
Guided Dental Implant Surgery: Systematic Review
 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Information Sources, Search
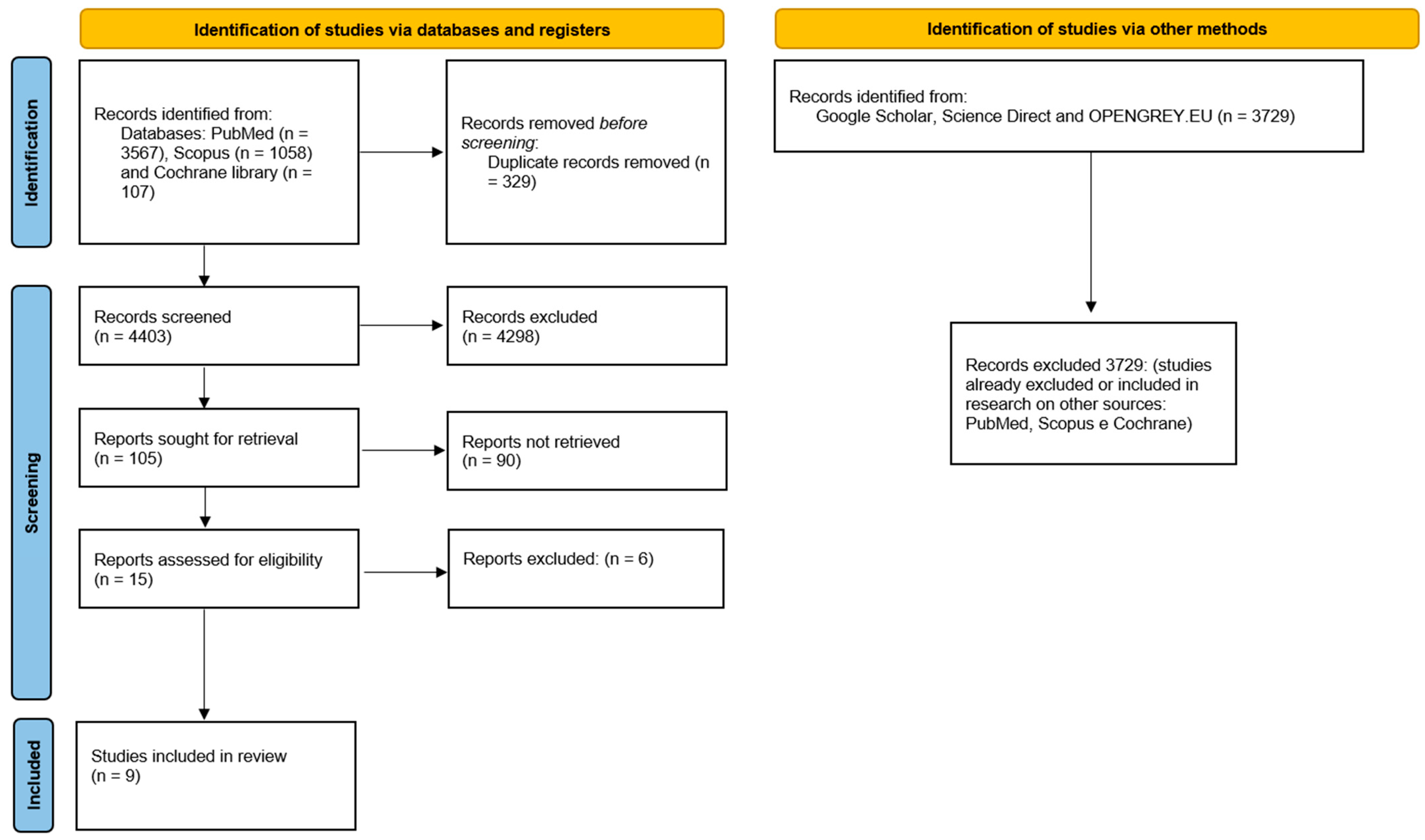
2.3. Selection of Studies
2.4. Data Extraction
2.5. Risk of Bias
3. Results
- ✓
- ✓
- ✓
- Intraoperative (surgery) complications, such as the impossibility of using a drill due to limited opening of the mouth of a patient, buccal bone dehiscence after osteotomy in another patient (both cases in the study by Derksen et al., 2019 [17]), insufficient bone quantity in one patient, and insufficient primary stability in three patients (Vogl et al., 2015 [20]; these cases were not considered in the study statistics, thus resulting in a 100% survival rate).
