
Influence of COVID-19 Pandemic on Colorectal Cancer Presentation, Management and Outcome during the COVID-19 Pandemic
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Study Design
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. Jama 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Ministero Della Salute. New Coronavirus News Section. 2020. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4184 (accessed on 1 September 2021).
- Osservatorio Nazionale Screening. Rapporto Sui ritardi Accumulati alla Fine di maggio 2020 dai programmi di screening Italiani e sulla velocità della ripartenza [National Screening Observatory. Report on the Delays of the Italian Screening Programs by the End of May 2020 and on the Re-Start Speed]. 2020. Available online: https://www.osservatorionazionalescreening.it/sites/default/files/allegati/Rapporto_ripartenza-maggio_2020_def_0.pdf (accessed on 1 September 2021).
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Wong, S.Y.S.; Zhang, D.; Sit, R.W.S.; Yip, B.H.K.; Chung, R.Y.-N.; Wong, C.K.M.; Chan, D.C.C.; Sun, W.; Kwok, K.O.; Mercer, S.W. Impact of COVID-19 on loneliness, mental health, and health service utilisation: A prospective cohort study of older adults with multimorbidity in primary care. Br. J. Gen. Pract. 2020, 70, e817–e824. [Google Scholar] [CrossRef]
- Karacin, C.; Bilgetekin, I.; B Basal, F.; Oksuzoglu, O.B. How does COVID-19 fear and anxiety affect chemotherapy adherence in patients with cancer. Future Oncol. 2020, 16, 2283–2293. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Morris, E.J.A.; Goldacre, R.; Spata, E.; Mafham, M.; Finan, P.J.; Shelton, J.; Richards, M.; Spencer, K.; Emberson, J.; Hollings, S.; et al. Impact of the COVID-19 pandemic on the detection and management of colorectal cancer in England: A population-based study. Lancet Gastroenterol. Hepatol. 2021, 6, 199–208. [Google Scholar] [CrossRef]
- Dinmohamed, A.G.; Visser, O.; Verhoeven, R.H.A.; Louwman, M.W.J.; van Nederveen, F.H.; Willems, S.M.; Merkx, M.A.W.; Lemmens, V.E.P.P.; Nagtegaal, I.D.; Siesling, S. Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands. Lancet Oncol. 2020, 21, 750–751. [Google Scholar] [CrossRef]
- Aguiar, S., Jr.; Riechelmann, R.P.; de Mello, C.A.L.; da Silva, J.C.F.; Diogenes, I.D.C.; Andrade, M.S.; de Miranda Marques, T.M.D.; Stevanato, P.R.; Bezerra, T.S.; Silva, M.L.G.; et al. Impact of COVID-19 on colorectal cancer presentation. Br. J. Surg. 2021, 108, e81–e82. [Google Scholar] [CrossRef]
- Programma Nazionale Esiti—Edizione 2021. Agenzia Nazionale per i Servizi Sanitari Regionali. Available online: https://pne.agenas.it/main/doc/Report_PNE_2021.pdf (accessed on 10 October 2022).
