

Response to Peptide Receptor Radionuclide Therapy in Pheocromocytomas and Paragangliomas: A Systematic Review and Meta-Analysis
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
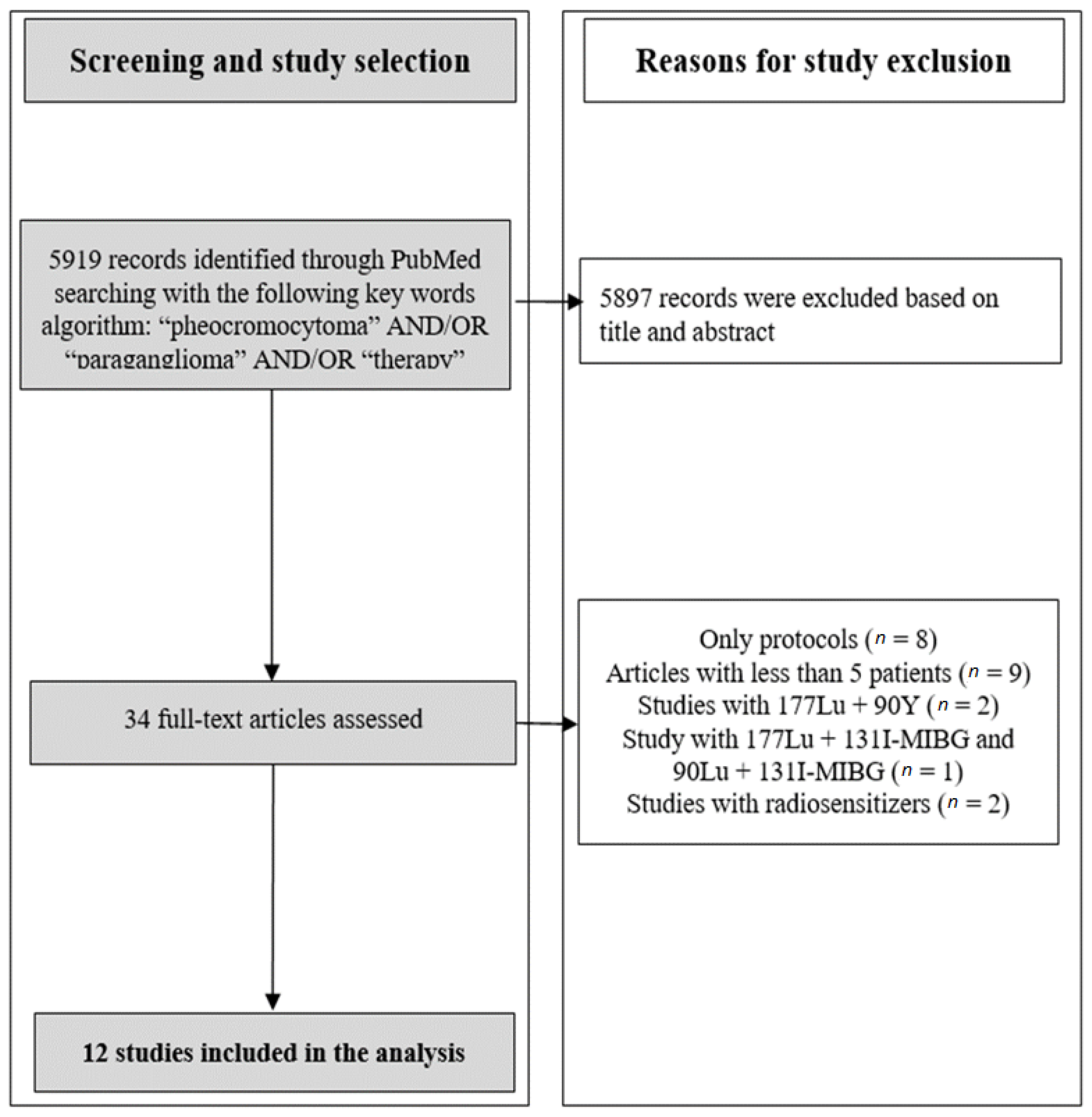
2.1. Search Strategy and Trial Identification Criteria
2.2. Data Extraction
2.3. Studies Quality Rating
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lam, A.K.-Y. Update on Adrenal Tumours in 2017 World Health Organization (WHO) of Endocrine Tumours. Endocr. Pathol. 2017, 28, 213–227. [Google Scholar] [CrossRef] [PubMed]
- Lenders, J.W.; Eisenhofer, G.; Mannelli, M.; Pacak, K. Phaeochromocytoma. Lancet 2005, 366, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Chrisoulidou, A.; Kaltsas, G.; Ilias, I.; Grossman, A.B. The diagnosis and management of malignant phaeochromocytoma and paraganglioma. Endocrine-Related Cancer 2007, 14, 569–585. [Google Scholar] [CrossRef] [PubMed]
- Korevaar, T.I.M.; Grossman, A.B. Pheochromocytomas and paragangliomas: Assessment of malignant potential. Endocrine 2011, 40, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Ilias, I.; Sahdev, A.; Reznek, R.H.; Grossman, A.B.; Pacak, K. The optimal imaging of adrenal tumours: A comparison of different methods. Endocrine-Related Cancer 2007, 14, 587–599. [Google Scholar] [CrossRef]
- Jing, H.; Li, F.; Wang, L.; Wang, Z.; Li, W.; Huo, L.; Zhang, J. Comparison of the 68Ga-DOTATATA PET/CT, FDG PET/CT, and MIBG SPECT/CT in the Evaluation of Suspected Primary Pheochromocytomas and Paragangliomas. Clin. Nucl. Med. 2017, 42, 525–529. [Google Scholar] [CrossRef]
- Taïeb, D.; Hicks, R.J.; Hindié, E.; Guillet, B.A.; Avram, A.; Ghedini, P.; Timmers, H.J.; Scott, A.T.; Elojeimy, S.; Rubello, D.; et al. European Association of Nuclear Medicine Practice Guideline/Society of Nuclear Medicine and Molecular Imaging Procedure Standard 2019 for radionuclide imaging of phaeochromocytoma and paraganglioma. Eur. J. Nucl. Med. 2019, 46, 2112–2137. [Google Scholar] [CrossRef]
- Neumann, H.P.H.; Young, W.F., Jr.; Eng, C. Pheochromocytoma and Paraganglioma. N. Engl. J. Med. 2019, 381, 552–565. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