- ✓
- Postoperative, (prosthetic implant complications) include loss of implants in almost all studies, loosening of the abutment screw in 2 cases in the study by Lopes et al., 2015 [7], in 3 cases in the study by Vogl et al., 2015 [20], in 10 cases in the study by Yamada et al., 2015 [21]; fracture of the definitive prosthesis in 7 cases in the study by Lopes et al., 2015 [22], in 9 cases in the study by Marra et al., 2013 [18], in 2 cases in the study by Vogl et al., 2015 [20]; fracture of provisional prostheses in 2 cases in the study by Meloni et al., 2010 [15], in one case in the study by Yamada et al., 2015 [21]; imperfect fit of the provisional prosthesis in 2 cases in the study by Meloni et al., 2010 [15], in 3 cases in the study by Vogl et al., 2015 [20]; need for occlusal adjustments in 2 cases in the study by Vogl et al. 2015 [20].
- ✓
- Total early failures: 24
- ✓
- Total late failures: 7
- ✓
- Total patients: 226
- ✓
- Patients with early failure: 9
- ✓
- Patients with late failure: 2
- ✓
- Total early failure rate: 1.60%
- ✓
- Total late failure rate: 0.47%
- ✓
- Total early failure rate: 3.98%
- ✓
- Total late failure rate: 0.88%
4. Discussion
- ✓
- does not cause allergies, toxic, or infectious reactions;
- ✓
- offers anchorage for the prosthesis;
- ✓
- does not show any signs of fracture or flexion;
- ✓
- does not show any mobility when tested through movements obtained with hand tools;
- ✓
- shows no sign of radiolucency on an intraoral radiograph using a parallel beam technique perpendicular to the implant surface.
- Positioning the implants as equidistant as possible and limiting the number of intermediate elements to less than two to avoid micro-movements;
- Adequate splinting of the implants with the provisional restoration;
- Avoid excessive occlusal loading by limiting occlusal contacts in the anterior six teeth and instructing patients to avoid hard foods for up to 8 weeks after the insertion of the provisional restoration.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Voulgarakis, A.; Strub, J.R.; Att, W. Outcomes of implants placed with three different flapless surgical procedures: A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.H.; Chan, H.L.; Bashutski, J.D.; Oh, T.J.; Wang, H.L. The effect of flapless surgery on implant survival and marginal bone level: A systematic review and meta-analysis. J. Periodontol. 2014, 85, e91–e103. [Google Scholar] [CrossRef]
- Moraschini, V.; Velloso, G.; Luz, D.; Barboza, E.P. Implant survival rates, marginal bone level changes, and complications in full-mouth rehabilitation with flapless computer-guided surgery: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2015, 44, 892–901. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Jiménez-Guerra, A.; Ortiz-Garcia, I.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Cabanillas-Balsera, D.; López-López, J.; Monsalve-Guil, L. Immediate Loading of Implants Placed by Guided Surgery in Geriatric Edentulous Mandible Patients. Int. J. Environ. Res. Public Health 2021, 18, 4125. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Jiménez-Guerra, A.; Ortiz-Garcia, I.; Garrido, N.M.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Rondón-Romero, J.L.; Cabanillas-Balsera, D.; López-López, J.; Monsalve-Guil, L. Implant Treatment by Guided Surgery Supporting Overdentures in Edentulous Mandible Patients. Int. J. Environ. Res. Public Health 2021, 18, 11836. [Google Scholar] [CrossRef]