- Willms, A.G.; CAMIN Study Group; Oldhafer, K.J.; Conze, S.; Thasler, W.E.; von Schassen, C.; Hauer, T.; Huber, T.; Germer, C.-T.; Günster, S. Appendicitis during the COVID-19 lockdown: Results of a multicenter analysis in Germany. Langenbecks Arch. Surg. 2021, 406, 367–375. [Google Scholar] [CrossRef]
- Zaborowski, A.M.; Abdile, A.; Adamina, M.; Aigner, F.; d’Allens, L.; Allmer, C.; Álvarez, A.; Anula, R.; Andric, M.; Atallah, S. Characteristics of early-onset vs late-onset colorectal cancer: A review. JAMA Surg. 2021, 156, 865–874. [Google Scholar] [CrossRef]
- Rossi, P.; Sileri, P.; Gentileschi, P.; Sica, G.; Forlini, A.; Stolfi, V.; De Majo, A.; Coscarella, G.; Canale, S.; Gaspari, A.L. Percutaneous liver biopsy using an ultrasound-guided subcostal route. Dig. Dis. Sci. 2001, 46, 128–132. [Google Scholar] [CrossRef]
- Sica, G.S.; Iaculli, E.; Benavoli, D.; Biancone, L.; Calabrese, E.; Onali, S.; Gaspari, A.L. Laparoscopic Versus Open Ileo-Colonic Resection in Crohn’s Disease: Short- and Long-Term Results from a Prospective Longitudinal Study. J. Gastrointest Surg. 2008, 12, 1094–1102. [Google Scholar] [CrossRef]
- Fina, D.; Franze, E.; Rovedatti, L.; Corazza, G.R.; Biancone, L.; Sileri, P.P.; Sica, G.; MacDonald, T.T.; Pallone, F.; Di Sabatino, A.; et al. Interleukin-25 production is differently regulated by TNF-alpha and TGF-beta 1 in the human gut. Mucosal. Immunol. 2011, 4, 239–244. [Google Scholar] [CrossRef]
- Sileri, P.; Sica, G.; Gentileschi, P.; Venza, M.; Manzelli, A.; Palmieri, G.; Spagnoli, L.G.; Testa, G.; Benedetti, E.; Gaspari, A.L. Ischemic preconditioning protects intestine from prolonged ischemia. Transplant. Proc. 2004, 36, 283–285. [Google Scholar] [CrossRef]
- Hermanek, P.; Sobin, L.H. TNM Classification of Malignant Tumors; New Edition; Springer: Berlin/Heidelberg, Germany, 1987. [Google Scholar]
- American Society of Anesthesiologists. ASA Physical Status Classification System. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 23 October 2019).
- Sica, G.S.; Vinci, D.; Siragusa, L.; Sensi, B.; Guida, A.M.; Bellato, V.; García-Granero, Á.; Pellino, G. Definition and reporting of lymphadenectomy and complete mesocolic excision for radical right colectomy: A systematic review. Surg. Endosc. 2022. [Google Scholar] [CrossRef]
- Sica, G.S.; Campanelli, M.; Bellato, V.; Monteleone, G. Gastrointestinal cancer surgery and enhanced recovery after surgery (ERAS) during COVID-19 outbreak. Langenbeck’s Arch. Surg. 2020, 405, 357–358. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar] [CrossRef]