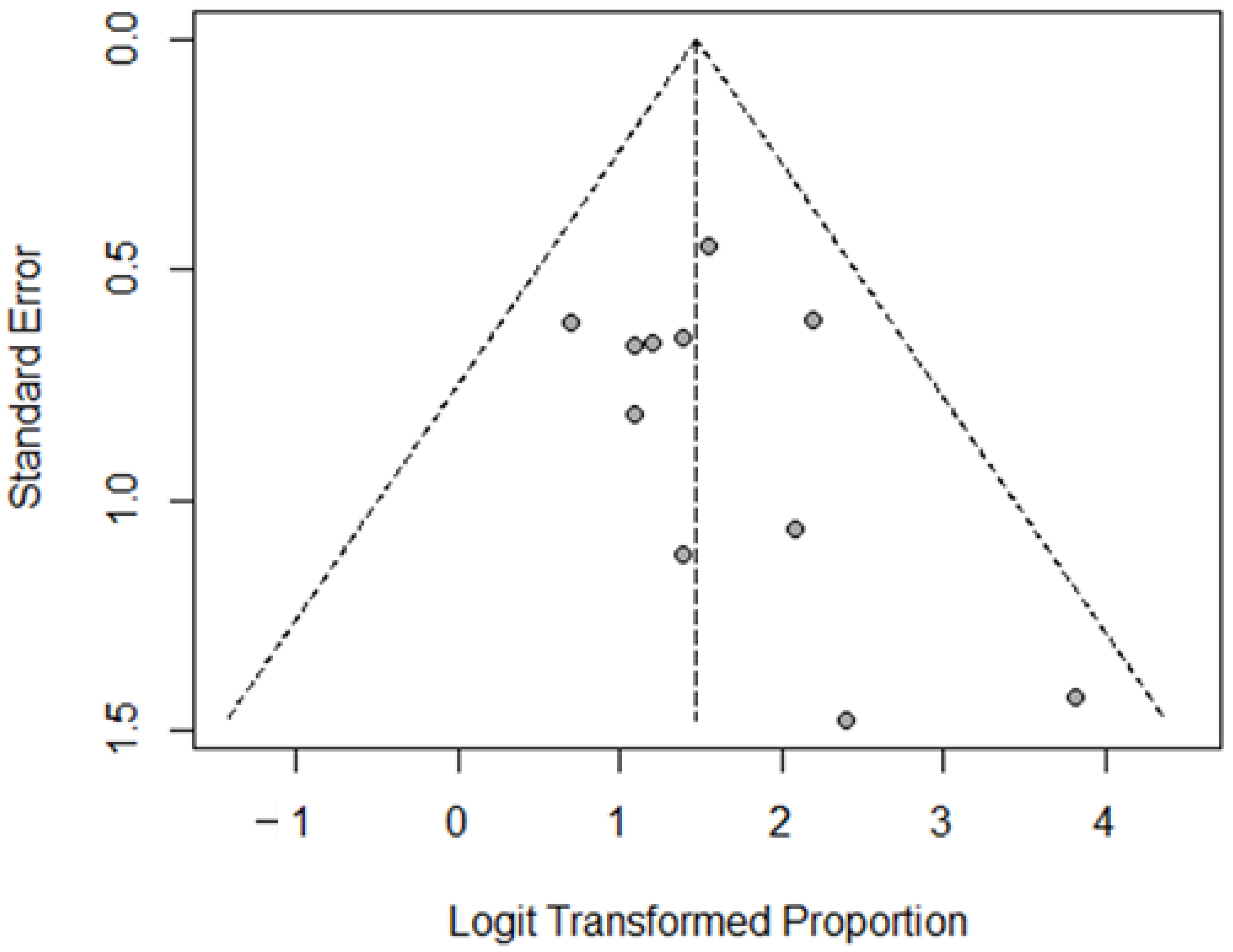
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- van Essen, M.; Krenning, E.P.; Kooij, P.P.; Bakker, W.H.; Feelders, R.A.; de Herder, W.W.; Wolbers, J.G.; Kwekkeboom, D.J. Effects of therapy with [177Lu-DOTA0, Tyr3]octreotate in patients with paraganglioma, meningioma, small cell lung carcinoma, and melanoma. J. Nucl. Med. 2006, 47, 1599–1606. [Google Scholar]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M.A. Response, Survival, and Long-Term Toxicity After Therapy With the Radiolabeled Somatostatin Analogue [90Y-DOTA]-TOC in Metastasized Neuroendocrine Cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef]
- Pinato, D.J.; Black, J.R.M.; Ramaswami, R.; Tan, T.M.; Adjogatse, D.; Sharma, R. Peptide receptor radionuclide therapy for metastatic paragangliomas. Med. Oncol. 2016, 33, 47. [Google Scholar] [CrossRef]
- Hamiditabar, M.; Ali, M.; Roys, J.; Wolin, E.M.; O’Dorisio, T.; Ranganathan, D.; Tworowska, I.; Strosberg, J.R.; Delpassand, E.S. Peptide Receptor Radionuclide Therapy With 177Lu-Octreotate in Patients With Somatostatin Receptor Expressing Neuroendocrine Tumors. Six years assesment. Clin. Nucl. Med. 2017, 42, 436–443. [Google Scholar] [CrossRef]
- Demirci, E.; Kabasakal, L.; Toklu, T.; Ocak, M.; Şahin, O.E.; Alan-Selcuk, N.; Araman, A. 177Lu-DOTATATE therapy in patients with neuroendocrine tumours including high-grade (WHO G3) neuroendocrine tumours. Nucl. Med. Commun. 2018, 39, 789–796. [Google Scholar] [CrossRef]
- Garske-Román, U.; Sandström, M.; Baron, K.F.; Lundin, L.; Hellman, P.; Welin, S.; Johansson, S.; Khan, T.; Lundqvist, H.; Eriksson, B.; et al. Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): Feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur. J. Nucl. Med. 2018, 45, 970–988. [Google Scholar] [CrossRef]
- Zandee, W.T.; Brabander, T.; Blažević, A.; Kam, B.L.R.; Teunissen, J.J.M.; Feelders, R.A.; Hofland, J.; De Herder, W.W. Symptomatic and Radiological Response to 177Lu-DOTATATE for the Treatment of Functioning Pancreatic Neuroendocrine Tumors. J. Clin. Endocrinol. Metab. 2019, 104, 1336–1344. [Google Scholar] [CrossRef]