- Lopes, A.; Maló, P.; de Araújo Nobre, M.; Sanchez-Fernández, E. The NobelGuide® All-on-4® Treatment Concept for Rehabilitation of Edentulous Jaws: A Prospective Report on Medium- and Long-Term Outcomes. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 2), e406–e416. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Ortega, E.; Cracel-Lopes, J.L.; Matos-Garrido, N.; Jiménez-Guerra, A.; Ortiz-Garcia, I.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Rondón-Romero, J.L.; López-López, J.; Monsalve-Guil, L. Immediate Functional Loading with Full-Arch Fixed Implant-Retained Rehabilitation in Periodontal Patients: Clinical Study. Int. J. Environ. Res. Public Health 2022, 19, 13162. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Del Rocío Jiménez-Martin, I.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Rondón-Romero, J.L.; Cabanillas-Balsera, D.; Jiménez-Guerra, Á.; Ortiz-García, I.; López-López, J.; Monsalve-Guil, L. Long-Term Treatment Outcomes of Implant Prostheses in Partially and Totally Edentulous Patients. Materials 2022, 15, 4910. [Google Scholar] [CrossRef]
- D’Haese, J.; Van De Velde, T.; Elaut, L.; De Bruyn, H. A prospective study on the accuracy of mucosally supported stereolithographic surgical guides in fully edentulous maxillae. Clin. Implant. Dent. Relat. Res. 2012, 14, 293–303. [Google Scholar] [CrossRef]
- Dioguardi, M.; Spirito, F.; Sovereto, D.; Alovisi, M.; Aiuto, R.; Garcovich, D.; Crincoli, V.; Laino, L.; Cazzolla, A.P.; Caloro, G.A.; et al. The Prognostic Role of miR-31 in Head and Neck Squamous Cell Carcinoma: Systematic Review and Meta-Analysis with Trial Sequential Analysis. Int. J. Environ. Res. Public Health 2022, 19, 5334. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Spirito, F.; Sovereto, D.; Alovisi, M.; Troiano, G.; Aiuto, R.; Garcovich, D.; Crincoli, V.; Laino, L.; Cazzolla, A.P.; et al. MicroRNA-21 Expression as a Prognostic Biomarker in Oral Cancer: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 3396. [Google Scholar] [CrossRef]
- Dioguardi, M.; Spirito, F.; Sovereto, D.; La Femina, L.; Campobasso, A.; Cazzolla, A.P.; Di Cosola, M.; Zhurakivska, K.; Cantore, S.; Ballini, A.; et al. Biological Prognostic Value of miR-155 for Survival Outcome in Head and Neck Squamous Cell Carcinomas: Systematic Review, Meta-Analysis and Trial Sequential Analysis. Biology 2022, 11, 651. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, G.; Cantoni, T. Five-year follow-up of immediate fixed restorations of maxillary implants inserted in both fresh extraction and healed sites using the NobelGuide™ system. Clin. Implant. Dent. Relat. Res. 2015, 17, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Meloni, S.M.; De Riu, G.; Pisano, M.; Cattina, G.; Tullio, A. Implant treatment software planning and guided flapless surgery with immediate provisional prosthesis delivery in the fully edentulous maxilla. A retrospective analysis of 15 consecutively treated patients. Eur. J. Oral Implantol. 2010, 3, 245–251. [Google Scholar] [PubMed]
- Ciabattoni, G.; Acocella, A.; Sacco, R. Immediately restored full arch-fixed prosthesis on implants placed in both healed and fresh extraction sockets after computer-planned flapless guided surgery. A 3-year follow-up study. Clin. Implant. Dent. Relat. Res. 2017, 19, 997–1008. [Google Scholar] [CrossRef] [PubMed]
- Derksen, W.; Wismeijer, D.; Flügge, T.; Hassan, B.; Tahmaseb, A. The accuracy of computer-guided implant surgery with tooth-supported, digitally designed drill guides based on CBCT and intraoral scanning. A prospective cohort study. Clin. Oral Implant. Res. 2019, 30, 1005–1015. [Google Scholar] [CrossRef]