- Amelio, I.; Bertolo, R.; Bove, P.; Candi, E.; Chiocchi, M.; Cipriani, C.; Di Daniele, N.; Ganini, C.; Juhl, H.; Mauriello, A.; et al. Cancer predictive studies. Biol Direct. 2020, 14, 18. [Google Scholar] [CrossRef]
- Sibio, S.; Di Giorgio, A.; Campanelli, M.; Di Carlo, S.; Divizia, A.; Fiorani, C.; Scaramuzzo, R.; Arcudi, C.; Del Vecchio Blanco, G.; Biancone, L.; et al. Ambulatory Surgery for Perianal Crohn’s Disease: Study of Feasibility. Gastroenterol. Res. Pract. 2018, 2018, 5249087. [Google Scholar] [CrossRef]
- Onali, S.; Calabrese, E.; Petruzziello, C.; Lolli, E.; Ascolani, M.; Ruffa, A.; Sica, G.; Rossi, A.; Chiaramonte, C.; Pallone, F.; et al. Post-operative recurrence of Crohn’s disease: A prospective study at 5 years. Dig. Liver Dis. 2016, 48, 489–494. [Google Scholar] [CrossRef]
- Sileri, P.; Mele, A.; Stolfi, V.M.; Grande, M.; Sica, G.; Gentileschi, P.; Di Carlo, S.; Gaspari, A.L. Medical and surgical treatment of chronic anal fissure: A prospective study. J. Gastrointest. Surg. 2007, 11, 1541–1548. [Google Scholar] [CrossRef]
- Vecchione, L.; Stintzing, S.; Pentheroudakis, G.; Douillard, J.Y.; Lordick, F. ESMO management and treatment adapted recommendations in the COVID-19 era: Colorectal cancer. ESMO Open 2020, 5 (Suppl. S3), e000826. [Google Scholar] [CrossRef]
- Sutherland, K.; Chessman, J.; Zhao, J.; Sara, G.; Went, A.; Dyson, S.; Levesque, J.-F. Impact of COVID-19 on healthcare activity in NSW, Australia. Public Health Res. Pract. 2020, 30, 3042030. [Google Scholar] [CrossRef]
- Cano-Valderrama, O.; Sánchez-Santos, R.; Vigorita, V.; Paniagua, M.; Flores, E.; Garrido, L.; Facal, C.; Ruano, A.; San-Ildefonso, A.; Moncada, E. Has the COVID-19 pandemic changed the clinical picture and tumour stage at the time of presentation of patients with colorectal cancer? A retrospective cohort study. Cir. Esp. 2023, 101, 90–96. [Google Scholar] [CrossRef]
- Kuzuu, K.; Misawa, N.; Ashikari, K.; Kessoku, T.; Kato, S.; Hosono, K.; Yoneda, M.; Nonaka, T.; Matsushima, S.; Komatsu, T.; et al. Gastrointestinal Cancer Stage at Diagnosis Before and During the COVID-19 Pandemic in Japan. JAMA Netw. Open 2021, 4, e2126334. [Google Scholar] [CrossRef]
- Mentrasti, G.; Cantini, L.; Zichi, C.; D’Ostilio, N.; Gelsomino, F.; Martinelli, E.; Chiari, R.; La Verde, N.; Bisonni, R.; Cognigni, V.; et al. Alarming Drop in Early Stage Colorectal Cancer Diagnoses After COVID-19 Outbreak: A Real-World Analysis from the Italian COVID-DELAY Study. Oncologist 2022, 27, e723–e730. [Google Scholar] [CrossRef]
- Kistler, C.E. Colorectal-cancer incidence and mortality after screening. N. Engl. J. Med. 2013, 369, 2354. [Google Scholar] [CrossRef]