- Vyakaranam, A.R.; Crona, J.; Norlén, O.; Granberg, D.; Garske-Román, U.; Sandström, M.; Fröss-Baron, K.; Thiis-Evensen, E.; Hellman, P.; Sundin, A. Favorable Outcome in Patients with Pheochromocytoma and Paraganglioma Treated with 177Lu-DOTATATE. Cancers 2019, 11, 909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolasinska-Ćwikła, A.; Pęczkowska, M.; Ćwikła, J.B.; Michałowska, I.; Pałucki, J.M.; Bodei, L.; Lewczuk-Myślicka, A.; Januszewicz, A. A Clinical Efficacy of PRRT in Patients with Advanced, Nonresectable, Paraganglioma-Pheochromocytoma, Related to SDHx Gene Mutation. J. Clin. Med. 2019, 8, 952. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, S.K.; Sarathi, V.; Memon, S.S.; Garg, R.; Malhotra, G.; Verma, P.; Shah, R.; Sehemby, M.K.; Patil, V.A.; Jadhav, S.; et al. 177Lu-DOTATATE therapy in metastatic/inoperable pheochromocytoma-paraganglioma. Endocr. Connect. 2020, 9, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Severi, S.; Bongiovanni, A.; Ferrara, M.; Nicolini, S.; Di Mauro, F.; Sansovini, M.; Lolli, I.; Tardelli, E.; Cittanti, C.; Di Iorio, V.; et al. Peptide receptor radionuclide therapy in patients with metastatic progressive pheochromocytoma and paraganglioma: Long-term toxicity, efficacy and prognostic biomarker data of phase II clinical trials. ESMO Open 2021, 6, 100171. [Google Scholar] [CrossRef]
- Prado-Wohlwend, S.; Bernal-Vergara, J.; Utrera-Costero, A.; Cañón-Sánchez, J.; Agudelo-Cifuentes, M.; Bello-Arques, P. Peptide receptor radionuclide therapy with [177Lu]Lu-DOTA-TATE. Rev. Española De Med. Nucl. E Imagen Mol. 2021, 41, 55–65. [Google Scholar] [CrossRef]
- Satapathy, S.; Mittal, B.R.; Bhansali, A. ‘Peptide receptor radionuclide therapy in the management of advanced pheochromocytoma and paraganglioma: A systematic review and meta-analysis’. Clin. Endocrinol. 2019, 91, 718–727. [Google Scholar] [CrossRef]
