, D.; Bastiaansen, B.A.J.; Bhandari, P.; Bisschops, R.; Bourke, M.J.; Esposito, G.; Lemmers, A.; Maselli, R.; Messmann, H.; et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline–Update 2022. Endoscopy 2022, 54, 591–622. [Google Scholar] [CrossRef]
- Lauwers, G.Y.; Riddell, R.H. Gastric epithelial dysplasia. Gut 1999, 45, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Correa, P. A human model of gastric carcinogenesis. Cancer Res. 1988, 48, 3554–3560. [Google Scholar]
- Choi, I.J.; Kook, M.-C.; Kim, Y.-I.; Cho, S.-J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.-H. Helicobacter pylori therapy for the prevention of metachronous gastric cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef]
- Song, J.H.; Yang, S.Y.; Lim, J.H.; Choi, J.M.; Kim, S.G. The effect of Helicobacter pylori eradication on the metachronous neoplasm after endoscopic resection for gastric dysplasia. Korean J. Gastroenterol. 2017, 70, 27–32. [Google Scholar] [CrossRef]
- Chon, I.; Choi, C.; Shin, C.M.; Park, Y.S.; Kim, N.; Lee, D.H. Effect of Helicobacter pylori eradication on subsequent dysplasia development after endoscopic resection of gastric dysplasia. Korean J. Gastroenterol. 2013, 61, 307–312. [Google Scholar] [CrossRef]
- Shin, S.H.; Jung, D.H.; Kim, J.-H.; Chung, H.S.; Park, J.C.; Shin, S.K.; Kil Lee, S.; Lee, Y.C. Helicobacter pylori eradication prevents metachronous gastric neoplasms after endoscopic resection of gastric dysplasia. PLoS ONE 2015, 10, e0143257. [Google Scholar] [CrossRef]
- Kato, M.; Nishida, T.; Yamamoto, K.; Hayashi, S.; Kitamura, S.; Yabuta, T.; Yoshio, T.; Nakamura, T.; Komori, M.; Kawai, N.; et al. Scheduled endoscopic surveillance controls secondary cancer after curative endoscopic resection for early gastric cancer: A multicentre retrospective cohort study by Osaka University ESD study group. Gut 2013, 62, 1425–1432. [Google Scholar] [CrossRef]
- Dixon, M.F. Gastrointestinal epithelial neoplasia: Vienna revisited. Gut 2002, 51, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C.; Korean College of Helicobacter and Upper Gastrointestinal Research. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J. Gastroenterol. Hepatol. 2014, 29, 1371–1386. [Google Scholar] [CrossRef] [PubMed]
- Conteduca, V.; Sansonno, D.; Lauletta, G.; Russi, S.; Ingravallo, G.; Dammacco, F.H. pylori infection and gastric cancer: State of the art (review). Int. J. Oncol. 2013, 42, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef]
- Choi, J.M.; Kim, S.G.; Choi, J.; Park, J.Y.; Oh, S.; Yang, H.J.; Lim, J.H.; Im, J.P.; Kim, J.S.; Jung, H.C. Effects of Helicobacter pylori eradication for metachronous gastric cancer prevention: A randomized controlled trial. Gastrointest. Endosc. 2018, 88, 475–485.e2. [Google Scholar] [CrossRef] [PubMed]
- Correa, P. Human gastric carcinogenesis: A multistep and multifactorial process—First American Cancer Society award lecture on cancer epidemiology and prevention. Cancer Res. 1992, 52, 6735–6740. [Google Scholar]