- Marra, R.; Acocella, A.; Rispoli, A.; Sacco, R.; Ganz, S.D.; Blasi, A. Full-mouth rehabilitation with immediate loading of implants inserted with computer-guided flap-less surgery: A 3-year multicenter clinical evaluation with oral health impact profile. Implant. Dent. 2013, 22, 444–452. [Google Scholar] [CrossRef]
- Pozzi, A.; Sannino, G.; Barlattani, A. Minimally invasive treatment of the atrophic posterior maxilla: A proof-of-concept prospective study with a follow-up of between 36 and 54 months. J. Prosthet. Dent. 2012, 108, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Vogl, S.; Stopper, M.; Hof, M.; Wegscheider, W.A.; Lorenzoni, M. Immediate Occlusal versus Non-Occlusal Loading of Implants: A Randomized Clinical Pilot Study. Clin. Implant. Dent. Relat. Res. 2015, 17, 589–597. [Google Scholar] [CrossRef]
- Yamada, J.; Kori, H.; Tsukiyama, Y.; Matsushita, Y.; Kamo, M.; Koyano, K. Immediate loading of complete-arch fixed prostheses for edentulous maxillae after flapless guided implant placement: A 1-year prospective clinical study. Int. J. Oral Maxillofac. Implant. 2015, 30, 184–193. [Google Scholar] [CrossRef]
- Lopes, A.; Maló, P.; de Araújo Nobre, M.; Sánchez-Fernández, E.; Gravito, I. The NobelGuide(®) All-on-4(®) Treatment Concept for Rehabilitation of Edentulous Jaws: A Retrospective Report on the 7-Years Clinical and 5-Years Radiographic Outcomes. Clin. Implant. Dent. Relat. Res. 2017, 19, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Malo, P.; de Araujo Nobre, M.; Lopes, A. The use of computer-guided flapless implant surgery and four implants placed in immediate function to support a fixed denture: Preliminary results after a mean follow-up period of thirteen months. J. Prosthet. Dent. 2007, 97, S26–S34. [Google Scholar] [CrossRef]
- Azari, A.; Nikzad, S. Flapless implant surgery: Review of the literature and report of 2 cases with computer-guided surgical approach. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2008, 66, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- van Steenberghe, D. Outcomes and their measurement in clinical trials of endosseous oral implants. Ann. Periodontol. 1997, 2, 291–298. [Google Scholar] [CrossRef]
- Calandriello, R.; Tomatis, M. Simplified treatment of the atrophic posterior maxilla via immediate/early function and tilted implants: A prospective 1-year clinical study. Clin. Implant. Dent. Relat. Res. 2005, 7 (Suppl. 1), S1–S12. [Google Scholar] [CrossRef]
- Villa, R.; Polimeni, G.; Wikesjö, U.M. Implant osseointegration in the absence of primary bone anchorage: A clinical report. J. Prosthet. Dent. 2010, 104, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 112–123. [Google Scholar] [CrossRef]
- Van Assche, N.; Quirynen, M. Tolerance within a surgical guide. Clin. Oral Implant. Res. 2010, 21, 455–458. [Google Scholar] [CrossRef]
- Vasak, C.; Watzak, G.; Gahleitner, A.; Strbac, G.; Schemper, M.; Zechner, W. Computed tomography-based evaluation of template (NobelGuide™)-guided implant positions: A prospective radiological study. Clin. Oral Implant. Res. 2011, 22, 1157–1163. [Google Scholar] [CrossRef]
- Rocci, A.; Martignoni, M.; Gottlow, J. Immediate loading of Brånemark System TiUnite and machined-surface implants in the posterior mandible: A randomized open-ended clinical trial. Clin. Implant. Dent. Relat. Res. 2003, 5 (Suppl. 1), 57–63. [Google Scholar] [CrossRef]
- Vanden Bogaerde, L.; Rangert, B.; Wendelhag, I. Immediate/early function of Brånemark System TiUnite implants in fresh extraction sockets in maxillae and posterior mandibles: An 18-month prospective clinical study. Clin. Implant. Dent. Relat. Res. 2005, 7 (Suppl. 1), S121–S130. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Giuliani, M.; Fabiani, C.; D’Alessandro, A.; Ciavarella, D.; Lo Muzio, L. Centering Ability of ProTaper Next and WaveOne Classic in J-Shape Simulated Root Canals. Sci. World J. 2016, 2016, 1606013. [Google Scholar] [CrossRef] [PubMed]