- van Hulsteijn, L.T.; Niemeijer, N.D.; Dekkers, O.M.; Corssmit, E.P.M. 131I-MIBG therapy for malignant paraganglioma and phaeochromocytoma: Systematic review and meta-analysis. Clin. Endocrinol. 2013, 80, 487–501. [Google Scholar] [CrossRef]
- Lenders, J.W.M.; Eisenhofer, G. Update on Modern Management of Pheochromocytoma and Paraganglioma. Endocrinol. Metab. 2017, 32, 152–161. [Google Scholar] [CrossRef]
- Niemeijer, N.D.; Alblas, G.; Van Hulsteijn, L.T.; Dekkers, O.M.; Corssmit, E.P.M. Chemotherapy with cyclophosphamide, vincristine and dacarbazine for malignant paraganglioma and pheochromocytoma: Systematic review and meta-analysis. Clin. Endocrinol. 2014, 81, 642–651. [Google Scholar] [CrossRef]
- Jhawar, S.; Arakawa, Y.; Kumar, S.; Varghese, D.; Kim, Y.S.; Roper, N.; Elloumi, F.; Pommier, Y.; Pacak, K.; Del Rivero, J. New Insights on the Genetics of Pheochromocytoma and Paraganglioma and Its Clinical Implications. Cancers 2022, 14, 594. [Google Scholar] [CrossRef]
- Amar, L.; Baudin, E.; Burnichon, N.; Peyrard, S.; Silvera, S.; Bertherat, J.; Bertagna, X.; Schlumberger, M.; Jeunemaitre, X.; Gimenez-Roqueplo, A.-P.; et al. Succinate Dehydrogenase B Gene Mutations Predict Survival in Patients with Malignant Pheochromocytomas or Paragangliomas. J. Clin. Endocrinol. Metab. 2007, 92, 3822–3828. [Google Scholar] [CrossRef]
- O’Kane, G.M.; Ezzat, S.; Joshua, A.; Bourdeau, I.; Leibowitz-Amit, R.; Olney, H.J.; Krzyzanowska, M.; Reuther, D.; Chin, S.; Wang, L.; et al. A phase 2 trial of sunitinib in patients with progressive paraganglioma or pheochromocytoma: The SNIPP trial. Br. J. Cancer 2019, 120, 1113–1119. [Google Scholar] [CrossRef]
- Prinzi, N.; Corti, F.; Torchio, M.; Niger, M.; Antista, M.; Pagani, F.; Beninato, T.; Pulice, I.; Rossi, R.E.; Coppa, J.; et al. Metastatic pheochromocytomas and paragangliomas: Where are we? Tumori J. 2022, 108, 526–540. [Google Scholar] [CrossRef]
- Granberg, D.; Juhlin, C.C.; Falhammar, H. Metastatic Pheochromocytomas and Abdominal Paragangliomas. J. Clin. Endocrinol. Metab. 2021, 106, e1937–e1952. [Google Scholar] [CrossRef]