- Rugge, M.; Capelle, L.G.; Cappellesso, R.; Nitti, D.; Kuipers, E.J. Precancerous lesions in the stomach: From biology to clinical patient management. Best Pract. Res. Clin. Gastroenterol. 2013, 27, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Parsonnet, J.; Harris, R.A.; Hack, H.M.; Owens, D.K. Modelling cost-effectiveness of Helicobacter pylori screening to prevent gastric cancer: A mandate for clinical trials. Lancet 1996, 348, 150–154. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chen, T.H.H.; Chiu, H.M.; Shun, C.T.; Chiang, H.; Liu, T.Y.; Wu, M.S.; Lin, J.T. The benefit of mass eradication of Helicobacter pylori infection: A community-based study of gastric cancer prevention. Gut 2013, 62, 676–682. [Google Scholar] [CrossRef]
- Ford, A.C.; Forman, D.; Hunt, R.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication for the prevention of gastric neoplasia. Cochrane Database Syst. Rev. 2015, 2015, CD005583. [Google Scholar] [PubMed]
- Ford, A.C.; Forman, D.; Hunt, R.H.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer in healthy asymptomatic infected individuals: Systematic review and meta-analysis of randomised controlled trials. BMJ 2014, 348, g3174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.N.; Wang, Z.; Li, X.; Zhou, Z.G. Helicobacter pylori eradication cannot reduce the risk of gastric cancer in patients with intestinal metaplasia and dysplasia: Evidence from a meta-analysis. Gastric Cancer 2016, 19, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Rokkas, T.; Rokka, A.; Portincasa, P. A systematic review and meta-analysis of the role of Helicobacter pylori eradication in preventing gastric cancer. Ann. Gastroenterol. 2017, 30, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Yanaoka, K.; Oka, M.; Ohata, H.; Yoshimura, N.; Deguchi, H.; Mukoubayashi, C.; Enomoto, S.; Inoue, I.; Iguchi, M.; Maekita, T.; et al. Eradication of Helicobacter pylori prevents cancer development in subjects with mild gastric atrophy identified by serum pepsinogen levels. Int. J. Cancer 2009, 125, 2697–2703. [Google Scholar] [CrossRef] [PubMed]
- Kawanaka, M.; Watari, J.; Kamiya, N.; Yamasaki, T.; Kondo, T.; Toyoshima, F.; Ikehara, H.; Tomita, T.; Oshima, T.; Fukui, H.; et al. Effects of Helicobacter pylori eradication on the development of metachronous gastric cancer after endoscopic treatment: Analysis of molecular alterations by a randomised controlled trial. Br. J. Cancer 2016, 114, 21–29. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.G.; Yoon, H.; Im, J.P.; Kim, J.S.; Kim, W.H.; Jung, H.C. Eradication of Helicobacter pylori after endoscopic resection of gastric tumors does not reduce incidence of metachronous gastric carcinoma. Clin. Gastroenterol. Hepatol. 2014, 12, 793–800.e1. [Google Scholar] [CrossRef]
- Choi, H.S.; Park, D.I.; Hwang, S.J.; Park, J.S.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I. Double-dose, new-generation proton pump inhibitors do not improve Helicobacter pylori eradication rate. Helicobacter 2007, 12, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-W.; Han, J.P.; Kim, K.O.; Kim, S.Y.; Hong, S.J.; Kim, T.H.; Kim, C.W.; Kim, J.S.; Kim, B.-W.; Bang, B.W.; et al. Ten-day empirical sequential or concomitant therapy is more effective than triple therapy for Helicobacter pylori eradication: A multicenter, prospective study. Dig. Liver Dis. 2016, 48, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, N.; Kim, S.E.; Jo, H.J.; Shin, C.M.; Lee, S.H.; Park, Y.S.; Hwang, J.-H.; Kim, J.-W.; Jeong, S.-H.; et al. Long-term follow-up Helicobacter pylori reinfection rate and its associated factors in Korea. Helicobacter 2013, 18, 135–142. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Parameter | Total (n = 673) | Eradication (n = 163) | Non-Eradication (n = 510) | p-Value |