- Zhurakivska, K.; Troiano, G.; Caponio, V.C.A.; Dioguardi, M.; Laino, L.; Maffione, A.B.; Muzio, L.L. Do changes in oral microbiota correlate with plasma nitrite response? A systematic review. Front. Physiol. 2019, 10, 1029. [Google Scholar] [CrossRef]
- Buonavoglia, A.; Lauritano, D.; Perrone, D.; Ardito, F.; Troiano, G.; Dioguardi, M.; Candotto, V.; Silvestre, F.J.; Muzio, L.L.O. Evaluation of chemical-physical properties & cytocompatibility of theracal LC. J. Biol. Regul. Homeost. Agents 2017, 31, 1–9. [Google Scholar] [PubMed]
- Maló, P.; Rigolizzo, M.; Nobre, M.; Lopes, A.; Agliardi, E. Clinical outcomes in the presence and absence of keratinized mucosa in mandibular guided implant surgeries: A pilot study with a proposal for the modification of the technique. Quintessence Int. 2013, 44, 149–157. [Google Scholar] [CrossRef]
- Brodala, N. Flapless surgery and its effect on dental implant outcomes. Int. J. Oral Maxillofac. Implant. 2009, 24, 118–125. [Google Scholar]
- Van de Velde, T.; Glor, F.; De Bruyn, H. A model study on flapless implant placement by clinicians with a different experience level in implant surgery. Clin. Oral Implant. Res. 2008, 19, 66–72. [Google Scholar] [CrossRef]
- D’Haese, J.; Vervaeke, S.; Verbanck, N.; De Bruyn, H. Clinical and radiographic outcome of implants placed using stereolithographic guided surgery: A prospective monocenter study. Int. J. Oral Maxillofac. Implant. 2013, 28, 205–215. [Google Scholar] [CrossRef]
- Sanna, A.M.; Molly, L.; van Steenberghe, D. Immediately loaded CAD-CAM manufactured fixed complete dentures using flapless implant placement procedures: A cohort study of consecutive patients. J. Prosthet. Dent. 2007, 97, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Villa, R.; Rangert, B. Immediate and early function of implants placed in extraction sockets of maxillary infected teeth: A pilot study. J. Prosthet. Dent. 2007, 97, S96–S108. [Google Scholar] [CrossRef]
- Novaes, A.B., Jr.; Suaid, F.; Queiroz, A.C.; Muglia, V.A.; Souza, S.L.; Palioto, D.B.; Taba, M., Jr.; Grisi, M.F. Buccal bone plate remodeling after immediate implant placement with and without synthetic bone grafting and flapless surgery: Radiographic study in dogs. J. Oral Implantol. 2012, 38, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Rosén, A.; Gynther, G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: A long-term follow-up study. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2007, 65, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Clelland, N.L.; Gilat, A.; McGlumphy, E.A.; Brantley, W.A. A photoelastic and strain gauge analysis of angled abutments for an implant system. Int. J. Oral Maxillofac. Implant. 1993, 8, 541–548. [Google Scholar]
- Clelland, N.L.; Lee, J.K.; Bimbenet, O.C.; Brantley, W.A. A three-dimensional finite element stress analysis of angled abutments for an implant placed in the anterior maxilla. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 1995, 4, 95–100. [Google Scholar] [CrossRef]
- Östman, P.O.; Wennerberg, A.; Ekestubbe, A.; Albrektsson, T. Immediate occlusal loading of NanoTite™ tapered implants: A prospective 1-year clinical and radiographic study. Clin. Implant. Dent. Relat. Res. 2013, 15, 809–818. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Felice, P.; Leone, M.; Checchi, V.; Esposito, M. Flapless versus open flap implant surgery in partially edentulous patients subjected to immediate loading: 1-year results from a split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 177–188. [Google Scholar]