- Rutter, M.D.; Brookes, M.; Lee, T.J.; Rogers, P.; Sharp, L. Impact of the COVID-19 pandemic on UK endoscopic activity and cancer detection: A National Endoscopy Database Analysis. Gut 2021, 70, 537–543. [Google Scholar] [CrossRef]
- Greene, G.; Griffiths, R.; Han, J.; Akbari, A.; Jones, M.; Lyons, J.; Lyons, R.A.; Rolles, M.; Torabi, F.; Warlow, J.; et al. Impact of the SARS-CoV-2 pandemic on female breast, colorectal and non-small cell lung cancer incidence, stage and healthcare pathway to diagnosis during 2020 in Wales, UK, using a national cancer clinical record system. Br. J. Cancer 2022, 127, 558–568. [Google Scholar] [CrossRef]
- Lou, J.; Kooragayala, K.; Williams, J.P.; Sandilos, G.; Butchy, M.V.; Yoon-Flannery, K.; Kwiatt, M.; Hong, Y.K.; Shersher, D.D.; Burg, J.M. The Early Impact of the COVID-19 Pandemic on Lung, Colorectal, and Breast Cancer Screening and Treatment at a Tertiary Cancer Center. Am. J. Clin. Oncol. 2022, 45, 381–390. [Google Scholar] [CrossRef]
- De Jonge, L.; Worthington, J.; van Wifferen, F.; Iragorri, N.; Peterse, E.F.P.; Lew, J.; Greuter, M.J.E.; Smith, H.A.; Feletto, E.; Yong, J.H.E.; et al. Impact of the COVID-19 pandemic on faecal immunochemical test-based colorectal cancer screening programmes in Australia, Canada, and the Netherlands: A comparative modelling study. Lancet Gastroenterol. Hepatol. 2021, 6, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Gentileschi, P.; Camperchioli, I.; Benavoli, D.; Di Lorenzo, N.; Sica, G.; Gaspari, A.L. Laparoscopic single-port sleeve gastrectomy for morbid obesity: Preliminary series. Surg. Obes. Relat. Dis. 2010, 6, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Lieberman, D. Screening and Surveillance Colonoscopy and COVID-19: Avoiding More Casualties. Gastroenterology 2020, 159, 1205–1208. [Google Scholar] [CrossRef] [PubMed]
- D’Ovidio, V.; Lucidi, C.; Bruno, G.; Lisi, D.; Miglioresi, L.; Bazuro, M.E. Impact of COVID-19 Pandemic on Colorectal Cancer Screening Program. Clin. Color. Cancer 2021, 20, e5–e11. [Google Scholar] [CrossRef] [PubMed]
- Yong, J.H.; Mainprize, J.G.; Yaffe, M.J.; Ruan, Y.; Poirier, A.E.; Coldman, A.; Nadeau, C.; Iragorri, N.; Hilsden, R.J.; Brenner, D.R. The impact of episodic screening interruption: COVID-19 and population-based cancer screening in Canada. J. Med. Screen. 2021, 28, 100–107. [Google Scholar] [CrossRef]
- Baran, B.; Mert Ozupek, N.; Yerli Tetik, N.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef]