- Oh, D.Y.; Kim, T.W.; Park, Y.S.; Shin, S.J.; Shin, S.H.; Song, E.-K.; Lee, H.J.; Lee, K.-W.; Bang, Y.-J. Phase 2 study of everolimus monotherapy in patients with non-functioning neuroendocrine tumors or pheochromocytomas/paragangliomas. Cancer 2012, 118, 6162–6170. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Type of Study | No. of Patients | Age, Years Median (Range) | Sex | Sites of Metastases (No. of Patients) | Genetic Characteristics (No. of Patients) | Previous Treatments (No. of Patients) |
|---|---|---|---|---|---|---|---|---|
| van Essen M. [14] | 2006 | retrospective | 12 (1 PCC, 11 PGL) | 39.7 (22–55) | 6 male, 6 female | liver (4), bone (7) | NA | surgery (9), CHT (4), RT (7), naive (2) |
| Imhof A. [15] | 2011 | prospective | 39 (11 PCC, 28 PGL) | 39 | NS | NS | NA | NS |
| Pinato DJ. [16] | 2016 | retrospective | 5 (5 PGL) | 34 (16–47) | 4 male, 1 female | nodes (1), bone (5), lung (1) | SDHB (5) | surgery (4), CHT (1), RT (1), 131I-MIBG (1) |
| Hamiditabar M. [17] | 2017 | prospective | 5 (1PCC, 4 PGL) | NS | NS | NS | NA | NS |
| Demirci E. [18] | 2018 | retrospective | 12 (NS) | NS | NS | NS | NA | NS |
| Garske-Román U. [19] | 2018 | prospective | 5 (2 PCC, 3 PGL) | 60.4 (25–71) | 2 male, 3 female | nodes (2), liver (2), bone (5) | NA | surgery (5) |
| Zandee WT. [20] | 2019 | retrospective | 30 (3 PCC, 27 PGL) | 47 (29–74) | 10 male, 20 female | nodes (10), liver (7), bone (13), lung (6) | SDHB (5), SDHD (11), familiar (2), sporadic (5), unknown (7) | surgery (19), CHT (5), RT (6), 131I-MIBG (3), SSA (2) |
| Vyakaranam AR. [21] | 2019 | retrospective | 22 (9 PCC + 13 PGL) | 60 (24–80) | 13 male, 9 female | nodes (7), liver (9), bone (17), lung (4) | sporadic (4), SDHB (4), SDHD (2), SDHA (1), NF1 (2), unknown (9) | surgery (16), CHT (1), RT (14), 131I-MIBG (6), naive (1) |
| Kolasinska-Ćwikła A. [22] | 2019 | prospective | 13 (4 PCC + 9 PGL) | 41.8 (27–62) | 8 male, 5 female | liver (6), bone (9) | SDHB (5), SDHD (8) | surgery (13), SSA (8) |