|---|---|---|---|---|
| Age, years, mean ± SD | 61.6 ± 9.7 | 60.9 ± 9.2 | 61.9 ± 9.8 | 0.284 |
| Male, n (%) | 465 (69.1) | 110 (67.5) | 355 (69.6) | 0.627 |
| Familial history of gastric cancer, n (%) | 0.279 | |||
| Yes | 63 (9.4) | 19 (11.7) | 44 (8.6) | |
| No | 610 (90.6) | 144 (88.3) | 466 (91.4) | |
| Smoking, n (%) | 0.020 | |||
| Yes | 251 (37.3) | 48 (29.4) | 203 (39.8) | |
| No | 422 (62.7) | 115 (70.6) | 307 (60.2) | |
| Alcohol drinker, n (%) | 0.352 | |||
| Yes | 250 (37.1) | 66 (40.5) | 184 (36.1) | |
| No | 423 (62.9) | 97 (59.5) | 326 (63.9) | |
| ASA physical status, n (%) | 0.626 | |||
| ASA 1 | 563 (83.7) | 134 (82.2) | 429 (84.1) | |
| ASA 2 | 110 (16.3) | 29 (17.8) | 81 (15.9) | |
| Lesion size, mm, mean ± SD | 11.7 ± 7.8 | 12.1 ± 7.6 | 11.6 ± 7.9 | 0.446 |
| Gross morphology type, n (%) | 0.001 | |||
| Elevated | 338 (50.2) | 62 (38.0) | 276 (54.1) | |
| Flat | 216 (32.1) | 60 (36.8) | 156 (30.6) | |
| Depressed | 119 (17.7) | 41 (25.2) | 78 (15.3) | |
| Tumor Location, n (%) | 0.486 | |||
| Upper 1/3 | 96 (14.3) | 19 (11.7) | 77 (15.1) | |
| Middle 1/3 | 293 (43.5) | 76 (46.6) | 217 (42.5) | |
| Lower 1/3 | 284 (42.2) | 68 (51.0) | 216 (42.4) | |
| Pathology, n (%) | 0.035 | |||
| Low-grade dysplasia | 567 (84.2) | 146 (90.8) | 421 (82.5) | |
| High-grade dysplasia | 106 (15.8) | 17 (10.4) | 89 (17.5) | |
| Atrophic gastritis, n (%) | 0.113 | |||
| Yes | 583 (86.6) | 135 (82.8) | 448 (87.8) | |
| No | 90 (13.4) | 28 (17.2) | 62 (12.2) | |
| Intestinal metaplasia, n (%) | 0.069 | |||
| Yes | 579 (86.0) | 133 (81.6) | 446 (87.5) | |
| No | 94 (14.0) | 30 (18.4) | 64 (12.5) |
| Variable | Eradication (n = 163) | Non-Eradication (n = 510) | p-Value |
|---|---|---|---|
| Metachronous gastric neoplasm, n (%) | 6 (3.7) | 22 (4.3) | 0.825 |
| Adenoma | 3 (1.8) | 13 (2.5) | 0.773 |
| Pathology | 0.188 | ||
| Low-grade dysplasia | 2 (66.7) | 13 (100) | |
| High-grade dysplasia | 1 (33.3) | 0 (0) | |
| Cancer | 3 (1.8) | 9 (1.8) | 1.000 |
| Pathology | 1.000 | ||
| Differentiated | 2 (66.7) | 7 (77.8) | |
| Undifferentiated | 1 (33.3) | 2 (22.2) |
| Univariable Analysis | ||
|---|---|---|
| HR (95% CI) | p-Value | |
| Age, years | 1.019 (0.979–1.059) | 0.357 |
| Sex | ||
| Male | Ref. | |
| Female | 0.890 (0.385–2.055) | 0.785 |
| Age group | ||
| 50–54 | 0.310 (0.062–1.556) | 0.155 |
| 55–59 | 1.944 (0.656–5.763) | 0.231 |
| 60–64 | 1.040 (0.310–3.487) | 0.949 |
| 65–69 | 2.045 (0.667–6.274) | 0.211 |
| ≥70 | Ref. | |
| Smoker | 1.722 (0.807–3.673) | 0.160 |
| Alcohol drinker | 0.938 (0.426–2.064) | 0.873 |
| ASA physical status | ||
| ASA 1 | Ref. | |
| ASA 2 | 1.118 (0.416–3.007) | 0.825 |
| Success for Helicobacter pylori infection | ||
| No | Ref. | |
| Yes | 0.848 (0.338–2.128) | 0.725 |
| Lesion size, mm | 1.016 (0.972–1.062) | 0.492 |
| Gross morphology | ||
| Elevated or flat | Ref. | |