- Rabeneck, L.; Davila, J.A.; El-Serag, H.B. Is there a true “shift” to the right colon in the incidence of colorectal cancer? Am. J. Gastroenterol. 2003, 98, 1400–1409. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Kopel, J.; Ristic, B.; Brower, G.L.; Goyal, H. Global Impact of COVID-19 on Colorectal Cancer Screening: Current Insights and Future Directions. Medicina 2022, 58, 100. [Google Scholar] [CrossRef]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371, m4087. [Google Scholar] [CrossRef] [PubMed]
- Sjo, O.H.; Larsen, S.; Lunde, O.C.; Nesbakken, A. Short term outcome after emergency and elective surgery for colon cancer. Color. Dis. 2009, 11, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Loveday, C.; Sud, A.; Jones, M.; Broggio, J.; Scott, S.; Gronthound, F.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; et al. Prioritisation by FIT to mitigate the impact of delays in the 2-week wait colorectal cancer referral pathway during the COVID-19 pandemic: A UK modelling study. Gut 2021, 70, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Watt, T.; Firth, Z.; Fisher, R.; Thorlby, R.; Kelly, E. Use of Primary Care during the COVID-19 Pandemic. Patient-Level Data Analysis of the Impact of COVID-19 on Primary Care Activity in England. 2020. Available online: https://www.health.org.uk/news-and-comment/charts-and-infographics/use-of-primary-care-during-the-covid-19-pandemic (accessed on 1 September 2021).
- Shinkwin, M.; Silva, L.; Vogel, I.; Reeves, N.; Cornish, J.; Horwood, J.; Davies, M.M.; Torkington, J.; Ansell, J. COVID-19 and the emergency presentation of colorectal cancer. Color. Dis. 2021, 23, 2014–2019. [Google Scholar] [CrossRef]
- Lee, T.; Cheng, D.Z.; Foo, F.J.; Sivarajah, S.S.; Ho, L.M.L.; Aw, D.; Chong, C.X.Z.; Ng, J.L.; Tan, W.J.H.; Koh, F.H. Did the COVID-19 lockdown result in a delay of colorectal cancer presentation and outcomes? A single centre review. Langenbecks Arch. Surg. 2022, 407, 739–745. [Google Scholar] [CrossRef]
- Williams, E.; Kong, J.C.; Singh, P.; Prabhakaran, S.; Warrier, S.K.; Bell, S. The impact of the COVID-19 pandemic on colorectal cancer diagnosis and management: A Binational Colorectal Cancer Audit study. ANZ J. Surg. 2021, 91, 2091–2096. [Google Scholar] [CrossRef]
- Mason, S.E.; Scott, A.J.; Markar, S.R.; Clarke, J.M.; Martin, G.; Winter Beatty, J.; Sounderajah, V.; Yalamanchili, S.; Denning, M.; Arulampalam, T.; et al. PanSurg Collaborative Insights from a global snapshot of the change in elective colorectal practice due to the COVID-19 pandemic. PLoS ONE 2020, 15, e0240397. [Google Scholar] [CrossRef]