| Jaiswal SK. [23] | 2020 | retrospective | 15 (5 PCC + 10 PGL) | 32.5 | 7 male, 8 female | nodes (3), liver (4), bone (6), lung (3) | VHL (2), SDHB (1), SDHD (1), negative (1), unknown (10) | surgery (10), RT (3) |
| Severi S. [24] | 2021 | retrospective | 46 (NS) | 52 | 20 male, 26 female | liver (8), bone (19) | wildtype (10), SDHD or SDHB (20) | NS |
| Prado-Wohlwend S. [25] | 2022 | retrospective | 9 (3 PCC + 6 PGL) | 45.8 (20–72) | 4 male, 5 female | nodes (6), liver (3), bone (8), lung (3) | SDHD (1)—SDHB (3)—NF1 (1)—sporadic (4) | CHT (3), RT (3), 131I-MIBG (2), SSA (8), naive (1) |
| Author (First Name) | Year | PRRT Agent | Treatment Characteristics | No. of Cycles | Response Criteria | Best Response to PRRT (Radiologically Assessed Patients) | Haematological Toxicity Grades 3/4 (No. of Patients) |
|---|---|---|---|---|---|---|---|
| van Essen M. [14] | 2006 | 177Lu | 7.4 GBq per cycle | NS | SWOG | PR (2), SD (6) | thrombocytopenia and anemia (2) |
| Imhof A. [15] | 2011 | 90Y | 3.7 GBq/mq per cycle | 2 (1–10) | RECIST 1.0 | PR (7) * | NS |
| Pinato DJ. [16] | 2016 | 177Lu | 6.6–7.6 GBq per cycle | 3 | NS | PR (1), SD (3) | none |
| Hamiditabar M. [17] | 2017 | 177Lu | 7.4 GBq per cycle | NS | RECIST 1.1 | SD (4) | NS |
| Demirci E. [18] | 2018 | 177Lu | 3.7–8.1 GBq per cycle | at least 3 cycles | RECIST 1.1 | PR (4), SD (2) | NS |
| Garske-Román U. [19] | 2018 | 177Lu | 7.4 GBq per cycle | NS | RECIST 1.1 | SD (5) | NS |
| Zandee WT. [20] | 2019 | 177Lu | 7.4 GBq per cycle | 73% of patients received 4 cycles | RECIST 1.1 | PR (7), SD (20) | anemia (2), thrombocytopenia (5), leukopenia (3) |
| Vyakaranam AR. [21] | 2019 | 177Lu | 7.4 GBq per cycle | 4.9 | RECIST 1.1 | PR (2), SD (20) | no |
| Kolasinska-Ćwikła A. [22] | 2019 | 90Y | 3.4 GBq per cycle | NS (61% of patients received 2 cycles) | RECIST 1.0 | PR (1), SD (9) | anemia (2) |
| Jaiswal SK. [23] | 2020 | 177Lu | NS | 4.13 | RECIST 1.1 | PR (1), SD (11) | none |
| Severi S. [24] | 2021 | 177Lu (34) and 90Y- (12) | 177Lu: 3.7–5.5 GBq per cycle 90Y: 1.1–1.85 GBq per cycle | 5 | RECIST 1.1 | 177Lu: PR (3), SD (25) 90Y: PR (1), SD (8) | none |