- Szmukler-Moncler, S.; Salama, H.; Reingewirtz, Y.; Dubruille, J.H. Timing of loading and effect of micromotion on bone-dental implant interface: Review of experimental literature. J. Biomed. Mater. Res. 1998, 43, 192–203. [Google Scholar] [CrossRef]
- Hultin, M.; Svensson, K.G.; Trulsson, M. Clinical advantages of computer-guided implant placement: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 124–135. [Google Scholar] [CrossRef]
- Komiyama, A.; Klinge, B.; Hultin, M. Treatment outcome of immediately loaded implants installed in edentulous jaws following computer-assisted virtual treatment planning and flapless surgery. Clin. Oral Implant. Res. 2008, 19, 677–685. [Google Scholar] [CrossRef]
- Laino, L.; Troiano, G.; Dioguardi, M.; Perillo, L.; Laino, G.; Muzio, L.L.; Cicciu, M. Patient discomfort during and after surgically assisted rapid maxillary expansion under local anaesthesia. J. Craniofacial Surg. 2016, 27, 772–775. [Google Scholar] [CrossRef] [PubMed]
- Maló, P.; Nobre, M.; Lopes, A. The rehabilitation of completely edentulous maxillae with different degrees of resorption with four or more immediately loaded implants: A 5-year retrospective study and a new classification. Eur. J. Oral Implantol. 2011, 4, 227–243. [Google Scholar] [PubMed]


{kind=link}
| First Autor, Data | Type of Study | Number Patient (Female/Male) | Age (Average) | Number Implant | Diameter/Length Implants (mm) | Follow up |
|---|---|---|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | Prospective | 32 (23/9) | 44–73 (59.5) | 197 in post-extraction sites; 88 in healed sites | / | 3 years |
| Derksen et al., 2019 [17] | Prospective | 66 (36/30) | 20–73 (52.4) | 145 | 3.3-4.8/8-10-12 | 1 and 2 years |
| Lopes et al., 2015 [7] | Prospective | 23 (13/10) | 34–70 (55.4) | 92 | 4/8-10-11.5-13-15-18 | 1, 3 and 5 years |
| Marra et al., 2013 [18] | Prospective | 30 (18/12) | / | 312 | 3.3-3.75-4/8.5-18 | 3 years |
| Meloni et al., 2010 [15] | Retrospective | 15 (10/5) | 40–70 (52) | 90 | 4.3-5/10-13 | 18 months |
| Polizzi and Cantoni, 2015 [14] | Retrospective | 27 (20/7) | 34–71 (55.8) | 92 in healed sites; 68 in post-extraction sites | / | 5 years |
| Pozzi et al., 2012 [19] | Prospective | 27 (12/15) | 38–77 (54.18) | 39 axials; 42 tilted | 2.8-3.2-3.-8/14.4 (axials)-16.1 (tilted) | 43.4 months |
| Vogl et al., 2015 [20] | Prospective | 20 (13/7) divided into 2 groups: 9 immediate occlusal loading; 10 non-occlusal load | 33-70 (54) | 21 (with immediate occlusal loading) 31 (without occlusal load) | / | 1 year |
| Yamada et al., 2015 [21] | Prospective | 48 (22/26) | 34–74 (56) | 278 | 3.5-4.3-5/8.5-18 | 1 year |
| First Autor, Data | State of the Dental Arch | Condition of the Implant Site | Flap/Miniflap/Flapless | Protocol (Immediate Loading, Conventional) | Final Restoration (Months) |
|---|---|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | Total edentulism | Post-extraction and healed | Flapless | Immediate | / |
| Derksen et al., 2019 [17] | Partial edentulism | Healed | Flapless (34) and miniflap (111) | Conventional | 4 |
| Lopes et al., 2015 [7] | Total edentulism | Healed | flapless | Immediate | 4 |
| Marra et al., 2013 [18] | Total edentulism | Healed | Flapless | Immediate | 4–6 |
| Meloni et al., 2010 [15] | Total edentulism | Healed | Flapless | Immediate | 6 |
| Polizzi and Cantoni, 2015 [14] | Partial/total edentulism | Post-extraction and healed | Flapless | Immediate | 6 |
| Pozzi et al., 2012 [19] | Partial edentulism | Healed | Flapless; miniflap | Immediate | 6 |