- Spinelli, A.; Anania, G.; Arezzo, A.; Berti, S.; Bianco, F.; Bianchi, P.P.; De Giuli, M.; De Nardi, P.; de Paolis, P.; Foppa, C.; et al. Italian multi-society modified Delphi consensus on the definition and management of anastomotic leakage in colorectal surgery. Updat. Surg. 2020, 72, 781–792. [Google Scholar] [CrossRef]
- ESCP EAGLE Safe Anastomosis Collaborative. ESCP Safe Anastomosis ProGramme in CoLorectal SurgEry (EAGLE): Study protocol for an international cluster randomised trial of a quality improvement intervention to reduce anastomotic leak following right colectomy. Color. Dis. 2021, 23, 2761–2771. [Google Scholar] [CrossRef]
- Urgent Intercollegiate General Surgery Guidance on COVID-19. ACPGBI. March 2020. Available online: https://www.rcsed.ac.uk/news-public-affairs/news/2020/march/intercollegiate-general-surgery-guidance-on-covid-19-update (accessed on 15 October 2022).
- Borghi, F.; Pellegrino, L.; Pruiti, V.; Donati, D.; Giraudo, G. Feasibility of enhanced recovery after surgery program in colorectal surgery during COVID-19 pandemic in Italy: Should we change something? Updates Surg. 2020, 72, 319–320. [Google Scholar] [CrossRef]
- McPhail, S.D.; Elliss-Brookes, L.; Shelton, J.G.; Ives, A.; Greenslade, M.; Vernon, S.W.; Morris, E.J.; Richards, M. Emergency presentation of cancer and short-term mortality. Br. J. Cancer 2013, 109, 2027–2034. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Group A (n = 147) | Group B (n = 133) | p-Value | |||
|---|---|---|---|---|---|---|
|
Age (mean, SD) Year | 69.5 ± 12.8 Median 72 | 70.7 ± 11.5 Median 74 | 0.452 | |||
| Sex | Male | 84 | 57.1% | 77 | 57.9% | 0.904 |
| (%) | Female | 63 | 42.9% | 56 | 42.1% | |
| BMI (mean, SD) | 25.3 ± 4.3 Median 25 | 26.2 ± 4.0 Median 25.8 | 0.072 | |||
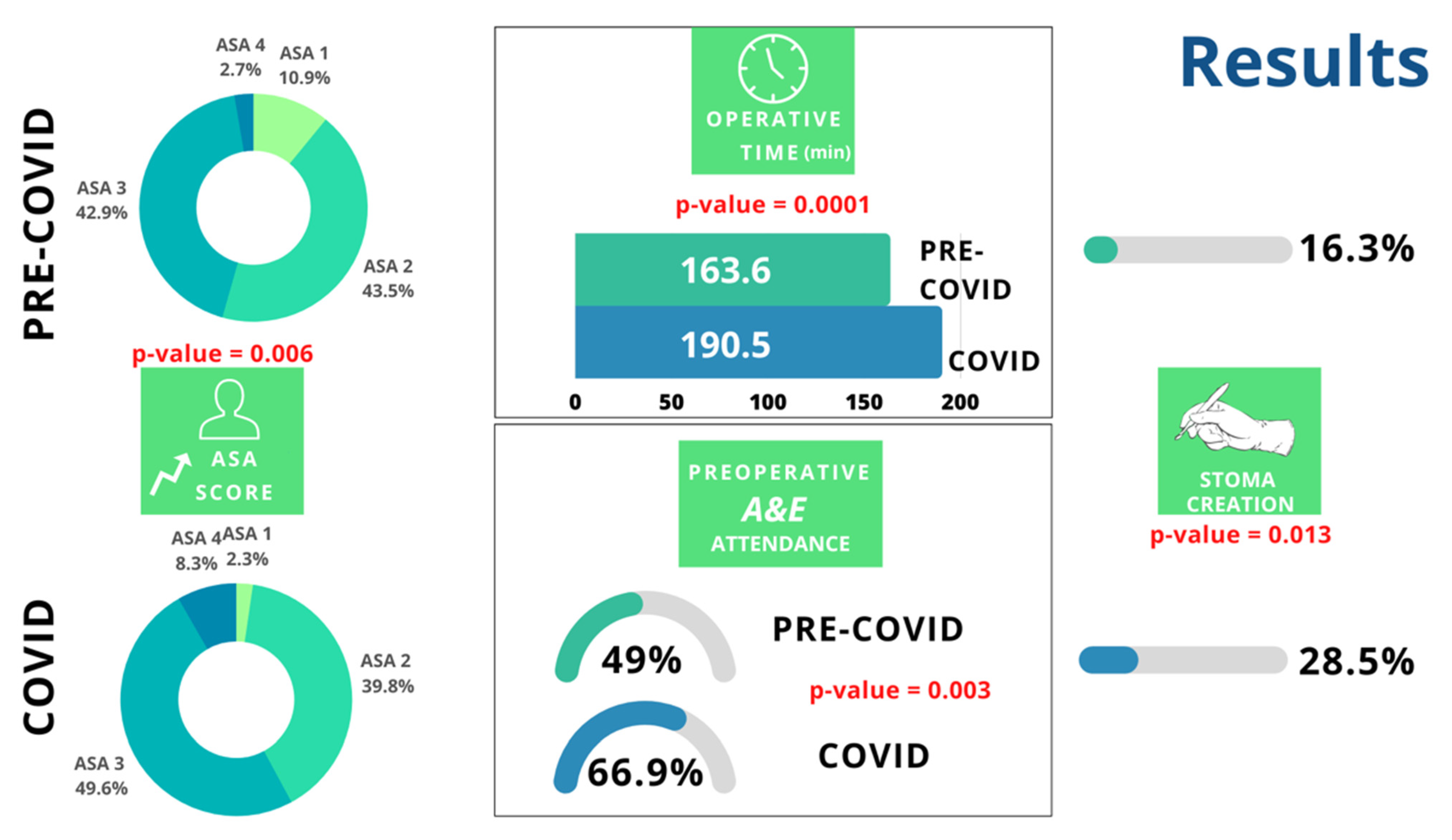
| ASA score % | 0.006 | |||||
| 1 | 16 | 10.9% | 3 | 2.3% | ||
| 2 | 64 | 43.5% | 53 | 39.8% | ||
| 3 | 63 | 42.9% | 66 | 49.6% | ||
| 4 | 4 | 2.7% | 11 | 8.3% | ||
| Localization | 0.534 | |||||
| Right Colon | 57 | 38.7% | 61 | 45.9% | ||
| Left Colon | 49 | 33.3% | 38 | 28.6% | ||
| Rectum | 41 | 27.8% | 34 | 25.5% | ||
| Time from diagnosis to Surgery | 12 ± 3.3 Median 14 | 13 ± 2.8 Median 15 | 0.962 | |||
| Staging | Group A (n = 147) | Group B (n = 133) | p-Value | ||
|---|---|---|---|---|---|
| I | 22 | 15% | 24 | 18% | 0.552 |
| II | 46 | 31.3% | 48 | 36.1% | |
| III | 56 | 38.1% | 46 | 34.6% | |
| IV | 23 | 15.6% | 46 | 34.6% | |
| Staging Right Colon Cancer | Group A (n = 57) | Group B (n = 61) | p-value | ||
| I | 5 | 8.79% | 10 | 16.4% | 0.620 |
| II | 22 | 38.5% | 20 | 32.8% | |
| III | 21 | 36.8% | 23 | 37.7% | |
| IV | 9 | 15.8% | 8 | 13.1% | |