| Prado-Wohlwend S. [25] | 2022 | 177Lu | 8.01 (7.4–8.4) GBq per cycle | 3.11 | RECIST 1.1 | PR (2), SD (6) | NS |
| Author | Year | Accrual Time | MINORS Score | Newcastle Ottawa Scale Score | |||
|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome | Total | ||||
| van Essen M. [14] | 2006 | NS | 7 | 3 | 0 | 3 | 6 |
| Imhof A. [15] | 2011 | 1997–2010 | 10 | 3 | 1 | 3 | 7 |
| Pinato DJ. [16] | 2016 | 2008–2014 | 9 | 3 | 0 | 3 | 6 |
| Hamiditabar M. [17] | 2017 | 2010–2016 | 8 | 3 | 0 | 3 | 6 |
| Demirci E. [18] | 2018 | 2010–2015 | 8 | 3 | 0 | 3 | 6 |
| Garske-Román U. [19] | 2018 | 2010–2014 | 8 | 3 | 1 | 3 | 7 |
| Zandee WT. [20] | 2019 | 2000–NS | 10 | 3 | 1 | 3 | 7 |
| Vyakaranam AR. [21] | 2019 | 2005–2018 | 10 | 3 | 1 | 3 | 7 |
| Kolasinska-Ćwikła A. [22] | 2019 | 2006–2018 | 11 | 3 | 2 | 3 | 8 |
| Jaiswal SK. [23] | 2020 | 2010–2019 | 8 | 3 | 1 | 3 | 7 |
| Severi S. [24] | 2021 | 2008–2018 | 10 | 3 | 2 | 3 | 8 |
| Prado-Wohlwend S. [25] | 2022 | 2014–2021 | 9 | 3 | 1 | 3 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marretta, A.L.; Ottaiano, A.; Iervolino, D.; Bracigliano, A.; Clemente, O.; Di Gennaro, F.; Tafuto, R.; Santorsola, M.; Lastoria, S.; Tafuto, S. Response to Peptide Receptor Radionuclide Therapy in Pheocromocytomas and Paragangliomas: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1494. https://doi.org/10.3390/jcm12041494
Marretta AL, Ottaiano A, Iervolino D, Bracigliano A, Clemente O, Di Gennaro F, Tafuto R, Santorsola M, Lastoria S, Tafuto S. Response to Peptide Receptor Radionuclide Therapy in Pheocromocytomas and Paragangliomas: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(4):1494. https://doi.org/10.3390/jcm12041494
Chicago/Turabian StyleMarretta, Antonella Lucia, Alessandro Ottaiano, Domenico Iervolino, Alessandra Bracigliano, Ottavia Clemente, Francesca Di Gennaro, Roberto Tafuto, Mariachiara Santorsola, Secondo Lastoria, and Salvatore Tafuto. 2023. "Response to Peptide Receptor Radionuclide Therapy in Pheocromocytomas and Paragangliomas: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 4: 1494. https://doi.org/10.3390/jcm12041494