| Depressed | 0.547 (0.162–1.843) | 0.331 |
| Tumor location | ||
| Lower third | Ref. | |
| Middle third | 0.920 (0.328–2.583) | 0.875 |
| Upper third | 0.410 (0.166–1.012) | 0.053 |
| Pathology | ||
| Low-grade dysplasia | Ref. | |
| High-grade dysplasia | 0.631 (0.187–2.130) | 0.459 |
| Atrophy | 1.299 (0.384–4.395) | 0.674 |
| Intestinal metaplasia | 1.369 (0.405–4.627) | 0.613 |
| Clinical Parameter | Total (n = 326) | Eradication (n = 163) | Non-Eradication (n = 163) | p-Value | SMD |
|---|---|---|---|---|---|
| Age, years, mean ± SD | 60.9 ± 9.4 | 60.9 ± 9.2 | 60.8 ± 9.6 | 0.921 | 0.011 |
| Male, n (%) | 215 (66.0) | 110 (67.5) | 105 (64.4) | 0.640 | 0.065 |
| Familial history of gastric cancer, n (%) | 0.513 | 0.091 | |||
| Yes | 43 (13.2) | 19 (11.7) | 24 (14.7) | ||
| No | 283 (86.8) | 144 (88.3) | 139 (85.3) | ||
| Smoking, n (%) | 0.810 | 0.040 | |||
| Yes | 99 (30.4) | 48 (29.4) | 51 (31.3) | ||
| No | 227 (69.6) | 115 (70.6) | 112 (68.7) | ||
| Alcohol drinker, n (%) | 0.570 | 0.045 | |||
| Yes | 126 (38.7) | 66 (40.5) | 60 (36.8) | ||
| No | 200 (61.3) | 97 (59.5) | 103 (63.2) | ||
| ASA physical status, n (%) | 0.883 | 0.033 | |||
| ASA 1 | 270 (82.8) | 134 (82.2) | 136 (83.4) | ||
| ASA 2 | 56 (17.2) | 29 (17.8) | 27 (16.6) | ||
| Lesion size, mm, mean ± SD | 12.0 ± 8.2 | 12.1 ± 7.6 | 12.0 ± 8.8 | 0.893 | 0.015 |
| Gross morphology type, n (%) | 1.000 | 0.026 | |||
| Elevated | 125 (38.3) | 62 (38.0) | 63 (38.7) | ||
| Flat | 118 (36.2) | 60 (36.8) | 58 (35.6) | ||
| Depressed | 83 (25.5) | 41 (25.2) | 42 (25.8) | ||
| Tumor Location, n (%) | 0.310 | 0.125 | |||
| Upper 1/3 | 33 (10.1) | 19 (11.7) | 14 (8.6) | ||
| Middle 1/3 | 149 (45.7) | 76 (46.6) | 73 (44.8) | ||
| Lower 1/3 | 144 (44.2) | 68 (51.0) | 76 (46.6) | ||
| Pathology, n (%) | 0.853 | 0.041 | |||
| Low-grade dysplasia | 294 (90.2) | 146 (90.8) | 148 (89.6) | ||
| High-grade dysplasia | 32 (9.8) | 17 (10.4) | 15 (9.2) | ||
| Atrophic gastritis, n (%) | 1.000 | 0.016 | |||
| Yes | 269 (82.5) | 135 (82.8) | 134 (82.2) | ||
| No | 57 (17.5) | 28 (17.2) | 29 (17.8) | ||
| Intestinal metaplasia, n (%) | 1.000 | <0.001 | |||
| Yes | 266 (81.6) | 133 (81.6) | 133 (81.6) | ||
| No | 60 (18.4) | 30 (18.4) | 30 (18.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, C.-K.; Lee, E.; Park, B.; Lim, S.G.; Shin, S.J.; Lee, K.M.; Lee, G.H. Effect of Helicobacter pylori Eradication Treatment on Metachronous Gastric Neoplasm Prevention Following Endoscopic Submucosal Dissection for Gastric Adenoma. J. Clin. Med. 2023, 12, 1512. https://doi.org/10.3390/jcm12041512
Noh C-K, Lee E, Park B, Lim SG, Shin SJ, Lee KM, Lee GH. Effect of Helicobacter pylori Eradication Treatment on Metachronous Gastric Neoplasm Prevention Following Endoscopic Submucosal Dissection for Gastric Adenoma. Journal of Clinical Medicine. 2023; 12(4):1512. https://doi.org/10.3390/jcm12041512
Chicago/Turabian StyleNoh, Choong-Kyun, Eunyoung Lee, Bumhee Park, Sun Gyo Lim, Sung Jae Shin, Kee Myung Lee, and Gil Ho Lee. 2023. "Effect of Helicobacter pylori Eradication Treatment on Metachronous Gastric Neoplasm Prevention Following Endoscopic Submucosal Dissection for Gastric Adenoma" Journal of Clinical Medicine 12, no. 4: 1512. https://doi.org/10.3390/jcm12041512