| Staging Left Colon Cancer | Group A (n = 49) | Group B (n = 38) | p-value | ||
| I | 11 | 22.4% | 5 | 13.1% | 0.150 |
| II | 12 | 24.5% | 18 | 47.4% | |
| III | 21 | 42.9% | 13 | 34.2% | |
| IV | 5 | 10.2% | 2 | 5.3% | |
| Staging Rectal Cancer | Group A (n = 41) | Group B (n = 34) | p-value | ||
| I | 6 | 14.6% | 9 | 26.5% | 0.606 |
| II | 13 | 31.7% | 10 | 29.4% | |
| III | 13 | 32.5% | 10 | 29.4% | |
| IV | 9 | 21.9% | 5 | 14.7% | |
| Staging | Group C (n = 59) | Group D (n = 74) | p-Value | ||
|---|---|---|---|---|---|
| I | 13 | 22% | 11 | 14.9% | 0.685 |
| II | 21 | 35.6% | 27 | 36.5% | |
| III | 18 | 30.5% | 28 | 37.8% | |
| IV | 7 | 11.9% | 8 | 10.8% | |
| Staging Right Colon Cancer | Group C (n = 24) | Group D (n = 37) | p-value | ||
| I | 7 | 29.2% | 3 | 8.1% | 0.103 |
| II | 7 | 29.2% | 13 | 35.1% | |
| III | 6 | 25% | 17 | 46% | |
| IV | 4 | 16.6% | 4 | 10.8% | |
| Staging Left Colon Cancer | Group C (n = 16) | Group D (n = 22) | p-value | ||
| I | 2 | 12.4% | 3 | 13.6% | 0.973 |
| II | 7 | 43.8% | 11 | 50% | |
| III | 6 | 37.5% | 7 | 31.8% | |
| IV | 1 | 6.3% | 1 | 4.6% | |
| Staging Rectal Cancer | Group C (n = 19) | Group D (n = 15) | p-value | ||
| I | 4 | 21% | 5 | 33.3% | 0.601 |
| II | 7 | 36.8% | 3 | 20% | |
| III | 6 | 31.7% | 4 | 26.7% | |
| IV | 2 | 10.5% | 3 | 20% | |
| Histopathological Data | Group A (n = 147) | Group B (n = 133) | p-Value | ||
|---|---|---|---|---|---|
| N+ % | 74 | 50.3% | 55 | 41.4% | 0.150 |
| EMVI | 64 | 43.5% | 64 | 48.1% | 0.472 |
| METS SITE | |||||
| Liver | 3 | 2% | 10 | 7.5% | 0.044 |
| Peritoneum | 1 | 0.6% | 3 | 2% | 0.394 |
| Lung | 3 | 2% | 5 | 3.6% | 0.484 |
| Grade | 0.624 | ||||
| 1 | 12 | 8% | 8 | 6% | |
| 2 | 84 | 57.1% | 61 | 45.8% | |
| 3 | 51 | 34.6% | 64 | 48.1% | |
| HISTOLOGY | 0.261 | ||||
| Adenocarcinoma | 104 | 70.7% | 88 | 66.2% | |
| Mucinous | 39 | 26.5% | 36 | 27.1% | |
| Signet-cell | 2 | 1.4% | 7 | 5.3% | |
| Other | 2 | 1.4% | 2 | 1.5% | |
| Histopathological Data | Group C (n = 59) | Group D (n = 74) | p-value | ||
| N+ | 23 | 39% | 32 | 43.2% | 0.732 |
| EMVI | 31 | 52.5% | 33 | 44.6% | 0.387 |
| METS SITE | |||||
| Liver | 4 | 6.8% | 6 | 8.1% | 1 |
| Peritoneum | 1 | 1.6% | 2 | 2.7% | 1 |
| Lung | 2 | 3.4% | 3 | 4.1% | 1 |
| Grade | 0.384 | ||||
| 1 | 3 | 5.0% | 5 | 6.7% | |
| 2 | 31 | 52.5% | 30 | 40.5% | |
| 3 | 25 | 42.3% | 39 | 52.7% | |
| HISTOLOGY | 0.372 | ||||
| Adenocarcinoma | 37 | 62.7% | 51 | 68.9% | |
| Mucinous | 15 | 25.4% | 21 | 28.3% | |
| Signet-cell | 6 | 10.2% | 1 | 1.4% | |
| Other | 1 | 1.7% | 1 | 1.4% | |
| Parameters | Group A (n = 147) | Group B (n = 133) | p-Value | ||