| Vogl et al., 2015 [20] | Partial edentulism | Healed | Flapless | Immediate | 6–8 |
| Yamada et al., 2015 [21] | Total edentulism | Healed | Flapless | Immediate | 4–7 |
| First Autor, Data | Failure | Implant Survival Rate | Medium Marginal Bone Loss | Implant-Prosthetic Complications |
|---|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | Early: 5 in extraction sites (after 6 months) late: 2 in healed sites (after 2 and 3 years) | 97.54% | Mm | Postoperative: implant loss (7). |
| Derksen et al., 2019 [17] | 1 early failure (6 weeks) | 99.3% | / | Intraoperative: Inability to use a drill due to limited mouth opening (1), vestibular dehiscence after osteotomy (1). |
| Lopes et al., 2015 [7] | Early: 2 after 5 months Late: 1 after 3 years | 96.6% | 1.9 mm | Postoperative: Abutment screw loosening (2), definitive prosthesis fracture (7), implant loss (3). |
| Marra et al., 2013 [18] | Early: 3 in the first 3 months, 2 after 6 months Late: 1 after 1 year, 1 after 2 years | 97.9% | Mm | Postoperative: Prosthesis Fracture (9), implant loss (6). |
| Meloni et al., 2010 [15] | Early: 2 after 6 months | 97.8% | 1.6 mm | Postoperative: Implant loss (2), imperfect fit of the provisional prosthesis (2), fracture of the provisional prosthesis (1). |
| Polizzi and Cantoni, 2015 [14] | Early: 2 after 6 months (post-extraction site) Late: 2 in healed sites (after 2 years) | 97.33% | 1.39 mm | Postoperative: Implant loss (4). |
| Pozzi et al., 2012 [19] | Early: 1 axial, 2 tilted, after 4 months in the same patient | 96.3% | 0.6 mm | Postoperative: Implant loss (3). |
| Vogl et al., 2015 [20] | 0 | 100% | 0.4 ± 0.5 mm | Intraoperative: Insufficient bone quantity (1), insufficient primary stability (3); Postoperative: Imperfect fit of temporary prostheses (3), occlusal adjustments required (2), fractures (2), abutment screw loosening (3). |
| Yamada et al., 2015 [21] | Early: 2 in one patient (2 weeks); 2 in a patient (1 month) | 98.6% | 0.32 mm | Postoperative: Abutment screw loosening (10), temporary fracture prosthesis (1), implant mobility (4). |
| First Autor, Data | N. Implant | Early Failure Rate | Late Failure Rate |
|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | 285 | 1.75% | 0.70% |
| Derksen et al., 2019 [17] | 145 | 0.69% | 0% |
| Lopes et al., 2015 [7] | 92 | 2.17% | 1.09% |
| Marra et al., 2013 [18] | 312 | 1.60% | 0.64% |
| Meloni et al., 2010 [15] | 90 | 2.22% | 0% |
| Vogl et al., 2015 [20] | 52 | 0% | 0% |
| Polizzi and Cantoni, 2015 [14] | 160 | 1.25% | 1.25% |
| Pozzi et al., 2012 [19] | 81 | 3.70% | 0% |
| Yamada et al., 2015 [21] | 278 | 1.44% | 0% |
| Total failure rate | 1.60% | 0.47% |
| First Autor, Data | N. Patient | Early Failure Rate | Late Failure Rate |
|---|---|---|---|
| Derksen et al., 2019 [17] | 66 | 1.51% | 0% |
| Lopes et al., 2015 [7] | 23 | 8.69% | 4.35% |
| Meloni et al., 2010 [15] | 15 | 13.33% | 0% |
| Polizzi and Cantoni, 2015 [14] | 27 | 3.70% | 3.70% |
| Pozzi et al., 2012 [19] | 27 | 3.70% | 0% |
| Vogl et al., 2015 [20] | 20 | 0% | 0% |
| Yamada et al., 2015 [21] | 48 | 4.16% | 0% |
| Total failure rate | 3.98% | 0.88% |
| First Autor, Data | Type of Study | Exclusion Criteria Adopted in Relation to Cigarette Smoking | Number Patient | Number Implant | Number of Smoking Patients | Number of Failed Implants in Smokers | Biological Complications | |
|---|---|---|---|---|---|---|---|---|
| Failures Due to Lack of Osseointegration (within 6 Months) | Peri-Implant Pathology, Periimplantitis | |||||||
| Ciabattoni et al., 2017 [16]; | Prospective | more than 10 cigarettes/day | 32 | 285 | \ | \ | 5 | \ |