|---|---|---|---|---|---|
| Emergency Department Attendance | 72 | 49% | 89 | 66.9% | 0.003 |
| Regimen of Surgery | 0.068 | ||||
| Elective | 124 | 84.4% | 122 | 91.7% | |
| Emergency | 23 | 15.6% | 11 | 8.3% | |
| Hospital stay Days | 6.3 ± 3.7 Median 5 | 6.2 ± 4.6 Median 5 | 0.841 | ||
| ERAS compliance | 92 | 62.5% | 84 | 63.1% | 0.905 |
| Clavien-Dindo > 3 | 16 | 8.8% | 21 | 15.7% | 0.223 |
| 30 days mortality | 2 | 1.4% | 3 | 2.3% | 0.671 |
| Parameters | Group C (n = 59) | Group D (n = 74) | p-Value | |||
|---|---|---|---|---|---|---|
| Age (mean, SD) Year | 69.3 ± 12.1 Median 73 | 71.6 ± 11 Median 74 | 0.252 | |||
| Sex | Male | 27 | 45.8% | 50 | 67.6% | 0.012 |
| (%) | Female | 32 | 54.2% | 24 | 32.4% | |
| BMI (mean, SD) | 26.3 ± 4.3 Median 26 | 26.1 ± 3.8 Median 26 | 0.776 | |||
| Localization | 0.282 | |||||
| Right Colon | 24 | 40.7% | 37 | 50% | ||
| Left Colon | 16 | 27.1% | 22 | 29.7% | ||
| Rectum | 19 | 32.2% | 15 | 20.3% | ||
| Hemoglobin (gr/dl) (mean, SD) | 12.3 ± 2.2 | 11.4 ± 2.1 | 0.017 | |||
| Regimen of Surgery | 0.754 | |||||
| Elective | 55 | 93.2% | 67 | 90.5% | ||
| Emergency | 4 | 6.8% | 7 | 9.5% | ||
| Emergency Department Attendance | 33 | 55.9% | 56 | 75.7% | 0.025 | |
| Stoma creation | 16 | 27.1% | 17 | 22.9% | 0.106 | |
| ERAS compliance | 40 | 67.8% | 46 | 62.1% | 0.196 | |
| Hospital stay Days | 6 ± 4.5 Median 5 | 7.4 ± 5.8 Median 6 | 0.13 | |||
| Clavien-Dindo > 3 | 8 | 13.5 | 13 | 17.5 | 0.34 | |
| 30 days mortality | 2 | 3.4% | 1 | 1.4% | 0.587 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirozzi, B.M.; Siragusa, L.; Baldini, G.; Pellicciaro, M.; Grande, M.; Efrati, C.; Finizio, R.; Formica, V.; Del Vecchio Blanco, G.; Sica, G.S. Influence of COVID-19 Pandemic on Colorectal Cancer Presentation, Management and Outcome during the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 1425. https://doi.org/10.3390/jcm12041425
Pirozzi BM, Siragusa L, Baldini G, Pellicciaro M, Grande M, Efrati C, Finizio R, Formica V, Del Vecchio Blanco G, Sica GS. Influence of COVID-19 Pandemic on Colorectal Cancer Presentation, Management and Outcome during the COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(4):1425. https://doi.org/10.3390/jcm12041425
Chicago/Turabian StylePirozzi, B. M., L. Siragusa, G. Baldini, M. Pellicciaro, M. Grande, C. Efrati, R. Finizio, V. Formica, G. Del Vecchio Blanco, and G. S. Sica. 2023. "Influence of COVID-19 Pandemic on Colorectal Cancer Presentation, Management and Outcome during the COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 4: 1425. https://doi.org/10.3390/jcm12041425