| Derksen et al., 2019 [17] | Prospective | smokers were not excluded | 66 | 145 | \ | 1 | 1 | \ |
| Lopes et al., 2015 [22] | Prospective | smokers were not excluded | 23 | 92 | 2 (heavy smokers) 1 | \ | 2 | 2 peri-implant pathology |
| Marra et al., 2013 [18] | Prospective | smokers were not excluded | 30 | 312 | \ | \ | 3 | 1 implant lost after 2 years (periimplantitis) |
| Meloni et al., 2010 [15] | Retrospective | smokers were not excluded | 15 | 90 | 5 (3 patients smoked up to 10 cigarettes a day, 2 smoked more than 10 cigarettes per day) | \ | 2 | 2 periimplantitis |
| Polizzi and Cantoni, 2015 [14] | Retrospective | Smoker patients (≤20 cigarettes/day) were not excluded | 27 | 160 | \ | 2 | 2 | 24 implants in 3 patients (periimplantitis) |
| Pozzi et al., 2012 [19] | Prospective | more than 10 cigarettes/day | 27 | 81 | \ | \ | 3 | \ |
| Vogl et al., 2015 [20] | Prospective | more than 10 cigarettes/day | 20 | 52 | \ | \ | 0 | 3 mucositis |
| Yamada et al., 2015 [21] | Prospective | smokers were not excluded | 48 | 278 | 13 | 4 | 4 | \ |
| First Autor, Data | Position | Implant Failure | Anterior Position (Number of Implant Failures) | Posterior Position (Number of Implant Failures) | Maxilla (Number of Implant Failures) | Mandibular (Number of Implant Failures) |
|---|---|---|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | Maxilla\mandible | 7 | \ | \ | 5\193 | 2\90 |
| Derksen et al., 2019 [17] | Maxilla\mandible | 1 | \ | \ | 66 | 1\79 |
| Lopes et al., 2015 [7] | Maxilla\mandible | 3 | Maxilla (lateral incisor) | 2Maxilla (first molar, second premolar) | 3\72 | 0\20 |
| Marra et al., 2013 [18] | Maxilla\mandible | 6 | \ | \ | 5\177 | 1\135 |
| Meloni et al., 2010 [15] | Maxilla | 2 | \ | \ | 2 | \ |
| Polizzi and Cantoni, 2015 [14] | Maxilla | 4 | \ | \ | 4 | \ |
| Pozzi et al., 2012 [19] | Maxilla | 3 | 2 ASW | 1 PSW | 3 | \ |
| Vogl et al., 2015 [20] | Mandible | \ | \ | \ | \ | \ |
| Yamada et al., 2015 [21] | Maxilla | 4 | 2 maxilla (incisive lateral R and incisive lateral L) | 2 maxilla (first molar R and first molar L) | 4 | \ |
| Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias | |
|---|---|---|---|---|---|---|---|---|
| Ciabattoni et al., 2017 [16]; | + | + | + | + | + | + | + | + |
| Derksen et al., 2019 [17] | + | + | + | + | + | + | + | + |
| Lopes et al., 2015 [7] | + | + | + | + | + | + | + | + |
| Marra et al., 2013 [18] | + | + | + | + | + | + | + | + |
| Meloni et al., 2010 [15] | + | + | + | + | - | + | + | + |
| Polizzi and Cantoni, 2015 [14] | + | + | + | + | + | + | + | + |
| Pozzi et al., 2012 [19] | + | + | + | + | + | + | + | + |
| Vogl et al., 2015 [20] | + | + | + | + | + | + | + | + |
| Yamada et al., 2015 [21] | + | + | + | + | + | + | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dioguardi, M.; Spirito, F.; Quarta, C.; Sovereto, D.; Basile, E.; Ballini, A.; Caloro, G.A.; Troiano, G.; Lo Muzio, L.; Mastrangelo, F. Guided Dental Implant Surgery: Systematic Review. J. Clin. Med. 2023, 12, 1490. https://doi.org/10.3390/jcm12041490
Dioguardi M, Spirito F, Quarta C, Sovereto D, Basile E, Ballini A, Caloro GA, Troiano G, Lo Muzio L, Mastrangelo F. Guided Dental Implant Surgery: Systematic Review. Journal of Clinical Medicine. 2023; 12(4):1490. https://doi.org/10.3390/jcm12041490
Chicago/Turabian StyleDioguardi, Mario, Francesca Spirito, Cristian Quarta, Diego Sovereto, Elisabetta Basile, Andrea Ballini, Giorgia Apollonia Caloro, Giuseppe Troiano, Lorenzo Lo Muzio, and Filiberto Mastrangelo. 2023. "Guided Dental Implant Surgery: Systematic Review" Journal of Clinical Medicine 12, no. 4: 1490. https://doi.org/10.3390/jcm12041490